
Abstract
Many policy interventions have attempted to address the entrenched disadvantage of Aboriginal Australians1; however, sustained improvement in social, cultural, physical, and emotional well-being is not evident. This disadvantage is compounded by paternalistic practices which do not promote Aboriginal self-determination or empowerment. This article presents the lived experience and voice of Aboriginal Australians spending time in parks in Perth, Western Australia. A community-based participatory action research approach informed by critical Indigenous methodologies involving collaboration between Aboriginal and non-Aboriginal service providers was used. Participants experienced disconnection from kin and country, serious risk to personal safety, homelessness, and problematic health; all related to, and intersecting with, time spent in the parks. The participants’ narratives highlight the enduring impacts of colonization, dispossession, and racism. These lived experiences are situated within contexts of rising moral panic from politicians, residents and mass media, and siloed policy and service delivery responses.
Keywords
Introduction
This article reports on a participatory and collaborative research project that explored the lived experiences of Aboriginal people who spend time in public parks and places in Perth, Western Australia. The research aimed to bring to light the voices of “people in the parks,” which had been rendered silent amid the dominant discourse which focused on “anti-social behaviour” and community disruption. The research reported here was a subset of a larger action research evaluation of a newly funded service considered innovative as it comprised both assertive outreach and community liaison. The outreach service was developed and funded in response to sustained objections by residents, businesses, and politicians about the perceived disruptive behaviors and impact on community and business. Some groups called for a curfew which would limit and exclude Aboriginal people from these public spaces (Guardian Express, 2014). In response, service providers working in the parks claimed that most people in the parks were “stuck” in the city, receiving essential, city-based treatment, such as renal dialysis, unavailable in their rural, regional, and remote home areas. Despite a number of health, alcohol and other drug, homelessness and Christian charitable organizations providing services in the parks, most people in the parks were reported to have poor health, safety, and well-being outcomes. Their experience of displacement, however, was rendered invisible in the cacophony of voices focused on their removal from these areas. This research aimed to balance the dominance of service provider, community, and business discourses by providing an opportunity for the voices and experiences of the people in the park to be heard and considered in relation to the intersections of health, well-being, homelessness, and Aboriginal dispossession.
History and Context of the “Problem”
This research was conducted alongside a larger evaluation of a new service focussing on improving the health and well-being of the people in the parks via two services: an assertive outreach program for the people in the parks and community liaison with businesses, service providers, the community, and other key stakeholders. Although it was not named as an Aboriginal-specific service, the funder expected the program to operationalize “cultural security frameworks” and align to the Western Australian Aboriginal Alcohol and Drug policy (Government of Western Australia: Drug and Alcohol Office, 2011, p. 3). Although the target group were Aboriginal people, the development of this new service delivery model did not consult with Aboriginal communities, service providers, or those with lived experience of issues such as spending time in parks, health problems, and homelessness.
An understanding of the physical space of the parks, the differences between these two locations and the significance to local Aboriginal people are important in understanding the context and research findings. The two inner city locations for the new service were Perth, the capital city of Western Australia, and Fremantle, a city located 16 km from Perth. These two locations have been gentrified over 20–30 years, with a concomitant increase in land value.
Cultural, spatial, and historical differences distinguish the two locations: The Perth location primarily involved one medium-sized park (Wellington Square), located at the edge of the central business district, adjacent to the city’s main public hospital and train station. This park’s proximity to the hospital has meant it is a place where Aboriginal people and accompanying family members from remote and regional areas up to 2,300 km away have congregated (Jones, Cox, & Cozens, 2016). Alongside apartment development, the area around the park includes food outlets catering for the employees of surrounding government departments and services (including an Aboriginal-specific health service) and is also used by community groups for sporting events and concerts. With gentrification, the park became a contested space, exemplified by the City Mayor suggesting in 2014 that service provision in the park should be re-located so that local residents could have “respite” (Perpitch, 2014).
The Fremantle location involved a number of parks and urban spaces offering similar amenities to those in Perth with a main train station, churches, retail and food businesses, and a variety of services, including the Local Government authority. The Fremantle area was subject to a “move on” policy from local Police, meaning that many street present people were regularly excluded from the area for 24 hours. The parks in both locations included public toilets, grassed areas, and water fountains. These amenities are managed by Local Government authorities, with community rangers the first contact point for issues pertaining to community safety and “suspicious” behavior.
Both locations have historical and current significance for the Noongar people, the traditional owners of the land. The Noongar people have resided in the south-west of Western Australia for over 45,000 years. Noongar boodja (the country) extends from Yued (Jurien) in the north to Balladong (Moora) in the east to Wagyl Kaip (Bremer Bay to Esperance) in the south (South West Aboriginal Land and Sea Council, 2016). Whadjuk is the dialect for the region and regardless of the location, “Noongar people have a profound physical and spiritual connection to country” (South West Aboriginal Land and Sea Council, 2016). The Whadjuk Noongar people’s historical use of the Perth park is significant as the area was a traditional place to meet kin, camp, and hunt for food (South West Aboriginal Land and Sea Council, n.d.-a). However, Aboriginal people’s access to the area was restricted with white “settlement” and further constrained in 1927, when Aboriginal people were prohibited from entering a 5-km area of the city after 6 p.m. without a “native pass” (South West Aboriginal Land and Sea Council, 2017). Therefore, nearly 90 years later, the calls for curfews and exclusion were, unsurprisingly, experienced as racist and insensitive by Aboriginal people and their supporters (Guardian Express, 2014).
The Research and Social Policy Context
This research has been undertaken in the context of a paucity of research evidence on the lived experience and perspectives of people in the parks, with one study undertaken by Watkins (2012) in the Fremantle area. Although Watkins’ (2012) study was undertaken without institutional ethics approval or peer review, it did provide an opportunity for the people in the parks to voice their concerns, experiences, and needs. An Australian study by Parsell and Phillips (2013) of Indigenous people in the Northern Territory documented public perceptions of “anti-social” behavior and service delivery responses. These service delivery responses were similar to Fremantle in that they involved excluding people and moving them on. Another Australian study exploring categories of Indigenous homelessness argued that policy and service delivery responses were myopic, using “reactive policing” (Memmott, Long, & Chambers, 2003, p. 39) which exacerbated the problematic intersections between health, homelessness, and social and cultural issues.
