
Abstract
Maternal mortality remains a significant public health challenge for Timor-Leste. Although access to quality family planning measures may greatly reduce such deaths, consideration of indigenous perceptions, and how they influence reproductive health decision-making and behavior, is crucial if health services are to provide initiatives that are accepted and helpful in improving reproductive health outcomes. We aimed to demonstrate that body mapping is an effective method to traverse language and culture to gain emic insights and indigenous worldviews. The authors’ two qualitative research projects (2013 and 2015) used a decolonizing methodology in four districts of Timor-Leste, body mapping with 67 men and 40 women to illuminate ethno-physiology and indigenous beliefs about conception, reproduction, and contraception. Body mapping provided a beneficial conduit for identifying established indigenous reproductive perceptions, understandings, and vocabulary, plus fears surrounding contraception. This may inform health service provision and engagement, ultimately improving the reproductive health of community members.
Keywords
International reproductive and sexual health strategies such as the Safe Motherhood Campaign and the Millennium/Sustainable Development Goals provide frameworks on which low-middle-income nations may focus their resources aimed at improving maternal health (Jaffre & Suh, 2016). The success of such strategies requires an intimate understanding of context and the targeted community (Mwaikambo, Speizer, Schurmann, Morgan, & Fikree, 2011; Say & Raine, 2007). Through probing indigenous knowledge, researchers have identified different interpretations of physiological concepts among stakeholders (Butcher & Kievelitz, 1997; Pelto & Pelto, 1997). The exploration of these alternate worldviews provides insights which may influence reproductive health decision-making, behavior, or service provision (Ireland, Narjic, Belton, Saggers, & McGrath, 2015; Mba, Obi, & Ozumba, 2007). The qualitative research method of body mapping, that is, asking people to draw and explain their anatomical and physiological perceptions, is an effective way to gain such insights (Cornwall, 1992; MacCormack, 1985).
Ignoring these emic ethno-anatomical and ethno-physiological beliefs decreases the chance of successfully implementing new health policy, as well as risks losing valuable indigenous knowledge. In addition, opportunities for health promotion may be jeopardized with the development of health messages or interventions that are ignored or unsuccessful if deemed inappropriate or irrelevant (Butcher & Kievelitz, 1997; Doyle & Faucher, 2002; Goodkind, Gorman, Hess, Parker, & Hough, 2015; Jordan, 1989; Senior, Helmer, Chenhall, & Burbank, 2014). Ethno-anatomy and ethno-physiology are described as “the ways in which we conceive of the body, its internal process, and its ideal configuration” (Dighe, 2011, p. 238). A person’s perception of their anatomy or physiology is particular to their worldview (Obermeyer, 2000). These beliefs stem from lay understandings and local experiences, and are perpetuated through cultural practices, social relations, behaviors, and explanations (Draper & MacCormack, 1987; Zaman, Mustaque, & Chowdhury, 1998).
This article aims to demonstrate that body mapping is an effective interdisciplinary qualitative research method to explore different ways of knowing. We explain how we used body mapping to sensitively navigate language, culture, and different levels of education to gain insight into reproductive ethno-anatomy and ethno-physiology of men and women of reproductive age, in this case in Timor-Leste. High maternal mortality and fertility remain significant public health challenges for Timor-Leste, and discussions surrounding reproductive health are often challenging due to the sensitivities associated with this arena. Through gaining such emic perspectives and determining what people know and believe about reproductive anatomy, physiology, and contraception, the reproductive health providers, policy makers, and health educators will learn about indigenous knowledge and be more informed to develop health messages and interventions that are relevant, appropriate, respectful, and understandable, aimed at achieving best possible reproductive health outcomes.
Body Mapping—Origins and Applications
Body mapping appears in the literature in diverse contexts with various applications (Brewis, 1994; de Jager, Tewson, Ludlow, & Boydell, 2016; Sobo, 1993; Victora & Knauth, 2001; Zaman et al., 1998). It has been used as a clinical, educational, anthropological, therapeutic, story-telling, and political tool, employing simple materials such as sticks to draw in the dirt (Cornwall, 1992) to technological tools such as 3D computer imaging (Tarr & Thomas, 2011). Given the varied applications, it is perhaps not surprising that a fixed definition is elusive.
The history of body mapping is opaque, and within the literature, two distinct origins are described— the “anthropological stream” and the “therapeutic stream.” Within the reproductive health literature, the method first appeared in Shedlin’s (1979) study focusing on modern methods of contraception in a Mexican community. Subsequently, MacCormack (1985) used body mapping to explore perceptions of contraception, reproductive anatomy, and physiology in a large study in Jamaica. MacCormack’s (1985) study served as inspiration for similar anthropological research by Cornwall (1992) in Zimbabwe, following which Cornwall devised the term “body mapping” (Cornwall, 1992, 2016).
This body mapping method has been used multiple times within reproductive health, not only primarily to gain insight into reproductive ethno-anatomical and ethno-physiological beliefs but also to explore perceptions of contraception, the impact of gynecological morbidity, the effects of vasectomy, and health-seeking behavior in the context of sexually transmitted infections (Belton, Whittaker, & Barclay, 2009; Brewis, 1994; Butcher & Kievelitz, 1997; Jaswal & Harpham, 1997; Sobo, 1993; Sturley, 2000). It is a respectful and gentle method to gain emic worldviews, a sensitive method to discuss taboo or delicate concepts, and an effective method to clarify ambiguities, investigate vocabulary, or gain access to perceptions across cultural, linguistic, or literacy barriers. Body mapping may be empowering for participants, potentially “giving a voice” to previously silent, marginalized participants (Victora & Knauth, 2001). The method is flexible—it may be conducted with individuals or with groups, and depending on the research question and context, participants may be provided with a template of a male or female body or asked to draw their own. Constants of the method include interviewing the participant about their map at the conclusion of its creation, reassuring participants that there is no “right” or “wrong,” and that benefit stems from the creation as well as the conversations the map invokes. Although this flexibility is reported as a strength, it could be argued that it adds to the method’s ambiguity.
