
Abstract
The importance of family’s involvement in care planning has been stressed to cater individualized, person-centered care in residential aged care. However, in reality, there are numerous structural obstacles and barriers that limit opportunities for their involvement. The aim of this article is to explore what they are. The findings based on the 12 focus groups, six groups of care professionals and six groups of family/relatives, reveal that the narrow pathway of communication between staff and families, which is hierarchically structured, one-directional, and clinically driven, enables the former to maintain and control professional boundaries between formal and informal care-giving. Such communication style delimits an opportunity for families to engage in quality discussion about care planning for their loved ones with care staff. Communication within residential aged care facilities embodies complex dynamics of care expectations and responsibilities held by care staff and families.
Keywords
Introduction
The importance of family involvement in care in residential aged care has been extensively discussed, highlighting the benefits of family’s contribution to care. For example, family members’ biographical expertise is of great importance for individualized, person-centered care that takes into consideration residents’ life history, purposes in life and preferences (Hertzberg & Ekman, 2000; Reid & Chappell, 2015). Family can provide psychosocial support for their loved ones, which is less likely to be delivered by care professionals due to the task-oriented care delivery and a lack of resources (Ryan & Scullion, 2000). Thus, family members have an important role in ensuring quality care. Furthermore, developing a quality staff–family relationship enables both groups to engage in reciprocal information sharing, which in turn develops mutual trust and understanding of care (Bauer, Fetherstonhaugh, Tarzia, & Chenco, 2014). A quality staff–family relationship results in staff spending less time resolving conflict with families, increasing the amount of time that can be spent for caring for residents (Utley-Smith et al., 2009).
Despite the acknowledged advantages of family’s involvement in care, there has been persistent discussion in the literature of perceived ambiguity of the family’s role in residential aged care (Pillemer, Hegeman, Albright, & Henderson, 1998; Ryan & Scullion, 2000; Schwartz & Vogel, 1990). Family members often wish to continue their caregiving role after their loved ones are admitted into residential aged care, however, discrepant expectations and perceptions exist between staff and family regarding informal care roles (Bauer, 2006; Konnert, Speirs, & Mori, 2017; Moore & Dow, 2015; Reid & Chappell, 2015; Ryan & Scullion, 2000). Ryan and Scullion (2000) reported that families overestimate their involvement in care, whereas, staff underestimate family involvement in care. In addition, tensions can arise when families are perceived to have invaded the domain of technical and professional care staff (Pillemer et al., 1998). Bauer (2006) found that care staff actively construct a role for families by assigning them to specific tasks such as activity assistance and emotional care, which keeps them at a distance from their professional care practices. In essence, the relationship between staff and family is hegemonic in that care professionals exert control over what kind of care and to what extent family can and should be engaged (Bauer, 2006; Ryan & Scullion, 2000). There is incompatibility between the ideal of family involvement in the person-centered care approach and care reality in institutionalized care settings.
The aim of this article is to explore levels of family involvement in the care of their loved one residing in an aged care facility. It further asks what hinders families from participating in effective communications with care staff in care planning. This article is part of a larger study evaluating an enhanced model of care in Australian residential aged care settings. The enhanced model aims to facilitate staff–family communication as well as multidisciplinary teamwork and improve person-centered care (Savvas, Gibson, Rizakis, Vaughan, & Scherer, 2017). It is important to identify factors which influence communication and interdisciplinary teamwork as these are fundamental for the provision of quality care. Boundary work as a conceptual framework was used to examine these existing patterns of staff and family communication, as well as to highlight different care expectations and role responsibilities among these two groups. In the following section, we unpack the conceptual framework in relation to institutionalized care in-depth.
Boundary Work in Aged Care
The concept of boundary work refers to the “constitution of an ‘independent and self-contained field of knowledge’ as the basis upon which professions can build their authority and exclusivity” (Fournier, 1999, p. 69). Within residential aged-care settings, care is institutionalized and professionalized, meaning that it is planned and guided with professional knowledge and expertise (Dahl, 2017). Here, “professionalizing” is favoring a certain form of knowledge over experience-based lay knowledge, which is largely undervalued (Dahl, 2017). Boundaries are fostered by professionalization where knowledge and expertise within a professional domain are fiercely defended (Fournier, 1999). These professional boundaries can be seen within the context of residential aged care wherein doctors, nurses, allied health professionals, and personal care assistants (PCAs) have rigid and distinct responsibilities of care as determined by their profession (Powell & Davies, 2012).
Within this context of aged care, boundaries exist not only within multidisciplinary care teams but between formal and informal caregivers as well. Within the care teams, there is a clear division of tasks in accordance with profession, for example, nurses do not provide physiotherapy and PCAs do not attend to medication-related tasks. As noted earlier, care staff consciously construct boundaries around the family’s role in caring for their loved ones by assigning them to nonclinical tasks (Bauer, 2006). Creation and maintenance of clear professional boundaries is necessary to protect care professionals and their practices within institutions (Sanders, Bullock, & Broussard, 2012). Furthermore, these boundaries between professional and unprofessional care assist staff to maintain a relationship with care recipients and their families at a professional level, which is seen as particularly important for end-of-life care (Sanders et al., 2012).