In relation to social policy, a wide range of responses and interventions from all levels of government are evident, yet Aboriginal Australians (who comprise 3% of the Australian population) continue to experience entrenched disadvantage, reflecting the ongoing and enduring impacts of colonization and limited opportunities to enact self-determination (Australian Indigenous HealthInfoNet, 2016; Yu, 2012). Given the plethora of federal policies, we focus our discussion on the two most pertinent: “Closing the Gap” and Income Management. While housing and homelessness policy would seem highly relevant, the period in which this research was undertaken (2014–2016) represented a policy vacuum and inertia in homelessness in Australia (Homelessness Australia, 2015). Therefore, we do not consider homelessness policy in our discussions here.
The Closing the Gap policy framework targets health and social inequities for Aboriginal Australians. The Income Management policy framework is for all Australians in receipt of government income support and claims to prioritize the well-being of children and families. These policies provide the context for the experiences of the people in the parks by first targeting Aboriginal Australians, second being relevant as the majority of Aboriginal people spending time in the parks were in receipt of income support, and third, highlighting a paternalistic policy approach of “doing to,” rather than creating the conditions for, self-determination. The research reported here sought to counter such paternalism by providing a mechanism for people in the parks to speak of their own experiences and hopes and which reflects calls by Aboriginal and Torres Strait Islander people and their allies for policies, interventions, research, and responses which privilege Indigenous self-determination (Yu, 2012). In addition, simplistic calls to move Aboriginal people to other areas or back “home” reinforce this devaluation of self-determination and ignore that worldwide, “health care systems are not working for Aboriginal people” (Hole et al., 2015, p. 1662).
Closing the Gap policy responses commenced in 2005, resulting from the advocacy of the then Aboriginal and Torres Strait Islander Social Justice Commissioner, Tom Calma (Holland, 2016). After 13 years, this policy is reported to have made minimal or no progress in improving the health and well-being of Indigenous Australians (Australian Indigenous HealthInfoNet, 2016). Examples of this policy failing to meet its targets include continuing low birthweights, Aboriginal Australians being almost five times more likely to live in overcrowded housing and comprising 27.1% of the homeless population, suicide rates are close to double that of non-Aboriginal Australians, and less than half (47.5%) of Aboriginal Australians are engaged in the labor market (Australian Indigenous HealthInfoNet, 2016; Australian Institute of Health and Welfare, 2014). Aboriginal Australians are much more likely than their non-Aboriginal counterparts to experience major health problems such as cardiovascular, respiratory, and circulatory diseases; diabetes and end-stage renal disease (Australian Indigenous HealthInfoNet, 2016); experiences which are further complicated by high levels of substance misuse, family violence, and imprisonment (Australian Bureau of Statistics, 2016; The National Indigenous Drug and Alcohol Committee, 2014).
While the majority of Aboriginal Australians are located in urban and regional areas (Commonwealth of Australia, 2016), the health disparities for all Australians living in rural areas are significant and result from distance, limited service availability, and reduced resource opportunities (Harvey, 2014), with disadvantage and social exclusion common outside metropolitan areas (Australian Institute of Health and Welfare, 2017). Aboriginal people from rural, remote, and regional areas requiring treatment such as renal dialysis travel to metropolitan areas with their families. However, in both metropolitan and regional areas, non-Indigenous health care systems rarely incorporate, or make space for, Indigenous worldviews (Mellor, McCabe, Ricciardelli, Mussap, & Tyler, 2016), with racist and judgemental responses found to contribute to poor health outcomes (Larson, Gillies, Howard, & Coffin, 2007; Waterworth, Dimmock, Pescud, Braham, & Rosenberg, 2016).
The second national policy significantly impacting, although claiming to not specifically target, Aboriginal Australians is known as “Income Management.” This policy commenced in the Northern Territory in Aboriginal communities in 2007 as a response to pervasive child sexual abuse and targets behavior stereotypically associated with welfare recipients such as child abuse, domestic and family violence, problematic alcohol and drug use, and “antisocial” behavior (Mead, 2000). The policy is said to extend the “history of paternalist management” (Bray, Gray, Hand, & Katz, 2015, p. 374) by Australian governments toward Aboriginal people. Income management excludes the purchase of alcohol, tobacco, gambling products, and pornographic material for those in receipt of income support (Commonwealth of Australia Department of Human Services, 2018). In Western Australia, Income Management is linked to statutory child protection services, with 70% of income support recipients subject to this policy, and 63% Indigenous (Australian Government Department of Social Services, 2014).
We conclude our discussions on the policy context by considering the State based Patient Assisted Transport Scheme (PATS). This policy directly impacted many people in the parks as it facilitated their relocation to the city for medical treatment. The scheme provided subsidized travel assistance to individuals from rural, regional, or remote locations for specialist medical treatment (Government of Western Australia, 2009). A 2015 parliamentary inquiry found that many people experienced significant financial disadvantage and homelessness after being transported to metropolitan areas by the PATS (Legislative Council of Western Australia Standing Committee on Public Administration, 2015). The Inquiry also found that travel to the Perth metropolitan area was overwhelming and isolating for many Aboriginal patients and accompanying family or carers (Legislative Council of Western Australia Standing Committee on Public Administration, 2015). The PATS was described as “overly bureaucratic” (Gartry, 2015), leading to people being “stranded” in Perth (Health Consumers Council of Western Australia, 2014, p. 1).
Method
We provide an overview of our methodological approach here with more detail in a forthcoming article. Critical Indigenous methodologies and principles from the Australian National Health and Medical Research Council (2003) informed the research approach, with a view to “transforming the institution of research, the deep underlying structures and taken-for-granted ways of organizing, conducting, and disseminating research and knowledge” (Smith, 2005, p. 88). Linda Tuhiwai Smith’s (2005, p. 92) framework guided our attempts to enact decolonizing research. Specifically, the focus on Indigenous self-determination and epistemic justice (Smith, 1999) resonated with the research project goals. Examples of enacting decolonizing research strategies (as proposed by Tuhiwai Smith, 2005) included questions raised by Aboriginal service providers forming the research questions for the project; co-design of the research framework by Aboriginal and non-Aboriginal workers, managers, and researchers; Aboriginal and non-Aboriginal outreach workers sharing their knowledge of the people in the parks to inform the research design; and Aboriginal outreach workers undertaking data collection and analysis. These approaches emphasize self-determination, epistemic justice, and the creation of spaces for re-storying away from colonizing gazes and practices.