The second stream of body mapping, the “therapeutic stream,” has foundations in the political arena of HIV/AIDS advocacy in South Africa, and developed from a project aimed at reducing stigma surrounding HIV/AIDS (de Jager et al., 2016; MacGregor, 2009). This method of body mapping asks participants to record symbols, words, and stories on life-sized outlines of their body, with this process often spanning several hours or days. It has provided the basis for multiple global workshops, and is viewed as a therapeutic procedure focused on individual empowerment, self-discovery, and resilience (Gastaldo, Magalhães, Carrasco, & Davy, 2012). Much of the literature engaging this stream of body mapping has centered on the therapeutic benefits for those living with HIV/AIDS. However, it has also provided an effective means to explore areas including eating disorders, chronic pain, trauma, chronic illness, and migrant health experiences (Brett-Maclean, 2009; Chenhall, Davison, Fitz, Pearse, & Senior, 2013; Gastaldo et al., 2012).
Although both streams of body mapping have unique origins and applications, they share numerous characteristics, including the ability to navigate different cultures, language, and levels of education; give a voice to the marginalized; and provide the opportunity to gain emic insights. However, as we wished to gain insight into indigenous perceptions of reproductive anatomy, physiology, and contraception, body mapping aligned with the anthropological stream was most appropriate for our study.
The Context for Our Study
The República Democrática de Timor-Leste (commonly abbreviated to “Timor-Leste,” formerly known as “East Timor”), is a tiny half-island nation in the Malay Archipelago in South East Asia (Gunn, 2010). Archeological research indicates that humans have been on the island for 35,000 years, with migrations of several different ethnic groups including Negritos, Proto-Malays, and Melanesians (Metzner, 1977). This population diversity remains evident today (Taylor-Leech, 2008). In the 16th century, the Portuguese began annual sandalwood harvesting expeditions to Timor, concurrently establishing Dominican and Franciscan missions (Hicks, 2003). Although many Timorese reportedly converted to Christianity, they simultaneously continued their animistic beliefs and practices—a “blending” that persists in contemporary Timor-Leste (Molnar, 2010). Traditional Timorese ways of life, including allegiance to local Kings and laws, were severely disrupted in the early 20th century, when Portugal flexed its colonial muscle, breaking up local kingdoms and imposing new regulations (Hicks, 2003). Portugal retreated from Timor-Leste in the mid-1970s, after which Indonesia, who occupied the western half of the island of Timor, violently invaded and occupied the country for 24 years (Gunn, 2010). A resounding vote for independence in 1999 led to the destructive withdrawal of Indonesia, and the beginning of an independent Timor-Leste (Molnar, 2010).
Independence has not been without its obstacles for Timor-Leste. Poverty, nation building, gender inequality, patriarchy, and violence are all significant challenges, and despite efforts toward improving health outcomes, the maternal mortality ratio (557 maternal deaths per 100,000 livebirths), and total fertility rate (TFR;5.7 births per woman) remain some of the highest in the region, whereas the contraceptive prevalence rate of 28% is well short of the Ministry of Health’s target of 40% (Ministry of Finance, 2010; Ministry of Health, 2015). Fertility has been, and remains, vitally important to the Timorese, and is aligned with good fortune and favor from the ancestors (Belton, Whittaker, Fonseca, Wells-Brown, & Pais, 2009; Hicks, 2003; Wild, Barclay, Kelly, & Martins, 2010). Traditional fertility promoting practices include rituals and offerings to ancestors, whereas traditional fertility regulating practices include the consumption of certain plants or teas, or the burying of the placenta further from the home for lengthier space between pregnancies (Thompson & Mercer, 2012).
In recent times, despite many women reporting the desire to cease or delay the birth of more children, a significant number state that they do not and will not use modern methods of contraception (Ministry of Finance, 2010). Such opposition may stem from pro-natalist ideals, Catholic values, reproductive obligations linked to bride-price (barlake), myths about side effects, or fear linked to Indonesian times when the Government sanctioned the family planning program Keluarga Berencana (KB; Thompson & Mercer, 2012). KB promoted a restrictive two-child policy, and employed coercive techniques to enforce contraceptive injections for girls and women (Sissons, 1997).
Although a recognized, pragmatic, public health approach to improve maternal health is to decrease the number of pregnancies a woman experiences through the provision of quality modern methods of contraception, the services provided need to be culturally appropriate with providers having insight into a community’s reproductive perspectives and worldviews (Diamond-Smith & Potts, 2011; Jaffre & Suh, 2016; Winikoff & Sullivan, 1987). Also, confidence to use contraception requires a knowledge of how one’s body works (Hartmann, 1995).
Timor-Leste is a conservative country where discussions concerning reproductive health and associated services are often very sensitive, and reproductive biomedical knowledge has been reported as minimal (Belton, Whittaker, Fonseca, et al., 2009; Richards, 2015; Thompson & Mercer, 2012). Although previous research in Timor-Leste exploring ethno-physiological beliefs has focused on conception, abortion, labor, and health-seeking behavior (Wild et al., 2010; Zwi et al., 2009), we wished to learn about indigenous perceptions regarding reproductive anatomy, physiology, and perceptions of modern methods of contraception, to inform service provision and focus education. We believed the body mapping method described in the anthropological literature (Cornwall, 1992; MacCormack, 1985) provided a gentle, nonthreatening way to glean such insights, respecting cultural sensitivities, language barriers, and educational differences. To our knowledge, there is only one example in the literature of body mapping within Timor-Leste, and this was with a small sample of women (Belton et al., 2009). We aimed to extend the application of this method to include many participants from a number of different districts and educational levels in Timor-Leste. Our two projects involving body mapping exercises took place in November 2013 (Project 1) and October 2015 (Project 2). Project 1 involved body mapping with women of reproductive age from eight locations across two districts of Timor-Leste, with educational levels ranging from no schooling to tertiary-level studies. A key finding was the almost unanimous recommendation of the need to speak with men regarding reproductive health and accessing contraception, and the recognition of men’s powerful influence over reproductive health choices. This led to Project 2, a component of which involved men of reproductive age taking part in body mapping exercises to explore the beliefs and perceptions on which they base these reproductive health decisions. Our studies also employed focus group discussion using vignettes and individual reproductive history interviews to further explore reproductive health perceptions and decision-making; however, these aspects will be reported elsewhere.
