
Abstract
A hereditary cancer predisposition can rattle families, creating dysfunctional interactions. Families need assistance navigating conversations about risk. Because mothers and daughters uniquely share breast cancer experiences and risk, there is a particular need for practitioners to assist them with communication. Three focus groups were conducted with 11 mothers with an elevated cancer risk (with adolescent daughters) receiving genetic counseling. We explored three inquiries to capture mother–daughter communication: emergent challenging topics (e.g., health-promotion behavior, daughter’s risk, mother’s risk of death), factors complicating discussions (e.g., balancing what to share and when, guilt and blaming, confusion about risk and prevention), and strategies enhancing conversations initiated by mothers (e.g., paying attention to daughter’s cues) or practitioners (e.g., inviting daughters to appointments). Findings suggested that mothers struggle to balance eliciting daughters’ concerns, providing them with support, and imparting knowledge without overwhelming them. We offer mothers and practitioners guidance to help facilitate these conversations.
Keywords
Family members can share genetic variations and, as such, disease risk. Families considered to be at elevated risk for breast cancer typically have breast and/or ovarian cancer diagnosed at early age(s) and sometimes in more than one relative. It is not only critical for these families to understand their family cancer history and risk, but also to communicate with each other about that risk and strategies for disease prevention.
Families who are at an elevated risk for genetic conditions commonly seek genetic counseling or genetic cancer risk assessment (GCRA). Genetic counselors play a prominent role in helping these families understand their risk. The presence of a hereditary cancer predisposition can rattle family dynamics, exacerbate anxieties, lead to confusion and disagreement, and result in dysfunctional family interactions (McDaniel, Rolland, Rubin, & Miller, 2006). It is imperative that families be offered assistance with navigating their conversations in a healthy manner.
In recent years, the genetic counseling field has called for theoretical paradigms to guide this medical practice (Galvin & Young, 2010). Because a genetic predisposition affects multiple family members, the use of a family systems lens enables genetic counselors, and other health practitioners who work with such women, to incorporate their understanding of the complexities of family dynamics and interactions into their clinical practice and recommendations (Galvin & Young). Using family systems theory and associated models, genetic counselors can tailor their counseling in a manner that addresses prominent family focused concerns. With this lens as a guiding framework, we sought to better understand the mother–daughter communication challenges faced by women with breast cancer and/or familial risk.
Family Systems Theory and Genetic Illness
Family systems theory offers a framework for the ways in which families might respond to health and illness. As Galvin and Young (2010) explained, When viewed as a system, families are dynamic, influenced by the ongoing development of family members and their relationships with each other. Ongoing fluctuations occur as every family member affects the other and is in turn affected by them. . . . Family systems foster the exchange of resources such as information and support, . . . influence action among family members and can change or evolve as a function of these actions. (p. 103)
Thus, to fully understand an individual’s experience with health and illness, their family environment should be taken into account.
Rolland’s (1994) Family Systems-Illness Model highlights how family functioning (in the presence of illness, health, and loss) relates to many complicated familial factors such as a multigenerational history of health and coping, individual and family development, the family’s health/illness belief system, social support, and the ability of the family to manage cancer-related information or crises. In 2005, Rolland expanded this model into the Family System Genetic Illness Model (see Rolland & Williams, 2005), which considers the psychosocial impact of hereditary or familial risk both before and after genetic testing. Several family system factors (relational closeness, rules, roles) can impede or facilitate kin communication following genetic testing (Chivers Seymour, Addington-Hall, Lucassen, & Foster, 2010). By utilizing a family systems approach, health practitioners can help families anticipate challenges that might arise and topics for discussion while guiding them within the context of that family’s unique patterns.
One important family dynamic for mothers with elevated cancer risk is their relationship with their daughters. Many women who are at “elevated risk” for breast cancer seek counseling about breast cancer susceptibility (BRCA) or BRCA1 or BRCA2 genetic testing, and those who have a daughter are more likely to do so (Geller, Doksum, Bernhardt, & Metz, 1999). They want to not only better understand their personal risk but also to identify how it impacts their family members (Douglas, Hamilton, & Grubs, 2009). There are several topics that commonly arise during genetic counseling sessions, including uncertainty about the testing process, personal risk, genetics in general, and the condition to which they are predisposed (Segal et al., 2004). Women also describe significant concern and uncertainty about implications of their genetic profile to their offspring’s health, in particular, their daughter’s disease risks and options for prevention (Bylund et al., 2012), regardless of their daughter’s age (MacDonald, Sarna, Weitzel, & Ferrell, 2010).
Parents who have BRCA1/2 testing are more likely to disclose results to daughters, and when a parent is a mutation carrier, the child is more likely to experience distress during this disclosure (Bradbury et al., 2012). Just talking about health promotion or risk is complicated for parents, and little is known about how to do so in an adaptive manner. Moreover, the mother’s challenge becomes how to foster her daughter’s growing independence without either letting these concerns inhibit the emergence of the daughter’s fledgling identity, or erupt into a battle for control over a future that neither of them can predict (Shrier, Tompsett, & Shrier, 2004). For both breast cancer experiences and disease risk, there seems to be an inherent mother–daughter connection to which health practitioners should attend (Wiggs, 2011).
Breast Cancer: A Mother–Daughter Connection
Research to date, although scarce, suggests that mothers and daughters tend to “share” the breast cancer experience psychologically, physiologically, and interpersonally. Mothers and daughters exhibit the same mental and physical distress after only one of them is diagnosed with cancer. Boyer et al. (2002) found that daughters mirrored their mother’s psychological distress (e.g., symptoms of posttraumatic stress disorder), and Cohen and Pollack (2005) showed that this can extend into physiological stress responses (e.g., immunological changes) for the daughter. They also share the disease experience interpersonally. Daughters often experience role changes when they support their diagnosed mother for the first time, a task that is not without difficulties (Berlin, 2008; Fisher, 2010, in press).
In addition, having a mother with cancer increases a daughter’s cancer risk. Wiggs’s (2011) narrative analysis of women’s writing about their breast cancer experiences demonstrates the prominent impact of the disease on the mother–daughter relationship, and also how concerns of personal and familial risk are at the center of women’s experiences. Daughters face a dual battle: a chronic fear of disease for themselves and fear of recurrence or progression for their mother. Kenen, Ardern-Jones, and Eeles (2003) have described this as a psychological chronic risk for daughters. Mothers manage similar fears: worrying about disease recurrence or progression for themselves as well as their daughter’s future disease risk.
In summary, breast cancer risk poses unique challenges to the development of this maternal relationship as both mothers and daughters cope with their own personal risk and, concurrently, might wish to support one another. In line with the Family System Genetic Illness Model (Rolland & Williams, 2005), this interconnectedness begins long before diagnosis or genetic testing. This heightens the need for practitioners to attend to mother–daughter issues in families with an elevated disease risk and contemplating BRCA testing. Practitioners are uniquely poised to help these women and their families manage these difficult interactions.
Mother–Daughter Communication and Breast Cancer
Research on mother–daughter communication and breast cancer has shown that the nature of their interactions plays a central role in determining their ability to cope and willingness to engage in health-promotion behavior (Bylund et al., 2012; Fisher, 2010, 2011, in press; Fisher, Miller-Day, & Nussbaum, 2013; Fisher & Nussbaum, 2012; Sinicrope et al., 2009). Recent research demonstrated that it is critical for mothers to talk to their daughters about health promotion with regard to cancer because mothers can influence their daughters’ health-promotion behavior across the life span, including adulthood. Sinicrope et al. examined the advice-receiving experiences of more than 2,000 adult daughters in later life. According to the daughters, mothers rarely provided them with advice (only 9% of this sample) about screening behavior (e.g., getting mammograms, exams, and so forth), but the daughters who received such advice tended to follow it (89%). Having a mother or first-degree relative with breast cancer helped predict whether daughters would follow their mother’s advice.
This research suggests that for elevated-risk families, mother–daughter communication is especially critical. Discussing risk-reducing behaviors with daughters when they are younger seems especially prudent. Mother–daughter communication could be an important pathway through which young women and girls adopt breast cancer screening and risk-reduction behaviors. Even though these women were of an earlier generation, for whom cancer was commonly considered taboo and not discussed, the impact of their mother’s advice sustained over time.
Still, mother–daughter communication about cancer and health risk can be emotionally charged and, thus, challenging. Even though mother–daughter communication can be a vital means of emotional support for both parties (Fisher, 2010, in press), talking about cancer is not easy. For diagnosed mothers, simply speaking about health-promotion behaviors (e.g., describing how to do a self-breast exam, when to get mammograms or genetic testing) with their adolescent (aged 11 to 17) or emerging-adult daughters (aged 18 to –25) can evoke emotional distress among the daughters, causing them to withdraw and cut off communication (Fisher, 2010, in press). The complicated nature of mother–daughter health communication extends to those women who are classified as high risk because they tested positive for a BRCA mutation, and to those with elevated risk because of a family history of cancer. These women admit to not knowing how to talk about risk with their daughters or what information to share with them (Bylund et al., 2012), and they worry about their daughters coping (Fisher, 2010, in press).
This research demonstrates that mothers need assistance and support from the medical community in talking to their daughters about their health, illness, and risk. These discussions have the potential to increase daughters’ awareness of their family history and play a critical role in disease prevention. Mothers guide daughters’ decisions to engage in health-promotion behavior and are a central source of knowledge and support. As such, facilitating talk about elevated cancer risk and prevention is a critical area in which genetic counselors and other health practitioners can intervene.