Community-based participatory research (CBPR) further informed the project, and while it is acknowledged that no research methodology can decolonize (Castleden, Mulrennan, & Godlewska, 2012), or completely address power differentials, CBPR offered a way to explicitly talk about and work with “power differentials that characterise conventional research paradigms” (Green et al., 2013, p. 18). The academic researchers prioritized social justice, transformation, and accountability to Aboriginal people and research participants. This involved demonstrating trustworthiness, and working collaboratively in locating power, knowledge, and control with the Aboriginal research partners. Furthermore, the academic researchers sought to enact ongoing reflexivity in relation to their relative power and privilege as non-Aboriginal, social work academics. Through processes mentioned above, the research project unfolded and had a substantial lead up period, which we now discuss.
Identifying the Issue
Although there was general consensus among service providers about the reasons for people being in both the Perth and Fremantle parks, both Aboriginal and non-Aboriginal agencies reported that their knowledge was not considered credible evidence by policy makers and funders. Furthermore, these agencies asserted that academic research stood a greater chance of being categorized as legitimate. These conversations highlighted that the Aboriginal and non-Aboriginal agencies and academic researchers shared similar concerns about a lack of epistemic justice, yet ideas about the injustice differed. The service providers were troubled that their knowledge and voice were not seen as credible, whereas for the academic researchers, the injustice centered on people in the parks not being heard or valued. Despite these different ideas, it was agreed that a partnership between the agencies and academic researchers would be beneficial.
The academic researchers renegotiated the terms of the originally funded evaluation study to include the lived experience of people in the parks. This led to half the study reported here being funded from the evaluation project, with the remainder funded from University institutional funds. Agencies contributed in kind by releasing outreach workers to attend research meetings (design, analysis, and writing) and to undertake interviews. The academic researchers offered to reimburse the agencies for outreach worker wages and four of the five organizations advised that while they appreciated the offer, they viewed their in-kind contributions of wages as a signifier of the research partnership.
Cultural guidance and leadership
Senior staff from Aboriginal agencies and the academic researchers identified that the project could only proceed if it was connected to the Aboriginal community and was led by at least one Aboriginal Elder. Elders are known as “keepers of knowledge” (South West Aboriginal Land and Sea Council, n.d.-b) and ambassadors for culture and community; highlighting the significance of an Elder being involved in this project, for the Aboriginal and non-Aboriginal agencies, outreach workers, and academic researchers. An Aboriginal Elder (CT), who in addition to her standing in the Noongar community, was employed as an Aboriginal Capacity Builder in an agency delivering services to people in the parks, offered to take a leadership role in the research project.
After a number of meetings between Aboriginal and non-Aboriginal agencies, police, local government, and community members, a reference group of five agencies representing homelessness, alcohol and drug and health programs was formed. The reference group was considered important by all partners as it promoted cultural accountability and responsibility, provided culturally specific guidance and advice at different points of the project, and created the space for a range of opinions to be considered within a cultural context. The academic researchers were mentored by CT who led discussions on research design, methodology, and approach, drawing on her broad personal and professional experience; including as an academic researcher. The reference group accepted CT’s proposal that outreach workers from the agencies undertake data collection with the people in the parks, particularly as it was seen as a way to promote the exchange of cultural knowledge and practice wisdom, while also developing research skills.
Collaborative Research Design
The research was collaboratively designed between the reference group, CT, the outreach workers, and academic researchers. Three research objectives were collaboratively developed, based on the questions of Aboriginal and non-Aboriginal service providers and focussed on providing an opportunity for the voice of the people in the parks to be heard; building opportunities for exchange between Aboriginal and non-Aboriginal outreach workers, programs, and researchers; and developing evidence which could be used to advocate for improvements to the health and well-being of people in the parks.
Through the process of collaboratively designing the research approach, many of the outreach workers expressed uncertainty about their research knowledge and skills. In response, CT guided and supervised the academic researchers in the development and delivery of six workshops on topics such as interview schedules, informed consent, ethical considerations, probing and respecting a participant’s right to not respond, asking sensitive questions, responding to intoxication, and interviewing techniques. The workshops were designed on the grounds of mutual learning with the academic researchers learning about cultural frameworks and outreach work and outreach workers reporting that they expanded their research knowledge and skills. Furthermore, the workshops provided the outreach workers with opportunities to network and build shared understandings of the experiences of the people in the parks.
During the workshops, some of the Noongar outreach workers expressed uncertainty about interviewing people from other regions in Western Australia, and CT facilitated discussions which highlighted that some workers had limited exposure to, or conversations with, Aboriginal people from other parts of Western Australia. As most of the non-Aboriginal outreach workers were well known to people in the park, CT proposed that the non-Aboriginal outreach workers introduce their Aboriginal colleagues while also demonstrating their approach to building rapport and trust. As some outreach workers had family, cultural, or professional connections with people in the park, the issues of conflict of interest, informed consent, and noncoercive engagement were particularly important. Outreach workers role-played conversations in areas they thought could be awkward once they entered the field and this included how to explain that participating in the research had no impact on the receipt of services from any of the agencies involved in the research project. The potential for conflict of interest, pressure to participate, and cultural safety were further balanced by the pairing of male and female outreach workers from different agencies and programs during data collection, meaning that the likelihood of existing professional relationships was minimized.
Institutional ethics approval was obtained from the WA Aboriginal Health Ethics (HREC 650) and Curtin University (HR 175/2015). In keeping with the co-design approach used in earlier stages of the research, this article was prepared and authored by the academic researchers, the outreach workers, and the Aboriginal Elder. The academic researchers vested ownership of the report with a lead Aboriginal agency involved in the research project. This stance reflects the academic researchers’ view that the material is not theirs to own—rather it belongs to the Aboriginal community.
