
Abstract
There is a call for drawing on client voice to provide a rich, nuanced understanding of factors influencing substance treatment engagement as to maximizing treatment benefits. We interviewed 60 clients in a short-term inpatient substance treatment program and examined facilitators and barriers to treatment engagement. Thematic analysis yielded four themes, including perceived treatment needs, trust and counselor rapport, peer inspiration, and organizational factors. Perceived treatment needs serve as both a facilitator and a barrier wherein the acknowledgment of needs led to greater treatment engagement whereas a lack of perceived needs hindered treatment engagement. The establishment of trust and counselor rapport and peer inspiration facilitated treatment engagement. Clients rated several organizational factors including a lack of treatment provision, gender-responsive treatment and infrastructure, and ineffective communication with nonclinical staff as barriers to treatment engagement. Clinical implications include enhancing treatment motivation and counselor rapport, establishing gender-responsive treatment programs, and providing trainings for staff.
Keywords
While acknowledging the effectiveness of substance abuse treatment (Greenfield et al., 2007; Prendergast, Podus, Chang, & Urada, 2002) for those whose recurrent use of substance causes clinical and functional significant impairment and failure to meet social functions (American Psychiatric Association, 2013), researchers have been striving with the mission to inform the public of practices that improve the delivery of treatment services and maximize treatment benefits, particularly given an increasing emphasis on tightened government budget, cost containment (Prendergast et al., 2002), and wise personal investment. However, premature treatment dropout has been deemed as a major barrier to maximizing therapeutic benefits. The rates of dropout range from 20% to 70% for inpatient programs (Rabinowitz & Marjefsky, 1998; Stark, 1992; Wickizer et al., 1994), and the first month of treatment is often a critical stage for successful treatment (Stark, 1992). Thus, treatment engagement, currently defined as treatment participation and positive treatment experience, is particularly worth attention given that it is one of the best predictors for favorable treatment outcomes (Broome, Knight, Hiller, & Simpson, 1996; Drieschner & Verschuur, 2010). Using a qualitative research method, the current study is intended to explore factors that hinder or facilitate treatment engagement in a short-term inpatient substance treatment program, the findings of which would shed light on practical implications in the interests of treatment planning.
Quantitative Research on Treatment Engagement
Numerous quantitative studies have explored a variety of factors that are associated with treatment engagement. A relatively old yet relevant study on substance treatment engagement with a sample of clients in an outpatient program in the United States revealed that, instead of client characteristics, the perceived utility of treatment, the availability of ancillary services, and client–counselor relationships predicted treatment engagement (i.e., operationalized as treatment intensity multiplied by the duration of treatment; Fiorentine, Nakashima, & Anglin, 1997). Another study conducted in the United States found that clients in community-based treatment programs with a higher level of met needs tended to stay longer in treatment (Hser, Polinsky, Maglione, & Anglin, 1999), which implies better treatment provision leading to treatment engagement. A more recent study with a sample of chronic substance users in six therapeutic communities in Australia found that autonomous treatment motivation was positively associated with treatment engagement (e.g., self-reported treatment participation), better psychological well-being at the initial stage of treatment, and autonomy support from therapeutic staff (Klag, Creed, & O’Callaghan, 2010). Similarly, several studies have shown that the therapeutic relationship is positively associated with treatment engagement and favorable treatment outcomes (Meier, Barrowclough, & Donmall, 2005; Simpson, Joe, Rowan-Szal, & Greener, 1997). Although the aforementioned studies based on quantitative methodologies are informative, more research is needed to obtain more detailed accounts of important factors that lead treatment engagement from treatment receivers, the concept of which has been included in the current study.
The literature indicates that client engagement is also influenced by organizational factors. Simpson and colleagues (2009) conducted a multisite, large-scale (1,539 clients and 439 counselors from 44 treatment programs) study in United Kingdom and found that client participation and client-rated counselor rapport were associated with staff ratings of professional attributes (e.g., staff growth, efficacy) and program atmosphere (e.g., stress in work). Similarly, using data from 115 outpatient programs across nine U.S. states, a study found that staff stress negatively predicted client engagement (Landrum, Knight, & Flynn, 2012). Another study using a sample of 249 treatment staff in the United States revealed that higher staff turnover was associated with better client treatment outcomes (i.e., less involvement in illegal activity and lower social risk; Garner, Hunter, Modisette, Ihnes, & Godley, 2012); the authors suggested that a high turnover would allow for effective utilization of staff reshuffling, particularly for those who were more willing or able to implement treatment innovation, which led to more positive outcomes. In addition, some old but important studies (Hubbard, Craddock, Flynn, Anderson, & Etheridge, 1997; Simpson, Joe, & Brown, 1997) using the U.S. national-sample data also revealed that treatment modalities (e.g., outpatient methadone, long-term residential, outpatient, and short-term inpatient programs) might impact treatment outcome and longer treatment programs (at least 3 months) tended to yield better treatment outcomes than did shorter programs. However, there is a lack of research investigating the difference on treatment engagement between different treatment modalities, which again suggests a great research need on factors influencing substance treatment engagement.
