
Abstract
This qualitative study examined how female breast cancer patients without partners conceptualized their relationship status. Qualitative data were collected from 20 participants who did not have partners during diagnosis and treatment. Phenomenology informed the methodology and thematic analysis. Breast cancer patients without partners discussed how they made meaning of their relationship status within the context of their cancer experience and barriers they faced dating post-diagnosis or treatment. Oncology care providers, public health professionals, and family scientists can use the study results to better understand the specific concerns and experiences of breast cancer patients without partners. Additional implications of these findings for patients, practice, and research are discussed.
Keywords
Breast cancer patients benefit from effective social support when they are undergoing diagnosis and treatment (Buki et al., 2008; Galván, Buki, & Garcés, 2009; Schmidt & Andrykowski, 2004). Previous research identifies intimate partners as a potential—but not guaranteed—source of social support for breast cancer patients (Fang, Manne, & Pape, 2001; Yang & Schuler, 2009). Less is known about the experiences of women who are single when they are diagnosed with breast cancer. By learning how women make meaning of their relationship status within the context of their cancer experience, medical professionals will have a more comprehensive understanding of the role of relationship status—including any meaning attributed to it—by people facing serious health issues.
Due to improved screening and treatment over the last few decades, more breast cancer patients are surviving longer (National Cancer Institute, 2015). Thus, there are more issues surrounding survivorship, including breast cancer patients’ perspectives on dating. While the literature varies on whether having a partner is a benefit or deficit to the breast cancer patient, to date, to our knowledge, there are no previous studies that examine the experiences of breast cancer patients without partners (Ginter & Braun, 2014a). Therefore, it is necessary to consider literature that discussed the role of intimate partners for breast cancer patients. By understanding the significance of partners’ roles, we might ascertain what it means not to have a partner when facing breast cancer.
Role of Intimate Partners for Breast Cancer Patients
Mastectomies and radiation therapies may affect female patients’ body image; chemotherapy may negatively affect their sexual desire and functioning (Fobair & Spiegel, 2009). For these reasons, breast cancer can have unique effects on patients’ intimate relationships. Among women with breast cancer, marital stress is associated with slower recoveries (Yang & Schuler, 2009). Patient distress can contribute to spousal stress; spousal stress often leads to marital stress (Fang et al., 2001).
One study found that being single may be a protective factor against depression among breast cancer patients (Vahdaninia, Omidvari, & Montazeri, 2010). One explanation for this association is that a breast cancer diagnosis may be the catalyst for relationship dysfunction or dissolution (Fang et al., 2001; Fobair & Spiegel, 2009; Vahdaninia et al., 2010). However, it is difficult to determine causality between breast cancer diagnoses and intimate relationship dysfunction (Kneece, 1995). Previous findings suggest that relationships and marriages that do not survive the breast cancer experience had preexisting problems that ultimately caused the dissolution, and relationships in which someone is diagnosed with breast cancer are no more likely to end than other relationships (Dorval, Maunsell, Taylor-Brown, & Kilpatrick, 1999; Taylor-Brown, Kilpatrick, Maunsell, & Dorval, 2000). (A significant limitation of these studies is their lack of racial and ethnic diversity.)
Characteristics of support from partners vary. In one study, African American breast cancer patients felt emotionally supported by their intimate partners, although the partners did not assist them in making health decisions (Ashing-Giwa & Ganz, 1997). Extant literature suggests that support may also vary by sex. Among a sample of same-sex couples, female partners played a crucial role in patients’ breast cancer treatment experiences, performing additional household roles and offering verbal support and encouragement (Boehmer, Freund, & Linde, 2005; White & Boehmer, 2012). At the same time, female partners who are caregivers of cancer patients generally report more anxiety and care burden than male partners (Perz, Ussher, Butow, & Wain, 2011). Opposite-sex partners’ reported reactions to women’s breast cancer diagnoses and treatment include avoidance and withdrawal strategies that caused distress to patients (Fergus & Gray, 2009; Manne, Ostroff, Winkel, Grana, & Fox, 2005). Among a sample diverse in relationship status, breast cancer patients who found a new partner post-diagnosis were more sexually satisfied than patients who retained the same partner (Ganz, Rowland, Desmond, Meyerowitz, & Wyatt, 1998). There is also information to suggest that a single woman is protected from the simultaneous stressors of illness and dysfunctional relationships (Vahdaninia et al., 2010).
Making Meaning of Relationship Status
Although “single” is frequently interpreted as people without partners, it is not a monolithic concept. One may be ever-single, divorced, or widowed (Lahad, 2012). Another set of classifications is whether an individual is voluntarily/temporarily, involuntarily/temporarily, voluntarily/permanently, or involuntarily/permanently single (Stein, 1981). These variations of relationship status invite different contextual explanations for women’s current life experiences (Lahad, 2012).