Both projects were collaborations—first between Charles Darwin University (CDU) and Marie Stopes Timor-Leste (MSTL), and second between La Trobe University (LTU), CDU, and MSTL. MSTL is a nongovernmental organization based in Dili working with the Ministry of Health. It provides reproductive and sexual health outreach and clinic services, including family planning education, counseling and services, screening for sexually transmitted infections, and some simple antenatal care, in 11 of Timor-Leste’s 13 districts, employing mostly local staff from the communities they serve. Our projects aligned with the global Marie Stopes Family Planning 2020 pledge of “understand[ing] who our potential clients are, what their needs are, and what tools and approaches work best to deliver modern family planning choice and services to them” (Marie Stopes International [MSI], 2013).
Method
We employed a qualitative research design with decolonizing methodology (Smith, 2012). This means we placed Indigenous knowledge in the center of our research, and considered respectfully Timor-Leste’s history of colonization throughout our projects (Marsh, Cote-Meek, Toulouse, Najavits, & Young, 2015). Decolonizing methodologies are founded on respect, trust, reciprocity, partnership, and collaboration, and throughout our projects, we strived to maintain these values through establishing and maintaining appropriate relationships between the members of our team and our research participants (J. G. Bartlett, Iwasaki, Gottlieb, Hall, & Mannell, 2007; Smith, 2012). Decolonizing methodologies must be beneficial and empowering for the Indigenous participants, and our projects prioritized Timorese knowledge and amplified Timorese voices (Simonds & Christopher, 2013). Qualitative methodologies engaging creative visual methods such as body mapping are sympathetic to decolonizing frameworks, bridge indigenous and Western knowledge, and valorize the voices of the participants, keeping indigenous ways of knowing at the forefront of the research process in an empowering and respectful manner (Cornwall, 1992; Guillemin, 2004; Huss & Cwikel, 2005; Lu & Yuen, 2012).
Buttressing our decolonizing methodology was the guiding principle of “Two-Eyed Seeing” (Hall et al., 2015). Two-Eyed Seeing, developed by Indigenous Canadian researchers (Iwama, Marshall, Marshall, & Bartlett, 2009), provides an approach to blend, weave, and bridge different worldviews (Martin, 2012). Two-Eyed Seeing does not elevate one way of knowing more than another, rather it “refers to the ability to see with one eye the strengths of Indigenous ways of knowing and with the other eye the strengths of Euro-Western ways of knowing, and using both these eyes together” (Vukic, Gregory, & Misener, 2012, p. 148). Advocates of Two-Eyed Seeing encourage users to view the concept visually as two eyes on two connected jigsaw puzzle pieces (C. Bartlett, Marshall, & Marshall, 2012). This illustrates the flexibility of the concept, as well as the possibility of connecting more pieces to the puzzle if required (C. Bartlett et al., 2012). This “multiple-eyed” approach illustrates diverse ways of knowing and the ability to modify approaches depending on what works best in a particular context (Hovey, Delormier, McComber, Lévesque, & Martin, 2017). The model recognizes diversity not only between Indigenous and Western knowledge systems, but within knowledge systems, promoting respect and trust between those involved (Vukic et al., 2012). As previously reported in this journal, Two-Eyed Seeing may result in “creating shared ownership of new knowledge and ultimately, adaptation to, and reconfiguration of such knowledge back into research and health promotion practices that are inclusive of both perspectives” (Hovey et al., 2017, p. 1285).
Our decolonizing methodology and guiding principle of Two-Eyed Seeing allowed the research team to blend, weave, and consider alternate worldviews, histories, and experiences (Hovey et al., 2017). This process influenced all phases of our research design, and facilitated the respectful collaboration and partnership within the team. The field research team for Project 1 consisted of the first author (a female Australian midwife), two East Timorese staff members from MSTL (a female and male), a non-Timorese female MSTL staff member, and an East Timorese midwifery lecturer from the National University of Timor-Leste. Project 2 consisted of the same first author and East Timorese MSTL staff members plus an extra male East Timorese staff member with extensive research experience, and a different non-Timorese female MSTL member. Although religion, especially Catholicism was important for a number of our research team, we were able to discuss the potential influence of these personal beliefs on our projects. In addition, MSTL staff are required to sign a code of conduct that supports family planning values. Ethics approval was obtained from Timorese and Australian research institutions (Human Research Ethics Committee, Cabinet of Health Research, Ministry of Health, Dili, Timor-Leste MS-INS/DF-DP/XI/2013/688 & 2015/527; Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research, Darwin HREC 2013-2084; Human Research Ethics Committee, LTU, Melbourne 15-072). Qualitative research training for Timorese field staff occurred at MSTL prior to each project. The research team collaborated with local experts and reproductive health service providers on all phases of the project. The research tools were piloted in Dili with nonclinical MSTL team members prior to data collection.
Research Sites
The districts of Dili and Viqueque were chosen for Project 1 due to their low contraceptive prevalence rates (CPR; Ministry of Finance, 2010), whereas for Project 2, Viqueque, Baucau, Ermera, and Dili were chosen considering CPR, TFR, and number of reported maternal deaths. The majority of research sites were situated in rural parts of Timor-Leste—70% of Timor-Leste’s population live in rural areas (Ministry of Finance, 2010). Timorese research team members approached the traditional leaders of each site and explained the project. All accepted inclusion. The MSTL team communicated with the nominated communities in the weeks preceding data collection, providing written explanations about the projects in the indigenous language, Tetum, and verbally conveying this information with respect to those with limited literacy skills. Many of the research sites were challenging to access, involving hours of driving over corrugated dirt roads or winding up through coffee plantations into remote mountain districts. The body mapping exercises took place in private, quiet spaces—under bamboo-roofed verandas, on plastic chairs under trees, or in open-sided shelters.
Sampling and Recruitment
Diversity across Timor-Leste with regard to location, age, and marital status is well-documented (Hicks, 2007; Molnar, 2010). Therefore, with both projects, we wished to speak with married and single women and men of reproductive age (18–49 years), from rural, peri-urban, and urban areas, with varying levels of education. We also wished to distinguish participants classified as “youth” (25 years or younger). We recruited participants purposively based on their age and location; some snowball sampling also occurred. For two groups in Project 2, we purposively sampled younger, unmarried men, as they are recognized as a challenging population to motivate regarding access to sexual and reproductive health services. Table 1 highlights our participants’ characteristics.
Body Mapping Participants’ Characteristics.
