
Abstract
The broad spectrum of problems caused by caring for a patient with mental illness imposes a high burden on family caregivers. This can affect how they cope with their mentally ill family members. Identifying caregivers’ experiences of barriers to coping is necessary to develop a program to help them overcome these challenges. This qualitative content analysis study explored barriers impeding family caregivers’ ability to cope with their relatives diagnosed with severe mental illness (defined here as schizophrenia, schizoaffective disorders, and bipolar affective disorders). Sixteen family caregivers were recruited using purposive sampling and interviewed using a semi-structured in-depth interview method. Data were analyzed by a conventional content analytic approach. Findings consisted of four major categories: the patient’s isolation from everyday life, incomplete recovery, lack of support by the mental health care system, and stigmatization. Findings highlight the necessity of providing support for caregivers by the mental health care delivery service system.
Keywords
Severe mental illnesses (defined here as schizophrenia, schizoaffective disorders, and bipolar affective disorders) can be associated with a significant loss of quality of life (Delespaul, 2012), increased rates of mortality and physical illness morbidity (Hert et al., 2011), high levels of service use, and significant economic costs (Whiteford et al., 2013). However, it is not only the patients who experience the effects of these conditions. When the movement toward deinstitutionalization of psychiatric hospitals began (Bauer, Kunze, Von Cranach, Fritze, & Becker, 2001; de Girolamo & Cozza, 2000; Pedersen & Kolstad, 2009), and patients were prematurely discharged without appropriate community support, many families became the primary source of care for their mentally ill family members (Awad & Voruganti, 2008).
The World Health Organization (WHO) report revealed that one in four families has at least one member with mental illness and family members often become their primary caregivers. Mental illness will account for the biggest burden of care among all diseases by 2020 (Herrman, Saxena, & Moodie, 2005). In Iran, 23.6% of the population aged 15 to 64 years meets the criteria for having at least one Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) psychiatric disorder in the past 12 months (Vandad Sharifi, Hajebi, & Radgoodarzi, 2015).
Family caregivers, as the primary caregivers, usually provide physical, emotional, and financial support to their relative with chronic illness (Oyebode, 2005). Chronic illness can act as a stressor and initiates coping. It can either contribute to or hinder coping (Honey & Halse, 2006; Muhlbauer, 2002; Robinson, 2017). Therefore, after a medical diagnosis of a chronic illness, family caregivers are faced with new situations that challenge their usual coping strategies. Caregivers employ all of their emotional and physical abilities to overcome this stressful condition, and to manage the problems associated with the disease (Karp & Tanarugsachock, 2000). These strategies are defined as factors that moderate or otherwise change the causative conditions affecting on phenomena (Strauss & Corbin, 1998).
Constant care of the patients with a chronic illness, including severe mental illness, without supportive resources could lead to frustration and burden in family caregivers and influence their coping skills and quality of life (Chadda, 2014; Creado, Parkar, & Kamath, 2006; Eaton, Davis, Hammond, Condon, & McGee, 2011; Salles & Barros, 2009). On the contrary, the problems associated with severe mental illness such as patients’ isolation, passive life (Raj, 2013), and nonadherence to treatment (Martin, Williams, Haskard, & DiMatteo, 2005) can reduce their families’ energy, and consequently causing helplessness and depression in other family members, especially parents and spouses whose quality of life may be severely impaired. Importantly, to health services, this potentially leads to the family members’ resignation from the caregiving role (Caron & Bowers, 2003; Steele, Maruyama, & Galynker, 2010).
Moreover, caregivers may encounter other negative consequences of mental illnesses such as stigma, which is a potent source of distress for families (Girma et al., 2014; Shamsaei, Kermanshahi, Vanaki, & Holtforth, 2013; Thornicroft, 2008) and increases the demand for mental health professional support (Gavois, Paulsson, & Fridlund, 2006). Some families find it difficult to deal with the stigma associated with mental illness, and this negatively influences the families’ ability to cope with patients suffering from a mental illness (Karnieli-Miller et al., 2013).
Some researchers found that the cross-cultural value paradigm “individualism-collectivism” can be applied to explain attitudes to mental illness on a cultural level (Franklin, Sarr, Gueye, Sylla, & Collignon, 1996; Papadopoulos, Foster, & Caldwell, 2013; Yip, 2005). As a result, it is necessary to consider the caregivers’ experiences of caring for a person with mental illness within the context of the culture in which they live.
There has been rapid advancement in the medical care of individuals with diagnoses of mental illness. However, some studies showed that mental health professionals often ignored recent advances in psychological treatment, which could lead to recurrence and treatment failure (Judd et al., 2000; Kallivayalil, 2008) and high financial burden in the family. These negative outcomes could make the situation more difficult for families to cope with mental illness (Shamsaei, Cheraghi, & Bashirian, 2015).
Taking caregivers into the mental health system policy and in the treatment plan could affect their coping skills. Eassom, Giacco, Dirik, and Priebe (2014) and Semrau et al. (2016) have stressed the importance of considering the needs of family caregivers in the mental health system. However, the results of some studies have shown that mental health professionals ignored the family caregivers’ needs and challenges in the care process (Ae-Ngibise, Doku, Asante, & Owusu-Agyei, 2015; Navidian, Kermansaravi, & Rigi, 2012; Onwumere, Learmonth, & Kuipers, 2016; Rahmani, Ebrahimi, Ranjbar, Razavi, & Asghari, 2016; Wainwright, Glentworth, Haddock, Bentley, & Lobban, 2015).