Research Inquiries
Although existing literature suggests the importance of mother–daughter communication about genetic risk, research on the nuances of both challenging and helpful interactions is lacking. To better understand the impact of elevated risk status on mother–daughter communication, and to seek useful knowledge for counseling families, we sought to explore multiple layers of mother–daughter interactions. From mothers’ perspectives, we sought to understand what topics mothers and daughters discuss, what challenges mothers perceive to complicate these discussions, and which communication strategies seem helpful. Our first aim was to capture what (cancer-related) topics elevated-risk mothers reported discussing with their daughters. Second, we explored challenges mothers perceived to further complicate such discussions. Finally, we examined strategies mothers perceived can enhance mother–daughter communication about these topics.
Method
Recruitment
The data we collected for this study were part of a two-phase project to study clinicians’ approaches to communicating hereditary risk information to mothers with breast cancer (or breast cancer risk) about their daughters and to produce information valuable to intervention development. Phase 1 of the project involved video recording genetic counseling sessions at the Clinical Genetics Service (CGS) of Memorial Sloan-Kettering (MSK) Cancer Center in New York, New York. We used these data to explore the nature of women’s genetic counseling sessions and interactions with providers, with a special focus on issues pertaining to their daughters. Our results from Phase 1 of this project are reported elsewhere (see Bylund et al., 2012; Maloney et al., 2012).
The study reported herein is based on Phase 2 of the study, in which we conducted three focus groups of mothers who had attended genetic counseling sessions (n = 11) to better detail their concerns about their daughters’ risk and their communicative approaches. Focus groups were used for Phase 2 because peer interaction among participants increased the richness and depth of understanding of these complex issues in a supportive environment. This level of appreciation is essential to allow overarching themes to emerge. Moreover, focus groups allowed women to explore issues of concern to them outside of a practitioner–patient appointment or counseling session, thereby increasing their comfort level and extending an opportunity for richer data collection. From a logistical perspective, focus groups were also the most practical method, given the difficulty of recruiting this particular group of participants (women with elevated risk) and the need to limit the time requested of them in a clinical setting (Morgan, 1997).
Participants
We recruited participants through the CGS and reviewed the clinic appointment schedule to identify potential participants. A consenting professional telephoned patients before or after their CGS visit to offer participation and explain the study. Each patient was given the opportunity to participate in both phases of the study. Criteria for inclusion were (a) having a personal history of breast cancer or having been classified as a potential gene carrier based on family history, (b) having a biological daughter between the ages of 12 and 20 years, (c) having received genetic counseling at the MSK CGS, and (d) having sufficient English fluency. Participants were 11 non-Hispanic White women aged 40 to 59 years; 5 were of Ashkenazi Jewish descent. Nine had a personal history of breast cancer, and 9 had a strong family history of breast or ovarian cancer. Five women had had lumpectomies; 5 had had mastectomies; 6 had undergone radiation therapy; 8 had undergone chemotherapy; 5 had undergone hormonal therapy; and 2 had had total abdominal hysterectomy/bilateral salpingo-oophorectomy (TAH/BSO). Eight women had received more than one of these medical interventions. Two women were BRCA gene mutation carriers.
Procedures
Upon arrival to each of the focus groups, participants were consented, introductions were made, and ground rules for confidentiality and respect for one another were established. The three focus groups were led by two members of the research team in accordance with the established methodology of Krueger and Casey (2000), keeping groups small and manageable (three to five women each) and conducting them in a series. Each group was moderated with the same semistructured script. We asked women questions about their experiences (as mothers who were at an increased risk of developing breast cancer) to capture the unique nature of living with a high or elevated risk of cancer. Women were asked to describe their concerns for and previous interactions with their daughters and probed for details about their communication dynamics. They were also asked about their interactions with providers about their daughter-related concerns. Participants were allowed to dominate the discussion and interact with one another. Each group lasted approximately 90 min. All groups were audio-recorded and transcribed for analysis.
Analysis
Transcripts for focus groups resulted in nearly 100 single-spaced pages of data. Analyses were conducted for each research question independently using Glaser and Strauss’s (1967) and Strauss and Corbin’s (1998) constant comparative method. This resulted in a set of themes for each inquiry. To become immersed in the data, we began by reviewing the transcripts in full multiple times prior to an initial team discussion; two authors subsequently conducted the analysis.
Analysis began with the creation of a coding manual for each research question by analyzing one focus group transcript. Data were analyzed according to van Manen’s (1990) “selective approach” using the qualitative management program ATLAS.ti.6.2 (Atlas.ti Scientific Software Development, 2010). We employed three analytical steps outlined by Strauss and Corbin (1998), beginning with the discovery of concepts and assignment of conceptual codes to text. The analysis then proceeded with the creation of categories by grouping related concepts in an effort to reach “thematic salience.” Thematic salience was reflected in recurrence, repetition, and forcefulness (Owen, 1984). When possible, category labels were generated in vivo to maximize trustworthiness of the findings. The final step involved refining themes and identifying dimensions that characterized these categories to ensure thick description (Geertz, 1973).
Once the initial coding manual was established, two authors analyzed the remaining data in three research phases. Each phase consisted of independently analyzing the data using the coding manual, according to the aforementioned analytical procedure. The authors kept individual memos to think and write about their interpretations of categories while coding. These were discussed when collectively comparing analyses to decide among different interpretations as they arose. Throughout this process, the coding manual was revised as necessary. This approach was conducted separately for each research question.
Also, because in this study we employed a focus group approach and questions remained generally the same for each group, frequency counts were included in the analyses to understand the more prominent experiences of mothers and daughters. Given the small sample size, frequency of themes was at the individual level vs. the focus group level and was noted in the tables; all themes emerged in at least two of the three focus groups and were reported by more than one participant. The final codebooks or sets of analyses were then reviewed by a third author and updated accordingly.
We present the analyses as thematic findings to answer each inquiry but do so in the form of thematic phrases and statements to increase the utility of these findingsfor health intervention design and implementation (Sandelowski & Leeman, 2012). Rather than only present labels or codes of emergent categories, we categorize topic labels (themes) into action-oriented thematic statements that can be integrated into interventions and psychosocial materials in an effort to enhance mother–daughter communication in families and medical practice. This approach is in line with Sandelowski and Leeman’s recent recommendations for health research to be more easily translated into practice. Findings are also presented in tables using Banning’s (2003) “ecological sentence synthesis” approach (see also Sandelowski & Leeman) to provide additional thematic statements.
Results
For each inquiry, thematic phrases, associated dimensions (characteristics), and frequency rates are presented in Tables 1 to 3. We use mothers’ own words to illustrate the thematic findings, which are presented from most frequent to least. We also include conversational excerpts to help illustrate the reiterative methodological process of data collection. When more than one mother in a group was talking, a number is used to differentiate between them. To protect women’s confidentiality, we do not include identifying information.
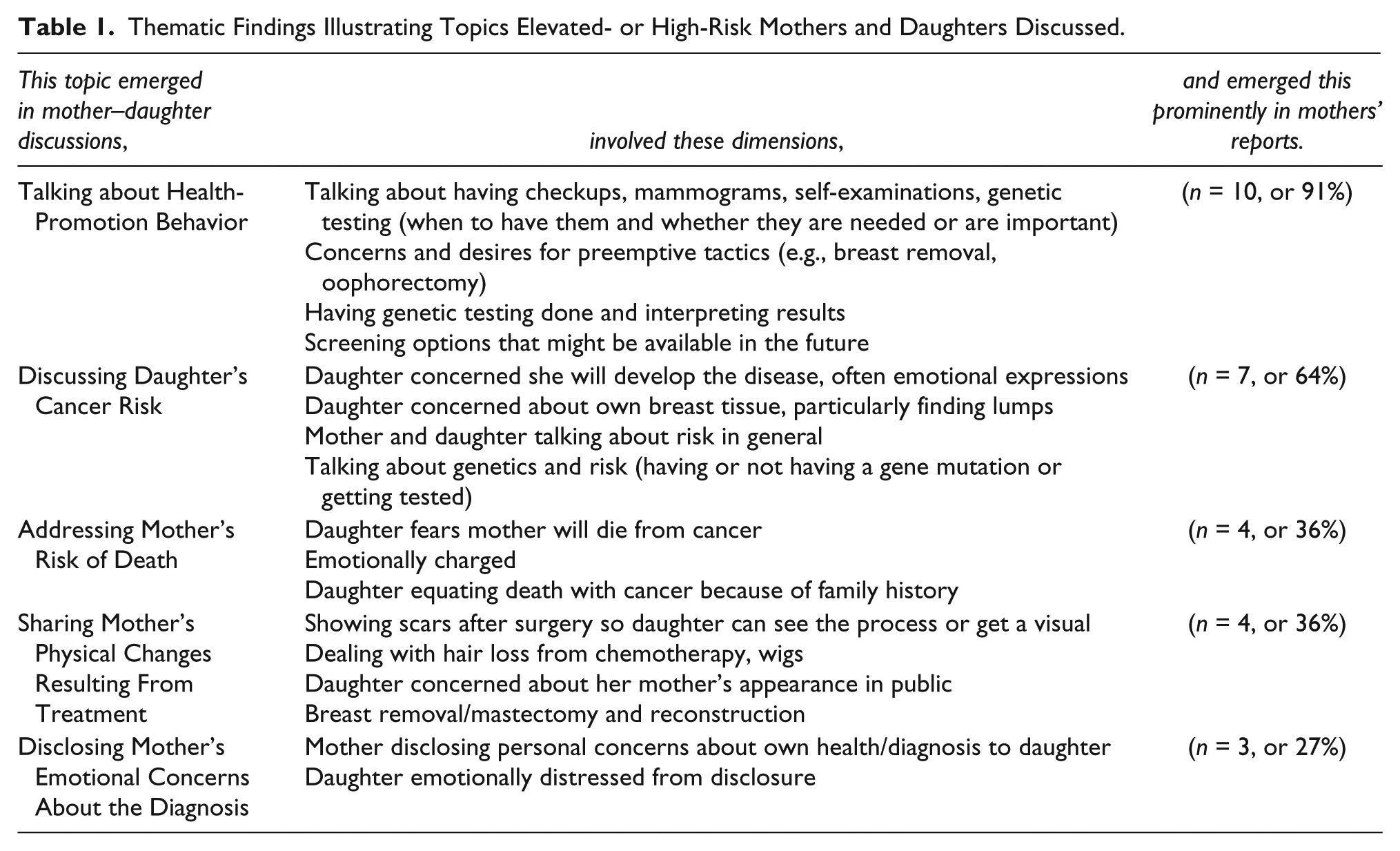
Thematic Findings Illustrating Topics Elevated- or High-Risk Mothers and Daughters Discussed.
