
Abstract
In this study, we investigate the subjective experience of a group of individuals, diagnosed with schizophrenia, undergoing outpatient treatment in four psychiatric clinics in Mexico City. Our objective is to use the paradigm of intersectionality to explore the most common forms of stigma and discrimination faced by people with this illness, as well as the coping resources they employ. The major contribution of this study is its use of in-depth interviews and thematic analysis of the information obtained to identify the importance of sociocultural aspects of participants’ experience of their illness. Schizophrenia, for them, was a problem of “nerves,” whose origins were linked to magical or religious elements they attributed to their illness and which influenced their response to it. This resignification was useful to participants as a coping resource; it helped them find meaning and significance in their experience of the illness.
Keywords
Schizophrenia is one of the serious mental disorders with the greatest disabling effects on the population, affecting an estimated 24 million persons worldwide (World Health Organization [WHO], 2001). Although it has a lower prevalence than depression, affective disorders, and substance abuse, the 2010 Global Burden of Disease Study showed that acute schizophrenia generates a greater level of individual disability than these other conditions (Whiteford et al., 2013). In Mexico, its prevalence in the general adult population varies between 1% and 2% (Medina-Mora et al., 2003) and, although it is the most frequently treated diagnosis (26%) in psychiatric hospitals (WHO, 2011), it is estimated that only one in five persons receives specialized care (Valencia, Díaz, & Juárez, 2012).
One of the major implications of this illness for those affected is social exclusion, which is the product of a series of structural and individual factors that work together to affect an individual’s subjective experience, giving rise to the internalization of social prejudice linked to psychiatric and pharmacological treatment (Corrigan & Watson, 2002). These internalized beliefs cause suffering in the majority of patients. They make enormous efforts to hide their illness and attempt to preempt discrimination by avoiding social contact (Link, Mirotznik, & Cullen, 1991), which constitutes a barrier to seeking care (Angermeyer, Beck, Dietriech, & Holzinger, 2004) and impedes treatment adherence (Fung, Tsang, & Corrigan, 2008).
It is now recognized that stigmatization and discrimination related to mental illness are a worldwide problem (Stuart, Arboleda-Florez, & Sartorius, 2012), and this recognition has generated an increased interest in research. One study reports that 9,939 articles in the PsycINFO database published between 1967 and 2012 have “stigma” as a keyword (Bos, Pryor, Reeder, & Stutterheim, 2013); of these, 4,278 were published between 2000 and 2005 (Mak, Poon, Pun, & Cheung, 2007). A large part of this output comes from medical and psychological research in Western countries and, to a lesser extent, from Latin America (Mora-Rios, Natera, Bautista-Aguilar, & Ortega-Ortega, 2013a, 2013b; Valdivieso, 2004).
Various studies have limited themselves to analyzing the phenomenon from an individual perspective; although these have made interesting contributions toward reducing the implications of stigma surrounding mental illness (Corrigan & Watson, 2002), they are limited in their focus on the individual experience of illness and the meaning attributed to it, and their lack of attention to the sociocultural context of these processes. The exclusion of those with mental illness is a social problem more than an individual one; it is public policy that stands in the way of social reintegration of persons with schizophrenia (Saraceno, 2003).
In the specific context of Latin America, stigma associated with mental illness is linked to questions of social justice and a history of exclusion and violence in the lives of the persons affected (Correa, Silva, Belloc, & Martínez, 2006; Martínez-Hernáez, 2009). Recovering their experience, through narratives that describe social and health systems founded in inequality (Amarante, 2007), is critical to a comprehensive understanding of the phenomenon. It cannot be reduced to a discourse of disease and nosology that lies outside the context of the individual’s daily life.
Along the same lines, Link and Phelan (2001) emphasized the importance of sociocultural context and macro-social variables that explain structural stigma to fully describe the stigmatization process. One such factor is gender, whose importance has been amply documented in mental health research (Scheyett & McCarthy, 2006), notably in studies by Nasser, Walders, and Jenkins (2002) and Jenkins and Carpenter-Song (2009) on the impact of schizophrenia on identity and gender roles, for which evidence has also been found in other sociocultural contexts. For example, Sajatovic, Jenkins, Strauss, Butt, and Carpenter (2005) reported gender differences in a group of 90 persons diagnosed with schizophrenia and undergoing outpatient treatment in two communities’ mental health centers in the United States. Men experienced greater difficulties in fulfilling their traditional role as economic provider while the social demands on women devoted to housework and child care were less. Similar findings have recently been reported in India (Loganathan & Murthy, 2011).
Other gender differences are seen in the ways in which people seek care. Women tend to have more favorable attitudes toward mental health services, seek help earlier, and even experience fewer relapses than men (Sajatovic et al., 2005; Vogel, Wester, Hammer, & Downing-Matibag, 2013). Gender also interacts with other social conditions on multiple levels, including race, ethnicity, inequality, immigrant status, social violence, and insecurity, which together generate an effect of social vulnerability and produce inequalities in health. The paradigm of intersectionality (Crenshaw, 1994), proposed in the field of women’s health, has been highly useful in understanding the interplay between systems of power and oppression on the structural level (Hankivsky et al., 2010).
In the case of serious mental disorders like schizophrenia, the work on immigrants by Collins, von Unger, and Armbrister (2008) showed how social determinants, including gender, have an influence on processes of exclusion that can also occur in other groups, such as people living on the street or in prisons. Qualitative studies have also found that women with serious mental disorders are more likely to be substance abusers (Borba et al., 2011) or victims of physical or sexual violence (Chernomas, Clarke, & Chisholm, 2000; Loganathan & Murthy, 2011); homeless women’s risk associated with victimization and trauma is double that for men (Wenzel, Koegel, & Gelberg, 2000). These women experience conditions of social vulnerability, which translates into greater difficulty with access to health services; they are left on the margins of programs that exclude them as a matter of public policy, which some authors identify as structural discrimination (Link & Phelan, 2001).
Nowadays, it is recognized that there are diverse sources of stigma and discrimination that originate in different parts of society: in the family, in educational institutions, and in the workplace, as well as in the persons affected by mental illness themselves, who can exhibit rejection toward others and even toward themselves in the form of internalized stigma (Corrigan & Watson, 2002). Chernomas et al. (2000) analyzed experience and perception relative to their illness in a group of women diagnosed with schizophrenia at different stages of their lives; they find that the secrecy surrounding the illness produces feelings of worthlessness and social inadequacy, described by the women as an overwhelming sensation of loneliness and isolation.