The experience of singlehood can differ by race, ethnicity, age, and gender (Lahad, 2012). Among a sample of single women, African American women were more likely to attribute their relationship status to structural issues (systemic shortage of available male partners) as compared with European American and Latina women (Tucker & Mitchell-Kernan, 1998). Older and divorced women are more likely to adjust to their single status as compared with younger or ever-single women (Allen, 1989; Lewis & Moon, 1997). As ever-single women age, they report an increased awareness of their changing social world (including the diminished pool of eligible partners) and acknowledge feeling displaced in their families, particularly if other relatives their age are married (Sharp & Ganong, 2011). While ever-single women may still hope for a long-term partner, they may simultaneously grieve for the absence of a partner and possibly children as well as the perception that their families have decreased interest in their romantic lives (Sharp & Ganong, 2011).
These experiences suggest singlism, discrimination against single people (DePaulo & Morris, 2005). Singlism reflects society’s ideological promotion of couples over singles “in everyday thoughts, interactions, laws, and social policies” (Sharp & Ganong, 2011, p. 957). Upon reviewing recent U.S. Census data as well as literature on single women, Sharp and Ganong (2011) posited, “women remain restricted (and face stigma and discrimination) in a society that promotes marriage and motherhood as central to women’s identities” (p. 958).
Relationship Status as a Health Disparity
Relationship status may be considered a health disparity. Unmarried women are more likely to be diagnosed with later stage breast cancer than are married women (Kuo, Mobley, & Anselin, 2011). Between 1970 and 2007, excess mortality of never-married cancer patients increased compared with married patients (Kravdal & Syse, 2011). Married individuals tend to have better overall health than never-married individuals; married individuals are also more likely to go to a physician when they experience suspicious symptoms (Kravdal & Syse, 2011; Nayeri, Pitaro, & Feldman, 1992; Osbourne, Ostir, Du, Peek, & Goodwin, 2005). Both marital status and the presence of a partner are predictors of breast cancer patients’ quality of life and functioning (Taira et al., 2011). However, research diverges on whether being partnered is a protective factor or a risk factor for patient functioning. One study found that among breast cancer patients, being single was associated with fewer depressive symptoms over time as compared with being partnered or married (Wittenberg et al., 2010).
Theory: Ecological Systems Framework
Ecological systems theory may offer a broad understanding of the impact of the social environment on the breast cancer patient. This framework is based on the concept that individuals live in four types of nested environmental systems and that there are bidirectional influences within and between systems (Bronfenbrenner, 1979). Additional assumptions of ecological systems theory include humans are social and need to interact with other humans, we can understand human behavior on multiple levels, and when the environment is no longer supportive, humans must adapt (White & Klein, 2008). Ecological systems theory and phenomenology (the guiding methodology for this study) work together to explain participants’ lived experiences within their nested systems (Spencer, 2007).
Nested Systems
Individuals do not live in isolation; rather they are constantly interacting with their microsystem, mesosystem, exosystem, and macrosystem (Bronfenbrenner, 1979). The microsystem consists of individuals and institutions that either directly affect the breast cancer patient or with which she is directly associated. These may include the patient’s family, friends, and associates; her job and co-workers; religious institution; and her medical team oncologist, surgeon, radiologist, and nurses. The size of the microsystem changes as people take up and end life roles (Berk, 2007). Thus, an individual’s microsystem might expand post-diagnosis, because it will include hospitals and new medical teams. The mesosystem comprises the relationships between microsystems. The mesosystem includes relationships between family experiences and job experiences, church experiences and hospital experiences, and hospital experiences and job experiences, and so forth. For example, if the patient’s family had bad experiences with physicians, those experiences are likely to influence how a woman in that family interacted with her medical care providers. Likewise, if chemotherapy treatments leave the patient feeling fatigued, then she might have had to take time off work. That time off might affect her work environment or her relationships with colleagues.
The exosystem refers to links between social settings in which the patient is and is not directly a part. For example, hospital policy, which is created by administrators and policy makers, might dictate that the medical team asks whether the patient has a supportive family that can accompany her to treatments. In asking this question, the medical team might learn that the patient does not have anyone to accompany her, and so they will put her in contact with Nurse Navigators for additional support. Hospital administration is not a setting that the patient is part of, but she has been impacted by the administration’s policies. The macrosystem refers to the patient’s cultural context . The macrosystem includes the socioeconomic status, race and ethnicity of its members, as well as federal policies on health insurance.
