
Abstract
Little is known about how men and women who test positive for a BRCA gene mutation or have a strong family history of carrying a BRCA mutation manage disclosures about their BRCA-related cancer risks and family planning decision-making. By conducting interviews with 25 men and 20 women, this study investigated men’s and women’s approaches to disclosing their BRCA-related cancer risks and family planning decision-making. Guided by the Disclosure Decision-Making Model (DD-MM), this study demonstrates that men and women assess both information and the recipients of disclosures when making disclosure decisions. Theoretical implications for the DD-MM are discussed along with practical implications for hereditary cancer risk and family planning.
According to the Centers for Disease Control and Prevention, tests are now available to diagnose individuals with gene mutations predisposing them to an increased risk for illnesses such as diabetes, heart disease, and a variety of cancers. For example, genetic testing for mutations in the BRCA1 and BRCA2 genes has increased throughout the decade leading to individuals having an improved understanding of their lifetime risk of developing hereditary breast and/or ovarian cancer (HBOC) and other BRCA-related cancers such as prostate, pancreatic, and melanoma. This increase has led to a new patient population—individuals who have a genetic predisposition to an increased lifetime risk of cancer but who have not yet developed cancer (Mahon, 2014).
Individuals with increased risks of developing BRCA-related cancers face numerous complex decisions regarding the management of their health and family. Women who test positive for a harmful BRCA genetic mutation have up to a 72% chance of developing breast cancer and up to 44% chance of developing ovarian cancer during their lifetime (Kuchenbaecker et al., 2017), compared with a 12.4% general population lifetime risk of developing breast and a 1.3% general population lifetime risk of developing ovarian cancer (www.cancer.gov). Men who test positive for a harmful BRCA mutation also have a higher risk of developing breast cancer than the general population (Tai, Domchek, Parmigiani, & Chen, 2007) as well as other BRCA-related cancers including prostate, pancreatic, and melanoma (www.cancer.gov).
Furthermore, both men and women also have a 50% risk of passing their genetic mutation to subsequent generations. As such, these individuals must consider their personal risk of developing BRCA-related cancers in tandem with family planning decisions. For instance, individuals consider when/if they should have biological children and the possibility of utilizing assisted reproductive technologies (ART) such as preimplantation genetic diagnosis (PGD) to have a child that does not carry the genetic mutation (Dagan, Gershoni-Baruch, Kurolap, Goldberg, & Fried, 2014; L. C. Friedman & Kramer, 2005). More specifically, women consider the timing of having preventive bilateral mastectomies (removal of breast tissue) and preventive oophorectomies (removal of ovaries) to accommodate their family planning choices (Dean & Rauscher, 2017; Donnelly et al., 2013; Werner-Lin, 2010).
Although previous research has examined women’s approaches to managing HBOC risk (e.g., S. Hesse-Biber, 2014; Hoskins & Greene, 2012; Howard, Balneaves, Bottorff, & Rodney, 2011), and a few studies have explored men’s approaches (e.g., S. Hesse-Biber & An, 2017; Moynihan et al., 2017; Rauscher & Dean, 2017), there is a paucity of work that has assessed both men’s and women’s approaches to managing and communicating those risks for themselves and their family. In addition, it is unclear how individuals with a BRCA mutation or who have a strong family history of carrying a BRCA mutation specifically disclose family planning decisions. Thus, the primary goal of this study was to simultaneously investigate how men and women who test positive for a BRCA gene mutation or have a strong family history of carrying a BRCA mutation manage disclosures about their BRCA-related cancer risks and family planning decision-making. Specifically, we utilize the Disclosure Decision-Making Model (DD-MM) to understand disclosure motivations. By achieving this goal, we enhance understanding of how disclosure decisions are made within the familial context. In the sections that follow, we discuss gendered differences for communicating about health and conversations about BRCA-related cancer risks and family planning as well as the DD-MM and how it applies to this context.
Differences in Communicating About Health
Previous research shows men and women manage and communicate about health information differently. In comparison with women, men are less likely to be communicative about their health (Ginossar, 2008; Koehly et al., 2009), slower to seek health services (Galdas, Cheater, & Marshall, 2005), and more likely to suffer from preventable illness (Bottorff, Oliffe, Robinson, & Carey, 2011). Moreover, within the family, communication about health is often done by women (Heisler, 2005). Gender differences in managing health information is particularly important for monitoring BRCA-related cancer risks because such risks are often categorized as female problems (Daly, 2009). Current research reflects the female focused nature of BRCA mutations by showing women are more likely to disclose their results (Smith, Zick, Mayer, & Botkin, 2002) and more likely to talk to family members (Daly, 2009; Koehly et al., 2009) than are men. In addition, men are less likely to seek out genetic counseling and genetic testing services (Daly, 2009; S. Hesse-Biber & An, 2017), be told about the implications for receiving positive genetic test results, and less likely to be included in family discussions about hereditary cancer risk (Mohamad & Apffelstaedt, 2008).
Men and women also approach communication about their hereditary cancer risk differently, influencing their decision-making. Broadly, women are more likely to communicate about BRCA than are men (Daly, 2009). Their communication is likely to be more focused on gathering and disseminating information (Koehly et al., 2009), providing support (Strømsvik, Råheim, Øyen, Engebretsen, & Gjengedal, 2010), and managing uncertainty (Dean, 2016; Fisher et al., 2017). However, when men communicate about BRCA, they are less open than are women (Smith et al., 2002) and more likely to target specific others (e.g., usually women) for such communication (Strømsvik et al., 2010). Yet, men are just as likely as women to pass a BRCA genetic mutation to a child and are also likely to struggle with consequences of family planning and cancer risk management. Thus, communicating about hereditary cancer risk is essential.