Authors like Pitt, Kilbride, Welford, Nothard, and Morrison (2009) highlighted the contradictory impact of the diagnosis: Although schizophrenia is a stigmatizing label, it also represents for the patient a means of naming the problem. Not all patients diagnosed with schizophrenia report being objects of stigma or discrimination related to their illness (Corrigan, Rafacz, & Rüsch, 2011). Those who have had such experiences develop strategies for dealing with the negative consequences, which has led to a line of investigation concerned with coping resources (Miller & Kaiser, 2001; Oyserman & Swim, 2001). Corrigan and Watson (2002), for example, identified a set of intermediary variables that influence the process of stigma internalization; they describe a “paradox of self stigma and mental illness” that arises from the tendency of individuals to apply negative stereotypes of their illness to themselves and isolate themselves from others to avoid rejection. Other individuals act with indifference, and still others react with anger against what they consider to be a violation of their rights, which leads them to active participation in defense of those with similar illnesses.
Because of the importance of the resources used to cope with the stigma and discrimination associated with schizophrenia, in recent years, there has been increased interest in qualitative research to identify positive factors in the experience of affected persons. Cardano (2010) identified such factors in a psychiatric population, linked to informants’ experiences, which represent a kind of education and personal growth. Some individuals, for example, seek alternative identities beyond their illness, characterizing it as something positive, a kind of “gift.” Shih (2004) noted that in focusing on the negative consequences of schizophrenia, research has neglected the ways in which individuals generate positive resources—like compensation, for example, through which they apply interpretations to their illness that go beyond a label as merely “sick”—that are linked to their resilience and empowerment. These issues have not received sufficient attention from researchers (Veseth, Binder, Borg, & Davidson, 2012).
Another issue needing further attention is sociocultural variation related to mental illness, which is fundamental to understanding processes of exclusion and their modes of expression among the population of Latin America. Research has thoroughly demonstrated how los nervios (“nerves”) is an expression frequently employed by rural and urban residents to interpret and ascribe meaning to their emotional problems (Castillo, 1996; López & Guarnaccia, 2000; Mora-Rios, Medina-Mora, Ito-Sugiyama, & Natera, 2008; Traverso-Yépez & de Medeiros, 2005). More recently, in a comparative cross-cultural study of psychiatric populations, Carpenter-Song et al. (2010) found that, in contrast with participants from other parts of the world, Latin Americans generally refer to such problems as a “disease of the nerves”; the authors interpret this term as a form of cultural resistance to medical diagnosis, one which could be a way of reducing the stigma of mental illness and which they propose for further exploration in research on sociocultural aspects of such illness.
The specific sociocultural context of Mexico is one of great social, cultural, and economic diversity, where social inequality is one of the major problems. According to official figures, in 2012, 45.5% of the population lived in conditions of poverty (Consejo Nacional de Evaluación de la Política de Desarrollo Social [CONEVAL], 2013). In the area of health care, a significant proportion of the population (34%) lacks social security (Instituto Nacional de Estadística y Geografía [INEGI], 2010) and relies on a variety of strategies to obtain medical attention, from the use of private services to alternative medicine, which at times includes magic or religious elements.
In this qualitative study, we investigate the subjective experience of a group of individuals undergoing outpatient treatment for a diagnosis of schizophrenia in Mexico City, with attention to the most common forms and manifestations of stigma and discrimination related to their illness, as well as the resources they employ to cope with such experiences. To provide a more comprehensive understanding of the processes of social exclusion, we incorporate into the analysis the paradigm of intersectionality (Crenshaw, 1994; Hankivsky et al., 2010).
Method
This study is part of a larger cross-cultural project conducted by research teams from Canada and Mexico, whose purpose is to investigate the processes of stigmatization of mental illness in different groups of the population (e.g., patients, family members, health care workers, and the general population), with the aim of proposing measures to reduce that stigma (Pedersen, 2009). The research received ethics clearance from the Bioethics Committee of the Ramón de la Fuente Muñiz National Institute of Psychiatry (EP09 4225.0). This institution’s guidelines provide that information obtained during research projects must be protected by the researchers involved for 5 years and subsequently destroyed. The names of participants, health centers, and other institutions were changed at the time the information was registered to guarantee participants’ anonymity.
The study was carried out with outpatients from four psychiatric care centers in Mexico City, from January 2009 to July 2010. A purposive subsample was selected of 23 persons with a diagnosis of schizophrenia.
Recruitment
We employed a variety of strategies to recruit subjects at least 18 years of age who met the following criteria: (a) diagnosis of schizophrenia according to the guidelines of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2003) and the International Classification of Diseases (ICD-10; World Health Organization, 2010), (b) undergoing outpatient treatment incorporated into their daily activity, (c) clinical stability sufficient to provide informed consent and participate in interviews. One strategy used treating physicians who, guided by these criteria, facilitated contact between potential subjects and the research team. An interviewer described the general objectives of the study and invited the potential subject to participate, emphasizing that the study activity was wholly independent of the medical care provided at the institution.
Another strategy was to issue general invitations to participants in orientation or psychoeducation courses in the same care centers. Members of the research team would explain the objectives of the study and collect telephone numbers of interested persons who met the inclusion criteria; these were contacted later to schedule interviews.
Of the 25 participants, two later decided not to continue for lack of time; the rest completed the study. In general, study subjects showed interest in participating: not only was the topic of interest but the study also represented an opportunity for them to be heard, which is not often the case in other contexts.
Participants
The informants included 12 women and 11 men from 22 to 63 years of age (average 40 years), with 2 to 27 years since the onset of illness. Of these, 10 received exclusively pharmacological treatment, and the rest also participated in institutional programs including psychoeducational courses, occupational therapy, and support groups, complemented with other resources such as exercise programs, crafts workshops, and alternative medicine.
With respect to other sociodemographic characteristics, 21 participants lived with their family at the time of interview (mainly with parents and siblings), 19 were single, and 3 had children. Ten had an educational level between high school and graduate study, and 11 (4 women and 7 men) were employed, mainly in informal occupations (e.g., shop assistant, self-employment, sale of handicrafts) from which they received limited income. Five participants had social security to support their treatment; one, who worked in a cafeteria and read tarot cards, was the family breadwinner.