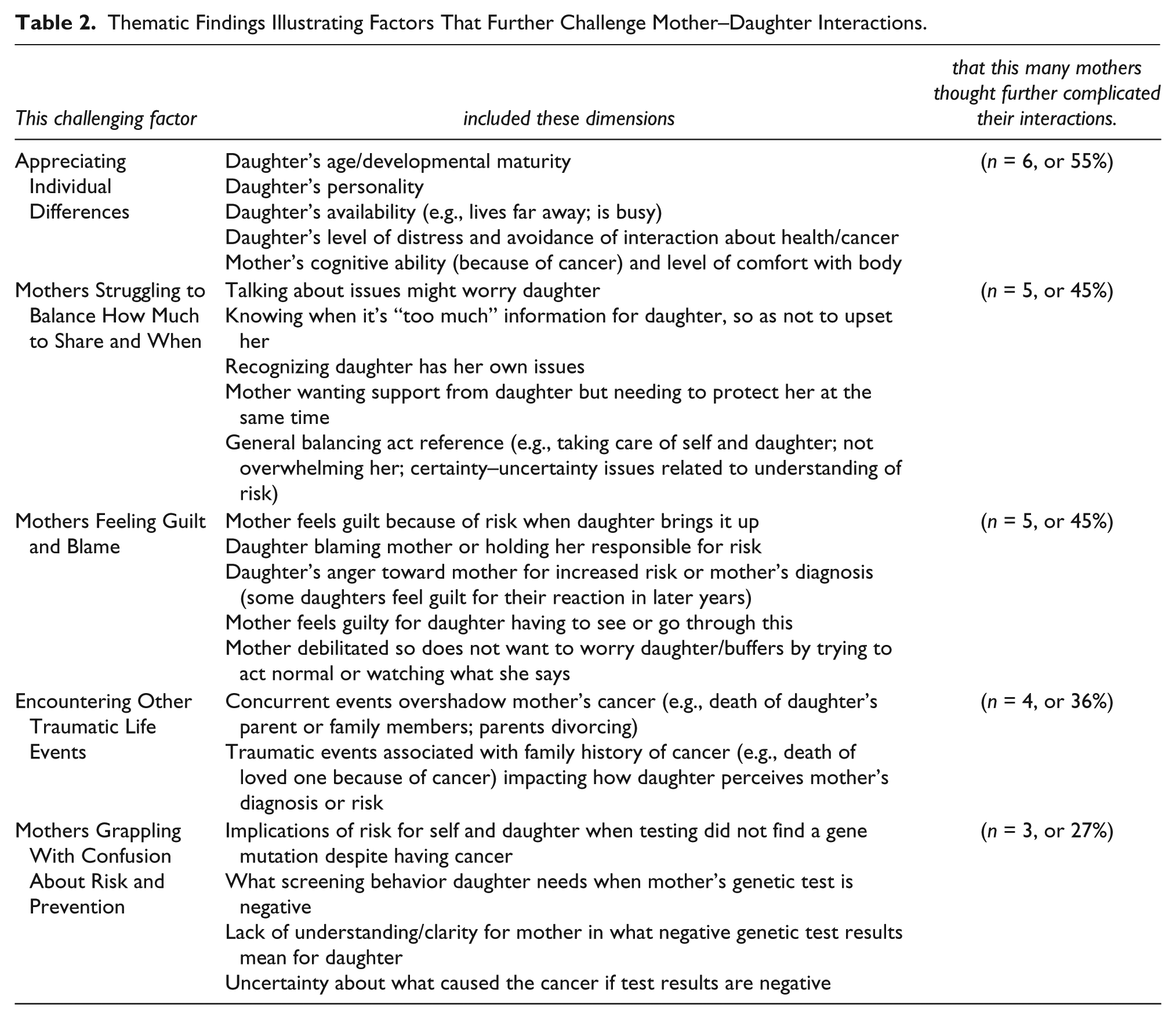
Thematic Findings Illustrating Factors That Further Challenge Mother–Daughter Interactions.
Thematic Findings Illustrating Mothers’ Communication Strategies to Enhance Mother–Daughter Communication.
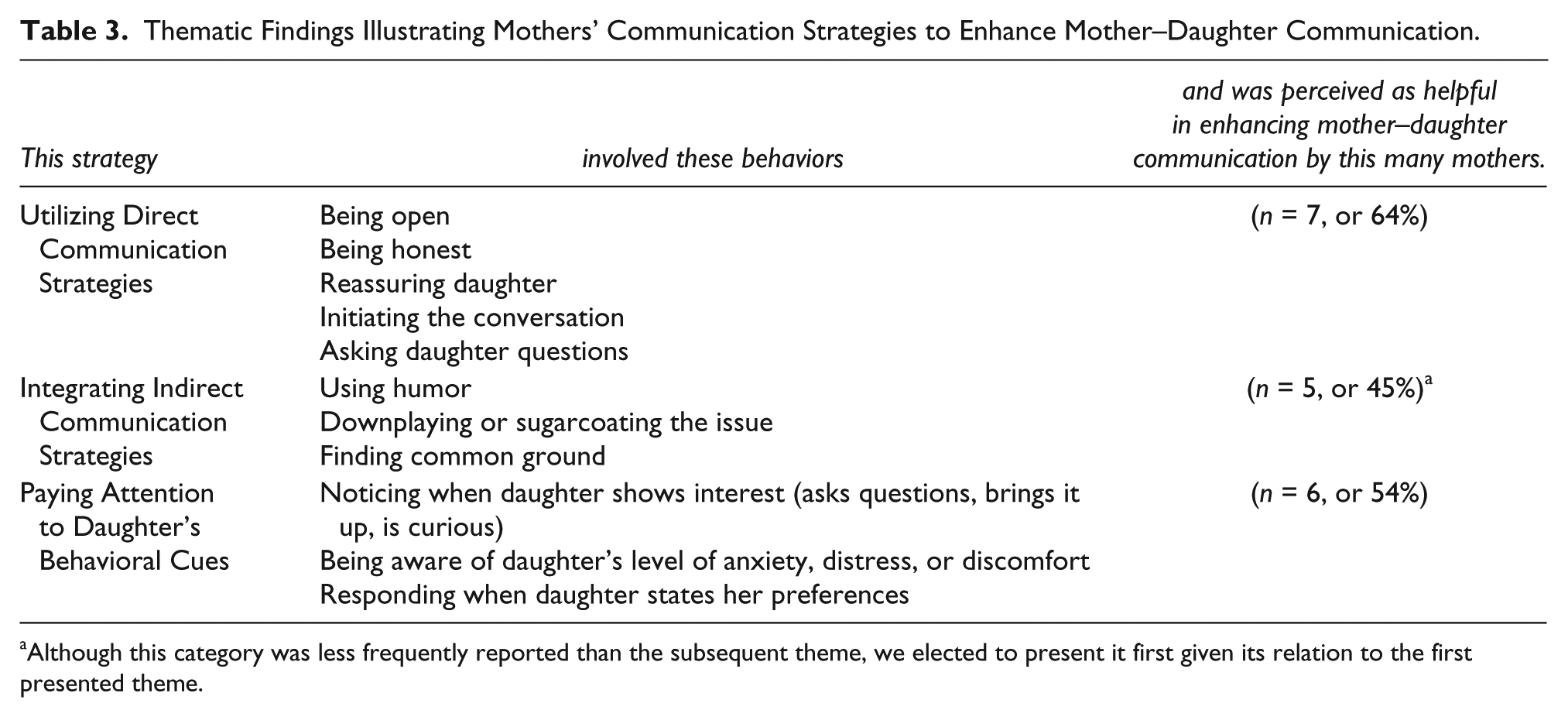
Although this category was less frequently reported than the subsequent theme, we elected to present it first given its relation to the first presented theme.
Research Question 1
For our first research question, we sought to better understand the nature of mother–daughter communication by capturing mothers’ perspectives of emergent topics in interactions between themselves and their daughter. According to mothers’ experiences, five themes emerged and bring to light topics daughters or mothers were concerned about or issues that could arise in their interactions and, therefore, warrant some discussion. In Table 1 we illustrate these themes.