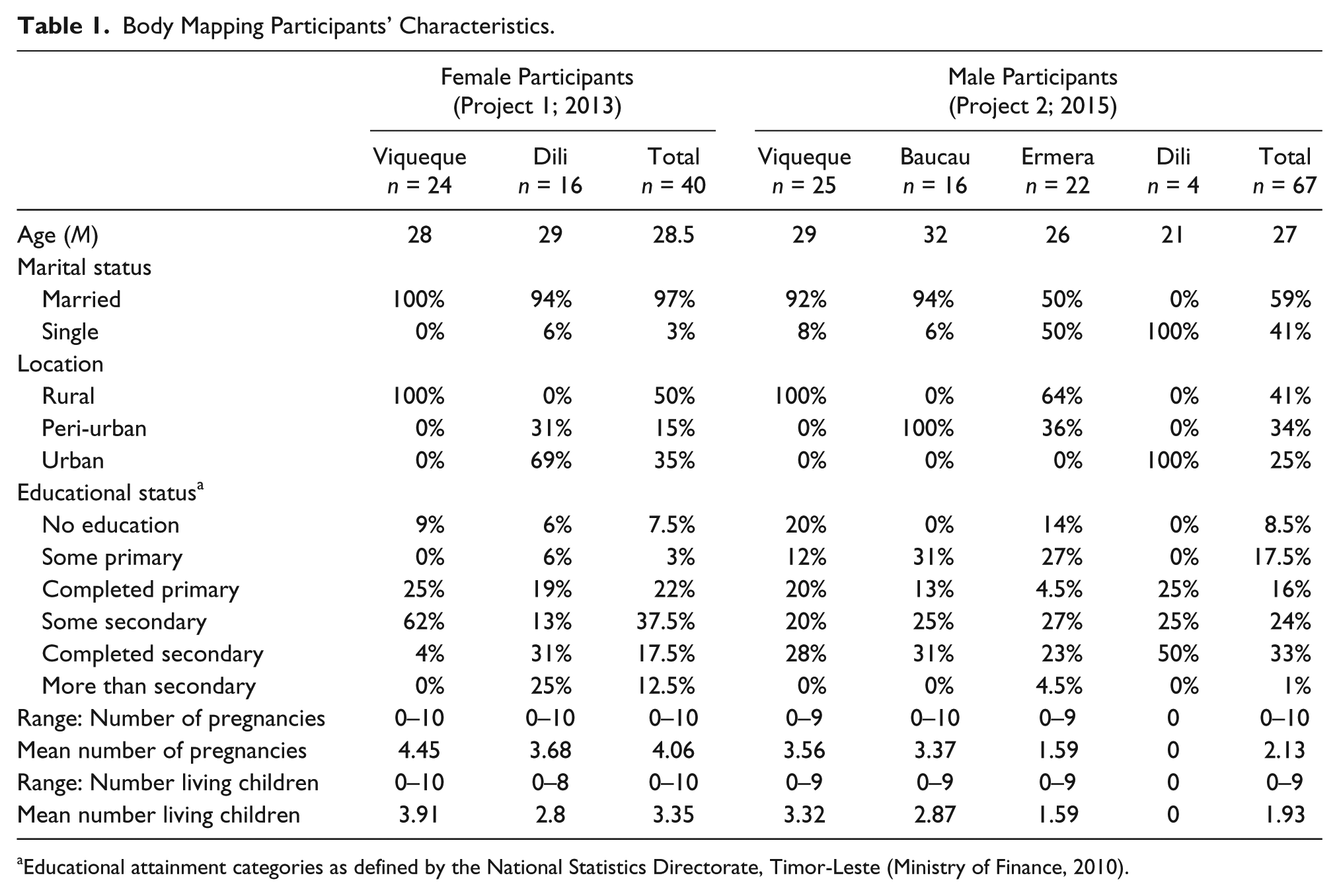
Educational attainment categories as defined by the National Statistics Directorate, Timor-Leste (Ministry of Finance, 2010).
Participants were verbally invited into the study by either the MSTL team working in that district or by the village leader or his wife. Participants may or may not have been MSTL clients. All provided informed consent, and were reassured that they could exit the study whenever they wished.
Body Mapping Exercise Method
Our body mapping exercises took place at the conclusion of our focus group discussions (to be reported elsewhere). Each participant was given an A4-sized page printed with the outline of a body (LLC, 2013; complexedbody.blogspot, 2015), and asked to draw their perceptions of the reproductive system, where a baby grew, and any known methods of contraception.
A Timorese female facilitated the women’s groups; these groups were provided with the outline of a woman’s body (Project 1; see Figure 1). The men’s groups were facilitated by a Timorese male, and were provided with templates of both male and female bodies (Project 2; see Figure 2). Timorese members of the research team recommended this for a comprehensive insight into the perceptions of Timorese men. The sociodemographic characteristics of sex, age, location, and marital and educational status of each participant were recorded on the back of their map.
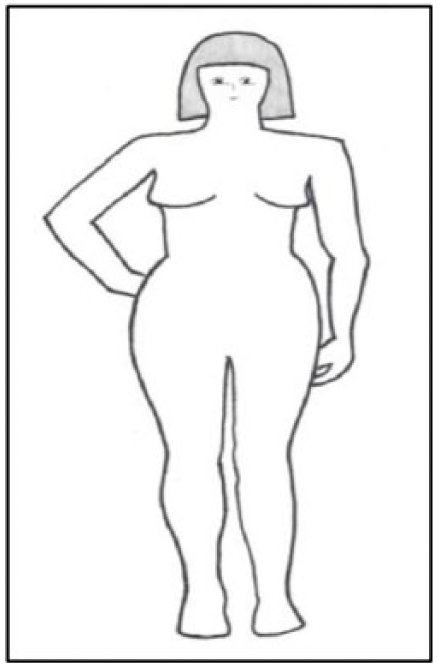
Template for female participants (LLC, 2013).