Communication About BRCA-Related Cancer Risks and Family Planning
Disclosure of positive genetic test results is important due to familial implications (Greenberg & Smith, 2016). Probands—the first individual in the family to get genetic test results—who test positive for a harmful BRCA genetic mutation disclose their positive genetic test results to their first-degree relatives at an average rate of 90% (Costalas et al., 2003; Finlay et al., 2008; McGivern et al., 2004). Extant research has found that probands are more likely to disclose their positive genetic test result under the following conditions: when the family members are female (Cheung, Olson, Tina, Han, & Beattie, 2010; Hughes et al., 2002), when the probands believe it is their duty to inform family members, and when the probands perceive the potential negatives of disclosure on the family’s relationships outweigh possible negative reactions from family members (Gaff et al., 2007; MacDonald et al., 2010; Seymour et al., 2010). For example, Dancyger et al. (2011) found both female probands who tested positive for BRCA, and their relatives believed that it was the proband’s responsibility to disclose their positive genetic test results to family members. Yet, the proband’s perception of their family members’ coping ability influenced the extent to which the proband edited and sometimes even withheld genetic information. However, probands are less likely to disclose their positive genetic test results when they believe that they are unprepared to discuss such issues (Costalas et al., 2003).
Although prior research has explored how and/or why families communicate about hereditary cancer risks (Chivers Seymour, Addington-Hall, Lucassen, & Foster, 2010; Forrest et al., 2003; Koehly et al., 2009; MacDonald et al., 2007), very little work has analyzed disclosures about family planning and BRCA-related cancer risks. Communication is the process of transmitting messages, whereas disclosure is the act of revealing personal and/or private information. Disclosing hereditary cancer risks and family planning decisions is important for a variety of reasons. For one, having these conversations can help patients make personal decisions about cancer risk management (S. Friedman, Sutphen, & Steligo, 2012; Werner-Lin, 2010) as well as familial decisions about the likelihood of passing the genetic mutation to their children and the implications of doing so (Dean & Rauscher, 2017; Donnelly et al., 2013). Second, being specifically knowledgeable about family planning options and engaging in discussions with health care providers and family members about family planning may assist patients in making informed family planning decisions. Although it is clear that conversations about family planning have important outcomes, men and women are still underinformed about their family planning options and undersupported in their decision-making (Dean & Rauscher, 2017; S. Hesse-Biber & An, 2017; Werner-Lin, 2008). By better understanding disclosure decisions patients make about family planning, health care providers can better prepare them for the types of conversations they will face and the options they should consider when making family planning decisions.
Moreover, disclosing information about BRCA-related cancer risks and family planning can affect not only a patient and his or her partner but also entire extended families. According to Werner-Lin (2010), a woman’s strong history of hereditary cancer in her family is likely to influence her family planning and cancer prevention decision-making. In Donnelly and colleagues’ (2013) study, women discussed their urgency to have preventive surgeries because they had watched family members die of cancer and felt their own genetic mutation would lead to a similar fate. In other words, these studies show that having a strong family health history of fatal HBOC, and talking about the implications for such a history, can influence a woman’s decisions about genetic testing, cancer risk management, and family planning. However, it is unclear to what extent disclosures about BRCA-related cancer risks and family planning affect men who test positive for a BRCA mutation or who have a strong family history of carrying a BRCA mutation. As such, examining both men and women’s disclosures about their BRCA-related cancer risks and family planning decision-making is important.
Theoretical Foundation
The DD-MM is one model used to analyze the decision-making process of disclosing information, specifically about health and illness (Greene, 2009). The model proposes three stages of disclosures: (a) the decision to disclose, (b) disclosure message strategies, and (c) disclosure outcomes. Of specific importance to the current study is Stage 1—the process individuals go through in making decisions to disclose information about family planning and hereditary cancer prevention strategies. In this stage, the DD-MM proposes disclosers evaluate their disclosure decision-making by assessing the information, assessing the recipient of the disclosure, and evaluating disclosure efficacy.
Greene’s (2009) model proposes individuals assess information as a first stage of disclosure decision-making. Such assessments occur by analyzing stigma, preparation, prognosis, symptoms, and relevance to others. Potential disclosers commonly evaluate stigma when making disclosure decisions (2009). Research has shown when individuals deem their diagnosis stigmatizing, they are less likely to disclose information (Steuber & Solomon, 2011). Individuals also evaluate their preparation—or their expectations prior to receiving a diagnosis. According to Greene (2009), being prepared for a disease gives an individual time to prepare a disclosure strategy; however, receiving a surprise diagnosis requires quick disclosure to procure social support. Third, individuals take their prognosis, the anticipation of negative outcomes, into consideration when evaluating their disclosure decisions. Greene (2009) argues the role of prognosis in disclosure decisions can be complex due to the uncertainty that commonly accompanies a prognosis. Individuals may also consider symptoms (i.e., illness visibility) when making disclosure decisions (2009). Greene (2009) proposes that as symptoms of disease become more visible, disclosures will increase. Finally, Greene (2009) suggests that individuals make disclosure decisions based on relevancy to the recipient. Specifically, she proposes that individuals increase disclosure to recipients most affected by the information. However, the ways in which assessment of the recipient predicts disclosure decisions is still unclear.