Data Collection and Co-research
Data were collected by teams of two to three outreach workers, involving mixed gender and Aboriginal and non-Aboriginal outreach workers. Potential participants were approached by outreach workers who explained the study. Written consent was obtained from 61 participants between November 2015 and April 2016. This involved 46 interviews in Perth and 18 in Fremantle. Three people were interviewed twice in Perth by different outreach workers and this duplicated interview data were excluded. In total, 35 women and 26 men participated, and four people chose to be interviewed in pairs (participant responses were disaggregated and considered as individual contributions). In all, 14 of the 61 interviews were conducted by a non-Aboriginal outreach worker who had Aboriginal marriage connections and was considered by other outreach workers and people in the parks to have legitimate kin connections.
The co-designed interview guide explored the following: how people came to be in the parks, housing and homelessness, safety, health and well-being, how time was spent while in the parks, and, finally, messages for other people about life in the parks. These topics were developed collaboratively and reflected the personal and professional experiences of the outreach workers, CT, and the academic researchers. In addition, the interviews asked people about their knowledge and experience of the service which was being evaluated (not reported here). These questions were only asked by outreach workers from other services to avoid conflict of interest. The interview approach was conversational and relied on “yarning”; a form of informal storytelling reflective of Indigenous Australian communication methods (Bessarab & Ng’andu, 2010). Participants were offered a $20 (AUD) retail gift voucher upon completion of an interview. An interpretive and critically reflective meeting of the outreach workers, academic researchers, and CT took place shortly after each round of interviews.
Collaborative Data Analysis
Interpretation and analysis of data were facilitated by CT and undertaken collaboratively by the outreach workers and academic researchers. This is similar to the approach adopted in a Western Australian Indigenous health study by Waterworth et al. (2016) in that it involved discussion, exploration, questioning, and agreement on emerging codes and themes. An inductive and iterative approach guided the analysis, enabling the research team to draw on the insider and lived experience knowledge of the outreach workers and CT (Smith, 2005). Analysis followed Braun and Clarke’s (2006) suggestions for thematic analysis with all team members familiarizing themselves with the transcribed and collated interview data. Through discussion, questioning and reflection led by CT, the team developed codes which were considered in terms of similarities, differences, patterns, and prevalence, leading to the generation of themes (Bernard & Ryan, 2010). Much of the analysis occurred at the semantic level (Braun & Clarke, 2006, p. 84), where participants’ words and phrases informed the development of themes.
The outreach workers valued quantified findings as they believed this provided a form of legitimacy to their observations and epistemic framing of the issues for people in the park. The outreach workers said this provided a way to talk about the size and nature of the “problems” people faced while spending time in the parks. Furthermore, it mirrored their everyday realities as many of the workers were subject to measures which accounted for their professional practice with key performance indicators and output measures. The academic researchers accepted this, and in some areas, descriptive statistics were generated to represent the frequencies and prevalence of particular experiences.
The analytic and interpretive approach promoted a form of trustworthiness in relation to the emergent categories and themes by considering Aboriginal cultural values and practices alongside the outreach workers’ knowledge. These activities mirrored the CBPR principles underpinning the project, with the team iteratively and recursively developing shared understandings and meanings (Clark & Ventres, 2016). In this process, exceptions, commonalities, and patterns were noted. At the request of the outreach workers, the academic researchers wrote up the collaborative analysis for the workers’ consideration, amendment, input, and endorsement.
Findings
The collectively derived findings highlight the various ways in which participants came to be in the parks and their lived experiences of housing and homelessness, safety and risk, health and well-being, and service delivery encounters. As such, they are a re-presentation of the participants’ experiences and an attempt to address the pervasive silencing of their voices. While major themes are identified, a range of sub-themes are also addressed, highlighting the complex and intersecting experiences of dispossession, culture, health, homelessness, well-being, and social connectedness.
The significance of home and “country” was expressed by the majority of participants (72%) and this reflects the framing of the issues by service providers who spoke about people being “stuck” in the city for medical treatment or experiencing long-term homelessness. Few people felt able to return to country, and if it did occur, it was short-term: People going for a funeral, they risk their life . . . they get sick and get sent back on the doctor plane.
Family supporters reported that it was not culturally acceptable for them to return home and leave their loved ones alone, away from home and kin. Furthermore, the ongoing impacts of government policies were cited as a barrier to return to country: Too sad to go home . . . from Stolen Generation
2
and lots of pain at home . . . stressed from loss.
The reasons for coming to the parks or public places varied and those in Perth were more likely to report medical treatment: Came down from Laverton with family, got stuck here.
In contrast, Fremantle participants were more likely to report homelessness as the reason they came to the parks. Figure 1 details all reasons for coming to the parks, according to location.