Interpersonal Relationships
When a woman is diagnosed with breast cancer, this disease and the treatment for it will greatly shape her environment: hospital visits, doctor’s appointments, medical jargon, and discussions of recovery and survivorship will permeate her life (Pereira, Brito, & Smith, 2012). As stated earlier in the literature review, a breast cancer diagnosis has a large impact on a woman’s interpersonal relationships. For example, she may seek deeper connections with her family and friends, or she may find that negative reactions to her diagnosis lead to faltering relationships. Requiring time off from work for surgical and medical procedures may impact her relationships with supervisors and co-workers. In turn, the woman’s interpersonal relationships will likely affect those medical appointments and discussions. There is a constant give-and-take between individuals or families and their surrounding systems. The necessity of change is another form of adaptation.
Adaptation
Adaptation is a crucial component of the ecological systems framework (White & Klein, 2008). When an individual’s system is perceived to be inadequate, then the breast cancer patient or family must adapt (Radina, Ginter, Brandt, Swaney, & Longo, 2011). Methods of patient adaptation include changing and enhancing personal environments (i.e., eliminating unsupportive individuals or including new individuals or groups of people that are supportive, such as a cancer support group; Erci, 2007). In turn, members of those environments must respond to the adaptations. Another example of bidirectional influences occurs when oncologists receive feedback from patients about their needs; oncologists must adapt their behavior to adequately communicate with them (Rottman, Helmes, & Vogel, 2010).
Ecological systems theory also applies to this study because previous research indicates that medical team members, who become an important component of the patient’s microsystem, must be vigilant in talking with their breast cancer patient about the patient’s relationships. Otherwise, they may make incorrect assumptions about the patient’s support systems. Thus, although the medical team’s primary concern is treating the patient’s breast cancer, it would also be extremely beneficial to inquire about the patient’s ability to rely on family and friends for instrumental and emotional support, because these things could in turn affect the patient’s ability to understand and act on the information that the medical team is providing.
By fully understanding the patient’s perspective on her illness, the medical team is better equipped to offer additional information and resources that will improve the patient’s health and overall quality of life (Thornton, Powe, Roter, & Cooper, 2011).
Method
Participants
Twenty women without partners were recruited for this study. This was the number at which saturation was reached. Saturation occurs when enough data have been collected that more data do not shed additional light on the topic under investigation (Glaser & Strauss, 1967). In one popular sampling technique, sampling for range, the researcher identified the sample’s subgroups and attempted to collect data evenly from individuals that belong to those groups (Small, 2009). The subgroups for this study included 10 Caucasians, nine African Americans, and one Indian American woman. The former two groups are the largest racial/ethnic groups in the United States.
To be eligible for participation, individuals must have been above the age of 18, unpartnered at the time of diagnosis and treatment, and treated for breast cancer in the last 5 years. The rationale for these inclusion criteria was that individuals who had not been treated for breast cancer recently might have forgotten some of their experiences. Not only was sampling done for range, but snowball sampling was also used within those groups. Snowballing expanded the sample by asking participants to recommend other potential participants who share the same racial, ethnic, or socioeconomic background (Small, 2009).
Recruitment
Breast cancer patients without partners were recruited through electronic mailing lists and by posting announcements on discussion boards on Internet-based support groups for breast cancer patients. Such online organizations include breastcancer.org and the Susan G. Komen online support forums. Permission was obtained from website hosts before posting announcements about the study. These patients were contacted with information about this study to determine whether they were willing and able to participate. The University of Maryland College Park Institutional Review Board (IRB) granted approval for this study (373050-1).
Initial recruitment efforts procured several Caucasian participants and one Indian American participant. To ensure even numbers of African American and Caucasian participants, recruitment was extended to African American-specific breast cancer support organizations (both local and national), and all nine African American participants were recruited.
Potential participants completed a short screening survey to ensure that they were eligible for the study (i.e., above the age of 18, were treated for breast cancer within the last 5 years, and did not have partners at the time of diagnosis and treatment). Participants self-identified their race/ethnicity, education level, age, year of breast cancer diagnosis, partnership status at the time of diagnosis and treatment, and income. Participants were entered into a raffle for a US$50 gift card. After all interviews were conducted, a name was drawn.
Interviews
The women took part in face-to-face or telephone interviews that lasted approximately 75 minutes. Informed consent was obtained prior to each interview. The interviews were semi-structured and included measures of health literacy, health status, spirituality, and demographic information. Ecological systems theory drove construction of the interview guide; there were questions pertaining to participants’ experiences in their microsystems, mesosystems, exosystems, and macrosystems. Questions of adaptation were also asked. The interviews were conversational in nature, allowing the participant to guide the interview. Each interview was digitally recorded and transcribed and the interview guide was pilot-tested.