Talking about health-promotion behavior
Mothers described discussing health-promotion behavior with their daughter. Although these discussions centered on the daughter’s screening behavior, at times the talk focused on the mother’s own health-promotion behavior. Mothers recalled conversational topics that included questions or concerns about various health-promotion behaviors and topics including routine gynecology visits (e.g., the daughter questioning whether she needed to see a doctor or the mother advising the daughter about needing checkups because of her risk), age at which the daughter should start mammograms or screenings, the mother informing her daughter that she genetic testing or what the results meant, concerns about whether prophylactic tactics (e.g., risk-reducing mastectomies or salpingo-oophorectomies) were necessary, doing regular self-breast examinations, and the importance of knowing their family medical history. Mothers also recalled talking to their daughter about how health-promotion behavior or screening could change in the future.
At times, these conversations seemed to emerge when the mother believed her daughter was mature enough to understand that she had an increased disease risk. As one mother stated, As years have gone by and she’s gotten older and more able to process things, I have told her that there is a certain amount of risk, and she has more of an understanding now that she has to—at a certain point—go for checkups and whatever is involved.
Often, mothers expressed that their daughter should be more “proactive” because of their heightened family risk
Even though I don’t have the gene now, [I told her] we have to be proactive and you’re gonna have to go here and you’re gonna have to be in surveillance. And you’re gonna have to have a mammography and breast exams earlier than the average person.
You really are sort of talking to them about what screening is gonna be like and that their health care is going to be different from other girls.
Yeah.
At the same time, not all mothers focused on their heightened risk when talking to their daughter. Some encouraged their daughter to be proactive, simply as good general health practice: I just tried to encourage her as a growing young woman who was off on her own in college that she had to be responsible for her own health and that if she was sick she had to get to the health center. That she should take responsibility and make appointments with the gynecologist, and I could make an appointment when she was home if she wanted. . . . I’ve just tried to be proactive with her, not because of anything special in particular because of my health, but these are just responsibilities for her and her health care that she needs to.
Regardless of the mother’s initial motivation for having the conversation, the topic often addressed what age a daughter should begin screening and what risk-reducing options the mother (or grandmother) might have used (e.g., bilateral salpingo-oophorectomy after having children). It was often tied to a second emergent theme: the daughter’s concerns of developing breast cancer.
Discussing the daughter’s cancer risk
More than half of the mothers recalled talking to their daughter about her cancer risk, a conversation often triggered because the daughter expressed general concern (e.g., “Will I get it [cancer]?” “Should I be concerned?”). Women sometimes recalled strong emotions from their daughter, which at times co-incided with the mother disclosing a positive genetic test result: “Well, I did tell them that I did have the gene and everything. They were nervous at first. I mean my little one cried and my big one was like ‘What does that mean for me?’” Sometimes daughters also disclosed anxieties about their own breast tissue or size. For instance, as one mother explained, “[My daughter said], ‘Mom, what does it mean if I feel something lumpy?’ She worries about that.”
Addressing the mother’s risk of death
According to mothers, talking about their risk of death was another emotionally charged topic for daughters. This theme emerged in the experiences of women who had a previous cancer diagnosis. Daughters disclosed fears that their mother was going to die from the disease, and this topic seemed especially emotional for younger daughters. One mother recalled her 11-year-old daughter saying, “Are you gonna die?” Sometimes this fear was tied to whether other family members had died from the disease (e.g., a grandparent). One mother explained how this fear seemed natural, even if the daughter did not know the individual who succumbed to the disease: [My kids] knew a lot about [cancer] because we have a lot of people in our family that have died from it already. . . . My mother died from it. And her sister died from it. And their other sister died from it, although they weren’t that acquainted with that particular sister because she lived [in another country]. They had really no memory because my mother has been dead since [before their birth]. . . . Their feeling on it was not that they expressed it but I found out later on, they just assumed that I would die too. They just thought that everybody who had cancer died automatically. They didn’t realize the ins and outs and how long it could be, that there could be a recurrence.
As this mother highlighted, daughters did not always disclose this fear when the mother had cancer, and instead waited until treatment was completed or even later in life. Regardless, the assumption that “a cancer diagnosis always results in death” might have seemed logical to some daughters, given their family’s prior experience.
Sharing mother’s physical changes resulting from treatment
Women with cancer also talked to their daughter about physical changes that occurred as a result of their treatment. They recalled showing their surgical scars, describing hair loss or the need for a wig because of chemotherapy, and also the experience of having a mastectomy and/or reconstruction. Several used humor to broach this topic. For instance, one mother framed her reconstruction as one of the “perks” of having breast cancer. At times this topic emerged as an effort to help the daughter understand what they were going through. One mother showed her scars, saying, “This is what it looks like.” Others used physical changes as a means of connecting with their daughter and of dealing with the change themselves:
The hair thing was a big deal in our house.
One good thing I did. I had my daughter come with me when I had my head shaved.
Oh boy, you’re brave.
Well, I also figured it was something that she could somehow relate to or get into, and we had my hair braided and we sent the braid—I had very long hair—and we sent the braids off [to the wig maker], and we were taking pictures. So I wanted to be part—
It’s like a bonding moment.
Yeah, as well as prepping myself.
Mothers described physical appearance as a particularly poignant issue for daughters. One mother recalled, “We were going for parents’ weekend and [my daughter] was very concerned how I was gonna look in a wig with her roommates.” Another mother echoed, Appearance is a big thing . . . especially with girls. . . . I’d gotten the wig ahead of time. I put it on and I hadn’t lost my hair yet. And I went into dancing class to pick [up my] sixteen-year-old, and she pushed me right out the door. Like don’t—and I was like, “What’s the big deal? In another two or three weeks I’m gonna have to be wearing it anyway.” And she was like, “Yeah, but you don’t have to wear it yet.”
Talking about the physical changes was also a time in which daughters could support their mother’s management of these changes and potentially normalize the experience for daughters: I actually never wore my wig. I hated it. It was itchy. I had three of them. I never wore any of them. And it was my kids who told me, “If the itching is bothering you don’t wear it. It’s stupid. Do what makes you feel comfortable.” I think that they almost see that chemo’s [chemotherapy’s] not as bad as it used to be.
Disclosing mother’s emotional concerns about the diagnosis
Mothers who had had a diagnosis sometimes disclosed their own emotional concerns with their daughter. Mothers initiated this conversation in an effort to cope themselves or to attain support from their daughter. According to mothers’ observations, some daughters were able to serve in this role, but not always. The following discussion between mothers illustrates this seemingly double-edged sword:
When I first found out I had bone cancer, because I’m a single woman, I came home and I dumped on her. And the whole night she was just so upset, which was the biggest mistake I could’ve made. And I really needed to just tell someone else.
You need someone else.
Or have a friend come over, but honestly, she’s the one I really wanted to tell because she’s a friend almost, which is not good, I know.
You’re close.
Yeah, we’re very close, and she had the worse—and then she told me later, “You can’t tell me. I can’t handle the cancer.” (laughs) So I think I learned my lesson.
I know the feeling.
Mothers at times recalled how voicing their emotional concerns seemed distressing for the daughter to hear, like other topics. As such, some mothers expressed that this topic should not always be shared in this relationship.
Research Question 2
In our second inquiry, we ascertained factors that made these conversations more challenging or complicated. The five themes that emerged are presented in Table 2. These factors help families and practitioners foresee challenges they might need to manage to better facilitate conversations about the aforementioned topics.
Appreciating individual differences
Mothers described how both the daughter’s and their own individual differences complicated their cancer-related interactions. Women focused on diverse factors, including the daughter’s availability, age/maturity, avoidance level (in terms of willingness to talk about cancer or health/illness), and personality. For example, mothers described how their interactions were influenced by their daughter’s availability, such as having a busy schedule or geographical distance: I don’t feel like I have closure so I don’t know. I’m still at this point [of], what do I do? And how do I handle that? I’m still clueless about that. How do I have a conversation? I mean, one [daughter] is out of the country. She’s been there, out of the country, for four years. How do I have this conversation with her?
Mothers also described the daughter’s developmental maturity as influencing their ability to initiate talk: “Depending on the developmental level, what to tell a child, what she needs to hear at that point . . . what each child can handle and should be aware of and how to present it.” One mother put this into the context of a daughter’s adolescence: I think for me it was really hard because my daughter didn’t want to even know me [laughs]. She’s thirteen and she’s kind of like, she stayed with her friends. And she just, she didn’t even—somehow I think they’re still young. You know? They just, they can’t talk to me about certain things. They just want to live in a happy world.
Mothers also expressed that their daughters differed in level of avoidance. Some daughters avoided talking about medical issues in general, whereas others only when it was personal (about the mother or daughter). Another recalled her daughter withdrawing after attending a chemotherapy appointment: “When she got home she just went up to her room and she stayed there. She didn’t come out. That was it. She was done. She didn’t want to talk about it.” Mothers sometimes perceived the daughter’s avoidant behavior as her way of coping with a distressful experience and were at a loss as to how to manage that. This often led to a communication impasse: “I really don’t know what I could’ve done differently or how I could’ve made it easier for her or could’ve talked to her. . . . She was totally like, ‘Leave me alone.’” Some mothers recognized multiple factors such as age and personality that played a role in their daughter’s avoidance: She has not taken it very well, and because of that I also have not been very forthcoming with her. I did not tell her that I did genetics counseling. I did not tell her the results. She’s a smart girl. She may have done inquiry on her own, but because of her own personality and her own grief and anger, she has not been a very sympathetic person to me. And I’ve kept her just kind of disinvolved from it. She did come home for my surgery and was very supportive at the initial stages, and even did some college fundraising of a raise for cure kind of thing. But that’s really it. She doesn’t want to know. I think she’s terribly frightened. I would like to give her information to make her less frightened of it but I see she’s not ready for it.