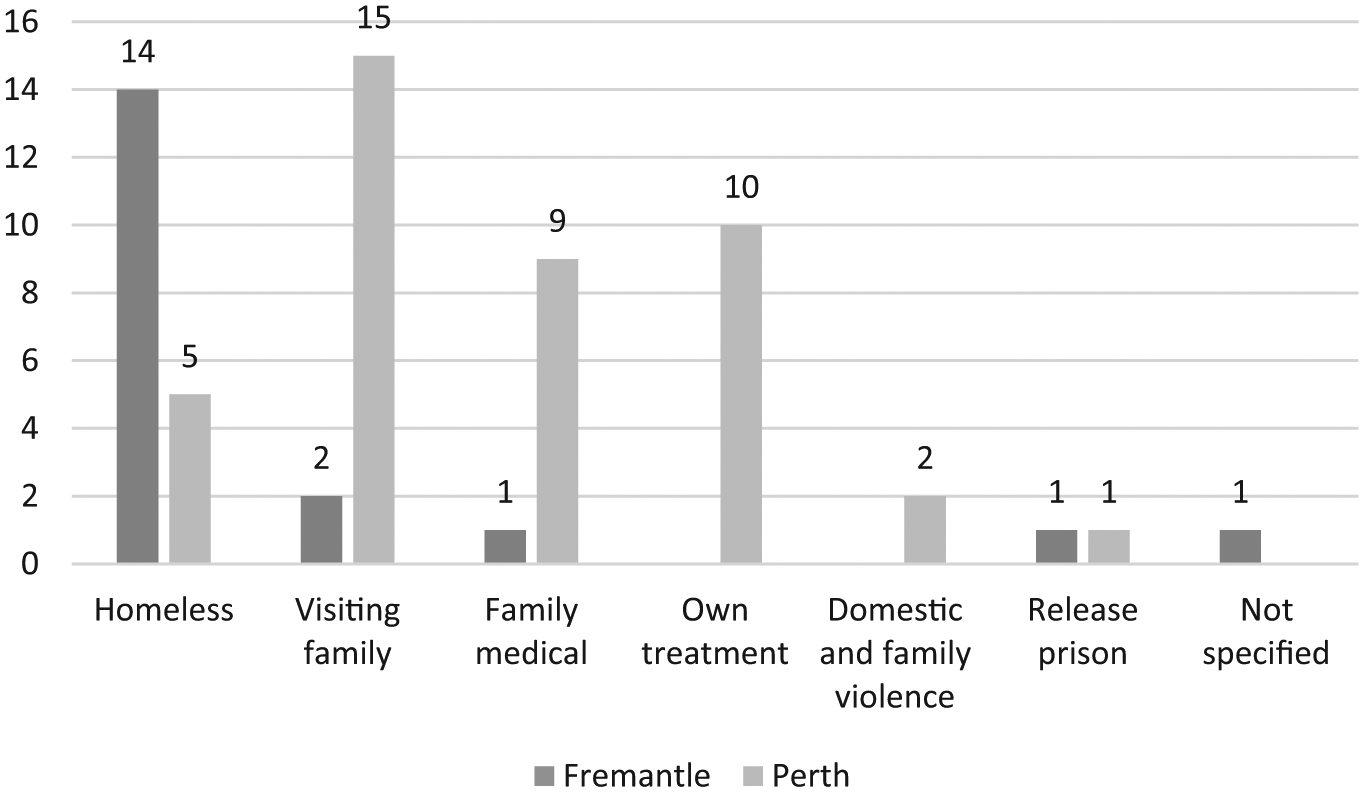
Original reason for being in parks.
Participants estimated that they had spent between “a few days” to 30 years in the parks and Figure 2 highlights the estimated average period of time spent in the combined Perth and Fremantle parks.
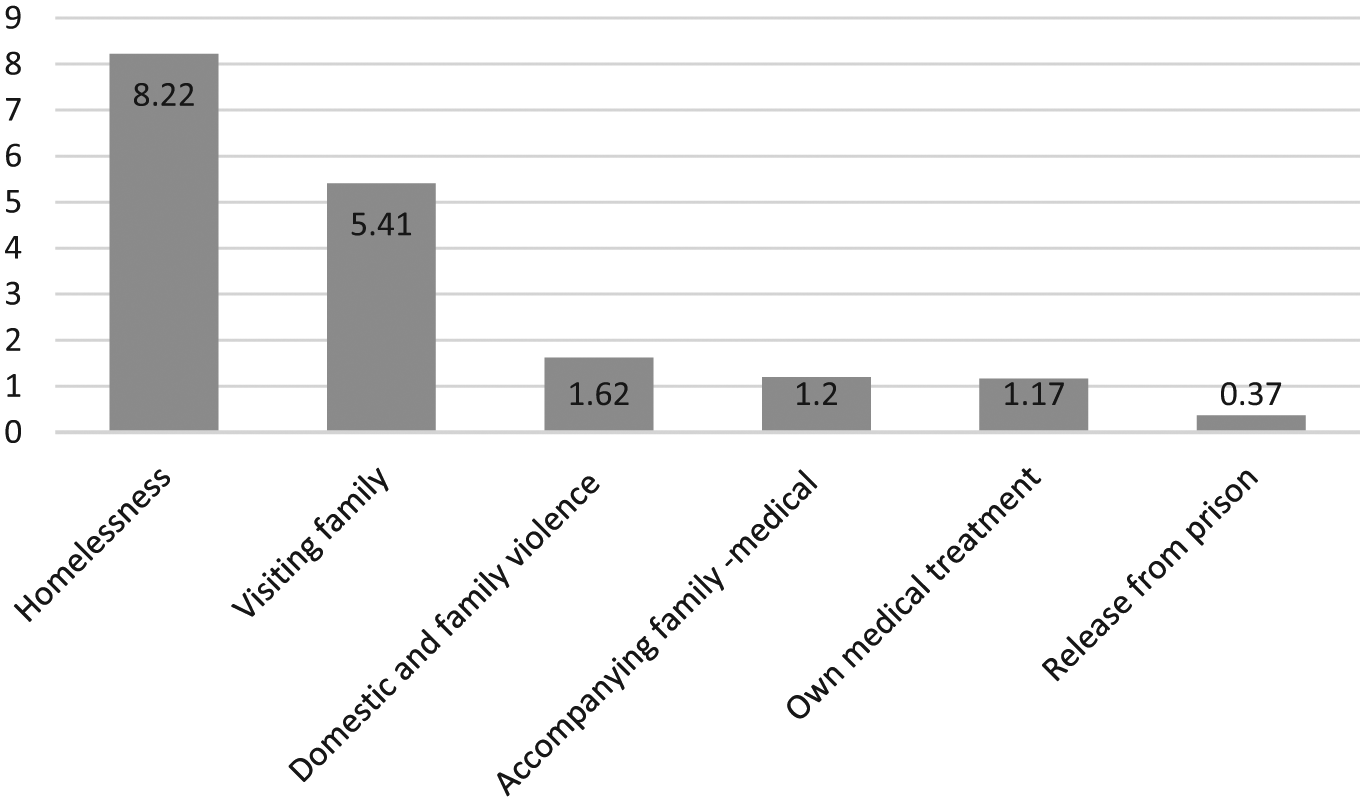
Estimated average time spent in the parks, according to reason.
Regardless of the reasons for coming to the parks, many reported that it intersected with other factors and morphed into something else, creating layered and complex experiences: I’m a sick person . . . I’ve been in and out of hospital and I’ve been sleeping in the park here . . . more than ten years.