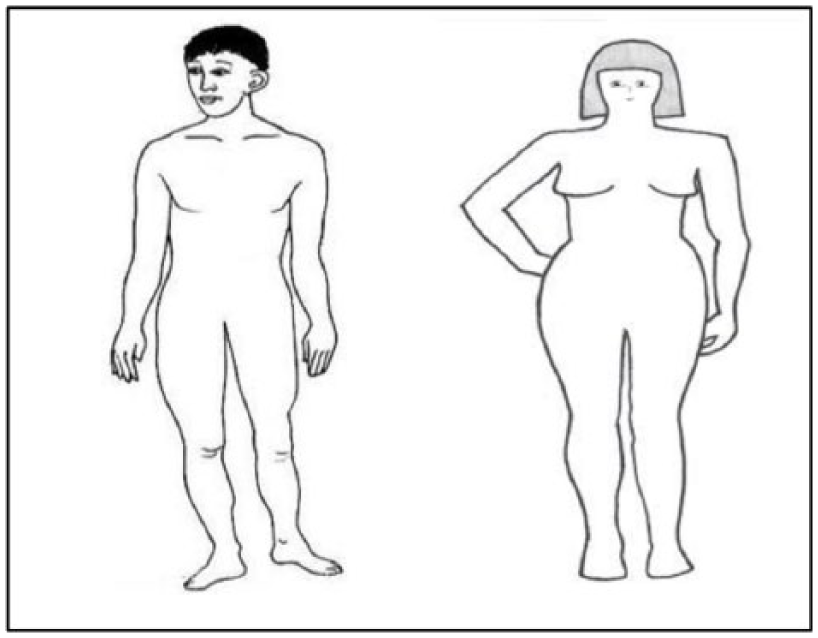
Template for male participants (LLC, 2013; complexedbody.blogspot, 2015).
We provided red and blue pens and requested participants draw anatomical perceptions in blue and contraception perceptions in red. Participants were reassured that the research team was not interested in their drawing skills. Participants sat quietly to complete their maps with little discussion, and for the most part, people appeared confident taking part.
Participants were invited to individually explain their maps to the facilitator at the conclusion of drawing (on average, 15–20 minutes), in a private space where they could not be heard by the main group. These discussions were iterative and open-ended in style, led by the participant, and based on their map. They provided participants the opportunity to explain their reproductive ethno-anatomical and ethno-physiological beliefs as well as nominate any modern methods of contraception they knew about, plus an opportunity for the researchers to ask questions to clarify any ambiguous concepts. Perceptions were summarized back to the participant for accuracy. For Project 1, the first author (non-Tetum speaker), sat with the multilingual female facilitator (fourth author), who translated the participants’ explanations from Tetum to English in real time. Translations were later verified using audio recordings of the discussion, plus notes made by the first author and facilitator. For Project 2, the participants explained their drawings to the male Timorese facilitator (sixth author), who made notes and audio recordings. Translation from Tetum to English took place with a translation panel consisting of two to three bilingual Tetum-English speakers at the completion of the data collection, allowing for shared, collaborative meaning-making and clarification. At the conclusion of the body mapping exercises, the research team requested to keep or copy the body maps, to which all participants agreed.
Analysis
We began by visually examining the body map, noting shapes, marks, or words. The map was then considered in partnership with the translated and transcribed verbal explanations. On numerous occasions, this changed the interpretation of the map, for example, when initially examining the body map illustrated in Figure 3, we thought that the participant had drawn two ovaries on either side of a woman’s pelvis. However, during the verbal-explanation phase, the participant explained that the structures on either side of the pelvis represented the uterus— if the baby was a boy, the uterus was on the right, and if the baby was a girl the uterus was on the left.
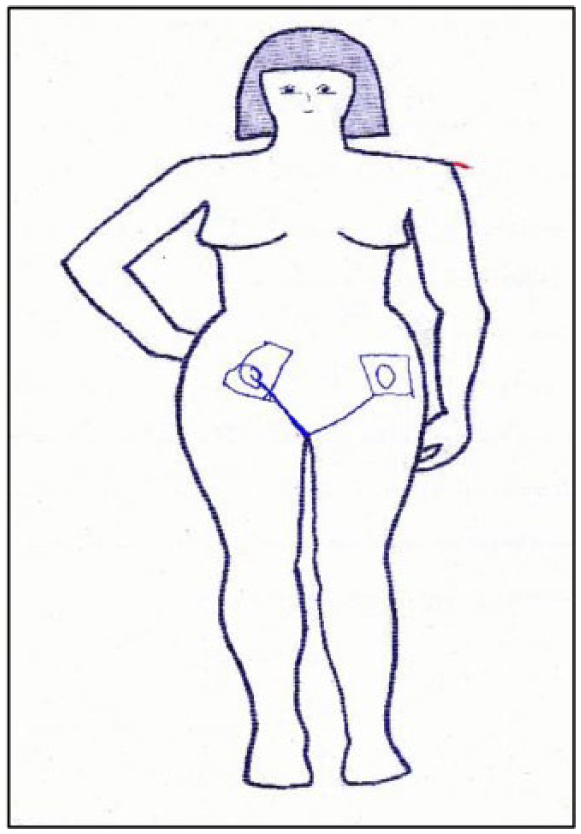
Body map completed by female participant, 28 years old, peri-urban area, completed primary school.
After examining each map, we inductively created a list with terms used by the participants to name reproductive structures, processes, and contraception. These lists expanded as new concepts emerged, and we formed tables representing each participant and their perceptions. A biomedical framework was used as a point of reference when comparing the body maps (Jaswal & Harpham, 1997; Victora & Knauth, 2001). We are mindful of the tension that exists between our decolonizing methodology and inductive coding when compared with a Western biomedical framework, and while acknowledging the need for a point of reference (Whittemore, Chase, & Mandle, 2001), we acknowledge the importance of Two-Eyed Seeing, the bridging of paradigms, and the sharing of perspectives (Hovey et al., 2017; Martin, 2012).
We compared maps first within individual groups, and then more widely across all groups, using our sociodemographic characteristics. This allowed us to identify common Indigenous terminology and beliefs. Previous anthropological studies using body mapping have described contributing to rigor via triangulation (Bam, Bhatt, Thapa, Dossajee, & Angdembe, 2014; Brewis, 1994), and we were able to do this with data collected via other methods during our projects, namely, focus group discussions and individual reproductive history interviews (reported elsewhere). Also, the consistent collaboration and clarification to determine meaning that was an integral component of our decolonizing research design added to our study’s rigor (Whittemore et al., 2001).
Results
Eighty men and 50 women consented; however, one group of body maps from Project 1 was excluded from analysis, as the local midwife present coached the participants in what to draw. In addition, one female participant declined body mapping using pen and paper, explaining she was unable to read or write. However, she requested to map her perceptions verbally. During Project 2, 13 men out of 80 declined to start, or complete, the body mapping exercise. Half of these men stated they had other time commitments, whereas the remaining declined to verbally explain their drawings. We excluded these drawings from analysis to minimize the risk of misinterpretation. The remaining 67 body maps by men and 40 by women were analyzed.