The aforementioned studies imply a complicated nature of substance treatment in which client treatment experience and engagement are influenced by multiple agents (e.g., client, counselor, program manager; Flynn, Knight, Godley, & Knudsen, 2012). The interpretation of a complex matter of perceptions and actions (such as, acceptability of treatment services and treatment-seeking behaviors) warrants knowledge that is socially and culturally constructed in meaningful interaction with people and things (Angen, 2000; Fried, Harris, Eyles, & Moshabela, 2015), which is often queried by qualitative research (e.g., Fried et al., 2015; Quintero, Lilliott, & Willging, 2007). Thus, the research on client engagement may benefit from alternative methodologies, such as qualitative methods, that suffice the exploration of behaviors in a complex context (Haggis, 2008; Holloway & Todres, 2003; Laudet, 2007; Laudet, Stanick, & Sands, 2009; Laudet & White, 2010; Orford, 2008; Orford, Hodgson, et al., 2006; Orford, Kerr, et al., 2006; Parkman & Lloyd, 2015; Sofaer, 1999).
The Importance of Qualitative Methods in Understanding Treatment Engagement
Despite qualitative research adding to an in-depth understanding of factors associated with treatment engagement, there is less research using qualitative paradigms in this area compared with quantitative methods. Orford (2008) suggests that the addiction field often fails to incorporate the patient’s point of view, instead relying on experimental or quasi-experimental designs. He calls for qualitative, patient-centered explorations that provide a richer, yet no less valid picture of recovery experiences. Despite the increasing attention, only a few qualitative studies have illuminated the complexity of treatment engagement.
A qualitative study using 12 women who were between the second and fourth weeks in an intensive outpatient program in a rural area in the United States revealed that, in addition to program structure and content, interpersonal factors (experiences with staff and treatment peers) were critical factors for the level of comfort, which is an indicator for positive treatment experience (Godlaski, Butler, Heron, Debord, & Cauvin, 2009). Likewise, a recent study using focus groups found that agencies with the provision of concrete support (e.g., diapers, birth control, temporal housing payment assistance, transportation), advocacy, and emotional support facilitated treatment engagement (Seay, Lachini, DeHart, Browne, & Clone, 2017). Based on narrative texts provided by 327 nonprofit addiction treatment agencies (the majority of which were free-standing substance treatment programs) in the United States, qualitative analysis revealed that poor staff engagement with clients, burdensome procedures and processes, difficulties addressing the complex lives and needs of clients (e.g., child care needs, limited resource), and problems with infrastructure (e.g., inadequate facility) were associated with a lack of client engagement (Ford et al., 2007). A mixed-methods study with 22 clients and 22 counselors from two outpatient programs showed that clinicians tended to attribute treatment dropout to client-level factors (e.g., a lack of motivation and support from family, physical or mental health issues) more than did clients; focus group data from clients and clinicians indicated that a lack of working alliance with staff and a lack of motivation were major reasons for dropout (Palmer, Murphy, Piselli, & Ball, 2009). Another study interviewed mentors, clients, and counselors involved with an alcoholism treatment program to uncover two groups of people with either overengagement or underengagement in mutual aids and emphasize the importance of maintaining a balance between treatment and life outside of treatment for holistic recovery (Parkman & Lloyd, 2015); the findings had implications for program-related strategies to sustain treatment benefits.
In summary, addiction researchers have called for more in-depth, nuanced, and multiple-perspective accounts of treatment engagement (Flynn et al., 2012; Laudet at al., 2009; Orford, 2008; Orford, Hodgson, et al., 2006). Hence, a robust examination of treatment engagement stipulates a qualitative approach to discovery. In response, the current study recounts on clients’ experiences as a helpful source of information about how they are engaged in treatment.
Current Study and Research Site
Using a sample of clients in a short-term inpatient facility, the current study used semistructured one-on-one interviews to investigate treatment engagement, during a period between treatment intake and discharge, with the perspective unfolded by clients, who are essential to the dynamic process of treatment delivery (Orford, 2008). More specifically, the current study explored client-identified factors in the following three aspects: (a) client background characteristics, (b) psychological processes (e.g., thinking) involved in client response to treatment, and (c) programmatic factors that impede and facilitate treatment engagement. The findings would be helpful for treatment planning with regard to providing effective interventions and strategizing program resources to maximize treatment utilization.