Taken together, existing DD-MM literature shows that individuals commonly evaluate disclosure decisions by assessing both the information related to their illness and their knowledge and expectations of the recipient of the disclosure. Because disclosure of family planning and hereditary cancer risk prevention decisions are important to how individuals, couples, and families manage decision-making, understanding motivations for disclosing this information could provide not only more detailed knowledge of how individuals manage disclosures related to hereditary risk but also opens the door for learning how their motivations might influence their individual and relational well-being. To achieve the goal of understanding individuals’ motivations for disclosing information about their hereditary cancer risk and family planning decision-making, the following research question guided this study:
Method
Recruitment and Participants’ Demographics
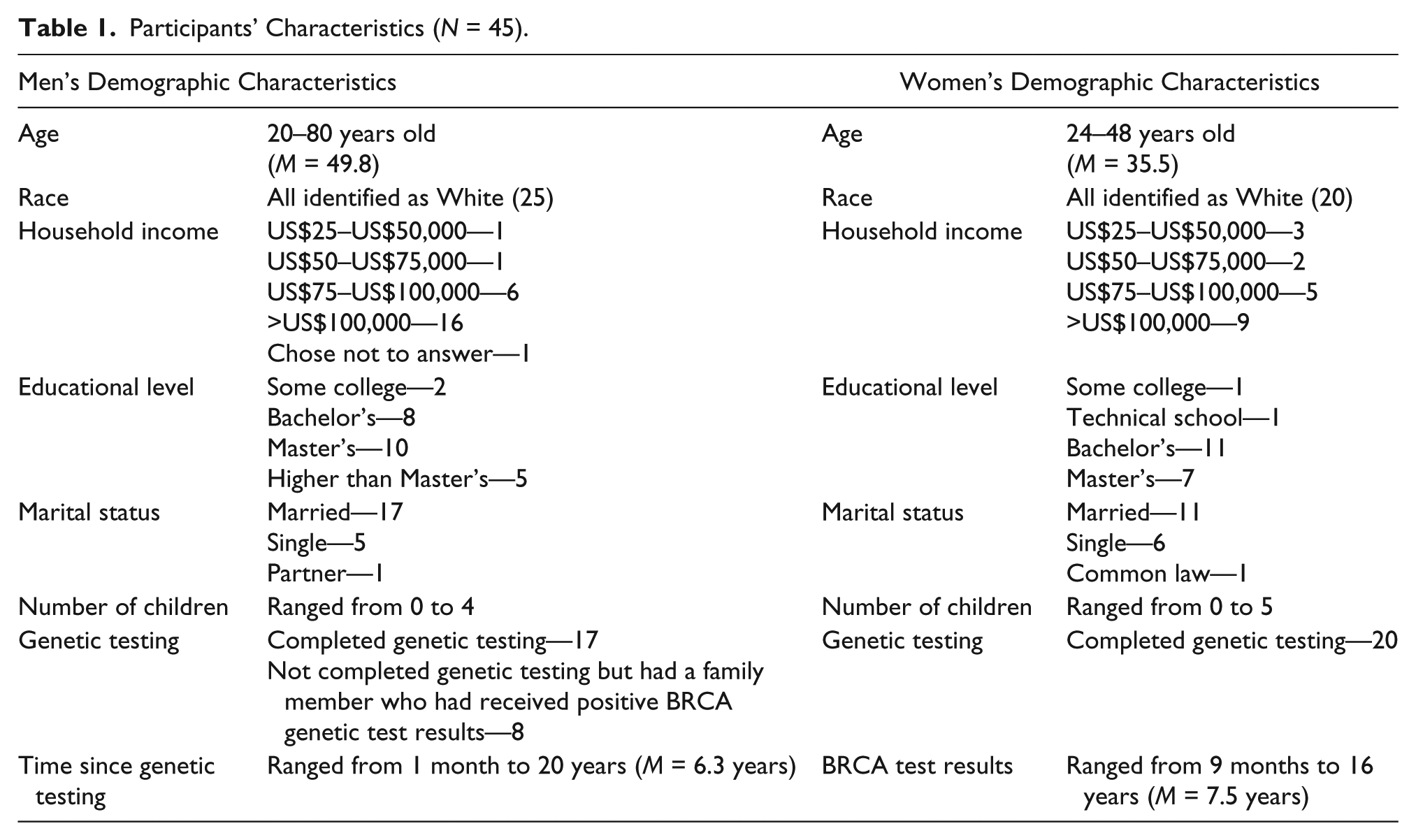
Upon receiving Institutional Review Board (IRB) approval, purposive sampling was employed (S. N. Hesse-Biber & Levy, 2006). First, participants were recruited by hosting a table at the 2015 Facing Our Risk of Cancer Empowered’s (FORCE) Joining FORCEs Against Hereditary Cancer Conference located in Philadelphia, PA. Participants were then recruited by posting an IRB-approved flyer on FORCE’s Twitter and Facebook. To be eligible for this study, participants (a) either tested positive for a harmful BRCA1/2 genetic mutation or had a strong family history of carrying a BRCA1/2 mutation, (b) tested positive for BRCA1/2 or aware of their family cancer history before completing their family planning, (c) spoke English, and (d) were more than 18 years old. A total of 25 men and 20 women participated in this study (see Table 1 for demographics).
Participants’ Characteristics (N = 45).
Data Collection and Analysis
After completing the informed consent process, participants conducted a telephone semistructured interview with one of the authors. Sample interview questions included the following: “Have you undergone genetic testing? Why or Why not?” “In what ways do you feel your experience with BRCA is different due to your sex?” “What health decisions have you made related to your BRCA mutation/high risk of hereditary cancer, and why did you make those particular decisions?” “In what ways do you feel private about disclosing information about your hereditary cancer risk?” “Do you feel like other members of your family include/exclude you in conversations about BRCA?” “Can you describe for me any conversations/decisions you and a partner have made regarding family planning when considering your hereditary cancer risk? How do you talk to friends about your hereditary cancer risk?” Probing questions supported a guided, yet conversational interview (S. N. Hesse-Biber & Levy, 2006). Interviews ranged in length from 23 to 71 min. Interviews were audio-recorded and then professionally transcribed.
Data were analyzed by the authors using an iterative approach—meaning emergent themes were compared with existing research and theories (Tracy, 2013). Specifically, the authors engaged in three levels of analysis. First, to gain a cursory understanding of the data and potential themes, both authors read all transcripts and engaged in memo writing. The authors had in-depth conversations about initial patterns while collecting data as well as once data collection was complete. During these conversations, the authors discovered that participants were discussing how they assessed information and disclosure recipients when making disclosures about BRCA-related cancer risks and family planning decisions. Second, both authors used first-level coding to categorize the data (Tracy, 2013). Using the constant comparison method, each author employed incident-with-incident coding by creating themes and recording possible meanings in the transcripts’ margins (Charmaz, 2014). During this phase, the authors reflected on extant research and specific theories that might inform participants’ assessments of information and the recipients of disclosures when making disclosure decisions. The authors agreed the DD-MM was a helpful theory in understanding participants’ disclosure decisions. That is, although the DD-MM provided structure for how the themes were organized and understood, it did not serve as a coding scheme. Third, the authors engaged in second-level axial coding to refine the themes identified during first-cycle coding (Tracy, 2013). In other words, data excerpts were selected and compared against the existing themes. After identifying the themes within the data, the authors outlined data excerpts per theme. The results presented below reflect the outlining of the excerpts within each theme. Data collection stopped once theoretical saturation was reached where no new themes emerged (Morgan, Fischhoff, Bostrom, & Atman, 2002). Finally, verification was done by the authors utilizing thick rich description of themes to allow readers the flexibility to decide the degree to which the findings are transferable (Creswell, 2007).