Data Collection
We carried out in-depth interviews, based on an interview guide that explored the subjects’ experience surrounding their illness and whether they believed they had been treated differently or rejected because of their schizophrenia. With the aim of retrieving the subjective experience of the users during the in-depth interview, we included an initial section on their personal histories to introduce and contextualize the respondents. This allowed them to convey their experience and retrospectively locate the significant events that had an impact on them, whether or not they were linked to the illness. The strategy employed was to ask open questions. For example, questions like “When did the illness begin?” “When did you seek treatment?” and “What happened during your first search for help?” enabled them to freely express their point of view of the subjects addressed in the interview. To approach the specific subjects of stigma and discrimination, we asked, “Have you at any time experienced rejection or been treated in a way that you considered unfair or inappropriate because of your illness?” We also questioned participants about their trajectories seeking care, their resources for coping with stigma and discrimination, and their suggestions for reducing stigma.
Interviews took place at participating institutions in spaces that guaranteed interviewees the opportunity to express themselves freely. The average duration was 2 hours; some interviews took place over more than one session. Around 90% of participants had been in treatment for more than 2 years. None were unstable, so the duration of the interview was not an obstacle. Participants were thankful for having their point of view considered as the topic was important to them. We made audio recordings of all interviews and then transcribed and reviewed them. Interviews were conducted by the first author, three psychologists, and one anthropologist, all of whom had previous experience in interview techniques and who were given additional training in handling the interview for this specific population. The emphasis throughout the study process was to place the well-being of the participants over the need for the interviews.
Data Analysis and Interpretation
The interview team participated in the transcription, review, and analysis of the interviews. We carried out a thematic analysis, using an inductive method with procedures based on grounded theory (Strauss & Corbin, 1990). This is a method useful to the exploration of the subjective experience; it seeks to gain an insider perspective while recognizing the role of the researcher as an interpreter in making sense of another person’s experiences. The analytical process began with individual review of each of the interviews by members of the team, followed by open coding of the contents, which allowed the development of a coding guide that could be modified throughout the analysis as we incorporated new information. Members of the research team coded interviews individually and later established categories by group consensus. This was not always an easy task, owing to the interrelatedness of categories: It was difficult to differentiate clearly whether certain responses referred to the impact of stigma or coping resources, or to other dimensions of subjective experience. Such problems were resolved by considering the general context of the interview to decide on the appropriate category. We also used constant comparison, memo writing, selection of core categories, and model building. ATLAS.ti software, version 6.2.23 (Cincom System, 2011) was used to organize the information.
Results
The thematic analysis showed three categories emerging from the accounts of the interviewees: (a) cultural factors: meaning and attribution surrounding schizophrenia, (b) manifestations and forms of stigma and discrimination, and (c) resources for coping with stigma, particularly regarding resistance to stigma, including the resignification of the experience of disease. As our analysis shows, gender emerges as a persistent category in the subjective experience of the participants.
Cultural Factors, Meaning, and Attribution Surrounding Schizophrenia
Although some interviewees reported feeling reassured on receiving the news of their diagnosis, because it at last provided a medical explanation for their problems, the majority described a significant emotional impact that included feelings of fear, shame, desperation, anxiety, and worry that it could interfere with their plans and personal projects:
I was very scared—to have such a fundamental psychiatric illness—I said, “no, maybe I’m just here for an emotional problem.”
Of the 23 study participants, 17 reported having doubts about their medical diagnosis, and a majority had a tendency to find a meaning in the experience (e.g., “Why me? Why is this happening to me?”). They also experienced a series of dilemmas about the implications of their illness: about medication, for example, or about whether to tell others about their diagnosis.
All participants described being informed of the psychiatric diagnosis as initiating a period of great vulnerability; they experienced a certain loss of identity and social status, a set of disadvantages with respect to the plans and achievements of others. Some described it as a crisis, others as “living in a separate world” or being “out of place,” which produced distress at feeling abandoned, feeling lonely, having a “feeling of emptiness,” feeling forced into isolation to avoid rejection, and having to make an enormous effort to prevent others from finding out about their illness.
A process of comparison can be seen between what is considered socially normal or abnormal (the separation between us and them) based on criteria like physical appearance; ways of reacting or behaving; achievement in sports, work, and school; intellectual capability; and lifestyle. This process is evident in the testimony of an informant:
I didn’t believe it at first, you know? It just seemed to me that to say “schizophrenia” was too much, to talk about a mental illness, because, I said, I don’t have anything wrong with my mind. I said, I can walk, I can talk, I can move, I can . . . I mean, I saw that I could do almost all the things I did, almost all the things that I could normally do, and that this, no, no, no, I don’t know, I mean, I saw it as if it were a kind of getting drunk, and that afterwards they had told me, aha, you’re a mental case. And I said, aren’t there guys who do crazier things than me? Why, if they’re drunks, they’re alcoholics [smiles], and I don’t do those things. So it seemed to me too much to accept that I had a mental illness. (Man)
Participants attributed the origin of their illness to various reasons, both internal (character, lifestyle) and external (experience of neglect and mistreatment, loss of employment, witchcraft, blows to the head, inheritance, and genetic causes). It is worth noting that there was a disconnect between medical interpretations (psychiatric diagnosis) and the meaning participants ascribed to their experience: There was a general tendency to define their illness as “a problem of nerves,” as an “emotional problem,” or as depression, which for them served as a resource that imparted more sense to the experience. It also made it easier to share information with others about their disease, as shown in comments like “I had told them that I was sick with nerves and not with schizophrenia” and “I started to lose weight because of my nerves.”
Sociocultural factors and gender also come through in the narratives: While women attributed their illness to witchcraft and disappointment in love, men talked about alcohol and drug abuse that unleashed delirious episodes, as well as work-related stress, which put them in a difficult situation of personal and economic instability, and threatened their social identity as providers.