Homelessness and Housing
I sleep in one blanket on the cement.
Unsurprisingly, housing and homelessness were major issues for participants and the vast majority (92%) experienced homelessness. Fremantle participants experienced longer periods of homelessness (8.85 years) compared with those in Perth (6.84 years). Two thirds of the participants were sleeping rough in parks and other public places at the time of the interview. A further 23% were temporarily staying with family (usually sleeping on the floor), and a small number of people (5%) were living in homeless crisis accommodation. Commonly, people moved between rough sleeping and sleeping on floors or couches with family. People did not wish to move frequently, rather they tried to minimize complaints of “overcrowding” and potential eviction for their family who held the tenancy. This strategy was adopted by one participant who had a house yet spent most days in the parks and public places with her family having a “good yarn” to discourage them from visiting her and thereby reducing the risk of being evicted from her social housing tenancy. She remarked that spending time in the parks kept her “out of trouble and from getting evicted.”
Given the high rates of homelessness, it was unsurprising that participants discussed the urgent need for suitable and secure housing. Participants did not want to continue to spend time in the parks and were frustrated that service providers and the broader community constructed them as the problem and attributed choice about being in the parks and homeless: People think we choose to live like this; we don’t always.
This quote also suggests that the social construction of people in the parks pays little attention to their lived experiences.
Many people recounted long-standing and continuous attempts to secure housing, yet were becoming resigned to the experience of homelessness or precarious, short-term housing: I’ve been waiting for years, darling . . . don’t ask. Over 25 years I’ve been trying to get a home, and I’m still on the street.
Waiting times, problems with previous tenancies, and serious physical health issues intersected to leave little hope of housing: It takes four or five years . . . and look, some people won’t last that long.
Others spoke about continuing to apply for private rental tenancies, despite not being successful: We went for a house inspection and . . . (someone else) turned around and offered the landlord a bit of extra money. And that’s after . . . (I) said I could have my pension deducted straight into their account and everything like that. It would have been ideal, nice and close the medical centre.
The cost of crisis accommodation was considered prohibitive and it was reported that there were few options for single women, couples, and families. The guidelines or “rules” of these agencies were considered restrictive, particularly in relation to the expectation that people must be alcohol free. Many participants reported that their eviction from crisis accommodation led to rough sleeping and homelessness. For some, this created further complications, such as missing essential medical appointments like renal dialysis, becoming seriously unwell, and in some cases anecdotally reported, death.
Spending Time in the Parks
The majority of participants described spending time in the parks “yarning,” connecting, and catching up on information with family. We have described “yarning” as a method utilized in the interviews with people in the parks, yet in this context yarning refers to connecting, conversing, sharing information, and being in company with other Aboriginal people. Half the participants said they spent “a little” or “some” time drinking alcohol and for many there was a functionality underpinning their drinking: When I’m sober, I can’t sleep at all. It’s insomnia . . . whatever they call it. I’ve got to get drunk to have a sleep.
Being at risk, assaulted and threatened, was mentioned by almost all participants. People were at risk from others in the park and those who did not spend time in the parks. In terms of intimidation, one person said, Sometimes people stand over you and you don’t feel safe.
The majority of participants spoke about the significantly higher risks for women in relation to sexual violence, physical assault, and exploitation: It’s not safe at night—there was a lady raped, and you can get mugged.
Participants reported that they managed these risks by keeping physically close to others: I feel safe with a group of my family; not on my own.
Daylight was seen to afford more safety. People shared stories of violence and threat while sick, suggestive of a high level of vulnerability and further compounding of intersecting factors. Similarly, having one’s belongings stolen (including essential medication) was common: People be coming, stealing our blankets off us.
A common strategy adopted by participants was to “sleep with one eye open” and maximize one’s safety: It is a bit of a worry, you’ve just got to be vigilant of where you are, try and sleep under lights so you know where you are. Sleep where places are light, that way you’ll know whose coming and the police will see you.
Many participants had experiences of no, or disinterested responses from police and other services after being sexually violated, physically assaulted, or having their belongings stolen. Consequently, participants felt they had to manage the risks on their own, without assistance.
Health and Well-being
I was run over by two cars two years ago.
Along with the risk to personal safety, the majority of participants reported health and well-being problems which intersected with racism, poverty, homelessness, and other forms of disadvantage. This included exposure to the weather resulting in colds and influenza, dehydration, and heatstroke. Injuries from assaults such as broken ribs and infections from wounds were also reported, with one person reporting they had been Hospitalized many times. For example, I was assaulted, had infections.
Complications from long-standing health conditions were identified by a number of people and the following quote from a man with serious long-term cardiovascular disease reflects the experience of a number of people who were discharged from hospital to homelessness: I’ve been sleeping rough since the day I got out of hospital.
Consequently, spending extended periods of time in the parks and living homeless mediated treatment and regular medication regimes: I’m on a lot of tablets and I don’t know which tablet I’ve gotta take—I’m getting blind and I can’t see. When I was crossing the road I nearly got run over.
In relation to emotional well-being, people spoke about the impact of not being able to store or keep their belongings, losing identity documents, and the impact on well-being of being moved on by the police which is discussed further in the next section: Nowhere to leave bags, so they get stolen and lose ID . . . and move on notices when it’s raining or when you’re not doing anything wrong. Makes life harder.
Service Delivery and Community Responses
A wide range of services were accessed by participants, including health clinics, hospitals, Aboriginal-specific services, homelessness agencies, food programs, and day centers. The length of time spent in the parks was tabulated with the number of services listed by participants, and no correlation was found between the length of time in the parks and the number of services engaged. It is possible that people who were new to the parks may have limited knowledge of services. However, those with lengthy experience in the parks spoke of sharing their knowledge: I’ll take them to the services where they want to go and get a food voucher or whatever, but once I get the food voucher I’ll say “Are you right now?” and they say “Yeah, we’re right. Righto. Thank you very much” and I’d go my own way. So they know where to go for next time.
Participants were also asked to share their perceptions and experiences of services and most said their involvement was “okay” or “good” (notwithstanding the concerns raised previously about crisis or short-term accommodation programs). Two main areas of concern were raised by participants with the first relating to free food services: It’s . . . soup every night and a person can only tolerate so much soup, and if you’re on the streets for years and years, soup becomes sort of a little off-putting. It doesn’t matter how good it is—it’s just soup all the time.