The mental health care system plays a significant role in the development of community-based mental health services for addressing family caregivers’ challenges in coping with their mentally ill family members (Forouzan, Ghazinour, Dejman, Rafeiey, & San Sebastian, 2011). Despite the significant achievements in the mental health care delivery system in developed countries (Patel et al., 2013), the psychiatric centers in developing countries do not have sufficient resources to address family caregivers’ challenges in the care of their mentally ill patients. Furthermore, the lack of community-based services and supportive resources in low-income and middle-income countries could negatively affect the mental health needs of both mentally ill patients and their family caregivers (Rathod et al., 2017).
Although family members are a valuable resource for patients with long-term conditions and play an essential role in supporting patients (Kopelowicz, Zarate, Smith, Mintz, & Liberman, 2003) this role is more prominent in Asian health care, because cultural rules, religious beliefs, and social structure are based on family cohesion (Navab, Negarandeh, & Peyrovi, 2012). Understanding the impact of culture in the meaning of designing process in caregiving is also very important, as the meanings of some illnesses are particularly embedded with cultural meaning (Rytterström, Unosson, & Arman, 2013).
On the contrary, some studies conducted in low- and middle-income countries showed that less than 10% of mentally ill patients were hospitalized during follow-up, suggesting that there were high levels of family involvement in patient care (Chadda, 2014; Ganev, Onchev, & Ivanov, 1998). Strong levels of family bonding and the social support role of the extended family network, which are central to developing countries, could reduce the perceived burden of family caregivers (Naheed, Akter, Tabassum, Mawla, & Rahman, 2012; Ohaeri, 1998).
Coping strategies could affect caring outcomes for both patients and their families. Caregivers who adopted less emotion-focused coping strategies reported a reduction in their feelings of burden (Eaton et al., 2011; Hassan, Mohamed, Elnaser, & Sayed, 2011). Evidence also suggests that coping strategies of caregivers can affect patient’s lives, relapses, and readmission (Rosland, Heisler, & Piette, 2012). In this regard, it is now important to focus on caregivers, especially in developing countries, where there is a lack of resources to support mentally ill patients and their family caregivers (Ae-Ngibise et al., 2010).
Therefore, opening dialogue with family caregivers about the caring situation and their challenges could help the mental health care delivery system to identify caregivers’ problems (Seikkula & Arnkil, 2014; Williams, Donnelly, Holmlund, & Battaglia, 2008). Few qualitative studies have been conducted aiming at exploring barriers to family caregivers coping with individuals who have severe mental illness.
The purpose of this study was to use a qualitative research method to explore barriers to coping with people who have severe mental illness as perceived by their family caregivers. The main question of this research is as follows: What are the barriers hindering family caregivers’ ability to cope with severely mentally ill patients?
Method
Design
This study uses a content analysis approach to focus upon barriers to coping with patients with severe mental illness as perceived by family caregivers.
Qualitative studies use different methods to evaluate interesting phenomena and collect relevant data from the perspective of process owners. This makes it possible to conduct in-depth, comprehensive examination and understanding of phenomena (Corbin & Strauss, 2014). For the purpose of this study, the conventional content analysis approach (Graneheim & Lundman, 2004) was adopted to clarify barriers to coping with patients diagnosed with severe mental illness as perceived by family caregivers,
Ethics
Ethical approval was obtained from the research deputy of the Tabriz University of Medical Sciences. All of the participants were informed about the purpose and method of the study. Furthermore, they were assured of their anonymity, privacy, and voluntary engagement before signing a written informed consent form.
Participants
The setting for this research was Tabriz, one of the largest cities in Iran and the capital of East Azarbaijan Province, located in northwest Iran. A Purposive sampling method was used to recruit participants who were referred to the Razi teaching hospital affiliated with the University of Medical Sciences in Tabriz. Razi teaching hospital is located in Tabriz and is the referral center for patients with mental disorders in the East Azarbaijan province.
The sampling was continued until the data saturation was achieved through interviews with 16 family caregivers, who were recruited according to the following inclusion criteria:
i. 18 years or older with no psychiatric disorder based on their self-report;
ii. The main person responsible for providing care for their family member with a severe mental illness such as schizophrenia, schizoaffective disorder, and bipolar affective disorder without comorbidity disorders and intellectual disability, which was diagnosed by a psychiatrist;
iii. Living in the same house with them; and
iv. With at least 1 year of caring experience.
Data Collection
The data were collected using semi-structured, in-depth interviews. All interviews were conducted in the participants’ native language by the last author (F.R.). The native language of all participants’ was Turkish. The interviews were translated to the English by the expert translator prior to analysis. Interviews lasted between 45 minutes and 90 minutes and were conducted in the participants’ choice of setting (e.g., home, hospital, coffee shop).
The key interview questions in the topic guide were as follows:
i. Can you tell us about your experience of living with a patient who has a mental illness?
ii. What kind of challenges or barriers did you face in coping with your patient?