Findings
Guided by the DD-MM, this study examined how individuals assessed information and often simultaneously assessed disclosure recipients when making disclosures about their BRCA-related cancer risks and family planning decisions.
Misconceptions
To begin, when assessing their decisions to disclose information about BRCA-related cancer risks and family planning decisions, participants discussed misconceptions as an information assessment component. Although the DD-MM utilizes the term stigma, these participants’ experiences were reflected as misconceptions. They explained feeling misunderstood by their family members and friends who had little knowledge or experience with BRCA-related cancers and medical experiences. Specifically, two subthemes were evident—ignorance and insensitivity.
The first subtheme was ignorance. Managing ignorance required a combination of revealing and concealing strategies. For example, in her explanation about why she felt her communication about her BRCA-related cancer risks and family planning decision-making was sometimes constrained, a female participant (BRCA2, married with children) said, “I think there’s a lot of ignorance surrounding BRCA mutations. I’ll say, ‘I’ve got a BRCA mutation,’ people look blank. But as soon you say, ‘Like Angelina Jolie,’ suddenly they’re like, ‘Oh, that, yes.’” A male participant (BRCA2, married with children) highlighted similar ignorance when explaining how others tend to react upon hearing his BRCA mutation status. He expressed, I tell them that I tested positive for the BRCA2 mutation. . .[and] sometimes when I’m talking to people, I’ll get a, “Aww, shucks” kind of moment, and they think that I’m going to die of cancer. And it’s, like, “No, no, no. It’s not like that. I don’t have cancer . . . I think [there’s] some general misconceptions about, when I talk about the mutation that people think that it means absolutely you’re going to get cancer.
So, when met with ignorance after disclosing their BRCA mutation status to their family members and friends, participants were less willing to disclose in the future because it would require them to further explain their BRCA-related cancer risks and family planning decisions.
The second subtheme was insensitivity. Although men and women both were met with ignorance, men did not experience the level of insensitivity to their disclosures that women did. For instance, women spoke of family members and friends to whom they had disclosed information and were met with insensitivity, mitigating future disclosures to those recipients. A female participant (BRCA2, married with no children) discussed having difficulties disclosing to her in-laws due to their lack of understanding of genetic risk and preventive options. She recounted, I have found that in my more extended family and my in-laws don’t know a lot about this stuff, and so they are hard to talk to, because if you are trying to convey that you have to do certain surgeries, and you don’t really have a choice about them, they don’t quite get it. And they don’t quite get the mutation, even if you try to explain the implications.
Another female participant (BRCA2, married with children) also experienced what she perceived to be insensitivity from her mother-in-law about her family planning decision to use PGD, making her hesitant to disclose future decisions. She said, I remember going home and talking to my mother-in-law about it, and she was like, “Oh, that’s wonderful. You know just test them, and then you get rid of the bad eggs.” And I was like, “Excuse me?” It was so hard. This conversation was like, “No. This is not happening.” Because, “They’re bad eggs, because they carry BRCA?”
In sum, after being met with ignorance and/or insensitivity from family members and friends, participants were less likely to make disclosures about their BRCA-related cancer risks and family planning decision-making. Yet, overall, misconceptions were a more important information assessment component for women, and ignorance was specifically more evident in men’s experiences with disclosing than insensitivity.
Preparation
Participants also discussed preparation as an important information assessment component. Preparation included the following two subthemes—family history of cancer and concern regarding the recipient’s lack of preparation. The first subtheme related to one’s family history of hereditary cancer. Participants explained that when they came from families with strong histories of BRCA-related cancers, they grew up hearing disclosures about hereditary cancer, cancer prevention and treatment, and family planning. In other words, those family disclosures inevitably influenced the disclosures of their own decision-making and prepared them for making their own disclosures. One female participant (BRCA1, single with children) was an example of how preparation lead to open disclosures within the family. She said, “I sort of feel like cancer is like the common cold in my family. We talk about it very openly.” A male participant (BRCA2, married with children) echoed how his family was also open to disclosing and discussing BRCA-related cancer risks and family planning when he stated, “We are exceptionally open to talk about anything in a very straightforward manner. Our family excels in that.”
Alternatively, women also discussed how a lack of previous family disclosures influenced their own decision-making disclosures. Particularly, this lack of preparation occurred most often in families where the mutation was passed through males. A female participant (BRCA1, married with children), who inherited her mutation from her father, exemplified this theme when she talked about having fewer conversations with family members because there was so little knowledge about BRCA in her family. She stated, “No one questioned it or had any concerns about it. I think because they weren’t even aware of what it meant to be BRCA positive.” A different female participant (BRCA1, married with children), who also inherited her mutation from her father and was unaware of a family history of cancer, when asked if she talked to her family about her family planning she said, “No, I mean I have not really talked to them a lot about it.”
The second subtheme was concern regarding the recipient’s lack of preparation. Participants discussed assessing their recipient’s preparation for dealing with the discloser’s disclosure and the recipient’s potential response to the disclosure. For instance, one male participant (BRCA1 in family, single with no children) noted that most of his male friends were not prepared to understand what he was going through, and therefore he was less likely to repeat disclosures. He explained, It’s more of a joke for a lot of men, and I’ve never found anybody that I’m comfortable enough talking to. I have a couple good friends that are guys, but I still, whenever it comes up to something like this, I don’t want to bother bringing anything up like that.