A couple of mothers shared how their own personality and coping complicated their mother–daughter interactions (e.g., being uncomfortable about their own bodies). One mother who had a mastectomy and reconstruction shared, “It makes me uncomfortable ’cause I wanna bring it up. I wanna say, ‘Do you wanna see?’ But I’m uncomfortable with being undressed.” For another, chemotherapy impacted her cognitive astuteness: I think that I had some issues with memory, a little memory loss. [I had] a lot of fuzziness after the chemo. I think it’s—I don’t know if it’s other factors, my aging, what it is. I always bring it back to that time. It’s harder for me to process things and retain things [as] another factor in terms of how I would talk with my daughter. What do I really know and how can I be so clear when I convey it? I really need outside help.
Regardless of whether individual differences pertained to the mother or the daughter, mothers described how these factors complicated interactions by impacting the comfort level of both parties in these discussions. One woman summed this up by stating, “They are all different. . . . You just have to figure out which [approach] is best for your daughter.”
Mothers struggling to balance how much to share and when
Mothers found it challenging to balance how much to disclose to their daughter and when. They described this as an ongoing balancing act they were aware they needed to manage, but often were unsure how to do so. This included attempts to ascertain what was “too much” information for the daughter. Mothers talked about not wanting to raise a topic because it might cause the daughter to worry. As with the previous theme, daughters’ ages, personalities (e.g., she’s a “germaphobe”), or avoidant behaviors were perceived to play a role.
Mothers also did not want to burden their daughter, knowing she had her own life and, therefore, daily challenges that had nothing to do with health or illness (e.g., school or work problems, romantic partner challenges). Mothers often faced the dilemma of desiring support from their daughter and wanting to protect her from unnecessary stress. Many mothers did not want to say too much to “scare them off” or make their daughters “fearful,” yet wanted to give their daughters knowledge to protect themselves:
I just want to say I think that the main difficulty is knowing, especially when you’re confused about your own health, knowing the line, like how much do you tell and how much do you not tell, because you want people to know the truth. My daughter thrives on knowing facts. Like, she becomes very, too anxious, and sometimes uncertain. She wants to know.
Right. Information is a pathway to coping. Yeah.
But you don’t want to overwhelm them with the information either.
And they’re still young.
Right.
And then defrost it. The imperfection of where genetic testing is right now is that you can’t achieve that level of certainty yourself.
Correct.
The above conversation also highlights how the uncertainty of science (such as with genetic testing) can further complicate this balancing act.
Mothers feeling guilt or blame
Mothers’ feelings of guilt or blame also complicated their interactions with their daughter. At times, this was felt when the daughter expressed blame to her mother for having passed along her increased risk. One mother recalled, “My daughter kind of holds me responsible both for cancer and the divorce. And she says, ‘I’m never getting married now and I know I’m gonna get cancer.’” Another mother stated, “My daughter just got really angry at me and said, ‘Between your cancer and so-and-so had diabetes and on Dad’s side whatever. . . . What does this mean for me?’ . . . So yeah, she makes me feel a little guilty.”
Guilt was an emotion mothers grappled with independently. Mothers felt responsible for their daughter’s disease risk or guilty that their daughter had to see them sick. Essentially, mothers described feeling responsible for their daughter’s distress. At the same time, though, mothers understood that their risk or disease was not their fault and not within their control. They recognized the guilt as an emotional, rather than intellectual, experience. Some avoided “cancer talk” so as not to trigger emotional reactions from their daughter:
Can you put into words more what you’re wanting to protect your daughters from?
Well, obviously the way I was looking. The way they knew I was feeling because [I] was also trying to mourn my father. And they knew my father had prostate cancer for eight years, and the last year was a living hell. So after seeing all of that I didn’t want them to have to see it through me.
If they saw you being more sick or more upset.
It made me feel guilty, I have to tell you.
Me too.
Okay. Okay. What do you feel guilty about?
Because when you see your mother laying there, and I didn’t wear a wig or anything, and I always wore the kerchiefs and everything. So that was a big joke in the house too. So now I’m like all excited like, when am I gonna get my first haircut? [laughs] Just silly things, just to try to lighten it up now. I felt bad that they have seen me going through this. . . . I think they were worried about me.
Encountering other traumatic life events
Some women encountered traumatic life events (e.g., divorce or loss of a loved one) that complicated their cancer-related discussions with their daughter. As one woman explained, other life crises (sometimes concurrent with diagnosis/treatment) were somehow much more present in their life, and devastating (e.g., the daughter’s father passed away), and overshadowed their own cancer or risk, thereby limiting communication about it. This factor also seemed to intersect with other thematic findings. For instance, as noted in mothers’ experiences of guilt and blame, one mother illustrated how her daughter blamed her for the parents’ divorce.
Cancer-related traumatic events occurring prior to their own diagnosis also affected how mothers talked to their daughter about their cancer. By virtue of being at an elevated risk for cancer, these women shared a family history with numerous cancer diagnoses and/or related deaths:
Well, [my parent] passed away from prostate cancer, and then six weeks later I was diagnosed with breast cancer [starts to get upset]. Yeah, so it was not a good year. And my daughters were very close to my father, so telling them was [takes a break because upset]. Sorry.
It was hard. Yeah.
One of the worst things I’ve ever did [crying].
What kinds of things have you all been talking about? You know, just to what kinds of questions they have.
Well, of course at first they were upset thinking that, because my father had just passed away, and that was their concern, [so] of course convincing them that that wasn’t going to be the case.
Mothers grappling with confusion about risk and prevention
Mothers described their risk (or their daughter’s) as very “confusing.” They expressed uncertainty about how to recommend their daughter address her own risk, which challenged their ability to talk to their daughter. This factor seemed especially difficult for women who had a negative genetic test result but knew they still had an increased risk because of their personal and/or familial history. One mother said, “I don’t know how clear I am myself about the results, to tell you the truth. . . . I don’t know how to convey it to my daughter clearly.” This challenging factor was also notable for mothers with a personal cancer history who did not carry the gene mutation:
I don’t have the gene. So then where—? . . . and then of course no one knows with cancer where does it come from. . . . So I think it is confusing. . . . And actually I thought I was gonna have the gene . . . that [a negative test result] made me okay. And then my sisters can get theirs and my daughter. But since I don’t know, I’m like, “Okay, where did this come from?”
Mmm hmm. Right. So a challenge is communicating about this uncertainty.
Right.
It sounds like, how do you talk to your daughter when you yourself—
Totally confused.
Right.
In essence, women found their risk difficult to understand and, therefore, were uncertain how to guide their daughter’s screening and prevention behavior.
Research Question 3
In our final research inquiry, we sought to identify communication strategies that mothers anticipated could help facilitate these important conversations. The strategies mothers described could be categorized as those employed by the mother or those involving medical provider assistance. A set of thematic findings emerged for both broad categories of strategies and are presented in Tables 3 and 4. These themes represent approaches mothers described as potentially helpful in navigating mother–daughter talk about cancer and disease risk.
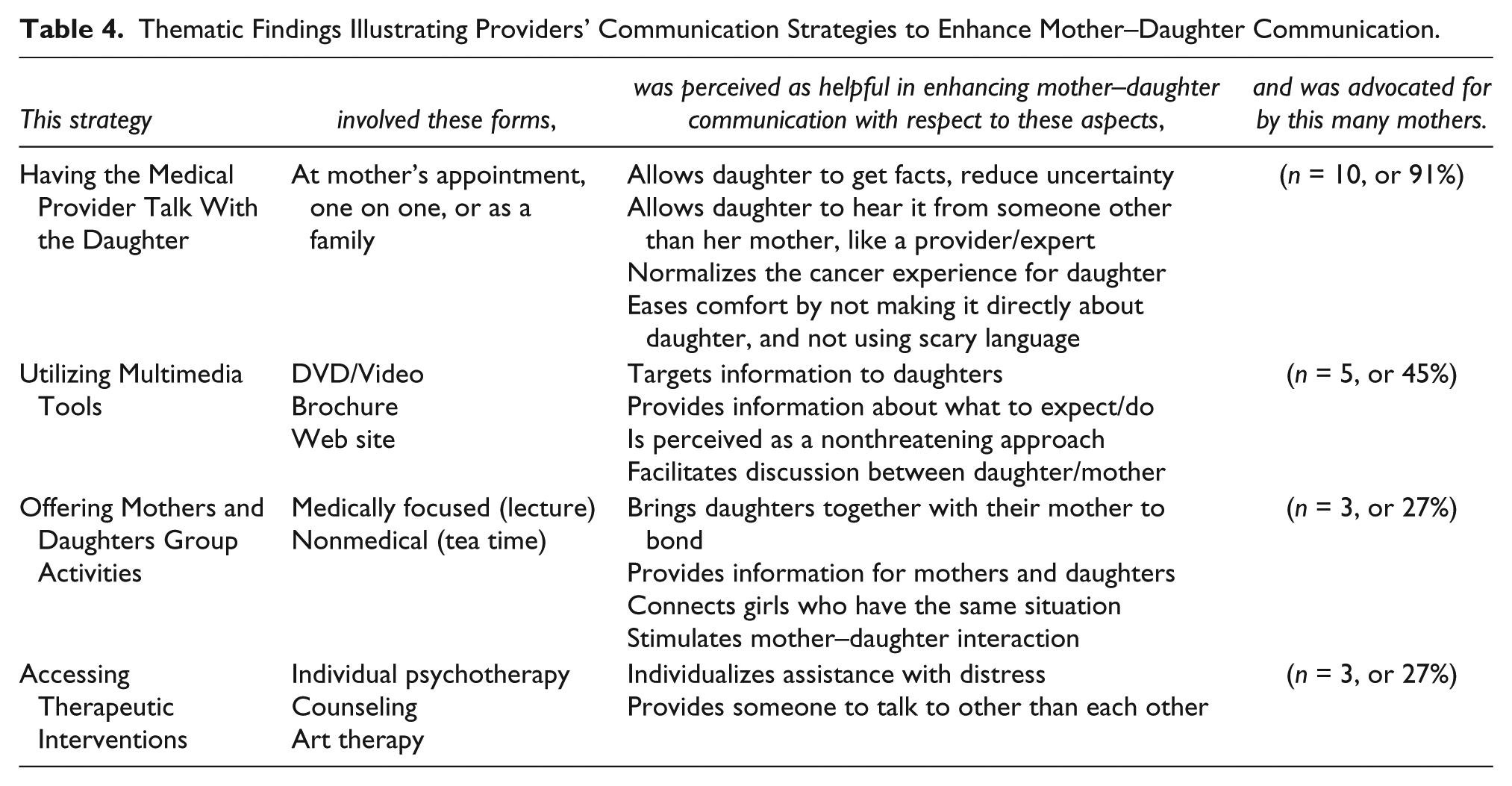
Thematic Findings Illustrating Providers’ Communication Strategies to Enhance Mother–Daughter Communication.