The research site is a 28-day public-funded inpatient substance treatment program affiliated with the Sheriff’s Office in a mid-sized southern city in the United States. This treatment facility, which receives approximately 1,000 adult clients per year from both legal agencies (e.g., drug court, local, jail, probation and parole office) and general clinical agencies (e.g., behavioral health clinics, detoxification facility, hospital, outpatient drug program) and maintains approximately 20 active caseloads per week, is the largest public-funded substance use treatment center in this geographic area encompassing three county equivalents. The facility is a restricted environment wherein guests are only granted to visit with administrators’ permission; the family is allowed to visit on every Friday during a 2-hour visiting window. This is a co-ed treatment facility wherein clients are scheduled to attend gender-specific and mixed-gender counseling groups and can receive individual counseling upon request. The program has two substance abuse counselors. This treatment program also collaborates with external organizations (such as churches, 12-step groups) in terms of inviting external agencies to the facility to lead recovery groups and sending clients to those organizations for additional recovery-related activities. Male and female clients live on the same floor of the building but in separate wings. Client residence is managed by technician staff who function as paraprofessional health educators and also assist substance abuse counselors in treatment to varying degrees.
Method
Participants were 60 clients (the demographic information is presented in Table 1) from the aforementioned research site. There was a slightly higher proportion of male clients (60%) and the majority of the clients were White (66%), followed by African American (29%) and Others (5%). With regard to the referral source, 35 participants (58%) were referred by clinical agencies (i.e., outpatient drug programs, health clinic, hospital); 20 participants (33%) were referred by drug court, probation office, or diversion programs, and the remaining five participants were referred by family or friends.
Client Demographic and Background Information.
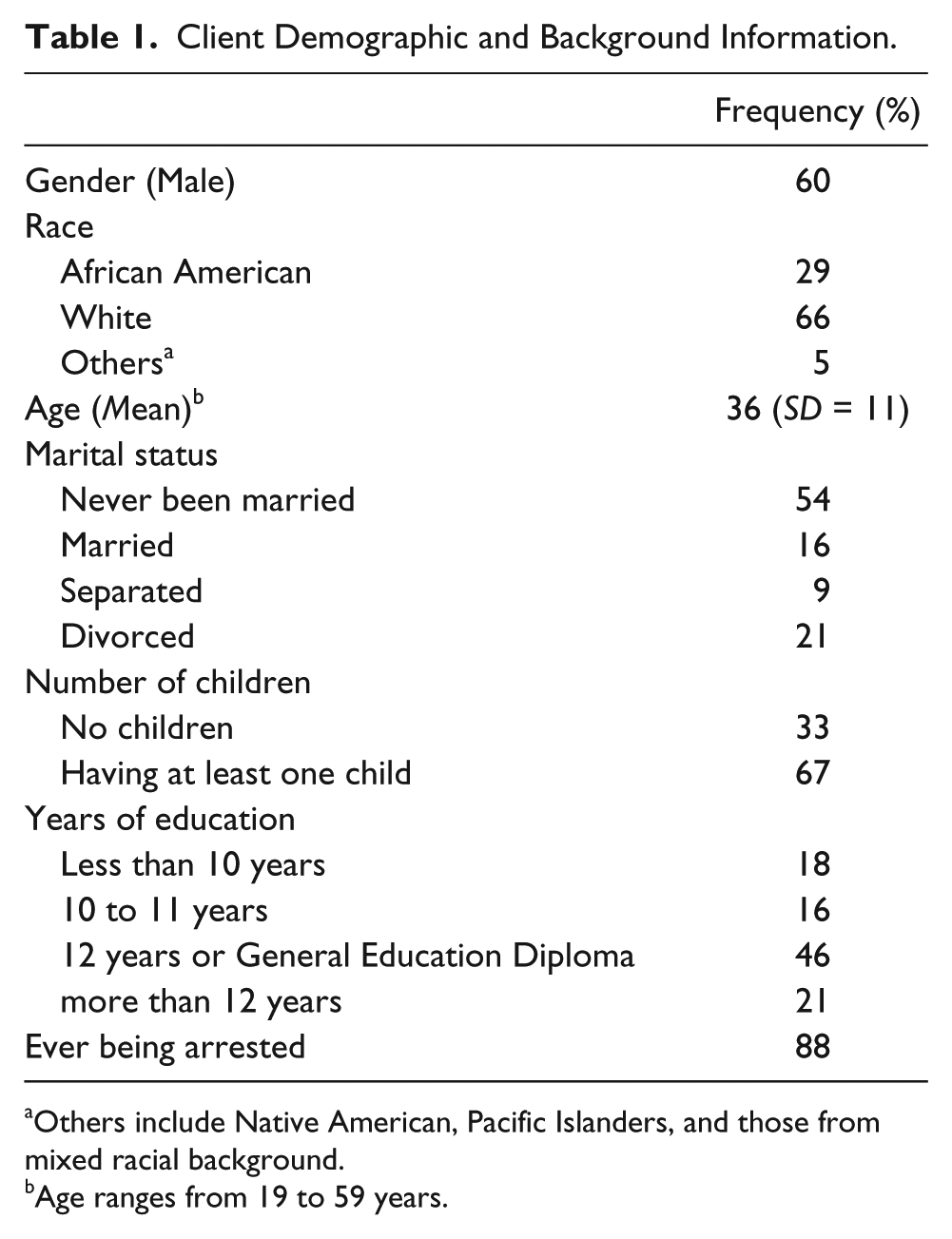
Others include Native American, Pacific Islanders, and those from mixed racial background.