Although professional boundaries are seemingly fixed in health care settings, scholars argue that they should be malleable to enhance quality of care (Fournier, 1999; Martin, Currie, & Finn, 2009; Nancarrow & Borthwick, 2005). Powell and Davies (2012) suggest that professional boundaries make inter-professional communication, collaboration, and teamwork challenging thus impacting provision of care. Furthermore, neoliberalism has empowered care recipients as consumers to situate themselves at the center of decision making about their care (Dahl, 2017). They can be considered as a potential partner in health care decision (Ruben, 2015), thus changing the dynamics of relationships with care professionals “whose knowledge and autonomy is assigned lower priority compared to the power of the consumer” (Dahl, 2017, p. 49). With the current societal trend that promotes person-centered, consumer-directed care, which necessitates experience-based lay knowledge input into care planning (Hertzberg & Ekman, 2000; Reid & Chappell, 2015), professional boundaries may need to be re-thought.
One way of enhancing collaboration among multidisciplinary care teams in a context where professional boundaries are rather fixed is carrying out effective communication (Colon-Emeric et al., 2006; Ruben, 2015). Ong, de Haes, Hoos, and Lammes (1995) note, “Communication can be seen as the main ingredient in medical care” (p. 903). That said, communication issues exist in clinical settings due to hierarchical relationships and established role-specific communication styles among care teams (Poole & Real, 2011; Ruben, 2015). For example, doctors play an authoritative role where health information is provided to patients in a unidirectional, mechanistic, and rational manner (Colon-Emeric et al., 2006; Ong et al., 1995; Ruben, 2015). Rigid professional boundaries further limit effective communication with clinical staff unlikely to take the advice and opinion of carers into their practices, where often their contributions are neither acknowledged nor valued (Allen, 2000; Walker & Jane, 2001).
In this article, we are particularly interested with the impact and maintenance of professional boundaries on family involvement in decision making with regard to care. In its exploration, we examine the ways in which communication plays a role to protect or even promote professional boundaries between formal and informal caregivers.
Research Design
Qualitative research methods, utilizing a critical interpretive approach, were adopted to gain in-depth understandings of how care professionals and families engage in communication. The critical interpretive approach helped us view the aged care facilities as providing a unique organizational culture, which leads to a particular form of action. As mentioned previously, this article presents a small part of a larger study that looks into holistic, person-centered approaches to residential aged care. The larger study involved the development of a communication tool for residential aged care, called Transition Maps (TMs). Briefly, TMs are an information-rich yet simple tool to track and coordinate the resident’s health/care journey over time and overall goals of care. The idea underpinning this is that residents and families are often ill-prepared when a resident declines in health and function and transitions to a substantially different level of care. TMs endeavors to assist care staff to navigate families through a residents’ care journey, which, in turn, will improve quality of communication between the two parties. It also encourages multidisciplinary care staff to achieve cohesive collaboration (Savvas et al., 2017).
The project obtained ethics clearance from Melbourne Health (Reference no. HREC/17/MH/296). Signed consent was obtained from all participants prior to commencing focus groups. Twelve focus groups were conducted by the research team to explore existing communication patterns between staff and families, moreover, examine the understandability, practicality and applicability of TMs within real settings through the viewpoints of care professionals and families. Participants were recruited from seven aged-care facilities run by one large not-for-profit organization in Victoria, Australia. The size of each facility varied ranging from 50 beds to 150+ beds. Two facilities were located in regional areas and five were in the urban settings. Although one facility was newly established, the rest of the facilities have been operating for a number of years.
The focus groups consisted of six groups of care professionals and six groups of family/relatives of residents living in aged care facilities. The former included two groups of registered nurses (RNs; n = 13), two groups of PCAs (n = 13), one group each of lifestyle staff (n = 4) and allied health staff (n = 8). These occupations represent clinical staff in the facilities. Despite our endeavor to maximize diversity in participants, it was difficult to recruit staff targeting all facilities due to their work schedule and time constraint. With assistance of the facility managers a focus group for RNs and PCAs was carried out at the two facilities (Facility E and O). Lifestyle staff participated from four facilities (Facility L, Y, E and N). All allied health professionals but one were from the largest facility (Facility N) and the group consisted of five physiotherapists, two physio-assistants, and one occupational therapist. The family focus groups included 37 participants, consisting of residents’ parents (n = 2), spouses (n = 8), sibling (n = 1), children (n = 24), grandchildren (n = 1), and other relative (n = 1), and were recruited from six facilities. The focus group discussions lasted for approximately 60 minutes on average.