And then when I was 16, my grandfather died and the problems started because I was doing mushrooms and marijuana, and that’s when I got sick, and they started to . . . I started to get delirious, but it turned out that I never got better. (Man) No, well, I thought [it was witchcraft] because the people who, there were some people I didn’t get along with. . . . But I felt it like it was the cause of being exposed to someone, without knowing who, that I had eaten something or they had given me something or something like that. (Woman)
One of the major themes we identified in the narratives of the participants was the implications of their illness on their plans and personal projects, particularly with respect to relationships and forming a family. Some of them considered that these experiences were not accessible to them; they asked themselves “What could I offer him/her?” There were those who internalized negative stereotypes about the illness and saw themselves as discredited or less desirable to others. The following examples show the impact of these beliefs on interviewees:
Now that I am sick, I don’t even think about having a relationship. Who’s going to want someone who’s sick? It wouldn’t be fair, it would be a burden for him, because he’d have to be looking after me all the time. . . . So I stopped thinking about it, I said, if I’m sick, no, it would make it even more difficult to have a family, children. How would I raise them if I’m sick? It seems complicated. Besides, all of that is stressful and could be a little dangerous for me. (Woman) I don’t have enough initiative to look for a permanent, stable relationship, or even to go out, like a lot of people do, to pick someone up. I’ve never been like that, much less now. (Man)
Gender as a socially constructed category was expressed through the subjective experience of the interviewees. Becoming a father and forming a family was one of the major desires of the men while women showed greater resignation, considering maternity to be an unattainable experience, in what may be a product of advice they have received in the course of their medical care. In both cases, religious considerations played an important role in ascribing meaning to these experiences, as can be seen in the following examples:
Yes I want to have children, but God hasn’t sent them to me. . . . Because the doctors always told me not to have children, that they would turn out the same as me, not to have children, that it would be better to have surgery so I wouldn’t have them, what would I do with a child, with my illness, and the child could have the same illness. . . . That’s the kind of advice they give me. (Woman) . . . that is my main plan, to fulfill my desire, it’s the only thing I ask of God, to get better and be able to reestablish myself in society and have my children. (Man)
Experiences of Stigma and Structural Discrimination
Of the 23 persons interviewed, 19 reported having been the object of stigma or discrimination on account of their illness. There were only four cases, 3 men and 1 woman, who said they had not experienced rejection. The main sources of stigma were the family (both nuclear and extended), health care workers, public legal and recreational institutions, and friends. We identified three types of rejection and discrimination toward participants, which we describe below:
Symbolic violence
This category includes mention of nonverbal practices that express rejection, either as indifference, well-established distance, or emotional barriers intended to avoid contact. Asked directly whether he had experienced rejection related to his illness, one interviewee responded that in his first contact with the psychiatric care center he perceived an indifferent attitude on the part of providers, an attitude that changed over time as he became more stable and began outpatient visits. A second participant provided a different example of perceived emotional distance maintained by people in general:
I’ve had doctors who didn’t talk to me before, or pretended not to see me, and now they say hello to me. (Man) I’ve tried to strike up conversations with people outside my family. They treat me well at first, but later they put up a barrier, they stigmatize the schizophrenic. Society still has a lot of prejudices about this disease. (Man)
Infantilization
Under this heading, we include attitudes and actions cited by participants that have a tone of cordiality or goodwill, but that tend to diminish the biological age of the person. The following examples show how these practices were reproduced in different situations: in health care, in a family context, and even in the subjects themselves, contributing to their marginalization and invisibility.
So it’s like I’m an innocent child, my brother sometimes tells me I behave like a child, and it’s true, if he’s the one who knows if I behave or don’t behave, that makes me a child, like he says. (Man) I have a classmate who calls me amiguito (“little friend”), and I don’t like it—it’s as if I were inferior, an intellectually inferior. (Man)
In general, in Mexico, conditions of social inequality constitute structural barriers that affect the opportunities of the population regarding jobs, housing, education, health, and income. These obstacles were even greater for those interviewed and kept them in conditions of economic and emotional dependence on their family members, contributing to their sense of infantilization. According to one participant,
There’s a feeling that I’m not fully adult, since I can’t rent a room, even a modest one, because it wouldn’t be certain that I could pay the rent and live independent of my family. (Man)
Provocation and violence related to gender
Provocation consists of carrying out a series of actions that seek to intimidate, through mocking and verbal or physical aggression toward persons with schizophrenia. Being described as loca (“crazy”) was one of the actions most often cited by women; in Spanish, this is a term with gender connotations, associated with sexual promiscuity and lack of self-control. In women, it produced emotions of anger, rage, impotence, sadness, and disappointment. The following narratives illustrate a certain naturalization of gender violence that female participants experienced on a daily basis. It would seem that the label loca, as socially understood, is attributed to women as a gender characteristic, which produced an emotional response in them of rage and defenselessness:
[Referring to a friend] I told him not to call me that again—because one day he was calling me crazy, crazy, crazy. I said you can call me hunchback—I have a hunchback because they damaged my spine—but that’s it, don’t call me crazy ever again, because I won’t put up with that. (Woman) My neighbors used to say “she’s crazy,” they called me crazy. In fact a lot of times when I would fight with them they would say “you’re crazy,” and we would grab each other [but I felt] really—what’s the word?—really defenseless. (Woman)
However, when male interviewees described being called names such as loco (the grammatically masculine form for “crazy”), some reported responding with physical and verbal aggression, but the most common reaction described was self-protective, an attempt to understand the verbal attacker to avoid an escalation of violence with someone who did not interest them. In the following narrative, a participant explained that one of the causes of his brother’s violent behavior was the hegemonic masculine role that is common in Mexico.
Before, when my brother lived with us, he was very aggressive. If I was feeling paranoia or isolation, he wouldn’t leave me alone, you know? I mean, he was completely ignorant, and he’s a Mexican macho, and they believe violence resolves everything, you know? . . . I don’t know why. . . . It’s that he looks at me strange, you know? He looks at me with my strange attitudes, and his ignorance. He’s crazy. One time we fought and he twisted my arm. (Man)
Intersectionality of stigmas and social vulnerability
In our analysis of their life histories and the context in which participants described their experiences of stigma and discrimination, we found men and women in different conditions of social vulnerability. These were manifested not only in the existence of physical or mental illnesses affecting participants and their families but also in their immediate surroundings, in the difficult conditions of their lives, and in their experiences of mistreatment, neglect, and sexual abuse. Of the 23 informants, 14 reported chronic illness in members of their immediate families, mainly parents and siblings: physical conditions such as diabetes, high blood pressure, paralysis, cancer, and skin diseases; and mental conditions such as schizophrenia, depression, Alzheimer’s, intellectual disability, and bipolar disorder. Their vulnerability had to do with their limited economic resources for medical attention (food, medicine, caregivers), which often generated catastrophic expenses, given their precarious income. Twelve interviewees depended economically on their families; those who reported having their own income had precarious employment with no benefits.