Methodology
Phenomenology is a method for investigating the lived experience of people in a study “from the standpoint of a concept or phenomenon” (Schram, 2006, p. 98) and was used as the method for understanding how women without partners navigate their breast cancer diagnoses, treatment, and recovery. Phenomenology lends itself to qualitative methods because researchers are gathering experiential material (Adams & van Manen, 2008). Although the lived experience is unique to every individual, researchers ought to be able to “convey a meaning that is fundamental to the experience no matter which specific individual has had that experience” (Schram, 2006, p. 99). There was an essential structure of the concept (breast cancer experiences of women without partners) that allowed for individuals’ varying perspectives (Creswell, 1998).
Interviews were conducted with participants to determine how they faced, have been affected by, and discussed their breast cancer experiences and what those experiences have meant in the context of their relationship status. The interview questions asked participants to describe their lived experiences (Creswell, 1998). The “basic tenets” of phenomenology are meeting, learning, discussing, and understanding (Schram, 2006, p. 100), and these tenets were used to learn how participants “experience, live, and describe” the phenomenon (p. 100) and subsequently uncovered the meaning of these experiences and descriptions (Creswell, 1998).
Thematic analysis
After transcribing an interview, notes were made of participants’ statements about experiencing the phenomenon. This inductive thematic analysis is often used in phenomenological research to find common threads indicated by the data (Creswell, 1998). Transcripts were reviewed multiple times for a deeper understanding of the data, and identifiable themes or “meaning units” (p. 150) were noted (Creswell, 1998). For a pattern to constitute a theme, there had to be substantial data from multiple participants. Word repetition, similarity in descriptions of experiences, and noting what participants did not say also contributed to the thematic analysis.
Patterns were analyzed into themes and shared with peer debriefers (three doctoral students trained in qualitative methodology, social science, and public health). They read the sections of transcripts and the analysis to offer alternative interpretations. Member checks were conducted with some participants. In this way, both depth and breadth of analysis of themes were achieved (Lincoln & Guba, 1985). After verifying with participants that these themes represented their descriptions of their lived experiences, the authors developed a final codebook.
After creating the final codebook, literature related to the patterns were sought to form an overall description of the concept and the essence of the phenomenon (Creswell, 1998). The phenomenon under investigation was the experiences of female breast cancer patients without partners. Ultimately, readers of this study should be able to say, “I understand better what it is like for someone to experience that” (Polkinghorne, 1994, p. 46).
Trustworthiness
Credibility was ensured by establishing rapport with the participants prior to the interview, by keeping a journal of experiences and thoughts throughout the collection and analysis of the data (researcher reflexivity) and by conducting member checks. Dependability refers to the consistency with which the data are collected throughout the study (Morrow, 2005). To demonstrate this, all journals, logs, and auditable records were maintained so that the specific research processes could be scrutinized.
By using member checks and peer debriefing, conclusions were deemed well-founded (Lincoln & Guba, 1985). After sharing the analysis with participants, they confirmed that the study clearly reflected their lived experiences.
Results
Twenty women were interviewed for this study. Their ages ranged from 36 to 70, with the average age being 52.2 (SD = 8.1). Ten participants self-reported as Caucasian–nine as African American, and one as Indian American. Nineteen self-identified as heterosexual and one self-identified as bisexual (Table 1). At the time of the interviews, 11 had never been married or in a domestic partnership, nine were divorced, and one was in a relationship that began after she completed treatment. All 20 women were single and had health insurance throughout treatment. The sample was well-educated, with 75% possessing college degrees and 50% possessing graduate degrees. More than half of the participants earned at least US $75,000 a year. Time since diagnosis ranged from 7 to 92 months, with the median time being 24 months (µ = 32.1, SD = 21.9). Data were collected on a number of topics, including the social support needs and health-seeking behaviors of single breast cancer patients. Information on needs and experiences of single mothers diagnosed with breast cancer have been published (Ginter & Braun, 2014b).
Results are organized around seven themes related to relationship status: descriptions of relationship history, thoughts on being single pre-diagnosis, reflecting on the differences between having or not having a partner during treatment, comparing relationship status to partnered patients, being single post-diagnosis, disclosing health status to potential partners, and impact of treatment on the participants’ bodies and sex drives.
Relationship Status in the Context of Treatment
Relationship history
Prior to diagnosis, 10 of the participants were divorced or were in the middle of divorce proceedings. Several characterized their previous partners as having been emotionally and verbally abusive. One woman said about her former husband:
The divorce was my idea. I had been pretty sick for 10 years with fibromyalgia and chronic fatigue, and he didn’t do illness. And just night and day, he was an angry person and very abusive. Emotionally abusive to me, because I wasn’t pulling my weight.
She did not file for divorce until her therapist said, “You need to get out of that relationship, or you’re going to die there.”
Another participant who was in the middle of divorce proceedings when she was diagnosed said,
My marriage was very stressful for me. I’m really glad that we did split up, because it gave me peace of mind and . . . he was a very stressful man. He was very stressful and very verbal . . . abusive. So I didn’t need that with my surgery.