A female participant (BRCA1, married with children) had similar experiences with her friends. She said, Even though they were my very good friends and very sympathetic I just felt like they had no idea what I was feeling. I don’t remember what their words were necessarily. I remember their looks. Freaked out. They really didn’t know what to say. That’s when I felt like, “Nobody understands what I’m going through.”
Yet in comparison with friends who were largely unprepared to hear their disclosures about BRCA as exemplified above, participants felt they could more openly disclose to family members due to their higher level of preparation. Later in her interview, the same participant noted that she disclosed to her sisters about her desires to have a second child because they were prepared to receive such a disclosure as they had had similar experiences. She shared, My sisters were older, so they were having family planning discussions too. One of my sisters was pregnant at the time that we were all getting our BRCA results, and then she had gotten breast cancer. Her belief was that being pregnant was one of the causes for [her breast cancer]. So, the discussion did come when I was looking to maybe have a second child. Both of my sisters thought that was a risk for breast cancer.
Similarly, a male participant (BRCA2, married with children) disclosed his positive genetic test results to his cousin because he knew she was well-versed in BRCA-related cancers and thus would react positively to such a disclosure. He recounted, The first person I spoke to was my first cousin, who was diagnosed as BRCA-positive [about] 11 years ago now. She had gone through a double mastectomy as a precautionary act. So, basically, as soon as I spoke to my cousin, she gave me all the genetic mapping information and connected me with the hospital that has been tracking our family and wanted additional information on my leg of the family tree and the new information that was added to their records.
Overall, participants with strong family histories of BRCA-related cancers were typically more prepared to disclose with family members compared with individuals from families without a clear history of hereditary cancer. Moreover, participants were less likely to discuss BRCA with friends who they believed were less prepared and were more likely to discuss BRCA with family members who were having similar experiences and thus were prepared for such disclosures.
Risk Perceptions
Third, when assessing their decisions to disclose, participants also made decisions by assessing their perceived risk of a possible hereditary cancer diagnosis. Although the DD-MM utilizes the term prognosis, these participants’ experiences were reflected as risk perceptions. Disclosures were often motivated by making sense of their risk and talking through their medical options, which was further compounded by rapidly advancing fertility and genetic technologies that gave them options for managing their BRCA-related cancer risks and family planning. Two subthemes emerged—individual risk perception disclosures and familial risk perception disclosures.
The first subtheme was individual risk perception disclosures. Although both men and women experienced uncertainty regarding their risk, women grappled with individual risk when making disclosures about managing BRCA-related cancer risks and family planning. Women made disclosures to family members to explore what medical options would lead to the best prognosis. For instance, due to the uncertainty of how her insurance might affect her family planning decision-making, a female participant (BRCA1, married with children) revealed information about family planning decisions to her in-laws: “Because my father-in-law had a career in medical insurance. So, he was always helpful in trying to help deal with any medical insurance issues I was running into.” Another female participant (BRCA1, married with children) also disclosed information about family planning to her sister: But my sister had to do IVF to have her first child, who she was pregnant with when she got her cancer, and they knew they were going to have to do IVF to have a future child, which they ended up not being able to do just because of the timing. But they had been planning, if they were going to do it, they were going to do the preimplantation genetic diagnosis [PGD] since they were doing IVF anyway. They figured they might as well.
She disclosed her family planning decisions to her sister because she had recently made similar decisions and could therefore help her manage her prognosis.
The second subtheme was familial risk perception disclosures. Because genetic mutations can be passed throughout generations, participants often made disclosure decisions not for themselves but for their children. Although a few women disclosed information about BRCA-related cancer risks and family planning decision-making because they were concerned not only for future generations, this concern was more prevalent among men. Men disclosed not because they were worried about their own risk but rather because of the future risk of their children and grandchildren. The most prevalent disclosure conversation men had was with their children, particularly their daughters. For example, one male participant (BRCA2, married with children) noted that his first phone call after receiving his positive BRCA genetic test results was to his daughter due to her potential BRCA-related cancer risks. He explained why he called her first: I think the reason it was to my daughter is because it’s more the family history that, you know, that, and I knew that she, and I knew she’d act on it. It was the easier discussion. Not that my son was difficult. It just, it was more important to her.
After disclosing to his wife, a different male participant (BRCA2, married with children) also disclosed his positive BRCA test results to his daughter before his sons because of his granddaughter’s potential risk. He explained his thought process after receiving his results: “First, it was confirmation of what was anticipated, then the relief of the minimal risk, and then concern for my granddaughter, although there’s nothing to be done about it [now].”
For men who had nonadult children, when disclosing their BRCA mutation status to their partners, participants still focused on their children rather than on their own risk. For instance, one male participant (BRCA2, married with children) explained that the disclosure conversation focused almost exclusively on his children. He told his wife: “Okay, here are the things we have to do to get, [and] we obviously have to get our daughter tested first and foremost, and our son, as well. But especially our daughter.”
It is also important to note that when making these disclosures, participants reported difficulty due to the fact that their intended family members had a more serious prognosis. They felt caught between wanting to disclose to family members and feeling pressured not to disclose because other family members had a more serious prognosis. A female participant (BRCA2, single with no children) discussed waiting to disclose to her family about her hereditary cancer risk until after her sister had completed cancer treatments. She said, I wasn’t really talking that much to people because I didn’t want to create this drama around me when my sister is dealing with every aspect of organizing her treatment, and recovering from her mastectomy, so I just was waiting.
Another female participant (BRCA2, single with no children) felt something similar when she concealed information about decision-making because she didn’t want to stir up negative feelings in her family again. She stated, “My family had been through theirs. They’d had their cancer, and it felt like talking about it was just bringing up more bad stuff, and making them feel bad, so I didn’t.” Likewise, a male participant (BRCA2, married with no children) explained how he did not heavily discuss his positive BRCA test results because his sister was undergoing cancer treatments at the time, and he was more focused on her treatment and recovery. He recounted, I told my sister I had it, and we talked about that briefly, but I wasn’t the one with the cancer. She was. She had to focus on battling cancer . . . And I didn’t want to burden her in a way of talking about it because, candidly, I didn’t sense that there was a great threat to me as opposed to the great threat that she had. And why talk about something that she’s battling, and she certainly was scared? My main concern was her, not me.