It’s very difficult for my mom, because I already have a brother with a mental disability, so if you add on another problem like my getting sick, well, it’s an economic problem, because the medicine is expensive, you know? And they’re paying for it, you know? They have to take care of my brother and then take care of me too. It has put a real burden on them. (Woman) What’s happened since I was born, it’s nothing but problems with my mom, who my dad used to beat. And he didn’t give her anything for groceries, he spent it all on drink. . . . And my brothers and I are sick, my father drank, he drank a lot. It’s in our blood, that’s why we’re sick. (Man)
There are also other social determinants that enter into the process of stigmatization: The naturalization of gender violence, which is aimed particularly at women, was seen in the narratives. Four of the women interviewed referred to having been sexually abused and were victimized a second time when they tried to report these experiences; as persons with a mental illness, they were discredited and dismissed:
When I was little, my brother-in-law and then my nephew tried to rape me. So when my friend said she had been abused, I said no, it was true, because it happened to me. So why did I keep quiet? Because if they didn’t believe me before, when I was little, when I was ok, so to speak, they’re not going to believe me now. That’s why, it’s really not right, but the social worker said it wasn’t true, that the girl made it up because of her illness. But no—because it happened to me, and I felt dirty all over again. (Woman)
As can be seen, discriminatory practices also come from psychiatric care workers. In this account, the social worker considered the woman’s description of abuse to be part of a delusion and invalidated her experience. Situations like these can contribute to double or triple discrimination in the treatment process.
Along these same lines, we identified practices in care perceived as inappropriate by participants. The following narratives show structural stigma at the institutional level during their trajectories of care. One of them compared the care received from personnel in two different services of the institution where he received treatment:
I’ve gotten to know different doctors and different ways of dealing with patients, and here it’s a lot better. It’s not so—what’s the word?—so patronizing. There they really spoil you, they called you enfermito (“little patient”), but here they don’t . . . Here it’s more demanding. It’s “Yes, you have schizophrenia, but we are dealing with the emotional, mental, and psychological aspects of your disease.” (Man)
The word enfermito in the Mexican sociocultural context is used often by health personnel. Some consider it proper to be overprotective with patients and maintain them in a passive role. The use of diminutive expressions implies a diminishing of biological age, which makes patients feel uneasy and uncomfortable. Another interviewee described the apathetic, uninterested attitude he perceived in family members and health care workers:
I see a certain attitude of conformism in everyone around the patient, including the doctor, because no one wants to see drastic changes in the patient. They want everything on an even keel, that you haven’t slept either too much or too little. It’s like they’re saying “It’s fine, keep taking the same medication every day so many times a day,” and if it were up to them, they would keep you on it forever. . . . It’s as if they’re saying, as long as you don’t give us any problems everything’s fine, as if nothing more could be expected of someone than that they don’t cause problems, as if they’re satisfied that you keep yourself under control. (Man)
There is evidence that these practices come not only from health care organizations but also from government agencies, as shown in the narratives of two women. One of these was prevented from using public recreational facilities and the other was denied legal assistance in problems with her neighbors. Both cases illustrate that discrimination against persons with psychiatric illness goes beyond considerations of gender. It involves violation of individual rights that can come even from institutions that supposedly provide social and legal support.
A while ago I had to go to that family violence agency, and it was the same as with the women’s agency, no support. I didn’t want to tell them, but they ask, “Do you have any disabilities?” I told them, yes, actually, this is my disability, and they tell me, “Oh, it must have started with that, it’s all because of your illness, so we can’t help you.” (Woman)
Stigma and discrimination toward persons with mental illness come from every part of society, including the media, which were identified as one of the major sources behind the social exclusion not only of persons with schizophrenia but of others as well. This section has analyzed some of the conditions of multiple vulnerability in this population, with women and men sharing experiences of violation of their rights through exclusion from education, employment, recreation, and social life on account of their illness.
Resources for Coping With Stigma and Discrimination
Interviewees described a variety of responses to experiences of stigma and discrimination; These were part of a dynamic process that varied from one individual to another, depending on their particular circumstances (such as the availability of social support networks, as well as individual characteristics and agency). Table 1 describes these resources. In general terms, two broad interrelated categories emerged: (a) tolerance and (b) resistance to stigma.
Coping Resources for Stigma in Persons Diagnosed With Schizophrenia.