Age ranges from 19 to 59 years.
Procedures
The potential participants who were eligible for successful were recruited for a one-on-one semistructured interview. We purposefully recruited participants for interviews right before discharge because this would allow them most “seasoned” in treatment and, thus, provide sufficient information on treatment experience. Seventy-three clients were approached approximately 2 days before treatment discharge. Thirteen potential participants declined due to a variety of reasons, mostly health issues or being busy with discharge paperwork. Prior to the study’s beginning, the Institutional Review Board of the authors’ university approved the interview guides, informed consent, and a survey of background information. All the participants provided informed consent before data collection and received no compensation for participation. Participants were aware that the (and a lack of) participation did not affect the regular treatment they received in the facility in any way.
The client interviews lasted 20 minutes on average, ranging from 10 to 47 minutes, the length of which is consistent with the literature (Baim-Lance, Tietz, Schlefer, & Agins, 2016). The one-on-one interviews were conducted face-to-face in a private room at the treatment agency by the research team, comprised of four graduate research assistants in psychology and two PhD researchers with extensive qualitative research experiences between September 2015 and March 2017. The graduate research assistants were trained by one PhD researcher and became familiar with the interview guide by conducting pilot interviews. All the research assistants were supervised by the same PhD researcher during their first two interviews. The digital recordings of all interviews were transcribed verbatim with a professional transcription agency.
The client interview began with a number of rapport-building questions about the individual’s background, including an exploration of how they described themselves, what hobbies they had, and some of their first experience with substance use. The interview then moved on to a discussion about earlier treatment experiences (if applicable) before introducing a variety of questions about the current treatment experience. In addition, clients responded to a range of questions about the characteristics of the program itself, which were intended to address a wide variety of factors that may influence treatment engagement. The following are question examples:
Has any specific event after entering this program shaped the way you looked at addiction and substance use treatment? If yes, what is the event?
What challenges have you experienced? Do these challenges make it difficult to stay on treatment?
In addition, client interviews included probing and specific examples to obtain more comprehensive explanations to questions.
Data Analysis
All the transcripts were de-identified before loading into ATLAS.ti, a qualitative software program, which was used to code and index data. For the qualitative analysis portion of the study, the three authors participated in coding using the philosophy of interpretative phenomenology analysis (IPA; Smith & Osborn, 2008) and a framework of thematic analysis (Braun & Clarke, 2006). Thematic analysis being particularly useful in providing structure for identifying patterns across data.
Broad codes were generated based on the interview guide. Next, all three authors immersed themselves independently in the data to create additional, more specific coding categories. Coders met biweekly to compare coding results to achieve consensus. Coders achieved an over 90 percent intercoding reliability, which was tested in two steps. First, three coders independently applied the codes to five randomly selected transcripts and calculated the percentage of the agreement on each segment before discussion. Second, two coders continue coding the rest of transcripts independently and calculated the percentage of the agreement again. The entire coding was consolidated after reaching consensus.
Within these discussions, additional codes would often be generated or discarded. For example, the code of “self-acceptance” was collapsed into the code of “self-evaluation” that encompasses more broad internal processes, and the code of “post-treatment emotions” was discarded as the researchers decided it was not theoretically feasible to identify emotions that clients had not specifically mentioned. Disagreements were minimal but were handled by employing widely accepted methods of validity such as remaining open, being willing to discard coding that was not well supported, and engaging in creative, thoughtful dialogue (Morse, Barrett, Mayan, Olson, & Spiers, 2002) and reaching consensus on conceptualization of codes and themes. In this way, not only did the researchers remain open and flexible to the creating of the codebook but also facilitated the conceptual understanding of the codes and themes.
Upon completion of all coding and the intercoding reliability checks, the authors identified 10 primary codes (past substance use history, previous treatment, current treatment, family, aftercare [i.e., continual treatment plans after the current treatment episode], future life plans, psychological growth, mental health issues, the self-evaluation, and social network) across the data. Furthermore, the coders defined secondary codes (e.g., counselor rapport, general outlook, treatment progress, family; resulted in a total of 127 secondary codes) embedded within the primary coding schemes and then applied those codes to refined elements. The coding process ceased when all authors reached high consensus about the codes, and when more specific coding elements either did not substantially add to the narratives revealed by the data or began to overlap (Braun & Clarke, 2006).