Mothers’ communication strategies to enhance mother–daughter interactions
Mothers described three types of communication strategies that enhanced communication about cancer-related topics. None of these strategies were described as sole approaches; rather, they were used in tandem with other strategies. In our presentation of the findings, we aim to elucidate this complexity.
Engaging in direct communication strategies
More than half of the mothers used direct communication to manage discussions. One direct approach was attributed to a family communication philosophy: “The best policy is always to be open and honest most times.” Some women described learning this approach from friends and loved ones who had experienced something similar. Additionally, several women described the importance of openness. Many referred to growing up with affected parents who did not openly discuss their experience with cancer, parents who emulated societal attitudes decades earlier when one could not say “cancer.” Some mothers describe how being open and honest is healthier:
If you ever tell them a lie, they will never believe you. Inevitably they are gonna overhear you on the phone with somebody at some point. And they’re just gonna think, “I know my mom’s telling me she’s gonna be okay, but I don’t believe her. She’s probably just telling me that.” So they [friends] all strongly encouraged me to make sure I keep clean on the whole thing. . . . In fact, I had other children of other nurses that I work with who were survivors who had very poor prognoses at the beginning. . . . Miraculously they’ve had recurrence and they’re still alive. . . . Their kids said [to me], “Don’t not tell them the truth. My mom—I found out stuff.” And I said, “But you were little. Maybe they were trying to—” [and the kids said], “Yeah, but even though I was little, I knew that there was something wrong. I knew there was something not right.”
They need to see, I think. . . . They need to have to see it.
And that they see you’re okay.
Mothers also used direct questions to facilitate conversations. Mothers perceived this approach as helping them gauge their daughter’s comfort level in discussing issues or when to stop: “Sometimes I’ll just say like, ‘Is this too much for you?’ Do you wanna talk another time?’” Another direct approach was to initiate the conversation; doing so seemed to relate to mothers’ openness, which enhanced the daughter’s comfort level: I think familiarity brings comfort too, if you talk about it, and it’s not so scary anymore. . . . The more those words will come out, the more they have the opportunity to ask some questions. I think it takes away the fear of cancer. . . . I don’t think any kids are ready for any of it until you bring it up most times, and that most times if you bring it up, even if they’re uncomfortable about it, at least it’s opened the door. And when they are ready there will be a discussion about it afterwards. But I think if you, if the parent or someone is the first one to suggest that, it’s okay to talk about.
Some women thought that having initiated discussions of health or illness earlier in life or across the life span was linked to the daughter being more comfortable in discussing a serious diagnosis or risk later on. Mothers also described how it helped girls feel more comfortable discussing their body when it came to issues of breast cancer risk or health promotion.
Another direct strategy mothers used was to offer reassurance to their daughter to ease her concerns or worry. Often this approach emerged when talking about screening or prevention. One mother used different approaches with her two daughters: Well, my [older daughter] . . . is pretty big busted. . . . She just wants to take them off. She’s not gonna take the chance. . . . I said, “Well, I wouldn’t rush to take them off right away. You’re only twenty-one.” . . . For the past two years she still voices that. . . . I’ve spoken to her about breast self-examination and that they’ve said that she really won’t start heavy surveillance until she’s twent-five. But she’s of the thinking she just—she’s gonna be proactive. But that’s personality. She’s pretty aggressive. She probably will remove them. I’m not gene positive, but she probably will remove them. The sixteen-year-old, she’s of a completely different variety. . . . She’s very loving, very much a worrier. I completely downplayed the whole thing with her. . . . I don’t want her to be fearful. . . . I don’t want her to be like, “Oh, you got to cut them off already.” I mean, that’s gonna be a completely personal decision of hers. But I reassured them with the surveillance [it] is gonna be better. Maybe there will even be a blood test to be able to discern this. They’re coming up with new stuff all the time to try to reassure them.
Her recollection highlights what many mothers reiterated: that their choice of approach had to account for daughters’ individual traits and differences (age, personality, avoidance level, and so forth).
Integrating indirect communication strategies
Although less commonly used, mothers did find some indirect communication strategies helpful. Of these, one of the most common was utilizing humor. Humor seemed to help mothers lighten the seriousness of the issue and was also implemented by daughters: “We do use humor a lot in my house. . . . If she wants a ride somewhere now, ‘Why is the laundry piled up? It’s not a chemo week. You should be able to do all these other things.’” Mothers also used humor about themselves in reference to the physical changes they’d encountered. One mother faced a challenge in balancing how much humor to use:
I laugh about mine and make jokes about it, but my kids know that mine look strange. I was radiated on this side. In fact my one breast is—I had both of them reconstructed, but they—one is completely shrunken into nothingness. So, I kid around about it, but I know that they [my kids] don’t. It’s like, “No, Ma. It’s more information than we needed to know.”
Yeah, there is a point where there is enough.
But I always joke about it all the time. I always joke about it.
Yeah, I always joke about it too. Like, oh my sad little breasts there. It looks like it’s all, it’s disappearing [laughs].
This balancing act also emerged when mothers used indirect strategies to downplay the situation. Some women described “sugarcoating” their experience with cancer, particularly if they felt their daughter was too young or distressed. Mothers felt it necessary to “protect” their daughter, although in retrospect, they learned this strategy should not be used in excess, because it could lead to unrealistic assumptions and future expectations for the daughter, as well as guilt:
My daughters were younger. They were eight and eleven. And I remember telling them that Mommy had breast cancer, and my eleven-year-old’s first reaction was, “Are you gonna die?” And I said, “No. I’m very early stage and [have] great doctors.” And I was very positive. Then my eight-year-old said, “Can I go back and watch TV now?” . . . What I found out years later was maybe I sugarcoated everything too much. And my older daughter said the way she took it in was she had to be the perfect daughter, that Mommy couldn’t handle one more thing. And she was always the perfect little girl, while my younger [daughter] was wild. . . . She was just, and she [my older daughter] also said, “Because my sister was so out of it, had no boundaries, I had to be the perfect daughter.” She then later developed anorexia and went into therapy.
The younger one?
This is the older one. The younger one said as she got older she felt very guilty that she didn’t realize how serious breast cancer was. She remembers how angry she was that I wasn’t picking her up from school, that I was always in bed. And she remembered how angry she was and that it wasn’t until she went into therapy that she could work through that guilt.
A few mothers tried another indirect approach. Rather than talking about cancer directly they “found common ground” with their daughter that facilitated bonding. One mother used this approach along with humor: A funny story. . . . I had eight (chemo) treatments and maybe by treatment number six, I had asked my doctor, I said I wanted to try medical marijuana. I said that I thought I earned it. And I was very disappointed that it was little pills. No cookies. My kids had me watching the show Weeds, and they were both college students. And that was their gift to me, to watch while recuperating. So, my daughter, and they were both saying, “Did you get the medical marijuana, Mom?” which was a point of finding common ground. And my daughter did see me while I had taken one of these pills, and you couldn’t cut it up so you couldn’t regulate the dosage of it. And I was so stoned. And I remember walking on Broadway with my daughter, and she was laughing at me. She was like, “Mom, you’re so stoned. You are like bouncing into walls.” And I said, “But I’m happy and I don’t care.” So, at least it was just odd that was our common bond, and that was the best and the only other time that she expressed any interest. You just have to find the common bonds where you can get them.
Paying attention to the daughter’s cues
Mothers also thought they needed to observe their daughter’s behavioral cues to determine her level of willingness to talk. Mothers attended to their daughter’s verbal communication as well as her nonverbal behavior. According to mothers, sometimes daughters would directly state their preferences, such as, “Mom, this is too much.” Women also noted more subtle cues from their daughter; for instance, if their daughter asked questions, this signified to the mother that she wanted to talk.
Similarly, a daughter chose to do a school project based on cancer after never before showing interest. Some daughters asked more general questions about the meaning of words or issues, cues mothers took that they were ready to talk. One mother disclosed how her daughter would lay with her on her chemo days. Her daughter said she needed to so she could take care of her mother if she needed anything. The mother stated, “I feel like she needs to be close to me then.” Another mother said, “I am also aware of her level of anxiety, so I try to keep that in mind.” This mother would ask her daughter direct questions to make sure she was comfortable. Another mother stated that she knew she needed to directly reassure her daughter when she appeared distressed, which she did when “she sits on me and cries.”