A few women were dating men casually but stopped seeing the men as soon as they were diagnosed, believing the men would not be supportive during treatment. One reminisced,
So the second time I was actually dating somebody, um, not all that serious but we were dating up until the time of diagnosis, and his response to my diagnosis weirded me out, so I ended that right away. Because when you go through this, you need to focus on you.
As another participant explained about her recent breakup, “I didn’t want to be in a relationship that wasn’t headed some place.”
Ever-single participants that had not dated recently were more inclined to describe their pre-diagnosis lives as lonely. As one woman commented, “It was sad not to have a partner to share things with . . . everybody needs a shoulder to cry on.”
Thoughts on being single pre-diagnosis
While some expressed sorrow for the end of previous intimate relationships, all said they were better off single than they would have been if they had stayed with their exes, regardless of their health status. Participants that were not dating in the months preceding their diagnoses not only expressed interest but also felt that their lives were full even without intimate partners. When asked what it meant to be single prior to her diagnosis, one participant said, “It meant I was single. Nothing thrilling, just single. Nothing thrilling. Me and my own life, don’t question it. Don’t have to answer to anyone.” She continued, “I was working two jobs, sometimes 60 hours . . . I didn’t really have that much time. So yeah, if it came up, I was good.”
Similarly, another woman explained,
I’m not averse to having a relationship, but it would have to be something so significantly added to my life, because I consider my life very good. I dated briefly when I moved here, but when I saw that I resented having to carve out time, and I said, “This really isn’t what you want to be doing.” I was like, “Well, do you think we could meet from 2:00 to 4:00 but I don’t know if I want any more time.” I think it was more that social norm that I should want to do it.
Speculating on a partner’s presence during treatment
There were four categories of responses to this question, reflecting participants’ varying beliefs about how relationships fare under the stress of a health crisis. Speculation was based on their pre-diagnosis experiences with intimate partners as well as observations of fellow breast cancer patients that were partnered.
First, many said that their experiences would have been easier if they had had a partner, but emphatically not one of their previous partners. When asked about how her breast cancer experience might have been different with a partner, a previously married participant immediately countered, “Do you mean a real partner?” Another woman responded, “It really depends on the partner. If it was the guy I was going to marry, so much worse. Just—oh my God, just infinitely worse.”
Second, other participants conveyed that if they had had a partner during treatment, they would have felt more emotionally supported. One woman replied, “I think I might not have felt so alone throughout my journey. Like I said, I have people that love me and that I love and they were there for me, but I still felt alone.”
Another participant reflected,
My treatment would have been different because I would have had a partner, I would have had a husband and somebody that really loved me; that was there. It really hit me, the women that are married going through this . . . I mean, man. To have a husband to know you, he’s there for you. I can’t imagine how wonderful that would have been. The love. He knows if you have a left breast or not, to help you make decisions: “Honey, get the breast or whatever makes you feel good, I’m okay with you.” That would have just been the ultimate.
The third category of participants suspected that a having a partner would have been nice, but that it was not critical to one’s overall health and well-being. These participants acknowledged the strain that cancer places on relationships. One participant said,
It’s nice to have a partner, but it’s not necessary. . . . Somebody once told me that if you’re with someone, and there’s an illness . . . that will test everything within a relationship. And I believe there’s some truth to that. You know, the focus has to be on your health, and what you need to do to be healthy. And depending on what type of relationship you’re in—if you’re with someone that’s needy, and now you’re the one that’s going to be needy, it’s not going to work. And that will make you more devastated than anything.
Another participant said,
I’ve heard so many horror stories. Would they be with me because they have to be, because why would you break up with somebody when they’re going through cancer? I’d feel guilty–would they really want to be with me? I think personally for me in the long run, it was probably better that I was by myself. It taught me to just see what I was fighting for and what was worth fighting for.
In the fourth category, participants were grateful not to have partners during treatment. Both via speculation and observing their friends’ partners, participants perceived partners as being a drain on one’s energy and focus. As one participant said,
I think that if I’d had a partner, I would have been more concerned about how my partner was doing than how I was doing. I think in some ways—for me, anyway—it was easier, because I could make all the decisions for myself. Focus on myself. Do what I wanted to do or not do, and if I wanted to lock myself in the house for a week and not get out of my pajamas or talk to anybody, then I didn’t have to. Versus if I were in a relationship, I’d still have to support that relationship at some level.
Comparing relationship status to other breast cancer patients
Participants often drew comparisons with breast cancer patients who did have partners during treatment. Even within one participant’s social network of breast cancer patients, there were notable differences among their friends with partners. One commented,
I think what that all comes down to is how your life could be different if you were in a marriage or not. You know, you have friends that have very supportive partners who were a total part of it and were there and had the other person’s back. You had other partners who were totally the opposite and were a drain on energy instead of any kind of caregiving, loving support, and then you have those in the middle who still need their demands met but help you out. It kind of goes all ways, and I’ve only seen one or two of my friends in that first category with supportive spouses who, once they were diagnosed, were there for them. More than that, friends who ended up divorced because of the cancer.