Among the people we spoke with, biomedical knowledge about reproductive anatomy and physiology appeared limited; however, body mapping provided an effective conduit for teasing out existing indigenous perceptions. The amount of detail drawn on the body maps did not necessarily correlate with the extent of knowledge a participant had, and was often expanded during the verbal explanation. The female participants embraced this verbal-explanation phase enthusiastically. The method was effective for identifying a number of reproductive ethno-anatomical and ethno-physiological perceptions, indigenous vocabulary, and beliefs surrounding modern methods of contraception.
Insight Into Reproductive Ethno-Anatomy and Ethno-Physiology
Ethno-Anatomy
Most men identified and named the penis. A variety of terms were used with the most common being “lasan” (Tetum for “penis”). However, some men used pseudonyms such as “Jose Belo” and “Manuel,” or animal names such as “asu” (“dog”), “samean” (“snake”), red-headed snake and “mano oan” (“little bird”). Only a few male participants included the testes—these men were married, older, and had completed at least some secondary school.
Most participants identified the abdominal region as the place where the baby grows. Again, a variety of terms were used, including “oan fatin” (“baby space”), “kabun” (“stomach region”), and “kandungan” (Bahasa Indonesian for “uterus”). Men named the vaginal region in a variety of ways, from “huin” (Tetum for “vagina”) and “oin lulik feto” (“sacred place of the woman”) to “bibi” (Tetum for “goat”) and “bibisiu” (“goat meat”). Our Timorese research team members explained that context around use of terms was important, and that a term such as “goat” may be used out of shyness, politeness, or in jest. It may also have been because people knew about external genitalia by observing the animals that were evident around their homes (our Timorese team explained that in other parts of Timor-Leste, people referred to the vagina as “pai” meaning pig, as that animal was common in their area). The women most commonly described the vaginal region as “dalan bebe moris” which is literally “the path for the baby’s birth.” The ovaries were identified four times—all by women from rural areas. The “ovarium” was described variably as the place in the woman’s body where the baby grew, or the substance necessary for conception. Most men identified the woman’s breasts as important postnatally, to “give strength” to the baby.
Ethno-Physiology
Process of conception
Almost half of the men identified sexual intercourse as necessary for conception, compared with the majority of the women. Men again used a variety of terms, including “relacion sexual” (sexual relations) and “together with woman we create the new generation,” as well as “het” (Tetum for “fuck”) and “the vagina taking a direct hit.” Women defined intercourse as “sexual relations” or “man and woman joining.” Men and women from rural areas were least likely to discuss sexual intercourse, whereas more young women and women with at least some secondary schooling named this process.
Necessary components for conception
Many women identified sperm from men, whereas fewer identified an equivalent conception component from women (named variably “ovum,” “sperm,” “egg cells,” “red blood”). Women with some secondary schooling or more identified a female conception component more often. Some men, most often single men, younger men, and men with some secondary schooling or more, identified sperm from the man; however, very few identified an equivalent from women. Three of the younger men identified a man’s knees as the site of spermatogenesis, as illustrated by the body map illustrated in Figure 4. Another participant from this group explained,
When the man has been doing sex and already got many children, the knees will be shaking. Also, the knees produce the sperm. (Male Participant, 19 years old, urban area, completed primary school)
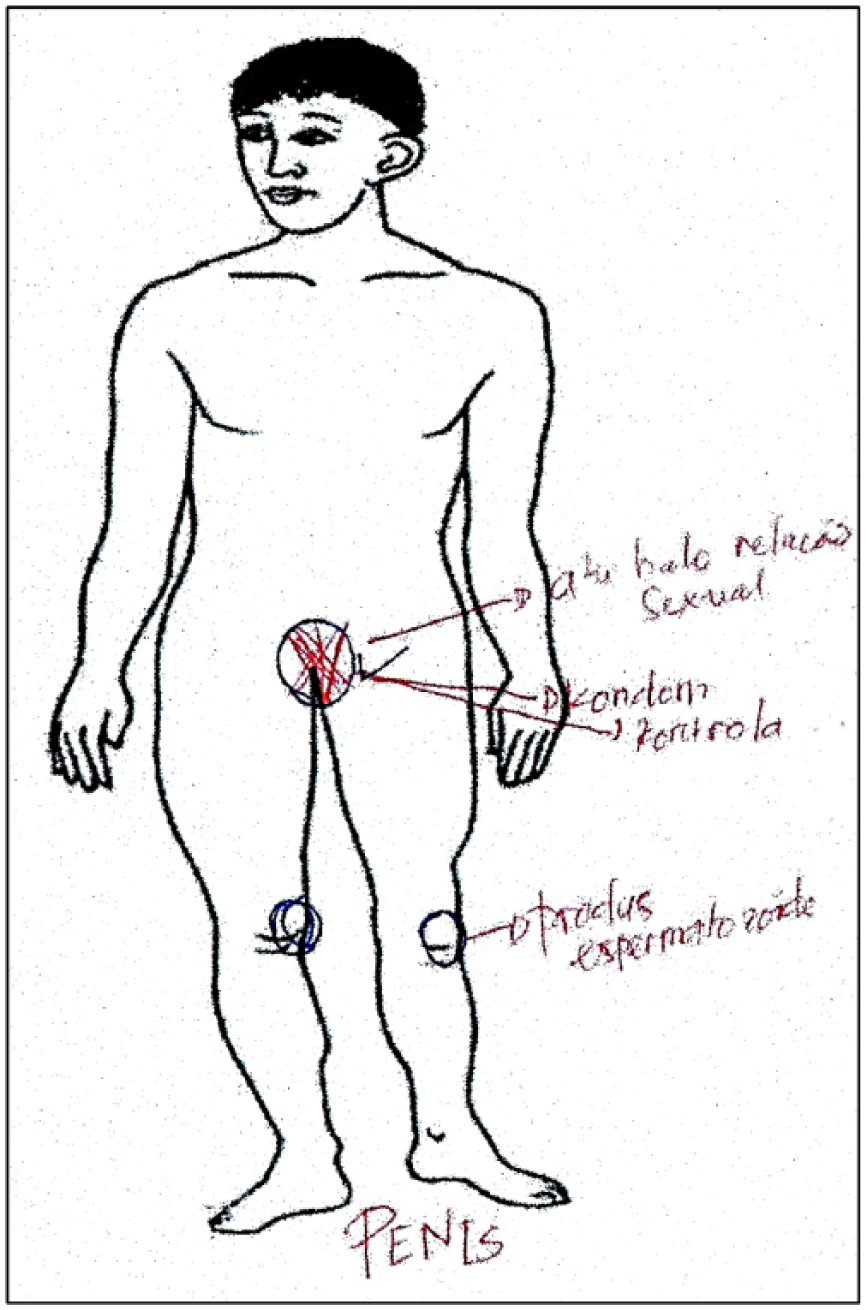
Body map completed by male Participant, 18 years old, urban area, completed secondary school.