Clearly, participants who had family members diagnosed with a more serious prognosis influenced when and how they disclosed their own BRCA-related cancer risks and family planning decision-making.
As a whole, uncertainty about whether or not they would develop cancer and how that risk might influence their family planning as well as future generations drove disclosure decisions. Women made individual disclosures to manage their hereditary cancer risk and evaluate their options for family planning, whereas men made familial disclosures due to future concerns about their children and grandchildren. Also, because participants often managed their own disclosures based on comparing their own risk to the prognosis of other family members, assessment of prognosis can become a family assessment rather than an individual assessment.
Relevance to Others
The last—and one of the strongest motivators to disclose information about BRCA-related cancer risks and family planning decision-making—was whether or not participants perceived the information to be relevant to the recipient. Relevance to others included the following three subthemes: duty to inform, advocacy efforts, and lack of disclosure to male family members.
The first subtheme was duty to inform. Participants disclosed about BRCA-related cancer risks and family planning decision-making under these two conditions: (a) when they felt a family member was also at risk of having a genetic mutation and (b) when a romantic partner might need to know the information. To begin, participants disclosed to family members who were also at risk for testing positive for BRCA. A female participant (BRCA1, married with children), for instance, disclosed her BRCA genetic test results in a formal letter to her extended family because she “wasn’t sure what information they really had or what they knew about BRCA.” The letter included her specific genetic test results, general BRCA-related cancer risks, and required screening for her family members who were at risk for testing positive. Another female participant (BRCA1, single with no children) talked about her intentions to disclose to her cousin someday about her decision-making: “It’s going to be something that my sister and I will probably speak more with her about and kind of help guide her through it because by then we’ll have more knowledge and experience with it.” A male participant (BRCA2, married with no children) disclosed his BRCA mutation status to his brother due to his potential BRCA-related cancer risks: I suggested heavily that he go get tested, and he just kept blowing it off. He eventually did do some genetic testing because he and his girlfriend at the time were going to have a baby. But he was unable to tell me if he had tested for BRCA2. He told that me that his girlfriend had, and she had come back negative, but he could not clearly articulate that he had a BRCA2 test done or not. To this day, I still don’t know if he even he did it or not.
Finally, participants disclosed to spouses/partners that would need to know the information for family planning purposes. One male participant (BRCA1 in the family, divorced with children) recounted his disclosure to his girlfriend at the time because he believed it was important information for her to know for family planning decisions. He explicated, When we were going through my mom’s [cancer] treatment and everything, we just talked about it—what BRCA is, the risk there, what my risk level was, what my daughter’s risk level was, and then any future children that we may or may not have, what that risk kind of looks like.
A female participant (BRCA1, single with no children) also disclosed her BRCA mutation status to her then-boyfriend because she knew they both wanted children. She narrated the conversation saying: I said to him, “What if I can’t have kids? What if, God forbid, something happens before we’re ready in our lifetime’—in our family planning to do that, and [then] I have to get my ovaries out earlier, or if I had cancer earlier. And he said, well, then you—we would adopt or we would foster. We would find another way to be parents.
Overall, participants disclosed to others when the recipients had experienced a similar situation and for family planning purposes.
The second subtheme was advocacy efforts. Participants’ disclosures did not stop with family members but also extended to advocacy. In other words, participants’ justification of relevancy-based disclosures was framed as a moral obligation to educate or warn others about BRCA-related cancer risks. One female participant (BRCA2, married with children) summarized the moral obligation she felt for being active in advocacy groups to reveal information about her decision-making: I’ve just realized there are so many women who feel like I felt, and my goal is that nobody feels like that. I can’t bear it when people say, “I’ve never met anyone else with a mutation,” because to me it’s so common. I don’t want people to feel lonely and like they don’t have anyone to talk to.
Another female participant (BRCA1, married with children) also discussed how she felt it was her job to educate people about BRCA and the impacts it can have on a family, “I feel like sometimes it’s my job to advocate for myself and for other people with gene mutations, and to educate people.”
Although the majority of men in this study did not discuss an obligation to inform others, there were two exceptions. The first exception was a male participant (BRCA1, married with children) who created a Facebook group for men who tested positive for BRCA or were at risk for developing BRCA-related cancers due to a BRCA mutation in their family. He explained that the reason why he created the group was to share information knowledge to other men as information for men was lacking. The second exception was a different male participant (BRCA1 in family, married with children) who explained that his sister asked him to conduct the interview for this study, so he could be an advocate for the men in their family, demonstrating the need to communicate about BRCA-related cancer risks. He said, “I want to make sure that my kids, nieces, and nephews have information early in their adulthood that they can make those decisions for testing, and if they want to have children that they understand what the risks are.” In contrast to other men in this study, these individuals prioritized disclosing their BRCA-related cancer risks and family planning decision-making to others.
The final subtheme of relevance to others was lack of disclosure to male family members. Some participants did not disclose BRCA-related cancers and family planning decision-making to the men in their family because they thought the information was not relevant to how that family member would manage their health. For example, women felt that their disclosures to the male family members did not need to be as in depth or as frequent because men’s risks are not as severe as women’s. One female participant (BRCA1, single with no children) said she felt uncomfortable talking about a “women’s cancer” with her father and brothers: I actually still haven’t really had the conversation with my dad or my brothers, and it’s just having a view for a women’s cancer issue. It’s a little awkward to talk to your dad about. I still want to talk to my brothers about it, because they need to know exactly what their risk is and what they should be doing, and that they might need to get tested.
This participant’s experience demonstrates some women’s discomfort with disclosing BRCA-related cancer risks and family planning decision-making to their male family members.