The second area of concern related to police responses. Participant comments indicate that the police response in Fremantle was characterized by moving people on. In contrast, the policy response in Perth was described as tolerant, although at times, intrusive. The following quote from a Fremantle participant highlights the experience: They . . . make it their point to come and look for us and we tell them, “There’s more criminals, worse criminals out there than us alcoholics.” They give us a move on notice . . . we’re on the streets here, where are we going to go?
While police action often left participants feeling unwelcome, some retailers and members of the public were responsive and kind: Most of the shop owners, they know us, and . . . they’ll give us something to eat.
Messages to Others
It’s very hard, living in the park (it) isn’t the right way. Hard to put up with people drinking. Hard to find somewhere to keep your stuff.
To counter the invisibility of people’s lived experience in community, service delivery, and policy discourses, participants were asked what they wanted others to know about their circumstances. There was a strong message to avoid the parks as they were framed as places of risk, vulnerability, and insecurity: It’s dangerous, you have to be on top of your game, looking out all the time—it’s very unsafe.
The specific issues for women were frequently mentioned, with many commenting “there is not enough for women.” It was also reiterated that to be safer, people needed to stick close with their family. Another clear message related to ideas about choice and homelessness: People think we choose to live like this—we don’t always.
Finally, the lasting legacy of dispossession and colonization was highlighted as key messages to others, with the succinct, yet powerful statement to others: This is not right for our people. This is our land.
This statement captures how time spent in the park intersected with culture, alienation, health, well-being, and personal security.
This description of the findings demonstrate that a number of sub-themes can be traced within and across the major themes listed above. Issues such as the experience of spending time in the parks exacerbated problematic health and well-being while also creating new problems and concerns. Overwhelmingly, the findings highlight that spending time in the parks was unsafe and created experiences of isolation and marginalization. Participants clearly articulated that they did not choose to spend time in the parks and it was dangerous and difficult. The findings reflect the ideas and explanations put forward by the service providers about people being “stuck” in the city and experiencing long-term homelessness. However, the findings go further by providing a space from which the lived experience of the people in the parks can be heard in a nuanced, detailed, and explicit manner. In other words, the detail comes to the fore, and in this, the projects’ aim of epistemic justice for the people in the parks is partially addressed in that participants’ voices are privileged. However, as we discuss in the next section, the ability of this research to make a significant difference to the lives of the people in the parks has been limited.
Discussion
This research sought to provide a vehicle for the lived experiences of people in the parks to be heard, respected, and understood. Concomitantly, the academic researchers aimed to enact decolonizing methodologies by, first, working from a position that privileged Aboriginal ways of being and knowing and, second, participatory and collaborative mechanisms and processes that reflected this positioning. The research project was situated in the context of the ongoing and ever-present impacts of colonization in the everyday and everynight lives of the Aboriginal co-researchers and the participants who spent time in the parks. The negative attention directed at people in the parks from the media, politicians, and community members peaked and ebbed; however, it was a constant presence.
The findings show that the lived experiences of the people in the parks intersected with a range of factors, often compounding and exacerbating health and well-being. Dislocation was widespread and characterized by being long distances from home and country, feeling socially and culturally isolated and for most, experiencing long-term homelessness. Disconnection and dislocation from land, culture, and kin have significant and far-reaching impacts on Aboriginal Australians’ spiritual, emotional, physical and mental health, and well-being (Australian Indigenous HealthInfoNet, 2016; Government of Western Australia Health Department, 2015 ; Memmott et al., 2003). Such experiences are long-standing and widespread, beginning with colonization and continuing in different forms to this day (Government of Western Australia: Drug and Alcohol Office, 2011), and were not a choice for the majority of participants. The fragmented, uncommunicative, and uncoordinated nature of policies and services where one element transports people, another provides health treatments, others provide accommodation and yet more services provide welfare and material support worked against the lived experience of interrelated and intersecting issues, often compounding and expanding vulnerability and risk. Similar findings are reported by Parsell and Phillips (2013), in relation to Indigenous peoples in Darwin who find themselves stuck in the city, far from kin and country.
These experiences sit in the context of long periods of homelessness, with 92% of the sample reporting experiences of homelessness. The importance of secure and stable housing was emphasized and desired, evidenced by participant’s comments on not staying too long with family to avoid jeopardizing tenancies. Such thoughtful and strategic decisions are rarely acknowledged by residents, businesses, or politicians and challenge simplistic “return (home) or relocate” solutions. Despite identifying the importance of secure housing, many people had lost hope of permanent housing (also found by Parsell & Phillips, 2013). Many people were evicted from crisis accommodation into homelessness, further compounding vulnerability, problematic health, and compromised well-being.
Participants used their time in the parks to socialize and yarn with family, addressing cultural and familial alienation through connection and information sharing. Drinking alcohol was identified as a functional response to aid sleep, pass the time, and minimize the sense of threat to safety (also noted by Parsell & Phillips, 2013). A range of strategies to maximize safety were identified including constantly being vigilant, staying close to family and sleeping with “one eye open.” The experience of the police being unresponsive and disinterested in the participants’ safety meant that people felt they needed to take control of their safety. Experiences of violence intersected with health and well-being, often further complicating existing medical conditions.
In relation to service delivery experiences, participants reported mostly satisfactory encounters; yet, the police and crisis accommodation services were identified as generally unhelpful. “Move on” policies by police reported in Fremantle are widespread in Australia and based on the presumption that an offense will be committed (Walsh & Taylor, 2007). This raises issues about Aboriginal people’s right to be in public places and the moral and ethical consequences of such policies within the enduring context of colonization. It also highlights that as history shows, Whadjuk Noongar people have occupied this part of Western Australia for at least 45,000 years; yet, they are discursively framed as problematic “anti-social visitors” and aliens on their own country. This sits in contrast to the fact that non-Aboriginal people have colonized these lands and more recently, the parks through processes of gentrification.