The subsequent step in the analytic process involved interpreting each code’s thematic meaning, or, as Braun and Clarke (2006) state, “tell[ing] the complicated story of your data in a way which convinces the reader of the merit and validity of your analysis” (p. 23). Data extracts were used to flesh out themes pertaining to treatment participation and treatment experiences and reveal nuances about the lived experiences of those undergoing treatment. Those themes are high-level abstract concepts derived from the interpretation of codes. All authors agreed on the themes identified from the analyses.
Results
The results present four major themes including perceived treatment needs, trust and counselor rapport, peer inspiration, and organizational barriers to treatment engagement (see Figure 1). Quotes are included to illustrate findings.
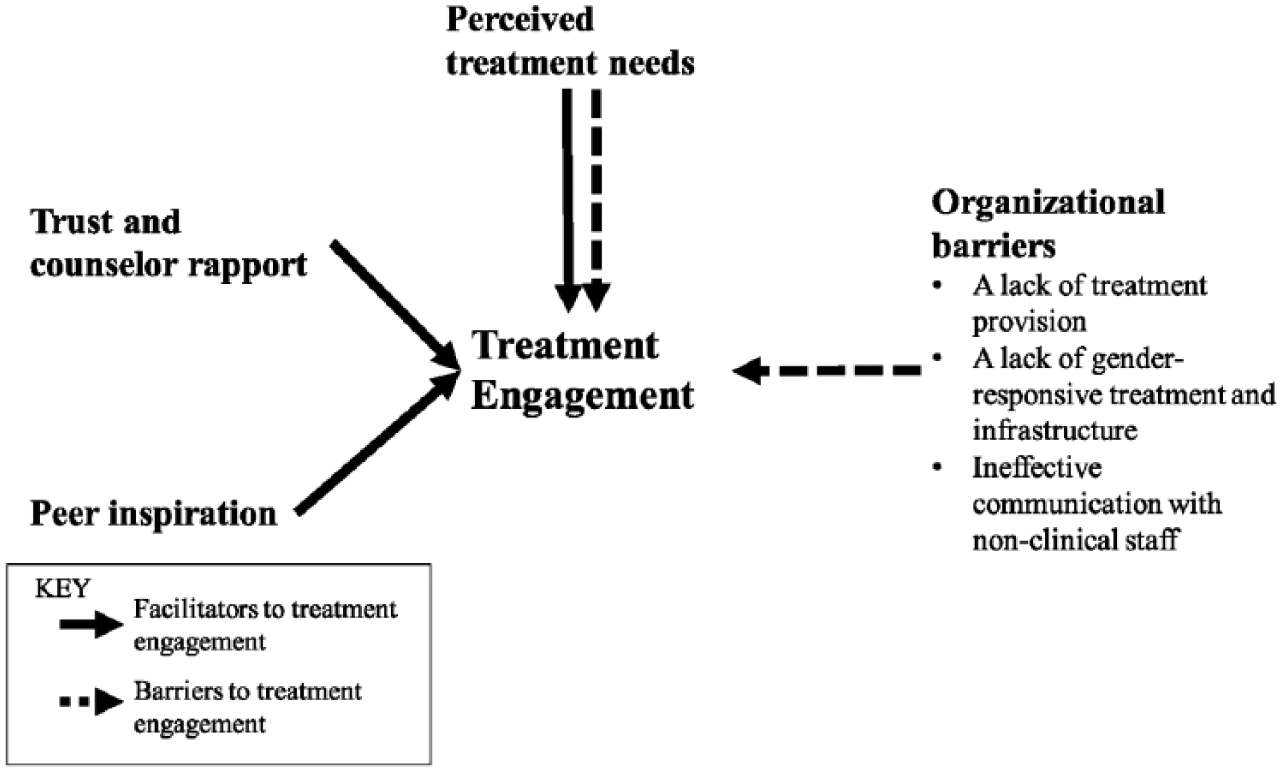
Four major themes of the qualitative findings.
Perceived Treatment Needs
When being probed about treatment experience, several clients revealed a lack of treatment motivation because they did not perceive a need for treatment. A male client in his late 20s without prior treatment experience who was referred to this treatment by probation officers stated that I don’t really think I really need treatment. It never affected anything. All the thing was—it’s illegal to smoke marijuana or anything, but I never had any problem with it in my family, or my work history, never was late.
Likewise, some clients claimed that the capability of being able to lead a normal life should distinguish them from being diagnosed as an addict. A female client in her mid 20s without prior treatment experience reported that they (counselors and peers) think I am in denial about my past and my drug use and stuff . . . I’ve never had cravings for drugs. I’ve never (overdosed) of stuff. (Interviewer: So do you feel like you did more recreationally?)Yeah. I mean, I don’t even use it socially. Say, if I wanted to smoke a joint or something, I’ll sit on the couch at home, put on a movie, and smoke a joint.