Yet, men were also less likely to disclose their male family members. After receiving his positive BRCA test results, one male participant (BRCA2, married with children) called his daughter, not his son. He explained he did not disclose to his son first because he did not see disclosing the genetic test results as important to his son because if his son did test positive for BRCA2, his cancer risks were significantly lower than his daughter’s potential risk. Interestingly, a different male participant (BRCA2, married, 3 children) stated that if he had not conducted the interview for this research study, he would not have discussed his BRCA-related cancer risks with his two sons. He expounded, Since I’ve had this discussion with you, I probably will mention it to him at some point in time, but it’ll be a short discussion. Otherwise, had I not had this discussion with you, I wouldn’t mention it to him when we were up there. The discussion with you will prompt me to do that. It just wouldn’t have come up otherwise. In the case of my youngest son—and he’s over 50 now as well. He’s 51—Anyhow, in the case of my youngest son, the issue, we haven’t really discussed that. He could still have children, and if he did get married, then the issue would—I would clearly have a discussion with him . . . If he were considering marriage, clearly, I would have a discussion with him about that. There’s just no doubt about that whatsoever.
Although men do not carry the high percentage risks of developing BRCA-related cancers that women do, they do have increased risks over the general population, and they have equal chances of passing the mutation to their children (Bratt & Loman, 2015). Yet, both women and men routinely disclosed less to their male family members about their BRCA-related cancer risks and family planning decisions. The tendency for men and women not to disclose to men due to a perceived lack of relevancy is problematic and could have health and family implications. In sum, participants assessed the relevance of information to others before disclosing their BRCA-related cancer risks and family planning decisions. Although many chose to disclose information to most of their family, some did limit the disclosures they made to the men in the family.
Discussion
This study examined the ways in which men and women assess both information and the recipients of disclosures when making disclosure decisions about BRCA-related cancer risks and family planning decisions. We begin by discussing the results of this study, followed by noting implications, limitations, and future directions.
Although previous research has investigated how families communicate about hereditary cancer risks (Chivers Seymour et al., 2010; Forrest et al., 2003; Koehly et al., 2009; MacDonald et al., 2007), little has looked at disclosure of other health care decisions related to BRCA-related cancer risks such as family planning decisions (i.e., Dean & Rauscher, 2017). Moreover, although a significant body of research has examined women’s experiences managing their BRCA-related cancer risks with some focusing on men’s experiences (S. Hesse-Biber, 2014; S. Hesse-Biber & An, 2017; Hoskins & Greene, 2012; Howard et al., 2011; Moynihan et al., 2017; Rauscher & Dean, 2017), minimal work has assessed both men’s and women’s approaches to communicating and managing those risks for themselves and their family. This study filled these gaps by revealing that men and women assess both the information they wanted to disclose as well as how the recipient of the disclosure would react to that information in similar and different ways.
Similarly, for disclosures to occur, participants needed to feel prepared themselves but also believed that their intended recipients were prepared for such disclosures. Participants with strong family histories of BRCA-related cancers tended to be more prepared to make disclosures. This finding supports past research indicating that individuals with a more extensive family health history of hereditary cancer risk are typically more informed and open about that risk with others (Wilson et al., 2004). In addition, participants disclosed their BRCA-related cancer risks and family planning decisions to family members who had similar experiences in contrast to friends who could not understand what the participants were experiencing. This finding also supports previous research showing individuals at an increased risk for developing hereditary cancer are more likely to disclose to others who have been through similar experiences (Chivers Seymour et al., 2010). At the same time, the results also extend past research, noting that families where the mutation was not always obvious struggled more with disclosing of BRCA-related cancer risks and family planning decisions than families who had family members diagnosed with cancer and/or family members who tested positive with the BRCA mutation.
Moreover, participants assessed the relevance of information to others, which was influenced by gender. Although participants disclosed their BRCA-related cancer risks and family planning decisions to the majority of their family members, both men and women often did not disclose to their male family members. Participants reported leaving men out of cancer prevention and family planning conversations because they felt the information was not as relevant to their male family members. A few women reported disclosing to male family members who were also at risk for carrying the mutation, yet these women largely left their male family members out of any conversations especially regarding preventive surgeries and family planning decisions. In addition, men noted disclosing to their spouses and daughters first before disclosing to their sons. This finding is somewhat supported by previous research showing private disclosures related to sex or to members of the opposite sex are often difficult (Rauscher & Durham, 2015). Furthermore, past research has shown that communicating about health is often done by women within families (Heisler, 2005). Thus, the proclivity for women to be the primary disseminators of health and genetic information, combined with women not disclosing to men, points toward a problem with how men are receiving information about BRCA. Overall, although this tendency to exclude men may be due to men’s lower BRCA-related cancer risks (Bratt & Loman, 2015), this exclusion has implications for at-risk men’s health as well as their family. For one, the lack of transmitting information to men who are also at risk for carrying a BRCA mutation could lead to men making decisions on insufficient information. Also, men’s lack of information may affect their ability to present information to their children.
Different though were the ways in which men and women disclosed their BRCA-related cancer risks and family planning decisions. Analysis revealed women made individual disclosures about risk, whereas men made familial disclosures. Women disclosed information to others through their desire to seek more information about medical treatment options for both hereditary cancer prevention and family planning. In doing so, they were managing the uncertainty of their increased risk for HBOC (Dean & Davidson, 2016). This finding is largely supported by existing research that demonstrates individuals with an increased risk for developing hereditary cancer make disclosures to seek information (Forrest et al., 2003). Yet this finding also extends research as men disclosed information due to their concerns about the future prognoses of their children and grandchildren (S. Hesse-Biber & An, 2017; Rauscher & Dean, 2017). In other words, men’s accounts demonstrated that the family is not simply viewed as a support system but also a collective that must manage their own risks and make their own disclosure decisions. Overall, these data reveal making disclosure decisions BRCA-related cancer risks and family planning is complicated, especially due to the familial nature of HBOC.