Interviews continued with follow-up exploratory questions such as “how?” and “would you elaborate?” to obtain further description of the experiences.
Data Analysis
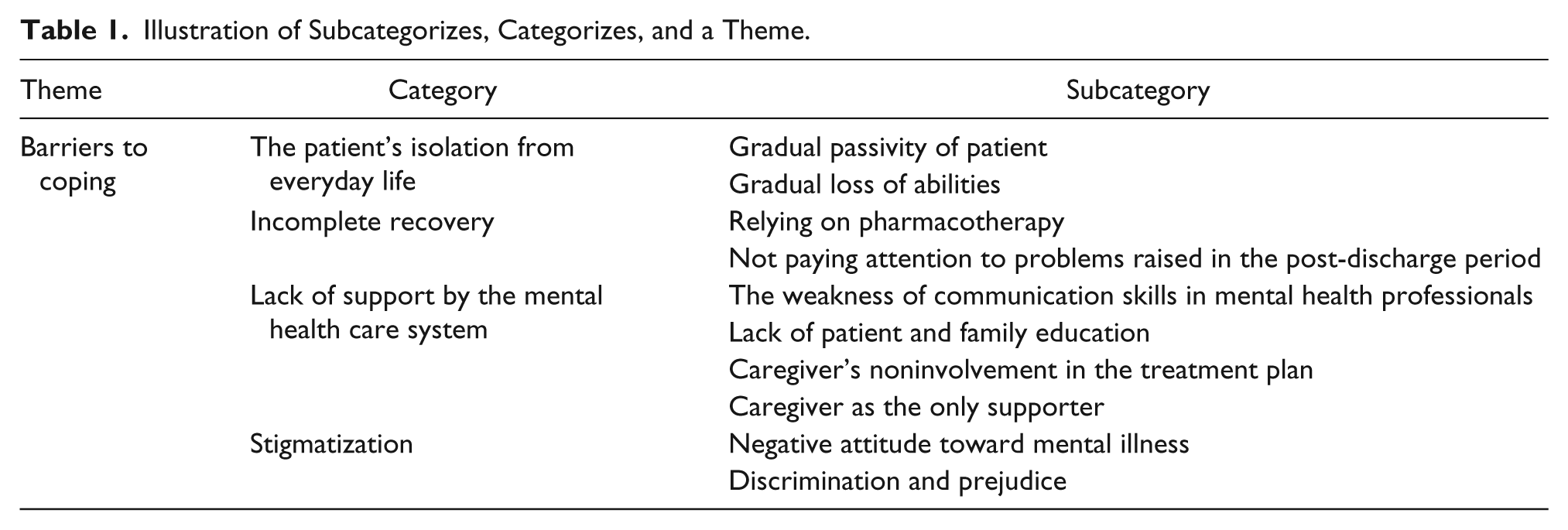
The analysis was conducted alongside the data collection, using a qualitative content analysis method, described by Graneheim and Lundman (2004). In the first step, two researchers (H.E. and F.R.[ Farnaz Rahmani]) listened independently to the recorded interviews several times to become familiar with the text. Then the interviews were translated and transcribed verbatim. In the second step, transcribed data were further reviewed to gain a holistic perspective of the participants’ experiences. In the third step, the last author (F.R.) collated the text (transcribed data) into original codes. In the fourth step, the codes were placed into subcategories based on their similarities and differences. In the last step, the categories were defined and abstracted into a theme. The last two steps of the analysis process were conducted by all researchers involved in the study. The analysis process is presented in Table 1.
Illustration of Subcategorizes, Categorizes, and a Theme.
To ensure the rigor of our analysis, four criteria including credibility, dependability, confirmability, and transferability were used (Speziale, Streubert, & Carpenter, 2011). Credibility of data was achieved through long-term involvement of the researcher with the data. In addition, four participants confirmed the compatibility of the results with their experiences. The dependability of the study was achieved through a process of external checks by two researchers who were not involved in the data analysis. The researchers documented the process of data collection and analysis procedures throughout the study. They also described the raw data, data reduction, combination, and data reconstruction precisely for achieving confirmability. To achieve transferability, a description of context, participants’ selection and demographic data, data collection, and results was presented.
Results
Participant Characteristics
In this study, 16 family caregivers were interviewed. The mean (SD) age of the caregivers was 44.6 (10.3) years. About 62.5% of them were females. A total of 57.1% were educated to high-school level. The employment status of 56.2% of participants was part-time work. Of these caregivers, 43.7% were spouses. About 62.5% of them had experienced 5 to 15 years of caregiving. There was no difference in the ethnicity of participants.
Following the content analysis, the barriers experienced by participants were identified in four categories: patient’s isolation from everyday life, incomplete recovery, lack of support by the mental health care system, and stigmatization (Table 1). These emerged in the theme of barriers to coping. The first category comprised two subcategorizes related to the gradual passivity of the patient and the gradual loss of abilities. The second category is focused on relying on pharmacotherapy and not paying attention to problems raised in the post-discharge period. The third category consisted of four subcategories: the weakness of communication skills in mental health care professionals, lack of patient and family education, the caregiver’s noninvolvement in the treatment plan, and the caregiver as the only supporter. The last category consisted of two subcategories: negative attitude toward mental illness, and discrimination and prejudices.