One woman noted that women with families of their own had more built-in motivation than women like her:
The other thing about being single is that a lot of the “inspirational” stories about women going through treatment is how they did it for their children or grandchildren. People without children or grandchildren have to find their own motivation, which I think is harder.
Several participants talked about how patients without partners needed to be more proactive in seeking support. As one participant explained,
I would imagine that women who didn’t have partners are more like me, in that you’re out there, like telling everybody, you’re on the message boards, not isolated at home with your husband, relying on him. You know, you’re relying on everybody.
At the same time, participants also acknowledged that professional support was not the same as having an intimate partner to rely on. Another said, “I know American Cancer Society does have somebody you can call, but you’re talking to somebody who is volunteering and listening, which is nice, but you don’t have a connection with them.”
Sometimes participants forgot that patients with partners could have very different experiences than they did. One woman recalled,
So one of my friends who was in the process of getting a diagnosis, when I told her, “Oh, you need to go see Dr. XXX, she’s fabulous.” I said, “Well, here’s her number, call her and make an appointment.” I told her, “Well, do you want me to go with you?” And she basically—she didn’t take me up on it. She was like, “Why would I want you to go with me? My husband will go with me.” [Laughs] Yeah, it was a little different, but I guess I wasn’t accustomed to the role that your husband would play.
Thoughts on being single post-treatment
Most participants were interested in dating again, even if they were not immediately prepared for the next steps. Participants admitted to feeling lonely. Although one woman felt the support of loved ones, she still felt something was missing: “And I had sooo much support from my co-workers, all of my family, my friends—I had plenty of support. But I still felt alone.”
Many expressed interest in dating in the future, but were nervous about getting back into the dating game. A never-married participant said, “I really would like to be in a relationship. At some point, I’d love to get married. But I don’t know that that’s necessarily going to happen.”
Participants varied in how quickly they wanted to meet someone. One said emphatically, “I’m looking for a spiritual partner to share my life with. That’s the bottom line.” In contrast, another stated, “I do want to get married again. But I don’t have issues with being single.” Some participants expressed interest in dating, but for the time being, they wanted to focus on themselves. As one woman explained,
Right now I’m still trying to get back to [name]. I know I’ll never be the old me, but I’m still trying to get myself back to where I feel comfortable . . . I am afraid to show my scar, talk about my situation . . . this is personal. I don’t think I want to share that right now with anyone.
Because she was not ready to show her scar, which represented her overall breast cancer experience, she knew she was not ready to date and disclose such a recent and big part of her life.
Disclosing health status to potential partners
At the time of the interviews, all but one participant were still single. Many discussed how they have or would disclose their health status to potential partners, and what it might be like to show their post-treatment bodies to those partners. One woman admitted, “Now that this is in my lap, I wouldn’t expect a guy to be interested.”
Another woman, who had attempted dating after completing treatment, said,
I didn’t know what to say about the cancer, when to say it. And even now I really don’t know, 5 years out. Even now I feel I try nonchalantly to bring it up, and that’s pretty much the end of me seeing whoever that is, because most guys just don’t know how to deal with it. Usually I make sure I’ve done something kind of active before I bring it up, just so that they know, “Okay, you’re not going to drop dead on me!” [Laughs] . . . I’ve done a lot of online dating, so when you tell somebody that you’re a cancer survivor, they construct images of you being really sickly, the idea that you’re walking around bald throwing up all over the place. Definitely not somebody anybody would want to date! [Laughs] So if you tell somebody after you’ve gone running or gone for a hike or whatever it is, it’s like, okay, they definitely know that you’re not sick anymore, that you’re fine, but still, hearing that that 31-year-old had cancer, it’s pretty scary for most guys. And then the fact that I can’t have kids—I guess that’s another deal-breaker for my age group.
Among participants who had shared their health status with men they were dating or wanted to start dating, many found that those men were never to be heard from again. One woman recalled,
The first guy I dated, I think he hesitated and didn’t want to get involved with me in case I was going to die. [Laughs] And then the second one—eh, he’s kind of like—it’s like he’s a real avoider of stuff like that. Like of course I told them, I was real casual. And there was another time he was like, “One day I’d like to hear more about that,” and I was like, “Okay,” and he never—that day never seemed to come. I think that’s how he is . . . He knows he should want to hear it, but he doesn’t.