On the contrary, several clients reported with a continual accumulation of negative life experiences due to a long-term use of drugs and the resultant mortality salience, and the weariness derived from problems associated with drug use reported perceived treatment needs. A male client stated that he was very serious about this treatment because “[at] the age of [50s this] might be my last [chance to get recovery] or may end up dead.” Likewise, a 48-year-old male client who had been in substance treatment more than 4 times expressed a strong sense of internal treatment motivation, in contrast with previous treatment episodes: In previous treatment episodes, I [would] try to be in legal situations, keep from going to jail, kind of do it for my mom and all of that. But right now, . . . I came on my own, and that’s what I really want this time because I’m tired. I’m 50 years old, and I’m tired.
Moreover, older age often in conjunction with multiple treatment episodes influences treatment responsiveness, as shown in the previous quote and the following quote by a male 30-year-old client who was a treatment veteran: It changed. The last time, like I say, I was court-ordered the last time I came too, and this time I came really because I had to and then everything changed. Like, I actually see I need it. Got out of denial.
Trust and Counselor Rapport
The connection among peers and the relationship between client and counselor have been deemed as an influential factor on treatment peer cohesion and treatment responsiveness (Center for Substance Abuse Treatment, 2006; Yalom & Leszcz, 2005). Despite client–counselor confidentiality, one male client in late 40s with multiple prior treatment experiences still raised a concern on the confidentiality given a close working relationship between this treatment facility and law enforcement: I believe I can tell my counselor everything but the part of deal is there’s so much that you can tell a counselor because they probably work with the staff or the police too.
Being aware of the trust issues and the importance of counselor rapport, counselors have strived for creating a sense of trust and empathy, which was corroborated by several clients, as exemplified in the following quote by a female client in early 20s who was a treatment rookie: At first, I was kind of standoffish, just like what anybody is. Us addicts, we always say we have trust problems, but we trust the wrong people . . . Once [a counselor] said he did [have the addiction], that kind of opened me up to where, okay, you understand what we’re going through and what-not. It’s easier to relate to someone that’s actually been through it rather than someone that hasn’t.
In addition, many clients mentioned treatment progress, in terms of being empowered and receptive to treatment plans, initiated by counselors. A female client in early 30s who had no prior treatment experience spoke about how her successes were facilitated with a counselor’s assistance.
When I came here, I still had the feeling that I was not validated, [and] not worthy . . . [A counselor] helped me realize that I was looking at things through different colored lenses, that I really needed to take a better look at myself and examine who I am as a person because that’s ultimately what led to the substance abuse at the time was how I looked at myself, how I was dealing with things.
Peer Inspiration
Several clients acknowledged the therapeutic value of being exposed to group sessions wherein group members shared life stories, substance use, treatment goals, and other matters. Several clients stated that group sessions provided opportunities for self-reflection via a different perspective, which prompt acceptance of treatment plans. Many clients expressed that the discussion of life stories led to an increasing degree of problem recognition. For example, a male client in early 20s who first received treatment for substance problems said that some tools I have gotten from over here is you only lying to yourself. And that’s one thing I’ve noticed is—and when I say that, I mean, you can’t get over on nobody, especially if that person has having used before and have been through the things you’ve been through. Especially them telling you, “I did that before. I’ve been there and done that.”
Organizational Barriers to Treatment Engagement
Even those clients (who self-acknowledged) making significant progress mentioned several barriers to treatment engagement, mainly due to discrepancies between client expectation and the experience of services offered by the treatment provider. Many of these discrepancies were identified as organizational barriers, including insufficient treatment provisions, a lack of gender-responsive treatment, and ineffective communication between clients and staff.
A few clients, particularly those who had extensive experience with treatment, mentioned a lack of sufficient treatment provisions in this public-funded inpatient program, as indicated by the following quote from a 29-year-old male client who had been more than 4 times in treatment: I’ve been doing this for a while so it’s cliché, textbook type of things. A lot of the things I heard of already heard before. I guess the part that I got was being honest about myself and expressing those things. Other than that nothing really . . . For me that comes from a private run facility that pays insurance to a state facility, it’s a whole other ballgame!
This issue is common among public-funded facilities wherein funding and resources have been a great concern (Pullen & Oser, 2014). By the same token, several clients expressed a desire to obtain more counselor time in treatment plans.
A lack of gender-responsive treatment services was another factor that clients stated hindered their treatment responsiveness. Clients, particularly female clients, expressed a lack of comfort and safety to disclose life stories in front of the clients of the opposite sex in the mixed-gender group sessions. When being asked about treatment changes, a female client in her mid 40s who had received treatment twice before reported, I feel that if the staff here has such a problem with the guys and girls being together that they should separate them . . . It is very distracting when they are constantly interrupting the treatment to tell someone not to talk to her, or her not talk to him. And then someone has a big blowout and that becomes even more distracting so maybe if it was separated it would be better. And if they had more individual counseling groups, that were gender specific I think it would be better. Because a lot of these girls have been raped or molested and it’s hard to talk about that in front of the opposite sex. There is even a lot of things that I did not put in my life story because I don’t want it to tell in front of a group of guys.