Medical providers’ communication strategies to enhance mother–daughter interactions
Our findings revealed four communication strategies that could be used by medical professionals to help facilitate mother–daughter conversations. Mothers volunteered ideas, and suggestions by the moderator are included only if the mother(s) agreed it would be helpful.
Having a medical provider talk to the daughter
A majority of women wanted their daughter to talk to a medical provider. Mothers suggested including a daughter at her appointment so she could speak with the provider if needed. Women thought daughters should talk to a provider alone, and some suggested a family meeting with a provider. Women also expressed that whether or not this strategy was helpful would depend on other factors (e.g., a daughter’s individual needs), and that there was not a “one-size-fits-all” approach:
I almost felt like there could be a little more in terms of [when] one has a daughter, to be more out there in terms of saying, “Well, someone can meet with you and your family.” Like, if someone met with the family as a whole and explained more clearly. Because also when one’s going through it, you’re just not that able to be that clear anyway. But if a girl was immediately brought into it by someone who could very clearly communicate [that] this is what’s going on with your mother. This is what’s gonna be done. You know? We expect to see that hopefully she’ll be fine. This is nothing depending on her age. Like, you would know depending on the developmental level [of the daughter] what to tell a child, what she needs to hear at that point. . . . I think it’s really important for kids to come away with a sense . . . that I can keep coming back and asking questions. So, even if a child sits through a whole session with the doctor and doesn’t say a word, as long as when they went home, they would know that they could ask their parents, whatever came into their mind. I think that would kind of be the ideal goal in a way, to have kids be open enough to say, “Why do you look like this?” or “What about me?” Anything that’s on their mind.
Yeah. So there has to be a sense of like, an open door? And not having time pressure that they have too. . . . This is your one shot. Right.
And you know kids respect the doctor differently than any.
This approach was described as enhancing mothers’ own communication with their daughter in a number of ways. In particular, mothers believed it would give the daughter an opportunity to get “facts” about her health and reduce any uncertainties that her mother could not address. Mothers also wanted daughters to be given information from another source (i.e., not the mother) and especially valued an expert (e.g., provider) speaking with the daughter. In addition, mothers thought that attending the appointment could enhance the daughter’s comfort or, as one mother explained (after her daughter joined her for an appointment), make it “a lot less threatening after she saw people as being real people.” Mothers also provided suggestions to help daughters feel comfortable with this type of interaction, and indicated that it was important that providers not come on “too strong,” not necessarily make it directly about the daughter, to ask them if they had any concerns, and to refrain from using “scary” language.
Utilizing multimedia tools
Multimedia strategies were typically prompted by the provider moderating the discussion but were validated by the participants. Strategies mothers talked about included brochures, Web sites, and videos or interactive DVDs. Women described how such strategies would allow tailored information about what to expect or do to be conveyed in a nonthreatening manner:
A DVD sounds so nonthreatening no matter what type of girl is involved. That would be wonderful.
It’d be helpful. It’d be helpful for me too. I mean, and just to sit there, and watch it with her. . . .
Right, kind of a facilitating discussion.
Right.
Providing mothers and daughters with group activities
Mothers also advocated for group-oriented activities led by medical communities, including medically focused activities (e.g., a medical lecture that mothers and daughters would attend together) and non-cancer-related activities (e.g., mother–daughter tea time). They believed that these activities would serve to bring mothers and daughters together and provide another platform in which they could interact about such issues.
Mothers also stressed that it was imperative for daughters to have some sort of group with other daughters of elevated-/high-risk or diagnosed mothers. This communication strategy seemed especially important when mothers described daughters not wanting to share a mother’s risk or diagnosis with her peers, or when they were concerned that the daughter did not have a large enough support network. A daughter group would help them “feel like they are not alone.” Mothers also explained that various formats for groups would be helpful, because daughters feel differently about interacting in larger vs. smaller group settings:
I think they want to seek out other teens that are going through the same thing as they are, because I’ve had kids express that to me: “I don’t want to talk to a counselor. I want to talk to another kid.” A lot of kids told me that. . . . But what I did was not do a formal group because I think if you say to your teenage daughter, “You know what? We have this group therapy or this teen group.”
Oh, right away they’d be like, “Nahhh.”
So, the way it developed is just. . . . It’s really raising awareness with young women. And having them feel that they’re not alone. So, we had about fifty or sixty girls on this committee this year. . . . Somebody had come and said. “You really should have a therapist here.” And I said that would kill it.
[laughs]
Yeah. I know the therapy is each other, really, and they just talk. And they hear us talking. . . . We put on a fashion show, and when we’re getting ready everybody’s sharing and showing scars. And [saying], “Can you see this?” And they see that we’re all laughing about it. And we’re all here to laugh about it. . . . No one knew each other to start. They usually come with a friend. And by the end after we have the event, they’ve made all these new relationships. So, you don’t even know what they’re really talking about, you know?
I think that’s terrific.
That is terrific.
Yeah.
It’s been an incredible journey. And I usually hear about it from the moms. But I’ve had so many girls write me little emails this week [about] how helpful it’s been. Where it’s opened up a dialogue between a mother and a daughter. . . . [Like] driving to my apartment on Sunday morning, they would be able to talk a little bit. You know when you’re not looking at each other. . . . And that it’s just been helpful because teens think they’re alone.
Who else can understand it better than someone else who is potentially thinking of the same things. What is going to be in my future? Is this like my destiny? You know, my girls assume it is their destiny: “Let me get prepared now.” Where I’m like, “Oh, you really don’t have to really be thinking about it yet.”
But they are. But they are thinking about it.
Yeah. Of course they are. . . . They assume it’s going to happen to them—in my house anyway, because it’s so many of us.
Accessing therapeutic interventions
Although less discussed, mothers did suggest that daughters receive more formalized medical intervention in the form of psychotherapy or art therapy. For daughters who seemed withdrawn or more anxious, this approach seemed especially critical, to encourage daughters to talk to someone about their mother’s cancer and its impact on them. Some thought this offered both mother and daughter a safe place in which they could manage their own independent issues:
I specifically wanted someone who would help me with this issue so that we each had someone that we could rely on to talk about this issue.
So part of the way you handled the communication was actually to bring someone else in.
Right.
Do you talk together about therapy? Or is therapy an off-the-table subject, never discussed?
Umm, sure. But again, with respect for each other’s therapy. . . . She knows this is private. This is between me and my therapist.
Discussion
Previous research has demonstrated that mother–daughter communication about breast cancer can impact both diagnosed women’s and their daughters’ coping ability and health-promotion behaviors. As genetic testing for BRCA1/2 gene mutations becomes more common, women are increasingly seeking genetic counseling. The present study serves as a first step in elucidating how health practitioners can help elevated- and high-risk mothers anticipate challenges that might arise and need to be discussed with their adolescent or young-adult daughters, while guiding them within the context of their family’s unique patterns or dynamics. This type of assistance is critical to both mothers’ and daughters’ abilities to cope, to adopt risk-reducing behaviors, to engage in mother–daughter discussions, and to facilitate healthier coping and health-promotion behavior.
Our findings elucidate mothers’ perspectives of these issues. In doing so, we build on previous research, although the scholarship is notably scarce. For instance, we have identified which topics mothers and daughters at elevated risk might encounter, the complexities of discussing them, and techniques mothers can use to enhance those interactions and manage challenges embedded within these conversations. Findings illustrate the challenges of speaking about these issues and how proactive, flexible, and responsive elevated-risk women must be in managing mother–daughter conversations.
Even though the current study was based on mothers’ experiences, these findings lend support to Wong, Ratner, Gladstone, Davtyan, and Koopman’s (2010) research, which focused on daughters’ perceptions. Together, this body of work can enhance clinicians’ understanding of mother–daughter dynamics. Wong et al. found that adolescent daughters experienced more emotional distress than sons, and those daughters need to feel supported; mothers’ behaviors can influence their perception of support. According to Wong et al., to feel supported by others (e.g., peers) during their parent’s illness, daughters need to feel listened to and understood; to receive encouragement or reassurance; to receive tangible assistance; to be able to talk about cancer and treatment; and to continue to engage in normal life experiences.
Wong et al. (2010) also found that various individual factors influence whether support is perceived as helpful, illustrating the importance of mothers attending to their children’s individuality when navigating these conversations. Our results additionally suggest that children could experience psychosocial effects (e.g., change in self-esteem and/or academic, social, or interpersonal changes). We suggest these changes might be exhibited as cues of distress (described herein), of which mothers should be observant. Our findings suggest that families need assistance navigating these conversations and, at the same time, they offer some guidance for clinicians and mothers on how to do so more effectively.
Implications and Guidance for Mothers
In an effort to facilitate the translation of our findings into health interventions, we provide recommendations to mothers, daughters, practitioners, and scholars, and suggestions for future research. The findings presented herein illuminate ways in which mothers can enhance communication with their daughters and learn to cope with cancer risk in a healthier manner.
We have identified topics that need to be discussed between parent and child as well as strategies that can help facilitate these often trying discussions. We have learned that it is not uncommon for mothers to avoid these discussions. Although avoidance might be helpful in preventing daughters from becoming overwhelmed, it is also widely regarded as an unhealthy coping approach. For families with an elevated cancer risk, avoiding conversations can also silence daughters, increase their fears and concerns, and prevent opportunities for their questions to be answered, thereby reducing the likelihood they will engage in health-promoting behavior.