The one participant who was dating someone at the time of the interview was also the only participant who had had a positive experience disclosing her health status to a potential partner. She said,
I told him about the mastectomy, the scars I had, and how uncomfortable I was exposing those. So he told me, “Don’t worry,” when I felt comfortable and wanted to talk about it some more we would! And one evening he came to visit me and we were talking about things in general and he asked me if I felt comfortable enough to let him see where I had the mastectomy and, you know, he wanted to see the scars I wanted to hide so bad. So I showed him. I was a little apprehensive, but I showed him, because I cared a lot about him for all those years—I had feelings for him and he had feelings for me. And he told me, he said, “There’s nothing wrong with those scars.” He said, “No. Girl, don’t feel ashamed.” He said, “No. Those are good, because that’s what helped keep you alive, so that you and I could go see each other.” So it’s like, “Oh, okay! I’ll look at it that way.”
Impact of treatment on the body and sex drive
Several participants talked about how much their bodies changed from surgery and chemotherapy: scars, missing breasts,
1
baldness, and extreme weight loss or weight gain. Participants framed these changes in the context of their relationship status and how it might affect their ability to meet potential partners. One woman said,
My thinking was, hey, I can’t walk around with one boob. I’m going to start dating again and hopefully fall in love. You know, I’m sorry to say, but my first thought was, who’s going to go out with someone with one breast?
A participant who gained 70 pounds after her diagnosis commented,
The first thing that guys would notice about me is that yes, I am overweight. And then, if they can get beyond that, then it’s like when you get to the bedroom, you know, it’s like to have to be, “Oh, by the way, my boobs aren’t real and I don’t feel anything on my chest.” I don’t know, I feel like it’s just too many strikes against me at this point.
She summarized, “Face it, most of us don’t want to be alone forever. We want to be social. We want to date, but this is just another thing that makes you feel like you can’t.”
One woman wondered aloud,
What are my breasts going to look like, um, post-radiation? And one of my friends who’s been through it says, “They’re going to look like a fried rib!” [Laughs] You know, how distorted will I be, and will I be attractive to someone? But anybody who comes into my life, to share that kind of intimacy with, will have to love you, not just on a physical level.
Another participant also felt that whomever she eventually met would have to be attracted to her on multiple levels:
I’m like, “Dear God, I couldn’t get a man when I was really pretty, and now, how the hell am I going to attract . . . ” But, in the long run, I thought, “Well, you know, maybe I didn’t meet the right guy before because of my looks or being superficial. And now I might meet somebody who really loves me for who I really am.”
A participant who underwent a lumpectomy reflected,
After I started to go through the surgery and all of that, it was like, wow. It didn’t actually start to bother me until after I went through all my treatments and everything. That’s when I started to think about, “Oh my goodness, I’m not married now,” and if you think about how I look physically, is a man going to want me?
Several other participants conveyed that if they started dating someone now with their post-treatment bodies, then they would know that person was interested in them on all levels, and not due solely to physical attraction.
Participants also acknowledged the impact that treatment had on their hormones. Some participants stated that sex was not as important to them as it was pre-diagnosis and that taking Tamoxifen had shut down any sexual desire. Others felt that chemotherapy had forced their bodies into premature menopause, which also lessened their sex drive. In contrast, one participant found that her sex drive increased during her radiation treatment:
I felt certain that it was chemical or there was something bodily about it, because who wants to have sexual feelings during radiation when you’re working all day and running to the hospital every single day. It’s like the worst time. Why would I be suddenly interested?
Discussion
The purpose of this study was to explore how breast cancer patients without partners make meaning of their relationship status within the context of their breast cancer experience. The following section presents major conclusions, implications, and limitations, and offers directions for future research. The practical implications of this study apply to many types of family and medical professionals. Overwhelmingly, participants stated that they were better off single than with their former partners and spouses. They also admitted that a supportive partner would have been desirable. Most felt that their experiences would have been different with the presence of partners; responses varied in terms of whether their experience would have been enhanced or worsened.
Major Conclusions
Distinguishing between an unworthy partner and a worthy partner
Participants discussed the numerous differences between having a good partner and having a bad partner. This was often based on their pre-diagnosis experiences with unsupportive and even abusive partners. Participants also observed how fellow patients that were partnered were not necessarily better supported; not all partners are the same. These perspectives are reflected in the cancer literature (Fang et al., 2001; Fobair & Spiegel, 2009).
Finding worthy partners post-diagnosis
There was a residual grief in some participants’ stories: Women pointed out that while they could get by on their own during diagnosis and treatment, it would have benefited them to have a supportive partner throughout that process. Although participants often had supportive friends and family, they still felt a deficit. This was compounded by their uncertainty about dating after being diagnosed. Of all the participants who had started dating post-treatment, all but one reported having negative experiences with dating post-diagnosis. They attributed this to potential partners (in all cases, men) not feeling comfortable with their health status—especially if the participant was in her 30s or early 40s when diagnosed.