The concept that successful conception was dependent on blood “matching” between wives and husbands was a sentiment expressed by women only. Many participants linked menstrual blood with conception, either as a necessary physiological component, or the absence of as a sign of pregnancy.
Uterine position, gestation, and movement
Some women believed that the sex of the fetus determined which side of the body the uterus was positioned during pregnancy. There was no consensus as to which side indicated which sex. A small number of men expressed this belief; however, more men believed that the baby’s sex determined the gestation of the pregnancy, with female babies perceived to require shorter gestations than males. The term “bookan” was used by a number of men to describe the small kicks and vibrations felt on the outside of a woman’s body when the fetus moves.
Modern Methods of Contraception
Overall, the participants offered limited perceptions about modern methods of contraception, and there appeared to be confusion or limited knowledge regarding method name, function, or side effects. Those methods identified were the male condom, the female condom, oral contraceptive pills (“pill”), hormonal contraceptive injections (“injection”), hormonal contraceptive implants (“implant”), and intra uterine devices (“IUD”). Many men identified the male condom, with a number naming disease prevention and/or pregnancy prevention as a recognized benefit. Those men who had received at least some secondary schooling or more, and those who were from a peri-urban location identified the male condom more often. Fewer men identified any female modern methods of contraception, with more married men than single men identifying such methods. Some men identified the ambiguous concept of “kesi” (Tetum for “to tie up”). This term described contraception in the mouth and arm—“to tie up in the mouth” and “to tie up in the arm.” The field research team was unable to determine the origins of this.
Most women identified at least one female modern method, with the injection named most often. Urban women identified a method more often than women from other areas, as did married women and women who had received at least some secondary schooling or more. Older women identified the injection more often, whereas younger women identified the implant. A minority of women, all of whom had received at least some secondary schooling or more, identified potential side effects from modern methods of contraception. These included perceptions that contraceptive methods could decrease menstrual bleeding, resulting in the uterus becoming narrow and dry, leading to difficulty conceiving in the future.
Overall, a participant’s level of schooling appeared to have the greatest influence on their biomedical knowledge of reproductive anatomy, physiology, and modern methods of contraception. Women appeared to have a greater knowledge of modern methods compared with men. Only two female participants spoke about the calendar method of family planning during the body mapping exercises, which they explained involved counting the days of their menstrual cycle to identify days of higher fertility. This may have been a result of the instructions for the exercise, whereby participants were asked to draw or locate the method on the body template, and representing the calendar method visually on a body may have been too confusing. This is a limitation of our study design.
Discussion
Our studies suggest that body mapping is an effective method to tap into indigenous knowledge and illuminate emic perceptions about reproduction, conception, and contraception. Although we found that some of these were similar to concepts found in Western biomedical explanations, others were unique or different. These emic understandings provide insight into how indigenous perceptions may influence reproductive health decisions. This may guide reproductive health service providers, policy makers, or educators, to identify the areas of need or to highlight the opportunities on which to build knowledge and strengthen links with the communities they serve, ultimately improving reproductive health service engagement and outcomes. Our findings highlight the diversity of perceptions that exist in Timor-Leste, with no single all-encompassing Indigenous worldview.
Timor-Leste is a conservative country, and discussions regarding sexual and reproductive health are often viewed as private and taboo (Belton, Whittaker, Fonseca, et al., 2009; Henfry, 2004). This was evident in our findings by the mostly respectful, polite, and nondirect ways many participants spoke about reproductive anatomy and physiology. However, the research team felt that the body mapping exercises provided a safe and reassuring space for participants to feel comfortable to share their perceptions. As with body mapping research from other parts of the world (Sturley, 2000; Zaman et al., 1998), our study provided insight into indigenous vocabulary, not only for direct translations of terms and processes, but also for concepts for which we have no equivalent in English, for example, “ovarium.” It also illuminated differences between how women and men discuss and describe reproductive anatomy and physiology. A limitation of our study was that we were unable to fully explore or understand certain concepts, and some terms were unable to be explained, for example, the term “kesi” to describe methods of contraception. Interestingly, anthropological research from Jamaica and Morocco has described similar “tie up” concepts related to blocking channels and flow within the body, therefore, preventing conception (Obermeyer, 2000; Sobo, 1993).
Although most language was gentle and polite, a small number of male participants chose to describe some anatomical and physiological concepts with different terminology. This included “Goat meat” for vagina, “red headed snake” for penis, the vagina taking a “direct hit” during sexual relations, and the Tetum word for “fuck” when describing sexual intercourse. Although this may simply be men using these words as part of their vocabulary, it may also be a small insight into the contentious arena of gender relations within Timor-Leste, where gender roles and patriarchal cultural norms shape and influence behavior and lives (Niner, 2011). However, an identified limitation of body mapping is the risk of overinterpretation (Zaman et al., 1998). Our Timorese team members explained that the context is vital, and shyness may be a significant contributing factor not only to the choice of terms used but also to the extent to which reproductive anatomy and physiology is viewed as polite to talk about. Nonetheless, it is important in reproductive health service delivery to determine what is shyness or etiquette as opposed to what is a different, limited, or gendered understanding of reproductive anatomy and processes.