Furthermore, female clients revealed that sharing common living space (i.e., living on the same floor of the facility) brought in an additional layer of concern to treatment dynamics. One female client said she felt that the presence of male clients led to a decreased perception of comfort. For example, when she cleaned the common area, the presence of male clients led her to be self-conscious about bending over and engaging in other behaviors that could lead to unwanted attention.
The inpatient program operates as a restrictive environment wherein the clients, apart from counseling, spend the majority of the time with the technician staff (techs) who are responsible for routine management. Quite a few clients conveyed that the staff were not sensitive to treatment needs, which led to a lack of open, effective communication, as indicated by the following quote from a male client in his early 30s without prior treatment experiences: There should be more open lines of communication between the techs (technicians) and the patients because we spend majority of our time with the techs. We see the counselors maybe two to four hours a week, and you spending the rest of the week following rules, and that’s not how life works when you get out to the real world.
Overall, participants revealed a process starting with a lack of treatment needs related to denial of drug-related problems, a lack of trust, a sense of stigma, and so on. The negative feelings then changed into a positive desire for treatment utilization caused by a fear of deteriorating health leading to death and empowerment from group sessions, which in turn changed the attitude toward treatment into seeing it as an accessible remedy. The positive changes they have seen evoked continued engagement and positive experience in treatment.
Discussion
The current study is intended to generate useful findings relevant to treatment engagement based upon qualitative analysis of interviews with clients in a short-term inpatient program. Greater knowledge of general areas of concern and positive factors identified by clients may provide new avenues of discussion that can be relevant to an overall positive experience in counseling and increase treatment participation. The findings respond to the call for qualitative, patient-centered explorations to provide a richer, more nuanced description of treatment experiences by Orford (2008) and highlight the importance of patient-center care in defining the health care quality (Baim-Lance et al., 2016; Epstein & Street, 2011). Some important specific findings are discussed here.
The Importance of Perceived Treatment Needs and Treatment Motivation
Client inputs stressed the importance of treatment motivation in seeking, attending, and complying with treatment, whereas a lack of problem recognition was rated as a barrier to treatment engagement and benefits by counselors, which is aligned with the literature indicating that treatment motivation predicts treatment engagement and favorable outcomes (Brocato & Wagner, 2007; Broome, Simpson, & Joe, 1999; DiClemente, Schlundt, & Gemmell, 2004; Joe, Simpson, & Broome, 1999; Serin & Kennedy, 1997). The findings also highlight that a willingness to address substance use behaviors is often triggered by a desire to minimize the negative consequences of an accumulation of life experiences derived from substance use (Cahill, Adinoff, Hosig, Muller, & Pulliam, 2003). However, a few participants still casted doubt on the severity of substance use and the necessity of receiving treatment, which negatively affected treatment engagement. This finding, coined by the transtheoretical model of intentional behavior change (Prochaska, DiClemente, & Norcross, 1992), emphasizes the importance of triaging clients upon stages of treatment motivation, adopting client-centered counseling techniques to discuss treatment needs, developing individualized treatment plans, and cultivating intrinsic treatment motivation for enhancing treatment engagement.
The Impact of Life Events
Consistent with previous quantitative literature (Chi & Weisner, 2008; Kalaydjian et al., 2009; Kohn, Mertens, & Weisner, 2002; Weisner, Matzger, & Kaskutas, 2003), age was a key factor influencing clients’ desire to seek and accept treatment services. Furthermore, the qualitative findings provide an additional explanation that some clients are not as receptive to hearing about the consequences of substance use when younger, due to not having experienced those long-term impacts of use. Individuals at the later stage of adulthood may experience long-term exposure to psychological and health risks and other substance-related problems, which make them more likely to recognize the importance of substance treatment (Orford, Hodgson, et al., 2006). This is consistent with the often-cited notion among many in treatment that one becomes more receptive to treatment after what is referred to as “hitting bottom” hypothesis (Khantzian, 1997). Conversely, once a client is receptive to treatment, there may be advantages to being younger, in the sense that younger individuals tend to be less rigid in adjusting cognition and behaviors (Schultz & Searleman, 2002), which in turn leads to a greater tendency to make positive changes. In addition, older adults seek and accept treatment for different types of substances compared with their younger counterparts (Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality, 2017). However, a dearth of clinical considerations have been rendered to treating older populations with substance use problems (Kuerbis & Sacco, 2013). The current study highlights that age-appropriate interventions should be expanded to address the entire life span, which is consistent with the efforts promoted by the National Institute of Alcohol Abuse and Alcoholism (2007).