The patient’s isolation from everyday life
Gradual passivity of the patient
According to the experiences of the caregivers, frequent hospitalizations would make patients accept institutional life, which made them forget that they should take care of themselves. One female spousal caregiver stated how the total dependence of her mentally ill husband upon her imposes a high stress on the caregiver so life becomes very exhausting: Despite the long years of my husband’s illness, he is still unable to take care of himself. He forgot that he can do some things. He is totally dependent on us. It seems that he is accustomed to depend on someone else. I will always take care of him. Constantly . . . every moment . . . It was really bothering me. He is completely passive. No matter what’s going on around him.
Patients gradually became indifferent to what was happening around them. The patient’s passivity to the events of his own life and others caused significant problems and made life more difficult: For example in my marriage, there were situations in which he must be present. I really wanted my father to help me make a right decision or participate in ceremonies but he didn’t. He was so indifferent to do this.
Gradual loss of abilities
The patients slowly lost their abilities to perform daily activities such as bathing, eating, or dressing which led to a tremendous burden on the family. A sister caregiver commented on how the patient gradually becomes incapable over time, which has led to burnout and resentment in the family: She lost her energy and motivation to do anything over time, and we couldn’t do anything about it. It was so painful for the whole family to continue this way.
The caregivers reported that their patients could not work or return to their previous work, and consequently the family experienced a high financial burden. One spouse caregiver reported her experience: When he got better, he could no longer go back to his work; he was no longer hired and wasn’t allowed to work there again. It was a disaster for the whole family. Moreover, he can no longer perform paternal duties or assume his responsibilities as before.
Incomplete recovery
Relying on pharmacotherapy
According to the participants, overreliance on medication leads to neglect of other forms of mental health treatment and incomplete treatment of patients. Patients who are not yet completely cured are returned to the family, which causes more stress in family caregivers. Most of the time, caregivers do not know what to do. Patients’ conditions confuse all the individuals involved in caring. One spouse described her challenges as follows: When he’s there (psychiatric hospital), we think that he should be treated. But when he’s back home, it seems like something is missed. We can’t expect too much from him. They (mental health professionals) insist that he should be discharged and we have to take care of him at home. They believe he’s ok and cured but he’s not. After all, we have to hospitalize him again.
Caregivers felt that the treatment plan for patients should not only include medication: They only prescribed him some pills. But I believe that medicine is not enough. This treatment method is definitely wrong.
Another father as a caregiver argued for what he expected from mental health professionals: When he got sick, our only hope is taking him to the hospital. We didn’t know what to do. We expect that he becomes well or at least doctors do something to treat him. But when we come back to take him home, we notice that his illness situation has not changed much . . . Doctors insist on discharging him but I am sure that his illness will get worse at home. This is the 28th time that we hospitalize our 34-year old son.
The caregivers stated that they wish to receive more special treatment both for their mentally ill family members and themselves. However, the mental health professionals did not give importance to other treatment approaches. Furthermore, psychiatrists tend to have a biological approach to mental illness, which ignores other dimensions of treatment: There has been a lot of progress in the science of treating diseases. It’s impossible that I believe the only way to treat mental illness is just a few pills. It is not true. They do not care about the other dimensions at all.
One mother caregiver shared her experiences: Well, my daughter has suffered from depression due to problems in her marital life. We also admitted her to treat her illness. They did not even pay attention to the fact that it was due to her marriage problems. She was admitted to the hospital for several days and was discharged with only a medical prescription. The main problem was still unresolved. They did not care.
Not paying attention to problems raised in the post-discharge period
Although pharmacotherapy was the most common treatment modality in the clinical setting mental health professionals did not pay attention to how patients take drugs in the post-discharge period. The caregivers stated that there was no planned strategy (such as follow-up programs) for patients to prohibit noncompliance in the post-discharge period. One male spousal caregiver stated, In the hospital, she uses her pills out of fear of punishment. And it is completely different at home. First of all, she throws her pills away and never listens to us. Whenever she stops her treatment, she loses control of her behavior and does whatever she likes. We have to deal with it, but it is so exhausting. This leads to a relapse and we’re forced to hospitalize her again. How do I make her realize that she might be harming herself by not taking the medications? I fully explain it to them (psychiatrists) but they did not care about it.
The patients diagnosed with mental illness have been shown to be partially or totally lacking insight into the presence of their mental disorder, which could cause more distress for families. One caregiver mother stated how the lack of her patient’s insight into the illness caused the upset in the family: He didn’t think of himself as a family member who has a mental illness. Despite all the quarrels, he even thinks he’s the best and strongest person. So, we are really helpless and desperate. Sometimes situations get so messy that there’s no choice for us but to hospitalize him again. Is there really no way to make him accept his illness? It is intolerable to live with him.
One female spouse caregiver stated, He thinks that he is healthy. Whenever we take him to hospital, he gets angry and hates us and when he comes back home, he revenges. It is really frustrating. He never accepts that his behavior is just because of his illness.