Theoretical Implications
The results from this study have several important implications for the DD-MM. Analyzing disclosures about BRCA-related cancer risks and family planning decision-making in the framework of the DD-MM highlights unique ways individuals simultaneously assess both the information they want to disclose and the person to whom they wish to disclose. Implementing such a theoretical framework deepens our understanding of how the interplay of multiple illness factors influence individuals’ disclosure of information about family planning and hereditary cancer risk, rather than focusing on the sole influence of any one factor.
One implication is the use of the model to analyze hereditary cancer risk. Although it could be argued that analyzing many illnesses from a family perspective is important, nowhere is it more important than with genetic disease. Currently, most tests of the DD-MM focus on illnesses that are often managed (or can be managed) at an individual level (i.e., HIV; Checton & Greene, 2012; Derlega, Winstead, Greene, Serovich, & Elwood, 2004). Yet, although genetic disease can be managed at an individual level, it is more often managed at a familial level (Rauscher, Hesse, Miller, Ford, & Youngs, 2015). In analyzing a health concern that commonly occurs in familial groups, several components of the DD-MM became more (or less) salient than in previous research. For example, the role of preparation in information assessments for participants was unique compared with previous tests of the DD-MM. Because our participants were often aware of the prevalence of hereditary cancer in their family, their preparation in understanding their risks and their preventive options often stimulated open communication that encouraged more disclosures. However, preparation was less salient as well because the flow of communication was so open they often did not assess the information nor the recipient before making disclosures (Venetis, Greene, Checton, & Magsamen-Conrad, 2015). In this way, preparation and misconceptions intertwined to predict the level of openness with which participants approached making disclosures. In showing the importance of preparation for both the discloser and recipient, the results of this study show additional complexity of the DD-MM concepts.
Finally, the results have implications for both the prognosis category of the DD-MM. These participants were aware of their BRCA-related cancer risks but had not been diagnosed with HBOC. Their disclosures were primarily driven by their desire to reduce uncertainty and seek more information to help themselves or their family members manage their risk, prevent cancer, and learn more about their family planning options. This focus on managing risk as proactive instead of reactive highlights the unique case of hereditary cancer risk in the DD-MM model and points toward the need to better understand how the model works differently for different illnesses. To further understand the application of the DD-MM to the context of hereditary cancer risk, future research should utilize, even test, this model in this context.
Practical Implications
Results of the current study also have practical implications. First, education of nonaffected family members and the general public is desperately needed. Participants reported a desire to disclose more to family members or friends, but due to the disclosure recipient’s ignorance and/or insensitivity about hereditary cancer risk and its implications, participants often felt they could not disclose to certain recipients. This motivation for concealing was especially problematic when recipients were individuals who were not at the same risk for hereditary cancer as the participant (i.e., friends, in-laws). More effort needs to be put into educating the public about hereditary cancer and the implications of living with a mutation. Although a number of scholars (Parrott et al., 2004), government agencies (CDC.gov), and advocacy organizations (facingourrisk.org) have studied the education of lay audiences and have attempted doing so, it seems the level of education of the general public about hereditary cancer risk is still a barrier.
Related to the need to educate the general public about hereditary cancer risk, members of an at-risk mutation carrier’s support system should also be educated on ways to make themselves a more supportive recipient of disclosure. Although we acknowledge that not all people want to be open about their BRCA-related cancer risks and family planning decision-making, research shows that most mutation carriers tell at least first-degree family members (Koehly et al., 2003) and require high levels of social support during decision-making (Werner-Lin, 2008). Therefore, it is important to educate family members (both those at risk for having the same mutation and those not at risk) on how to provide the best support. Health care providers and genetic counselors are especially essential to educating family members. Given this study’s results, suggestions for teaching family members to be better recipients of hereditary cancer risk disclosures include (a) being open; (b) getting informed about risks, preventive surgeries, and family planning options; (c) respecting decisions and privacy; (d) providing unconditional support; not judging decisions; sharing experiences (if solicited); and (e) considering pre-existing family dynamics. Each could be pieces of advice provided to members of a patient’s support network as strategies to help provide the patient with better support.
A final practical implication is a need to address inequities in conversations about BRCA. Participants’ accounts showed men and women are not consistently communicating about BRCA to men. Based on the lack of communication in families where the mutation is passed by men and the lack of communication about BRCA with males in the family, it is clear a gender imbalance has emerged in conversations about BRCA. Although many may consider this gap natural because BRCA often has more severe impacts on women, men are still affected by experiencing an increased risk of developing breast, prostate, and pancreatic cancer as compared with the general population (Bratt & Loman, 2015). They also have a 50% chance of passing a mutation to their children. Due to these impacts, it is important to garner a better understanding of how men navigate conversations about BRCA-related cancer risks, why they are commonly not included in these conversations, and how to get them more included in the sharing of BRCA information. Health care providers, genetic counselors, and public health campaigns are starting points for disseminating information about BRCA more broadly to men and for probing into justifications for excluding men from BRCA conversations.
Limitations and Future Directions
The strengths of this study need to be interpreted in light of a few limitations and possible future directions. First, although this study focused on how information is shared within a family, it only focused on the perspective of one member of the family. Future research should investigate how information about hereditary cancer risk and family planning is managed by multiple members of the family. Second, the self-selecting nature of the data collection was also a limitation for this study. It is likely that most individuals who participated in this study are those who are open with family members. Finally, participants tended to be well-educated, had incomes above US$100,000, and were all White; this is a limitation of purposive sampling, and as such, the generalizability of the claims made from this data is limited. Moreover, because participants were recruited at a conference dedicating to informing the public about hereditary cancer, it is likely that participants were personally invested in participating in this research. Future research should investigate whether similar themes emerge in more diverse populations.
Footnotes
Acknowledgements
The authors would like to express gratitude to Facing Our Risk of Cancer Empowered (FORCE) for allowing them to recruit participants and thank the BRCA-positive men and women for sharing their experiences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Texas A&M University’s College of Liberal Arts Seed Grant.