Despite a lack of research on the experiences of breast cancer patients without partners, a literature search yielded one article on the experiences of young women with breast cancer susceptibility genes (BRCA; Hamilton & Hurley, 2010). Those women talked about difficulty disclosing this information to potential partners. However, participants in that study could only speculate whether they would be diagnosed with breast cancer, whereas participants in the current study had already been diagnosed and were undergoing or had recently been treated. Findings regarding dating post-diagnosis may have implications for other cancer patients and survivors.
Utility of Theoretical Framework
This study used ecological systems theory to understand the lived experiences of breast cancer patients without intimate partners. Ecological systems theory posits that individual experiences occur within integrated systems of family and contextual factors. Thus, a single woman who is facing a breast cancer diagnosis is surrounded by multiple systems of factors that will influence her reaction to the diagnosis, treatment, and holistic experience.
Participants discussed the positive and negative reactions and relationships they sustained with these groups throughout their diagnosis and treatment experience. Encounters with potential partners formed a significant portion of participants’ microsystems. The mesosystem—the interaction of two microsystems—was evident in participants’ observations of partnered patients; these observations impacted their opinions on the necessity of partners. The macrosystem included broader attitudinal influences. Participants discussed the impact of the cultural idealization of breasts on their reconstruction decisions (Figure 1).
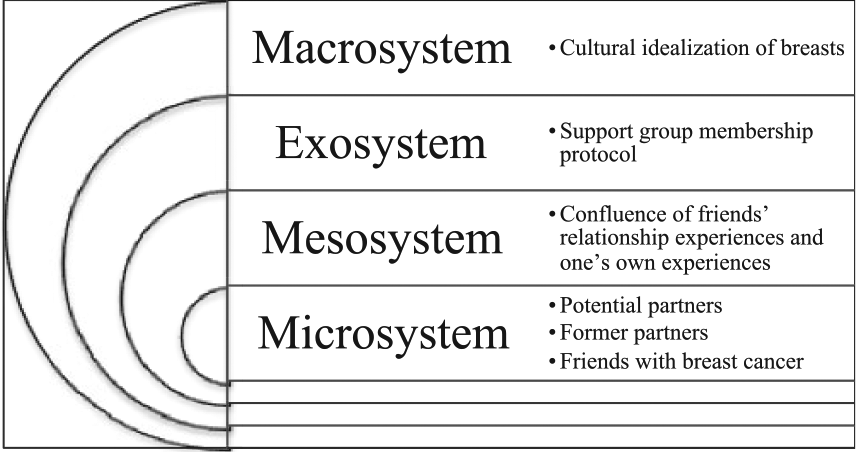
Ecological Systems of Breast Cancer Patients without Partners.
Another premise of ecological systems theory is that individuals learn how to adapt. If the system is inadequate, then people will make the necessary changes to survive. This was very apparent in the study. Participants talked about finding in-person and online support systems to make up for the absence of partners. Adaptation also applied to the bidirectional influences of patients and the medical team.
Directions for Future Research
This exploratory study uncovered important themes that should be examined further. Many women were interested in dating—often to find a serious partner, rather than a casual fling—but either feared or had experienced potential partners’ loss of interest subsequent to the disclosure of their health status. This was particularly true of younger participants (i.e., under age 45). Future research should look at how breast cancer patients seek intimate partners and when they choose to disclose their health status. Some of these results might be generalized to other cancer diagnoses and to chronic health issues.
This study had no age parameters except a minimum age of 18 years old. Women aged 36 and 55 alike indicated interest in dating. However, there were notable differences between women who had never had children and those who had. Future studies might examine age, cancer stage, prognosis, and parity as factors in expectations for dating post-diagnosis. Although saturation was reached in this exploratory study, future researchers might usefully consider larger samples stratified by age. Participants’ comments about their age being a factor in diagnosis, treatment, and overall experience led the authors to this conclusion.
Conclusion
This study illuminated a specific group in the breast cancer community: women without partners. This group was previously unrecognized in the literature. The purpose of this qualitative study was to examine how women without partners make meaning of their relationship status in the context of their cancer experiences. By learning how these women made meaning of their relationship status within the context of their cancer experience, family scientists will have a more comprehensive understanding of the role of relationship status—including the meaning attributed to it—by people facing serious health issues.
Participants drew comparisons between themselves and patients with partners. They discussed what it meant to have less built-in support—and what it meant to not be burdened by unsupportive partners. They speculated on the prospect of dating as patients and survivors, and they pondered how their experiences would have been different with partners.
To best support breast cancer patients, it is vital that medical teams and family scientists understand patients’ challenges and strengths. This includes understanding how the absence of intimate partners might produce different experiences for women. This exploratory study yields new insight concerning how women without partners think about their relationship status in the context of breast cancer. The results have implications for research, practice, and personal health care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.