Some caregivers reported that they wanted the mental health professionals to pay more attention to their problems: I ask them (psychiatrists or psychologists) to talk with my husband about nonviolence with family members after discharge and to teach him how to control the anger. My husband is very furious and nervous. He is skeptical, always questioning me and the children. I want the doctor to explain how to react to my husband in these situations. He did not pay much attention to this issue.
Lack of support by the mental health care system
The weakness of communication skills in mental health professionals
According to the caregivers’ experience, the mental health care team including the psychiatrist, psychologist, and psychiatric nurse usually did not listen to them seriously and did not care to communicate with them. There was a lack of relationship between the mental health professionals and family caregivers. One daughter caregiver explained how the lack of relationship with the psychiatrist made her feel so lonely: The psychiatrist had no idea what my caregiving problems are and how I deal with them. My mother was severely depressed. She didn’t talk to anyone and eat anything. These are not important to the psychiatrist. I was deeply upset when I came home from the hospital on the first night because I felt so helpless.
According to the participants’ experiences, mental health professionals did not give patients and their families enough time to ask questions. For family caregivers, their contact with mental health professionals is limited to meetings during office visits or admission periods. A father as a caregiver expressed his concerns: There are strict rules in the hospital that do not allow you to get in touch directly with a psychiatrist, so there’s a real barrier. In the visit room, there are always many students and others and I do not like to ask any question in their presence. Moreover, they are always busy; they do not have enough time to answer my questions.
Caregivers’ noninvolvement in the treatment plan
Mental health professionals did not listen to and include family caregivers in their mentally ill relative’s treatment and care plan. Family caregivers felt that they were excluded from treatment decisions and the care-planning process. Their questions were not taken seriously by the mental health professionals in the clinical setting. One father as a caregiver stated in this regard, I think the decisions are made without us (the father and his daughter), and then we are invited into the ward as a token. Their decision is one-sided. I cannot give my opinions or interference because the decision is made and whatever I say will not change it.
Noninvolvement of the family caregivers in the treatment plan could have other negative results such as lack of knowledge of how to care for mentally ill family members at home after discharge. A mother caregiver stated in this regard, I want to take part in the treatment plan of my son, but no one takes me seriously. It seems that the plan has already been set. I am like a stranger to them. Who cares me? What should I do after discharge?
Lack of patient and family education
According to the caregivers’ experiences, mental health professionals did not pay attention to their educational needs. The family caregivers did not know the nature of their loved ones’ mental illness, nor do they know what medications their patients take and what side effects they may have. They were dissatisfied with the information provided by mental health professionals on how the illness would develop in the long term or how they would be able to manage their patients when they are in a critical condition. A caregiver mother stated, No one has ever spoken to me about my daughter’s illness or explained anything to me yet. I don’t understand what is going on. They (health care team) are always too busy to give me an opportunity to share problems with them. What should I do if her symptoms recurred?
They expressed an obvious desire to learn more about their loved one’s illness, care, and treatment. Regardless of the mental health professionals being a key source for providing information, participants were still ignored. One male spouse caregiver expressed his experience: I did not know how to take care of her when she was discharged. I still do not know much about it. No one tells us anything. I want to know more about my wife’s disease. I also think that the training sessions are very helpful for us. Even my wife and I want to know more about her illness but no one takes us seriously or cares about this issue.
Furthermore, the participants stated that they became caregivers unintentionally, without preparation, knowledge, or familiarity with its tasks. A female spousal caregiver stated, I did not already know that such a horrible thing would happen in my life. I was not ready for it but I must accept it.
Caregiver as the only supporter
The caregivers stated that they thought of themselves as the only caregiving source for their family member. They were forced to bear the burden of care for a patient with severe mental illness along with other responsibilities and tasks due to lack of support resources in society. They had to accept the caregiving role to continue their lives and to try to preserve the integrity of the family. They have handled the problems by their own. They also perceived themselves as being ignored, or uncared. One female spousal caregiver shared her experiences, I’m the one who should manage all of these. Who would help me out? The government doesn’t help. The hospital doesn’t care how to provide care for my husband. No help, no advice . . . nothing ma’am, nothing. There is no support when we are in crisis. I perceive myself as being abandoned in the caregiving role.
On the contrary, the lack of financial support, high costs of treatment, frequent relapses, and readmissions were the biggest barrier to dealing with mental illness. Another female spousal caregiver stated in this regard, The most important issue is the financial problems . . . The medical insurance support is here to make the process simple and easy for us, however, costs are very high.
Another male spousal caregiver shared his work problems caused by constant caregiving and lack of support: Sometimes I have to work less to manage my family matters, and ultimately I have to work fewer hours than desired. In the end, I get less pay and with all this extra cost, I’m really helpless. I wish that there would be rules that support us in such cases.
Stigmatization
Negative attitude toward mental illness
Experiences of stereotyping engendered reactions that caregivers received from people of the community. The main reason that they did not disclose the illness of their relatives and isolated themselves from public view was their fear of being negatively judged by people. One daughter caregiver stated, I can’t tell anyone. They think differently. Their judgment is not good about mental illness. They’d think of him as a lunatic. A dangerous person who must be left alone and never trusted. As if he has a contagious disease. For people, a mentally ill person is like a murderer or retard or even something worse. Unfortunately, their attitude toward this illness is not good. This makes life very difficult for us. We can’t deal with it. People think I’m not normal either because I live with a mentally ill father.