Counselor Rapport and Peer Inspiration
Although efforts are being made to identify treatment motivation, a lack of perceived treatment needs is of note a product affected by several factors, such as counselors’ styles, in the context of counseling (Miller, 1999). This highlights the importance of counselor rapport and treatment peer support. The empathic bonding between clients and the counselor has been highly regarded for greater treatment engagement (e.g., Klag et al., 2010; Meier et al., 2005; Simpson, Joe, et al., 1997). The literature also indicates that therapeutic alliance not only facilitates therapeutic engagement and retention (Gibbons et al., 2010; Meier et al., 2005; Urbanoski, Kelly, Hoeppner, & Slaymaker, 2012) but also enhances psychological functioning (e.g., self-efficacy, psychological well-being) over the course of treatment (Hartzler, Witkiewitz, Villarroel, & Donovan, 2011; Klag et al., 2010), which potentially leads to greater treatment engagement. Overall, the findings add to the literature that therapeutic groups are very effective and practical in creating a supportive and expressive environment wherein group members, with a skilled, well-trained group leader (such as a counselor), can help each other grow in ways that are healthy and creative (Center for Substance Abuse Treatment, 2005; De Leon, 2000; Khantzian, Halliday, & McAuliffe, 1990; Scheidlinger, 2000, 2004).
Organizational Factors
Negative treatment experiences derived from a discrepancy between client expectation and actual treatment provision delineated by the current participants could be attributed to clients’ lack of knowledge and understanding of treatment plans particularly upon treatment entry, which might in turn lead to the reluctance to talk about treatment aspirations with the treatment provider. Previous research has suggested that being unaware of treatment plans at the early treatment phase among clients contributes to poorer outcomes (Pulford, Adams, & Sheridan, 2011). Thus, clinicians may consider providing more opportunities for clients to discuss treatment plans at the first phase of treatment, which helps cognitively engage in treatment and obtain treatment benefits.
Gender-responsive treatment is typically designed to provide a secure environment for women to safely discuss histories of trauma, abuse, and addiction without fear of judgment (Bloom, Owen, & Covington, 2003), the need of which is also held by men. Thus, program administrators might consider adjusting treatment plans and program infrastructure (e.g., separate living and entertainment areas) to allow for a safe therapeutic conversation for both genders with a mixed-gender treatment environment.
A frequently occurring theme in the client interview data was the expression of concerns about treatment from nonclinical staff. A lack of positive relationship with nonclinical staff may serve as a barrier to continuing treatment, which is aligned with the previous findings that staff attributes and program atmosphere were associated with treatment engagement (Landrum et al., 2012; Simpson et al., 2009) and a lack of connection between treatment staff and clients leads to a lack of treatment participation (e.g., Palmer et al., 2009). Given that a decent proportion of clients in current sample were referred by criminal justice agencies, clients were less likely to make positive comments about program characteristics that were perceived as critical or unnecessarily punitive. Increased emphasis on training of nonclinical staff in handling of clients may be beneficial, as well as greater investment in recruitment of personnel qualified for working with at-risk populations, all of which echo the importance of a more patient-centered form of quality of care in the interest of maxim treatment benefits.
Limitation and Future Direction
The client interviews only included those who completed 28-day treatment, the experience of which might differ from those who dropped out treatment (according to administrative records, the average dropout rate is 10% in the program). Future research might consider obtaining perspectives from those who terminated treatment prior to completion, which would shed light on how to improve treatment effectiveness. Given the literature (e.g., Hubbard et al., 1997; Simpson et al., 1997) indicating different treatment outcomes among various treatment modalities, the application of the current findings to other treatment modalities warrants further investigation. In addition, even though a need for gender-responsive treatment was raised by clients, the current study did not examine gender-specific factors associated with treatment engagement. Given gender as an essential contextual factor that implicates treatment process, future research may consider examine gender differences (e.g., client–therapist gender matching) in the way they respond to treatment. Another research direction includes gender differences in treatment engagement in a mixed-gender treatment facility, the findings of which would have implications for enhancing gender-specific treatment responsiveness.
Collectively, given the wide range of factors listed by interviewees as relevant to the successful engagement of treatment, more emphasis should be placed on treatment plans being tailored to the specific risk and treatment needs, which facilitate nuanced understanding on the role of factors on treatment engagement. Aligned with the literature (Fiorentine et al., 1997; Hser et al., 1999; Prendergast, Greenwell, Farabee, & Hser, 2009), this study suggests the enhancement of treatment experience, in terms of strengthening the client–counselor relationship, and creating an empathic and inspiring friendship between treatment peers, matching clients to services, and providing gender-responsive services, may improve treatment engagement, which ultimately leads to recovery. The current study also responds to the request by several researchers (e.g., Laudet et al., 2009; Orford, 2008; Orford, Hodgson, et al., 2006) regarding the essential role of client and counselor inputs in treatment research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.