Body mapping provided the opportunity to identify ethno-physiological perceptions. Many of our participants did not draw or speak about testicles or ovaries, and their biomedical function of producing sperm and ovum; rather they explained that successful conception depended on “blood-matching.” This concept has been described before in research from Jamaica, with blood’s importance linked to kinship, family, and community (Sobo, 1993). In our studies, the most commonly cited site of spermatogenesis was a man’s knees. Our Timorese research team members substantiated this, explaining that many men engaging MSTL’s services expressed this ethno-physiological perception. Research from Brazil using body mapping revealed that men believed spermatogenesis occurs in the back of one’s head or in one’s brain, with sperm transported around the body via tubes (Victora & Knauth, 2001). Similarly, a study from Nepal using body mapping with men, described similar tubes and channels within a man’s body, which are greatly affected by vasectomy (Sturley, 2000). These different perceptions are important to consider when delivering reproductive health information or services—a woman’s life may be significantly affected if she perceives her blood to not match her partner’s, therefore, negating the need for contraception.
Health-seeking behavior may also be affected by ethno-physiological beliefs regarding gestation and uterine positioning. Previous research in Timor-Leste involving a small number of women and body mapping concluded that a woman had two uteri—one for a male fetus and one for a female (Belton et al., 2009). Although participants in our study did not describe two uteri, some perceived the uterus to move from side to side depending on the baby’s sex, and some believed gestation was determined by the baby’s sex. If the woman perceived she was pregnant with a male baby due to the side of her body on which her uterus was positioned, this may influence her decision to relocate to closer proximity to a health facility, or arrange timely skilled assistance for the imminent birth of her baby. Obtaining appropriate assistance and care for pregnancy and childbirth in Timor-Leste already presents multiple challenges, without including mistimed perceptions of gestation (Wild et al., 2010).
Our findings identified many perceptions of reproductive health anatomy, physiology, and modern methods of contraception not aligned with those from a Western medical paradigm. Cornwall (1992) has argued against correcting so-called biomedical misperceptions if they are not harmful, but rather use them as foundations on which to impart new knowledge. Although we are cautious of not advocating for cognitive imperialism, that is, positioning “positivism as the only correct way of understanding the world” (Martin, 2012, p. 33), we also appreciate the need to minimize harm, especially when indigenous perceptions or knowledge may be detrimental to women’s health (Ireland et al., 2015). Advocating a Two-Eyed Seeing framework offers a respectful opportunity for an effective approach to priority setting in reproductive health. Two-Eyed Seeing offers the opportunity to weave back and forth between different worldviews, blending perspectives so as to arrive at an understanding or an approach that is best suited to that circumstance at that time for that community (Hovey et al., 2017; Marsh et al., 2015). We know from previous research in Timor-Leste that the Timorese engage with epistemological pluralism, for example, Catholicism with animistic beliefs, or traditional law with national law (Belton, Whittaker, Fonseca, et al., 2009; Hicks, 2007; Wild et al., 2010; Zwi et al., 2009). The challenge is perhaps for health service providers to reciprocate, and explore ways to successfully combine and integrate indigenous and Western paradigms to maximize health benefits—for example, MSTL who use clinical and scientific language in the delivery of their services may now integrate indigenous vocabulary and terminology alongside such biomedical language, bridging indigenous and biomedical knowledge to optimally address the reproductive health needs of a particular community.
The need for appropriate, targeted, and comprehensive sexual and reproductive health education across ages, locations, and educational categories is evident from our findings. To date, there is often limited opportunity in Timor-Leste for young people to access sexual and reproductive health information, in part due to sociocultural norms and political sensitivities, for example, the influence from the Catholic church (Richards, 2015). The confusion we found surrounding different modern methods of contraception, their actions, and potential recognized side effects illuminates for policy makers the need to focus education on this issue. Low health literacy surrounding reproductive anatomy and physiology contributes to a woman’s reluctance to engage with contraception (Hartmann, 1995; Mattson, 2010). Similarly, misinformation, myths, and suspicion of modern methods of contraception contribute to contraceptive opposition (Richards, 2010; Samandari & O’Connell, 2011). Side effects such as decreased menstrual bleeding, although accurate from a bio-pharmacological perspective, may be incredibly concerning to a Timorese woman, whose ethno-physiological belief links this decreased bleeding with “narrowing” and “drying” of the uterus resulting in difficulties conceiving in the future. When offering services or information, reproductive health providers would be advised to acknowledge women’s concerns about the impact of modern methods of contraception on their fertility, as well as remember the coercive contraception regimens of the past, and work toward allaying women’s and men’s fears, suspicion, and misunderstandings.
Our body mapping exercises overcame literacy, language, and cultural barriers allowing participants from various educational backgrounds to share emic insights and understandings. It also provided a valorized space for the participants to share their stories (Cornwall, 1992). This is of particular importance for all people in Timor-Leste, who due to their history of colonization, and more recent history of invasion and occupation, require reassurance and support to behave autonomously and with self-determination (Wigglesworth, 2012). The opportunity to have their voice heard is perhaps even more important for Timorese women, who live in a society dominated by patriarchal values and behaviors (Niner, 2011; Richards, 2015).
Despite the sensitivities of discussing reproductive health in Timor-Leste, body mapping provided a respectful and effective method that encouraged participants to share their perceptions, as well as traversing the divide between Western biomedical and indigenous knowledge. Although many of the emic ethno-anatomical and ethno-physiological ideas presented by the Timorese may be at odds with concepts found within the Western biomedical realm, in other parts of the world, and through various other emic lenses, those ideas may not seem as unique or foreign. What is important is the recognition that there are multiple ways of knowing, and having an understanding of this is essential when providing or integrating reproductive health services or information. Body mapping offers a means to gain insights that may help build bridges between indigenous and Western knowledge systems. Combining these insights with pertinent sociocultural and historical influences on reproductive health may enhance the relevance, appropriateness and provision of services and education, as well as strengthen community engagement, ultimately improving reproductive health and decreasing maternal deaths.
Limitations
Our participants had higher levels of education compared with national education attainment averages (Ministry of Finance, 2010). This may have influenced our findings. In addition, the provision of a template of a male or female body may have compelled participants to draw within the outlines, rather than include any perceptions of external or out-of-body influences on reproductive anatomy, physiology, and contraception.
Footnotes
Acknowledgements
We would like to acknowledge and thank the women and men who took part in our studies. We would also like to acknowledge and thank the three anonymous reviewers who provided insightful and beneficial feedback and suggestions for this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We declare that four of the eight authors (AIM, EC, LCM and HH) were employed by Marie Stopes Timor-Leste at the time of the research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Marie Stopes Timor-Leste (MSTL).