The caregivers noted that they preferred to hide the mental illness of their family members due to fear of public negative reaction to them. One female spousal caregiver stated, You know I prefer to participate alone in the parties or ceremonies. I don’t like to go with him. He gets bored and doesn’t like to talk a lot. I can’t bear people who make judgments and label him. I can’t bear people who stare at him as well. It is better to hide his illness from people. Their attitude toward this illness is very negative.
Discrimination and prejudice
Discrimination and prejudice act as major barriers to caregivers in seeking help from others. They experienced the negative consequences of discrimination both for themselves and their patients such as isolation, ridicule, and incivility. The amount of discrimination and prejudice that they experienced was so powerful that they perceived it more destructively than the illness itself. One brother caregiver stated, I’m aware of others’ behavior and always tries to hide his illness, like when he should go to his children’s school I’ll go instead. No one socializes with us; it’s like they’re afraid of us and treat us differently. This has made our life very hard.
For caregivers, shame is a consequence of living with a mental illness, especially in the face of ongoing stigma. One mother caregiver stated, My son has been sick for 5 years. I’ve always felt embarrassed by his behavior and his hospitalization in the psychiatric hospital. When my colleagues realized, they asked if my child was really hospitalized in a psychiatric hospital. I’m embarrassed by their behaviors. I don’t want anyone to know.
Discussion
To the best of our knowledge, this is the first qualitative study based on a content analysis approach, which presents barriers to Iranian family caregivers’ coping with a family member who has a severe mental illness diagnosis. The experience of family caregivers was illuminated in the four categories: the patient’s isolation from everyday life, incomplete recovery, lack of support by the mental health care system, and stigmatization.
Living with a mentally ill family member has been perceived as a highly stressful situation for family caregivers who participated in this study. They reported that mental illness has caused interruptions in the daily lives of their patients, resulting in gradual passivity and the gradual loss of abilities in them. Furthermore, it induced high stress in the family caregivers and led to a barrier to coping. This is consistent with other studies reported that as the level of patients’ functioning decreases, maladaptive coping strategies increase (Creado et al., 2006; Raj, 2013; Salles & Barros, 2009).
According to participants’ experiences, their mentally ill family members became gradually dependent on caregivers. It made life very hard for them and limited their normal lives. In this regard, Yasemi, Hajebi, and Bagheri (2006) pointed out that custodial care for patients limited access to the outside world in a psychiatric hospital and organizing patients’ lives by the institutional routine led to patients’ passivity and separation from the life process.
Although psychiatric services have changed from large psychiatric hospitals to community-based mental health services for patients and their families in most developed countries (Bauer et al., 2001; de Girolamo & Cozza, 2000; Pedersen & Kolstad, 2009) psychiatric hospitals are considered the only centers for the treatment of mentally ill patients in some low- and middle-income countries. There was a serious lack of rehabilitation programs in these hospitals to prepare patients for returning to the community or living with their families (Foruzandeh & Parvin, 2013; Karim, Saeed, Rana, Mubbashar, & Jenkins, 2004; Nizamie & Goyal, 2010; Shamsaei, Cheraghi, & Esmaeilli, 2015).
A growing body of evidence suggests that the combination of pharmacological and psychological treatment has a positive effect on patients’ recovery, hospitalization rate, compliance with medication (Pfammatter, Junghan, & Brenner, 2006; Pharoah, Mari, Rathbone, & Wong, 2010; Bäuml et al. 2006), and quality of life (Bobes, Garcia-Portilla, Bascaran, Saiz, & Bouzoño, 2007). However, family caregivers in our study reported that there was no psychotherapeutic treatment approach in the treatment plan of their mentally ill relatives. According to their experiences, absolute reliance on pharmacotherapy rather than other therapeutic approaches leads to incomplete recovery of patients. In this regard, Kallivayalil (2008) and Judd et al. (2000) found that overreliance on medication without considering other treatment approaches can lead to relapse and readmission. They emphasized psychotherapy as an essential part of the patient’s treatment plan, especially when drugs do not seem be sufficient alone. Furthermore, consideration of mental illness as a multifactorial disorder, which affects all aspects of a person’s life, confirms the importance of considering other treatment approaches along with pharmacological treatment in the treatment plan for patients with severe mental illness (Butler, Chapman, Forman, & Beck, 2006; Dobson et al., 2008). Lobban et al. (2013) also concluded that the most frequently used family interventions, which have a positive effect on patients and their families, were psychoeducation, problem-based behavior management, and emotional support.
On the contrary, family caregivers reported that patient’s nonadherence and unawareness of the disease were certain problems that were raised in post-discharge periods and were ignored by mental health professionals. Patients’ nonadherence could be a pervasive threat to the health of all patients with chronic disease, which could lead to recurrence and frequent readmission and impose a high economic burden on the family (Martin et al., 2005). Although evidence emphasizes the importance of posthospital discharge programs to achieve continuity of care there was no follow-up or plan to address the patient’s problems, which increase in post-discharge period (Bäuml et al., 2016; Mizock, Russinova, & Millner, 2014; Rahmani et al., 2016). Therefore, there is a gap between the actual needs of patients and their families and the routine care of people with severe mental illness in some mental health care delivery systems (Matsuda & Kohno, 2016; Navidian et al., 2012).