People come together in the parks for a range of cultural and practical reasons; however, they were presented by politicians, mass media, and local residents as a “threat to societal values and interests” (Cohen, 1972, p. 9), based on their supposed difference and deviance, all of which represented an apparent threat to social order. Nowhere in these activities were the voices of the people in the park heard; which this research attempted to counter by focussing on lived experience. Consequently, the moral panic has ebbed and flowed, associated with the homogenization of people in the parks as dangerous and threatening. Media representations which construct Indigenous Australians’ poor health and social well-being outcomes as a combined “failure of Government policy and individual responsibility” (McCallum, 2007, p. 13), reinforce moral panic, positioning people as both ‘a risk’ and ‘at risk’ and most definitely the ‘other’ (Bogen & Marlowe, 2017).
The presence of the people in the parks is discursively constructed as a ‘problem’ by colonizing residents and businesses; however, this dislocates the enduring impacts of colonization and reframes the ‘problem’ as the people, their drinking, and ‘anti-social’ behavior. Policy and service delivery responses are constructed and operationalized to ‘manage’ this ‘problem’; however, we see little to no evidence of policy makers demonstrating accountability for the ways in which social policy has created silos that constitute and reinforce other ‘problems’. A key problem is the lack of joined up or integrated policy and service delivery responses to people who experience a wide range of multiple, intersecting and at times, competing needs.
Despite acknowledgment in policy that Aboriginal people’s control over their lives and communities is a key ingredient in positive health outcomes (see, for example, Australian Government, 2017), very little has been done to bring about individual or collective self-determination and a crisis management approach continues. The recovery pathways that involve reconnection, restoration, and community resilience that could address the individual and collective trauma from the history of colonization remain ignored (Milroy, Dudgeon, & Walker, 2014). Despite policy rhetoric about service coordination for Aboriginal Australians in rural areas (see Australian Government, 2017), evidence of planning and coordinating service delivery once people arrived in Perth was not uncovered. Instead, individuals and families were left to fend for themselves. The gaps created by siloed approaches were taken up by a small nongovernment agency program with two frontline staff.
However, despite policy and program descriptions which promised joined up service delivery, the people in the parks were clear that their needs were basic—secure and suitable housing, safety and an expectation that the response from services like the police would meet the minimum community standard. Police procedural responses which move people on do not reflect service integration principles or practices; instead, they symbolize an “out of sight, out of mind” response. Yet, while services operate in isolation, the people in the parks’ voices continue to be inaudible, their lived experience erased from the broader discourse, and they are blamed.
Strengths and Limitations
For a range of reasons such as the nature of the data collection methods, lack of trust in research and researchers and cultural considerations in relation to eliciting thick descriptions, limitations arose in relation to the breadth and depth of information collected. The intention to undertake in-depth interviews did not occur consistently with many participants providing single-word and limited answers to questions. While the outreach workers had co-designed the open-ended interview guide, they reported feeling uncomfortable asking personal questions and probing when they did not have a pre-existing connection with participants. This meant that responses often comprised single-word answers, limiting the information collected.
Feedback from the outreach workers was that while many participants were willing to talk to them, they were often not able, or chose not to, describe their experiences in great detail. Therefore, demographic data on age, gender, income source, relationship status, dependents and where people stored their belongings were not collected. In addition, the interview contexts sometimes proved challenging; for example, as outreach workers were preparing to conduct interviews with 15 people in Fremantle, the prospective participants fled when they noticed that police had arrived. The outreach workers’ explanation was that the people left to avoid a police “move on” infringement, which would have excluded them from the area for at least 24 hours. While the two interview sites were identified by service providers as “hot-spots,” other well-known meeting areas throughout the metropolitan area were not included, indicating that this research provides a contextually specific snapshot of lived experience.
This research was based on thoughtful relationship and collaboration between Aboriginal agencies, managers, outreach workers, and academic researchers. Having an Aboriginal Elder lead, facilitate, and mentor gave the project a meaningful connection to the Aboriginal community. The research represented a genuine desire to build on the questions the Aboriginal and non-Aboriginal service provider community had about the experience of the people in the parks. Furthermore, the research has provided a forum for the voices of people in the parks to surface and importantly, a form of epistemic justice. However, it has had limited impact on community concern for this group of people, or in ensuring adequate, joined up health and human service delivery. This means the voices and lived experience of people in the parks remains subjugated to the constructions and narratives of others such as residents, service providers, politicians, and the mass media. Despite this, we recommend this way of working together—starting with the issues that Aboriginal and non-Aboriginal service providers find themselves querying and using this as the foundation for collaborative and critical research.
Although the research has uncovered many unanswered questions, we are disinclined to suggest future research topics. Our hesitation is based on the limited responsiveness and desire to deeply listen and respectfully respond to the people in the parks. We are, however, clear that any future research should be situated within critical Indigenous methodologies and community-based participatory approaches while centering and privileging the lived experience of people spending time in parks and public places.
Conclusion
Although many Aboriginal and non-Aboriginal services are genuinely concerned about the experience of people spending time in Perth parks, their capacity to address systemic policy siloes is limited. That is not to say their efforts go unrecognized by the people in the parks, nor are they unappreciated. Rather, the experiences of the people in the parks reflect the opposite of service integration; many people fall through service delivery and policy gaps and find themselves stuck in Perth, or homeless for extended periods of time. The safety of people who do not spend their time in parks is privileged and seen as somehow more important than those who choose or are compelled to spend time in the parks. This all sits within the context of a sense of déjà vu or history repeating itself when non-Aboriginal people call for curfews to restrict Aboriginal people’s access to areas of historical and contemporary cultural significance within city boundaries. Homogenizing and demonizing this group of diverse peoples as dangerous and a threat to physical and moral safety renders invisible their lived experiences: these are real people, with unmet basic needs and hopes and dreams for themselves, their families, and their mob.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: As part of the CBPR methodology of the project organizational representatives from the Aboriginal Alcohol and Drug Service, St. Patrick’s Community Support Centre, Nyoongar Outreach Services, and 360 Health and Community contributed to the study design; collection, analysis, and interpretation of data; writing of the report and article in their roles as co-researchers and stakeholders.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Half of this project was funded by St. Patrick’s Community Support Centre.