Discussion is helpful to transmit knowledge about screening and prevention because medical management opportunities exist that were not available to prior generations. As the mothers in our study suggested, earlier generations of parents did not typically initiate discussions about cancer, essentially keeping children in the dark and often leading to distress. Mothers should try to initiate conversations with their daughters. Still, a clear goal is to strike a balance between eliciting daughters’ concerns and imparting knowledge about risk/screening without overwhelming them so much so that they withdraw. Another goal is to help mothers and daughters to find alternative sources of support. Based on our findings, we offer mothers some practical tips.
It is important for mothers to incorporate both direct communicative approaches (e.g., being honest and open or asking questions) and more indirect strategies (e.g., using humor, sugarcoating, or finding common ground). Mothers are in a unique position to provide emotional validation, psychoeducation, and medical information. They might also find it helpful to discuss the paradoxical impact of avoidance to their daughters, explaining that although avoidance is very understandable and helps reduce or prevent distress in the short run, in the long run, it often ends up making a situation more challenging, leading to even greater distress.
Conversations should be a give and take, and daughters should have permission to disclose their concerns to their mothers as needed. Thus, mothers’ ability to listen is also key to children feeling supported (as noted by Wong et al., 2010). Mothers should initiate the conversation and attempt to have multiple interactions over time so that daughters will sense that it is okay to talk about cancer risk and other health-related issues. Doing so can help facilitate a family culture of openness and honesty. It also can allow mothers to stay on top of their daughters’ evolving concerns, which are likely to vary at different developmental stages in their lives. It is important, however, that mothers not overwhelm their daughters by trying to talk about cancer too much or in too personalized a manner, which can invoke fear. Mothers can help mitigate this outcome by incorporating a life outside of cancer into their relationship, even in the face of cancer. Having a life outside of cancer is critical for children to feel supported by their parents, as well as for the diagnosed parent’s well-being (Fisher, 2010, in press; Wong et al.).
It is also critical that mothers be aware of their daughter’s unique traits (i.e., personality, age, developmental maturity, comfort with her body, concurrent experiences in her life other than cancer) and be flexible in their approach. As other research suggests, age or developmental maturity seems to be a particularly important factor in daughters’ distress, and should be considered in how mothers can change their approach in talking about health-promotion behavior and/or screening results (Bradbury et al., 2012; see aslo Fisher, 2010, in press). Mothers should carefully observe their daughter’s verbal and nonverbal cues for markers of distress (e.g., avoidant behavior or expressions of fear/sadness), curiosity (e.g., asking questions sometimes indirectly about cancer-related issues), and comfort level (e.g., showing mother support or avoiding discussions). This observational approach will help mothers determine how much to share and when to bring up these topics, and ensure that daughters are knowledgeable, feel comfortable, and are supported.
Implications and Guidance for Practitioners
The perspectives of these mothers provide guidance for health practitioners who work with increased-risk women and their families, such as genetic counselors, physicians, nurses, and psychotherapists. Our study findings reinforce the sense that experiences of health and disease are familial concerns rather than solely individual experiences. Mothers need an opportunity to voice their concerns about their children, ask questions, and have their uncertainties alleviated. It is important that practitioners consider patients’ concerns for their daughters in their coping and health-promotion strategies.
Women have expressed a desire to talk to health professionals about these concerns and, specifically, about how to discuss this with their daughters. Mothers in our study suggested that practitioners invite their patients’ daughters to attend appointments, with or without their mother, thus including them in the dialogue. Women seemed hungry for opportunities to include their daughters in their cancer screening and/or treatment. They believed doing so would promote their daughters’ comfort and knowledge concerning their mother’s disease or risks as well as their own.
Practitioners and institutions might consider ways to open the door to daughters and other children by including them in appointments, offering activities or events (health-focused or not) that unite parent and child, and help them navigate these conversations while simultaneously learning about health promotion together (e.g., through lectures, videos, brochures, expressive art therapy). In doing this, practitioners will be instrumental in boosting mother–daughter communication at home.
It is worth reiterating mothers’ beliefs that daughters need a place to connect with other daughters. Adolescent and young-adult daughters of elevated-risk mothers are in a phase of life in which identity development is key to their health (La Sorsa & Fodor, 1990). Their growth and struggles with their sense of self will involve their mother’s cancer experience and their own disease risk. As the mothers in our sample disclosed, these daughters might feel very alone or different from other girls their age. It would be advantageous to have a space in which daughters at increased risk can connect with others who share this unique and often emotionally challenging experience. Ways to unite daughters and offer them a culture of support might include a peer-mentoring program (matching daughters whose mothers have similar risk or diagnoses), monthly support group meetings for daughters only, or awareness events in which daughters join together to engage in advocacy or to learn health-promotion skills.
Considerations for Future Research
Even though our findings can help enhance mother–daughter communication and coping, and health-promotion behavior for families at higher risk for cancer, these results also warrant further exploration. Additionally, we have decided to focus on two such issues that emerged, given their complexity and significance for both mothers’ and daughters’ health.
First, women in our study experienced confusion with negative genetic test results, meaning the test showed they were not carriers of the gene mutation. This issue could easily be overlooked by health care providers and patients alike, even though at least one study suggests that parents with negative test results are more likely to communicate those results to their offspring (Bradbury et al., 2012). Negative genetic test results are at times given by a practitioner in group format or by phone (as was the case with this sample of women). This approach could lead to confusion about risks to them and their daughters, thus further complicating mothers’ ability to explain risk to daughters.
Women with confusion could be encouraged to schedule an in-person genetic counseling follow-up appointment with or without their daughter. Often when patients test negative, they are informed that they still have an elevated risk but that this risk is harder to quantify (e.g., it could be tied to untested breast cancer genes and/or risk factors). Moreover, not all women are given empiric numerical risk estimates for their daughter for various reasons (e.g., daughter is too young; it is not a routine part of the session). Hence, it is understandable that negative results can cause confusion.
Future research could aim to improve provider–patient communication about test results. Hypotheses could be tested to gain knowledge to improve procedures of provider–patient communication about test results (e.g., when communicating negative test results, numerical risk estimates for older daughters to develop cancer can be helpful). The impact of children’s ages and family history of cancer on feelings of confusion after a negative test result could be explored. Given differing procedures at various medical institutions, as well as provider time constraints, more research should examine how variant health practices might better alleviate patients’ confusion.
A second issue that emerged of particular concern is mothers looking to their daughters for support. This is not uncommon. Research does show that mothers lean on their daughters for emotional, instrumental, and informational support when diagnosed with cancer (e.g., Fisher, 2010, in press). Nevertheless, for younger daughters, this could be a stressor that compounds their distress. Because of their age, daughters might also be less emotionally mature than their mothers, and thus less able to cope with the emotional stress associated with disease and risk.
Previous research does indicate that younger daughters (late adolescence or emerging adulthood, ages 15 to 25) sometimes respond to their mothers’ desires to talk about the disease experience by withdrawing and avoiding (see Fisher, 2010, in press). This dynamic is indicative of the daughter’s distress and poor coping and, in turn, could inhibit the mother’s well-being (given her heightened concern for her daughter). At the same time, it can create discord in the bond. Daughters can mirror their mothers in psychological and physiological distress associated with disease (see Cohen & Pollack, 2005). Given this connection, when mothers seek support from their daughters before they are developmentally ready to serve in this maternal role, daughters’ mental and physical health might be negatively impacted.
Future research should examine the impact on daughters’ coping behavior and quality of life when mothers seek their support, so we can better advise mothers about this issue. Researchers should also aim to capture the voices of the daughters to enhance our understanding of their coping needs. It might be especially prudent for scholars to utilize a critical approach to explore these issues, one that considers the gendered expectations of women and how that might be burdensome to both mothers and daughters.
Given this reaction, it is important for practitioners to advise mothers to consider their daughter’s emotional stability prior to seeking her support and assess whether they are looking to their daughter as a primary source of support. Mothers should be encouraged to seek independent means of support, such as family, friends, therapy, social work, support groups, or online resources. Support groups created through genetic counseling services can be particularly helpful. Some mothers might need to be reminded that their diagnosis is not only personally challenging but difficult for their daughters. Thus, identifying independent sources of support for their daughters (e.g., a counselor, peer groups) could be beneficial as well.
Limitations
Findings from this study are limited by the fact that this sample of women was small. The sample was also homogenous in ethnicity and socioeconomic status, and findings are thus not necessarily generalizable to a larger public. In addition, most of these women had already experienced a cancer diagnosis (with varying treatment trajectories), and two mothers had genetic mutations. The challenges in their mother–daughter interactions were inevitably influenced by such disease and risk factors. Our findings were limited to the mothers’ perspectives. Although mothers and daughters often mirror one another, they might also differ, further complicating their interactions. Daughters also need a voice.
Our primary concern was to heighten our appreciation and understanding of the unique needs of mothers and daughters of elevated cancer risk. Further attention should also be given to researching other familial bonds, such as those among multiple children or with husbands/fathers, and how their communication impacts the family’s ability to cope with cancer more collectively or communally. In sum, findings from this study provide preliminary insight into the complexities of mother–daughter communication about elevated familial breast cancer risk and, we hope, aids families, practitioners, and scholars in navigating these difficult conversations while attending to both mothers’ and daughters’ sense of well-being.
Footnotes
Authors’ Note
Portions of this article were presented at the American Psychosocial Oncology Society Conference, February 2012, in Miami, Florida, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from Oki Data Americas, which is gratefully acknowledged.