The caregivers of this study experienced a general lack of support from mental health professionals and perceived themselves as being abandoned in caregiving roles. Their major complaint was the lack of relationship between them and mental health professionals. This issue has also been discussed in other studies in which family caregivers were dissatisfied with the information, advice, and support received from the mental health professional (Doornbos, 2002; Gavois et al., 2006; Shamsaei, Cheraghi, & Esmaeilli, 2015). Wainwright et al. (2015) argued that despite the setting of priorities for supporting family caregivers, many families of people experiencing mental illness continue to feel unsupported by the mental health system. They concluded that improved support, supervision, and training are required for staff to deal with relatives’ distress and their mental health problems.
Participants reported that mental health care professionals do not care about communication skills with the family. This was also reported in another context where mental health professionals’ negative attitudes toward communicating with families impeded effective communication with them (Rowe, 2012). Heru (2004) also found that communication with respect and compassion, along with willingness to listen, promotes a collaborative working alliance with the patient and family. They conclude that continuing professional education can serve mental health professionals, and help ensure that they maintain their knowledge and awareness in managing family interactions and providing interventions to support family caregivers. Therefore, working with families should be emphasized in undergraduate mental health training (Mansouri Alirezaie, 2009; Stiberg, Holand, Olstad, & Lorem, 2012).
According to our participants’ experiences, one of the main reasons for the lack of relationships between family and mental health professionals was high workload in their work process, which requires more attention to the existing working conditions in the mental health system (Javanbakht & Sanati, 2006).
Participants in this study had a great desire to participate in the treatment of their family member patient. However, they were excluded from their patients’ treatment plans. Glick, Stekoll, and Hays (2011) highlighted the positive results of family caregivers’ involvement in mental health care planning. Eassom et al. (2014) also argued that organizational cultures and paradigms can limit family engagement. They suggested that effective implementation seems to work through a coordinated effort by the whole team at every level of the organization, supported by strong leadership, where family work is considered a shared goal of all members of a clinical team and/or mental health service, including the leaders of the organization.
Semrau et al. (2016) conducted a systematic review of the experience of the service user and caregiver involvement in the mental health system in low- and middle-income countries. They reported service user and caregiver involvement at service-level in relation to the delivery of services such as self-help and support groups rather than at systems-level (e.g., at policy, planning, monitoring, or evaluation-level). In the study by Malakouti et al. (2009), it was found that the consumers’ family members (CFM) as case managers are able to provide follow-up treatment services at home for individuals with severe mental illness. As the result, the involvement of family caregivers in treatment and considering them as partners in care may be more useful for the patients, families, and the mental health system. However, there is a lack of a formal program that addresses the caregivers’ needs in the mental health system of Iran (Forouzan et al., 2011).
What was most striking in the participants’ experiences was that they were thrown into caregiving without any preparation, while having a lot of questions and uncertainty about their caregiving role. This is similar to other findings on the lack of readiness of Iranian family caregivers in caring for their relatives with chronic illness (Hashemi-Ghasemabadi, Taleghani, Yousefy, & Kohan, 2016; Shamsaei, Cheraghi, & Esmaeilli, 2015; Shamsaei et al., 2013). This finding was reported in other contexts in which caregivers have experienced a lack of understanding of their relatives’ symptoms and a long process of learning how best to cope with them (Onwumere et al., 2016; Wainwright et al., 2015).
Despite the major role of family caregivers in providing care for patients with chronic illness (Navab et al., 2012), family caregivers’ involvement should be prioritized across all levels of health care provision. However, there is no comprehensive and planned program to support them in clinical and community settings in Iran (Abdollahpour, Noroozian, Nedjat, & Majdzadeh, 2012; Masoudi, Abedi, Abedi, & Mohammadianinejad, 2014). The family, who provides care for patients, needs as much support as the patient does (Kulhara, Chakrabarti, Avasthi, Sharma, & Sharma, 2009). The policy makers should, on one hand, find a balance between shifting responsibilities to family caregivers and involving families in the treatment plan and on the other hand, providing them with support resources both in the clinical setting and community (Ae-Ngibise et al., 2015).
The financial strain was another barrier experienced by our participants, which is also often reported in other studies (Greenberg, Fournier, Sisitsky, Pike, & Kessler, 2015; Shamsaei, Cheraghi, & Esmaeilli, 2015). Lai (2012) stated that caring for an individual with a chronic illness requires notable financial support because of the recurrent nature of the disease. Therefore, medical insurance may not cover certain types of treatment or medications, which could result in financial burdens. On the contrary, most of the participants were working part-time, which could cause further financial problems. According to Moradi-Lakeh and Vosoogh-Moghaddam (2015), one of the main objectives of Iran’s health sector evolution program, launched in 2014, was to reduce the cost of health care for patients and their families. There are some gaps, also perceived by participants in this study, in its policies to support family caregivers of chronically ill patients. Therefore, it requires more attention to implement reforms thoroughly in all parts of the health system (Heshmati & Joulaei, 2016).