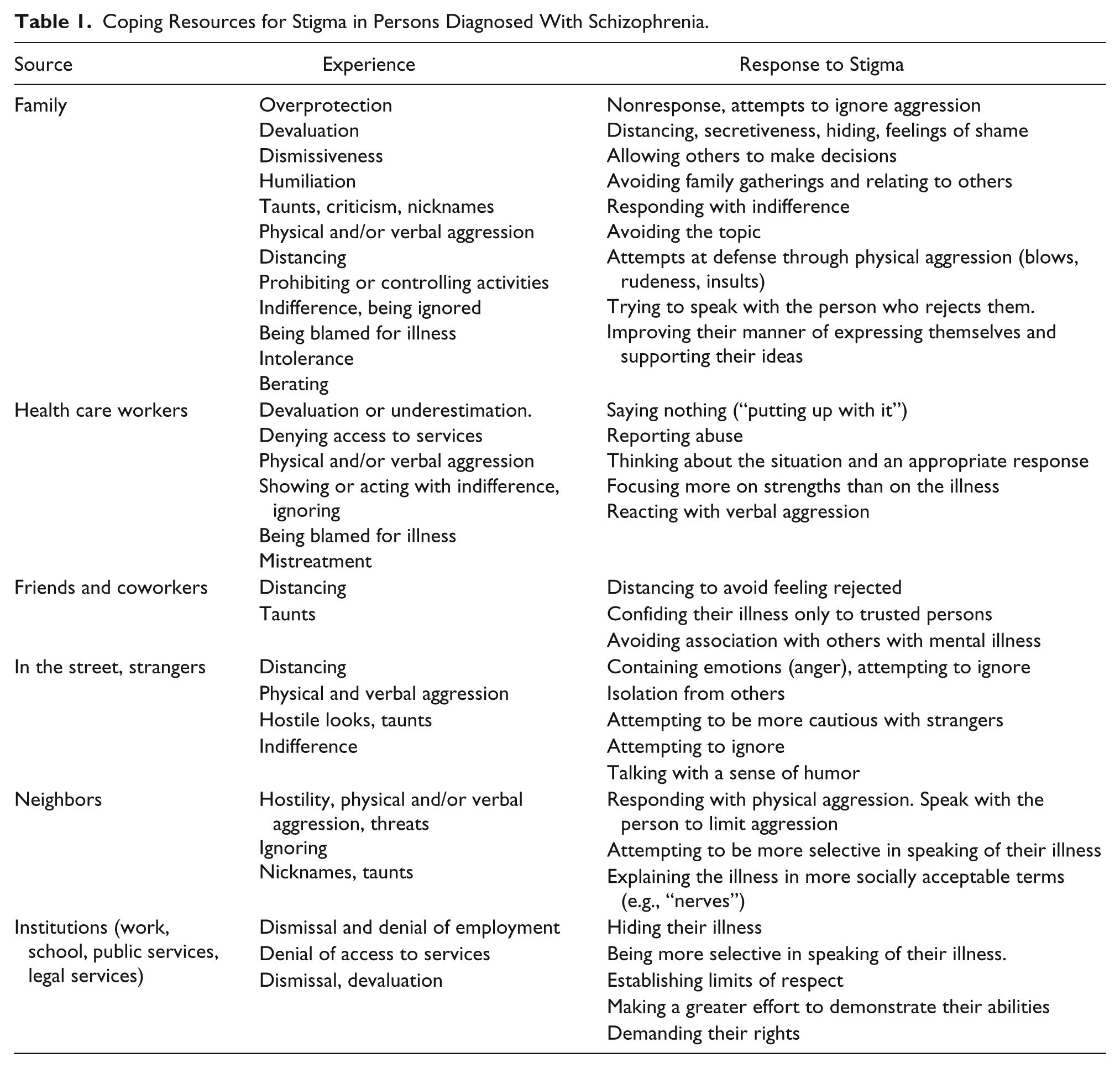
Tolerance
This category combines secrecy, resignation, and withdrawal, and includes those who act as passive recipients of rejection, resigning themselves in a way to the discrimination they experience, reacting with tears, sadness, and impotence without confronting it. This leads to an effort to hide their illness, to avoid communicating their experience, and an internalization of the negative beliefs and stereotypes associated with it, producing emotional distress and suffering. It is also characterized by dependence on others, seeking to have others make decisions for them. These types of responses were the less frequently found, and they came primarily from women.
I had a teacher who always rejected me, and even when they threw me out, they locked me in a room when I was 12, she told me I was crazy, that I was sick. I left it in God’s hands and told him that thanks to my father I have never said anything to anyone. Things always happen to people who bother me and I never wish anything on them—they say something to me and I keep quiet. (Woman)
Another type of experience participants described was the rejection of others with similar psychiatric illness. None of the participants was an activist in the sense of participating in defense of the rights of people affected by this type of illness. On the contrary, we observed a tendency on the part of the interviewees to distance themselves from other persons with psychiatric illness, as if being close to them would provide evidence that they were “mentally ill.”
There was a boy interested in me, but then nothing happened. He invited me out, and we went out for a little while. . . . He and I talked but that’s as far as it went. . . He had problems—what’s it called?—a learning disability, and I said, no way, I don’t like that he has this problem. It bummed me out, and my mother asked me why. It’s that he has a learning disability and I feel weird being with him, I mean, I feel like the two sick ones got together. (Woman)
Resistance to stigma
This category refers to the actions a person takes to limit social rejection caused by his or her illness; it is related to the individual’s capacity and resources to cope with the stigma associated with the illness. Within this category, there are three dimensions: limiting aggression, selective secrecy, and resignification of experience. The latter consists of a search for the personal meaning and significance of the experiences of stigma and discrimination and was the most common coping resource reported by participants.
Selective secrecy consisted of participants being open about their illness only with those persons who were closest and most trusted; it was a way of maintaining greater control over their integrity and avoiding the risk of exposure to criticism. It also helped them avoid being treated with condescension: One strategy, as noted previously, was to explain their illness to others as a problem of “nerves.”
The enfermito is this idea that since you’re sick, they have to treat you worse. I don’t like it. . . . I’m learning now to be more discreet about my illness, to know who to share it with. It’s not a secret—it’s an illness: an illness that’s a little painful, and, well, it’s difficult, you know? (Man)
Although both men and women tried to limit rejection in the form of physical or verbal aggression related to their illness, women tended to describe their emotional response in more intense terms, whereas men tended to ignore such rejection as “not worth the trouble.”
I said to my cousin, “Stop it! Why are you hitting me?” And she says, “Because you’re crazy.” And I told her, “Well you’re the crazy one, because you’re hitting me!” And we started to argue, and then we fought, she scratched me here, in the face, and I pulled her hair, and we started hitting each other. (Woman)
Seeking a different meaning or significance for the illness (resignification) was another resource for limiting discrimination. This involved the positioning of the subjects with respect to their illness, their attitude, and what they have learned through the experience of managing their illness. All of these provided resources for self-reflection, for supporting their ideas, defending their rights, and articulating their position in the face of aggression.
The processes of resignification did not happen automatically; they emerged gradually over the course of an individual’s experience with the illness, a process in which patients had an active participation. Once they received a diagnosis of schizophrenia, they often felt very vulnerable and became the target of multiple experiences of discrimination. Individuals who managed to deal with these experiences, however, took a more active role in creating alternative interpretations that allowed them the possibility to learn from their experience and manage their illness in a better way.
Knowing and understanding myself in a normal way helps me to think logically and rationally. (Man)
Other participants related how going to therapy or self-help groups helped them to gain a different sense of the experience of their illness. Some described this process as “trying to be strong and trying to work hard,” a process of demonstrating through their actions that prevailing negative perceptions and beliefs about their illness were wrong. One of the interviewees described it as a process in which people seek “dignity in the eyes of others by working to gain their respect.”