Furthermore, the strength of the extended family system and collectivist culture (Hsueh, Hu, & Clarke-Ekong, 2008), which are two of the main characteristics of the society in developing countries, play an essential role in the constant care of a member of the family with chronic illness. Consequently, most of the people with mental illness from these families are staying in a family that surrounds and provides them with adequate care. Recent studies have also suggested that extended family networks and collectivist culture can reduce the perceived burden of care (Ganev et al., 1998; Kurihara et al., 2000; Naheed et al., 2012; Ohaeri, 1998). Nevertheless, in contradiction to the findings in these previous articles, the participants in this study felt isolated and abandoned. It may be explained by the fact that the destructive nature of mental illness and its specific problems, which arise in the care process, led to further isolation and exclusion in them. Therefore, extended families and friends support, which is often emotional support, could have less impact on it. The family caregiver has remained a neglected lot, often ignored by the mental health professionals. Hence, it is important to take care of the needs of the family caregivers. It seems that the mental health system should address caregivers’ specific needs in the care process to help them overcome their problems.
Stigmatization was perceived as a strong barrier to family caregivers’ coping in this study. They reported that the public negative judgment against mentally ill patients and their families led to discrimination between employers’ recruitment practices, social support loss, social stigma, and social restrictions. These findings are in agreement with other studies showing that negative thinking about people with mental disorders and their families may be even more of a barrier to coping (Chien, Yeung, & Chan, 2014; Girma et al., 2014; Heflinger, Wallston, Mukolo, & Brannan, 2014; Karnieli-Miller et al., 2013).
Lauber and Rössler (2007) argued that compared with Western societies, in Asian countries there is a more widespread tendency to stigmatize and discriminate against people with mental or emotional disabilities, as they are considered aggressive and dangerous, which increases their social distance. It seems that one of the main reasons for this difference is cultural background. Seeman, Tang, Brown, and Ing (2016) also found that the tradition, culture, and access to education and health care all form the public perceptions of mental illness. Therefore, stigma reduction strategies may vary according to the contextual factors including socioeconomic status, politics, religion, culture, and media (Hanafiah & Van Bortel, 2015; Sewilam et al., 2015).
The mental health system can play a critical role in setting up and developing anti-stigma interventions (Thornicroft et al., 2016). However, Soltani, Moayyeri, and Raza (2004) reported that health policy makers in low- and middle-income countries usually place a higher priority on infectious conditions, especially those that result in high mortality. Another significant challenge for anti-stigma activities in low- and middle-income countries is the pervasive low level of mental health literacy. Nongovernmental organizations (NGOs) focusing on mental health are few. For example, Taghva et al. (2017) found that there are very few NGOs in Iran, and they do not play an active role in stigma reduction.
According to participants’ experiences, members of the general public did not agree that certain mental illnesses exist or that they can be treated. They perceived mentally ill patients as being lunatic or even dangerous people. Gureje, Olley, Olusola, and Kola (2006) and McDaid (2008) suggested that it is necessary to develop approaches that improve knowledge about mental health and mental disorders, and promote explanatory models that support best practice interventions. Therefore, more culturally sensitive and contextual studies are needed to evaluate specific conditions and appropriate strategies in different countries.
On the contrary, family caregivers in this study had similar experiences about caring. It seems that they could develop their own strategies and abilities through sharing their difficulties and becoming more resilient. Some studies have shown that promotion of self-help and support networks within the families who care for a member with mental illness can help them become more resilient (Coldwell, Meddings, & Camic, 2011; Greeff, Vansteenwegen, & Ide, 2006). So, developing NGOs in Iran could be considered as a potential protective factor against negative outcomes of caring for a mentally ill family member.
Our analysis has further limitations. First, the generalization of this study is limited by a small and self-selected sample from one metropolitan city in Iran. Second, the limited diversity of participants’ ethnicity may be another limitation. So, the findings cannot be extrapolated to other geographic areas, populations, and communities with more ethnic diversity. We recommend that future research be undertaken with a larger sample consisting of a diverse sociodemographic background for better understanding of the barriers perceived by families that affect their coping with their relatives with mental illness.
Conclusion
The findings show that there is a gap between the actual needs of patients and their families and the policies and priorities of the mental health system. This creates barriers for family caregivers to deal with their mentally ill relatives. An unsupportive mental health system increases caregivers’ concerns and stress, which could lead to a high burden and the failure of families to cope. Furthermore, the serious lack of supportive resources in the clinical settings and community, the lack of mental health professionals’ communications with families along with excluding family caregivers from the patients’ treatment plan has created barriers that prevent family caregivers from coping. It is strongly recommended that mental health professionals use a combination of other therapeutic approaches along with pharmacotherapy, involving caregivers in the patient’s treatment plan and planning programs to reduce the stigma associated with mentally ill people and their caregivers (see supplementary appendix for more detailed information about demographic charectristics of the participants).
Footnotes
Acknowledgements
This article has been extracted from a Nursing PhD dissertation with Ethic Committee Number TBZMED·REC.5825. The authors appreciate the research deputy of Tabriz University of Medical Sciences for their financial support. They are also deeply grateful to staff working in psychiatric wards of Tabriz Razi teaching hospital and all families who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Grant TBZMED·REC.5825 from the deputy of research in Tabriz University of Medical Sciences.
Supplementary Material
Supplementary material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.