Along these lines, a woman informant who reads the tarot mentioned that her illness even had certain benefits in her profession, as her customers saw a magical component to her schizophrenia that could increase her abilities, in addition to allowing her to learn from her experiences. In this sense, her illness has allowed her to face up to certain challenges that she would otherwise not have managed:
It was a real shock, especially the first time, because I had never experienced it so intensely, but I didn’t take it as something tragic, not even as something that was going to change my life. Now that I am better I think it was an opportunity to know myself better, or to understand myself better, and well, somehow I keep going, but we’re not taking it like, oh no, I’m going to die. In the end [smiles] no one dies of schizophrenia. I’m living normally now, I tell you, I have schizophrenia, I don’t hide it, and well, I feel like at least me they don’t stigmatize. (Woman)
It should be noted that the experience of the participants included a spiritual and religious dimension at various stages in the process of managing their illness. With the exception of four interviewees, God was a fundamental part of their narrative; using expressions like “Thank God” and “I put myself in God’s hands,” they ascribed meaning and significance to their experience.
It’s a mental support, psychological, religious support is also very important, because there are a lot of believers here, there is a lot of religious faith in Mexico, and most of us are Catholics, so you approach religion and you approach the Commandments. One way of behaving is with values that people shouldn’t forget even if they have a mental illness. . . . They are indispensable sources of religious support for any mental patient. (Man)
The narratives of the participants testified to a set of coping resources originating in their history and experience with their illness. These resources had a sociocultural context that showed an active role throughout the trajectory of care and management of their illness, a role that was far from that of the “patient,” an infantilized vision in which their role was solely to be the passive recipient of a process of psychiatric service. Social support was, moreover, fundamental to their processes of resignification; together with subjects’ individual resources, it was involved in every aspect of their situation:
I was working and they fired me for being sick. I wanted to go back and my boss says to me, “You know what? You can’t come back.” I said, “No? What do you mean, no?” And I went with the doctor and he told me, “Fight for your job.” And so I argued with her. I said, “If you say I’m disabled, well, you’re going to have to pay my disability insurance, you’re going to have to pay for my medication, my hospital bill, and everything.” And because she’s so cheap, she said, “No, it’s better that you come back.” (Woman)
Even though participants identified health care workers as one of the major sources of stigma, as illustrated in a previous example, these could also be agents of change when they provided different types of resources to their patients: information, emotional support, accompanying them where helpful, and above all encouraging processes of resignification that helped patients continue with their personal plans and goals. In this example, the doctor’s intervention was very useful: The participant was able to defend her rights at work and keep her job; her boss asked her to forget about the affair and go back to work.
Discussion
This study provides a greater in-depth understanding of the impact of the process of stigmatization in persons with a diagnosis of schizophrenia in outpatient care in Mexico City. The findings of the study allow us to confirm the structural character of stigma and discrimination toward mental illness (Link & Phelan, 2001), as well as the dynamic of the processes of social exclusion by which its individual and sociocultural dimensions are linked.
One of the major contributions of this study is its perspective on the sociocultural context of the subjective experience of illness. This is shown in different places in the interviews: in participants’ interpretation of their psychiatric diagnosis and in their description of the resources they employ to face their illness. A majority of the interviewees, for example, referred to their condition as a problem of “nerves” originating in religious or magical experiences, including witchcraft, which in some cases defined their first attempt to seek attention. These interpretations form part of the daily context that surrounded them in which becoming ill from “nerves” was more socially acceptable than a schizophrenia diagnosis, which in the social imagination is linked to negative stereotypes of violence, lack of control, and madness (Mora-Rios et al., 2013a). In this respect, authors like López and Guarnaccia (2000) have referred to an attack of “nerves” as idioms of distress, a resource often employed in Latin American contexts to describe emotional problems (Castillo, 1996; Mora-Rios et al., 2008; Traverso-Yépez & de Medeiros, 2005). In a study reporting similar findings in a Latino population, Carpenter-Song et al. (2010) argued that “nerves” constitutes a form of cultural resistance to medical knowledge, used to reduce the stigma associated with mental illness. Along the same lines, Yang et al. (2007) hold that sociocultural factors are fundamental to an understanding of how stigma threatens the moral experience of individuals and groups and also how it influences subjective processes related to social exclusion. Based on the findings of our study, we believe that contemporary theory concerning stigma and mental health must incorporate the sociocultural dimension as part of a holistic and comprehensive approach to understanding these complex phenomena.
The paradigm of intersectionality (Hankivsky et al., 2010) is a useful frame of reference for analysis of gender as a transverse variable, which, together with other social determinants, such as sociocultural factors, inequality, and lack of access to academic and employment opportunities, generated an effect of multiple vulnerabilities affecting the well-being of the subjects. The testimonies also revealed different forms of violence, sexual abuse, discrediting, and experience of childhood neglect and mistreatment, as identified in previous studies (Borba et al., 2011; Chernomas et al., 2000; Loganathan & Murthy, 2011). The majority of the interviewees, for example, had no income of their own or worked in precarious employment without steady income, which left them in a situation of uncertainty and economic dependence on their families.
With respect to gender, research (Loganathan & Murthy, 2011; Sajatovic et al., 2005) has consistently shown that men generally appear to be more affected by the illness than women. One of its major effects is on employment; many of those with schizophrenia end up doing housework, which is socially more acceptable for women, and which generates conflict for men whose traditional role is provider for the family. This could explain the desire expressed by some male interviewees to have children, a spouse, and a family—which was not articulated by women.
Approximately, 87% of those interviewed mentioned having been the object of stigma or discrimination at least once in their lives. The principal sources of discrimination were their nuclear and extended families and health care workers, and the most common forms were symbolic violence, infantilization, and direct provocation. In addition to these experiences described in relation to social rejection, we also identified certain practices, such as indifference, apathy, and discrediting, which reproduced the stigma and discrimination. As has been described in other studies (Hansson, Jormfeldt, Svedberg, & Svensson, 2013; Jenkins & Carpenter-Song, 2009), these practices are found even among those providing psychiatric services.
These findings demonstrate that scientific knowledge about mental health and level of contact do not necessarily generate favorable attitudes and practices toward the mentally ill on the part of health care personnel (Arvaniti et al., 2009; Lauber, Nordt, Braunschweig, & Rössler, 2006; Rao et al., 2009). According to interviewees, medical providers are prone to blame them for their illness, discount their experiences, and show fatalistic attitudes with regard to their prognosis and life plans. This attitude was also mentioned as coming from other groups, including family and friends, and as being reproduced in different institutions, such as the media, as reported also in Sayre (2000). We also found, however, that health care personnel were a potential source of support in helping interviewees resignify their illness and pursue their personal plans and projects.
We should also not lose sight of the fact that health care workers too are the object of stigma and discrimination associated with their work, which is related to other problems of a more structural character. These have to do with public policy that marginalizes the problems of health care, particularly for mental health, which translates into services provided by limited and low-paid personnel with inappropriate or insufficient training. Such factors combine to create significant emotional fatigue in health care workers in this area, and the reproduction of inappropriate practices, which leads to a vicious circle that promotes exclusion in every area, not just that of persons with serious mental disorders. In any case, one of the major challenges continues to be the design of intervention strategies that successfully sensitize these workers, emphasizing the consequences of the stereotypes and negative beliefs on the quality of life of their patients.
The coping resources of participants in this study relative to stigma and discrimination did not differ greatly from those reported in other countries (Yow & Mehta, 2010). Participants frequently mentioned resources for coping with stigma and in particular the resignification of experience. For them, schizophrenia not only had negative implications but also represented for them the possibility of ascribing a different meaning to their lives that in some way gave them greater strength. This is consistent with other studies in which the illness represented the possibility of personal and intellectual growth and a challenge to realize goals they might otherwise never have set for themselves (Cardano, 2010; Knight, Wykes, & Hayward, 2003; Shih, 2004; Veseth et al., 2012).
These findings have implications for the care and empowerment of these individuals. Resignification is a valuable resource that could be useful in promoting the process of recovery, not only of those who have such resources but also of others in situations of greater vulnerability. The work of Moran, Russinova, Gidugu, Yim, and Sprague (2012; Moran, Russinova, Yim, & Sprague, 2014) has shown the effectiveness of having patients play a more active role during their recovery by acting as providers in self-help groups for others with psychiatric conditions. This activity represents an important resource for institutions as well as other patients. It empowers patients and provides them with jobs—sources of economic support consistent with their ideals—that proceed from secrecy to openness and that bring with them a process of transformation in identity from that of patient to one of activist.
Another type of cultural resource in the Spanish-speaking world also promotes these ideas: radio programs from Spain (Radio Nikosia, 2005), Argentina (“La Colifata”), and more recently Mexico (“Radio Abierta”), which seek to encourage those with psychiatric histories to embrace “alternative” identities—as writers, musicians, and poets, for example—that go beyond that of a “mental patient.” Participants in these radio programs contribute a variety of such suggestions.
Our analysis of participants’ processes of resignification of their experience of the illness likewise shows how this process is linked to sociocultural factors, and in particular to spiritual and religious ones, in explaining the origin of their illness, in describing their expectations for recovery, in their everyday language, and in their personal coping resources, which makes sense in a country like Mexico where the majority is Catholic: almost 83% of the population, according to the census of 2010 (INEGI, 2011). Religion clearly plays an important role in situations of conflict and crisis such as unemployment, illness, and death.
Today, this role is widely recognized around the world as important to the process of recovery. In our study, the majority of participants identified religion as one of their major sources of support, but others did not, and one even described having moved away from religion because it generated increased delusions. Religion, as Fallot (2007) argued, should be seen as part of subjective experience and should figure in the analysis of processes of social exclusion and their forms of expression in different parts of the world, though it is important to exercise care, as religious ideas could exacerbate the symptoms and delusions of some patients.
Limitations and Implications for the Future
Among the methodological limitations of this study, it is important to mention that the findings are based on a purposive sample of outpatients in specialized mental health care and it should be noted that their experiences may be different in people within community settings. However, our qualitative approach was highly useful in enlarging our knowledge about the social factors linked to structural processes of stigma and discrimination from the perspective of persons experiencing the illness. The use of thematic analysis and associated methodologies allowed us to approach the subjective experience of the interviewees. With regard to theoretical saturation, limitations emerged from the analysis owing to the complex and dynamic nature of the subjective experience, which includes interrelated biological, psychosocial, and cultural factors, and whose study presents a continuing challenge to research in this area. In this sense, one of the major strengths of qualitative methodological strategies is that they allow consideration of social practices surrounding the process of health–illness–care from the perspective of the principal actors involved, encouraging reflexiveness on the part of the researchers as well as the subjects of the study, which consider the ideological and cultural factors that underlie such practices.
Another of the major contributions of this study is its analysis of stigmatization processes through the narratives of the social subjects. As Link and Phelan (2001) showed, the critical eye of the social subject is evidence in such narratives, and this is where the roots of structural stigma can be identified, allowing us to identify specific necessities in this area. It remains to identify additional factors that favor the development of resources for coping with stigma in different sociocultural contexts. Such knowledge, together with the insights of the persons affected, could be incorporated into specific interventions directed at these populations, with the purpose of helping them to assume a more active role in defense of their rights (Bos et al., 2013; Whitley & Drake, 2010). We should remember that none of the interviewees participated in activist organizations; it would be worthwhile to promote such activity, which could have beneficial effects on psychiatric health care in Mexico City.
In sum, even while the literature has shown evidence for an improved outlook for persons diagnosed with schizophrenia in developing countries like Mexico (Castillo, 1996), our findings show various practices of stigma and discrimination, coming from distinct sectors of society, that are one of the major obstacles to care. For this reason, it is important to include geopolitical, social, cultural, and epidemiological differences in analyses of the stigmatization process and also the forms in which these inequalities manifest themselves at the local level. In this respect, one of the major challenges continues to be the development of more inclusive public policy in the field of mental health to influence social practice at the institutional level.
Footnotes
Acknowledgements
We wish to thank Dr. Duncan Pedersen of the Institut Universitaire en Santé Mentale Douglas, Montreal, Quebec, and Dr. María Elena Medina-Mora, Director of the National Institute of Psychiatry Dr. Ramón de la Fuente Muñiz, for supporting this cross-cultural research initiative. We are also grateful for the valuable contributions of the individuals and institutions who participated in the study, as well as the team of interviewers.
Authors’ Note
A preliminary version of this work was presented at the 5th International Conference on Stigma, Ottawa, Canada, June 1 to 3, 2012.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. We are grateful for financial support from the Fondo Sectorial de Investigación en Salud y Seguridad Social and Consejo Nacional de Ciencia y Tecnología (FOSISS-CONACYT-069261) and the program Igualdad entre Hombres y Mujeres 2013.