Focus group discussions were based on open-ended, semi-structured questions that explored (a) what form of communication was integrated into care professionals’ practices and (b) how family felt and experienced existing communication with care staff, including levels of commitment and satisfaction. All focus group discussions were audio-recorded upon participants’ consent and transcribed verbatim. Any information that could identify participants were changed or removed. The transcripts were analyzed systematically and thematically involving three steps of analysis. In the first phase, the research members familiarized themselves with the transcripts by reading them repeatedly. In the second phase, group-by-group open-coding and axial coding were conducted. Open coding was used first to identify comments which represented concepts and themes within the data (Neuman, 2006). The highlighted comments were then set out in a table based on the shared meanings that formed coding schemes. Next, axial coding was carried out for further elaboration of the analyses. By using axial coding, we were able to identify connections with codes, investigating causes, consequences, interactions, and relationships, which enabled us to cluster categories together. (Neuman, 2006). Concurrently with coding, the authors engaged in analytic memo writing to understand patterns, highlight potential themes and elaborate on thoughts. The research team met regularly to discuss the coding documents and any coding related issues were solved to enhance intercoder agreement.
The third phase involved cross-group comparisons in communication patterns through a combination of variable-oriented and case-oriented strategies. Miles and Huberman (1994) argue that using these combined strategies enables preservation of the complexity of contexts and narrative sequence. The variable-oriented strategies involve looking for themes that run across cases. In this process, prominent commonalities and differences were sought across different groups. When searching for different features across the data, attention was paid to locating “cases that are similar in many respects but differ in a few crucial ways” (Neuman, 2006, p. 473). The approach of seeking differences was particularly useful in identifying communication styles each group of care professionals engaged in and seeking rationale underlying the actions, which led us to identify the themes of hierarchical communication structure and boundary work. With case-oriented strategies, a theoretical (or conceptual) framework is used for an in-depth investigation on one case and applicability of the framework is examined in the other case (Miles & Huberman, 1994). This method was useful in elucidating a striking difference in communication experiences between care professionals and families. It also navigated us to explore further how such structured communication influenced levels of families’ involvement in care discussion.
Findings and Discussion
Both staff and families emphasized the importance of communication and their commitment to it. However, there were prominent differences in patterns and purposes of communication between staff and families that were involved. Staff predominantly engaged in “information giving” practices and the families’ role was mainly “information receiving.” Families are contacted by staff when something happens to their loved one living at the facility, for example, a medication change, a sudden decline in health condition or an incident such as a fall. Communication was often “one-way” (from staff to families). Levels of satisfaction in communication experienced by these two groups were also polarized. Often, staff believed they made continuous efforts to communicate with families (mainly via phone), and therefore, were content with their levels of commitment in their communication. Whereas, many families experienced certain levels of frustration in the way staff communicated because they are usually passive information recipients or they do not hear anything from staff if there is nothing to be reported regarding their loved ones’ health. This conflict was derived from the different expectations the two groups held in terms of what they hope to achieve through communication. Staff use communication as a means of incident reporting. In contrast, many families hoped to manage their feeling of uncertainty through communication with staff. For many, their loved ones’ future is uncertain because of their health conditions (dementia or multiple comorbidities in many cases) that require close medical attention and care. Many find it difficult to understand their family member’s diagnosis and health journey without thorough explanation. Many families hoped to discuss with staff what to expect in the near future but our findings revealed that such opportunity is not always available.
The following sections are divided into two. First, we look into organizational barriers for effective communication. We argue that the hierarchical nature of communication policies hinder satisfactory communication flow within the multidisciplinary care teams and enforces rigid division of tasks. This, then, affects the quality of communication between staff and families. Next, we examine different patterns of communication that staff and families engage in and discuss what they entail.
Hierarchical Communication Structure as a Barrier for Harmonious Communication
Families rely on communication with staff to assuage the uncertainty and anxiety they experience around their loved one’s health and care. Families frequently raised concerns regarding difficulties in finding appropriate staff to ask care-related questions. This is illustrated in G’s (Daughter, Facility O) comment, . . . because there’s one RN to the whole place and they (other care staff) have to refer everything to the RN. To find the RN in this place takes hours and how many hours can you sit and wait, so you don’t often get an answer.
Similarly, A (Son-in-law, Facility O) stated, “it has driven my family mad. I agree that the staff, it is just so hard to find them, really really hard.” Both G and A’s comments convey the difficulty in finding staff to ask questions and, consequently, are unable to resolve issues in a timely or well-informed manner. Moreover, G’s comment shows that staff engage in role-specific tasks and not all staff can accommodate families’ queries. Based on the focus group findings, a hierarchical communication structure became apparent whereby RNs manage all reporting by other care staff and are in charge of communicating with families (Figure 1). Colon-Emeric et al. (2006, p. 173) describe this type of vertical communication as “chain of command’ between care professionals, characterized by thin communication and limited information exchange.” This context provides, “bureaucratic efficiency and indicates an internal, control orientation focused on stability” (Scott-Cawiezell, Jones, Moore, & Vojir, 2005, p. 342) but little opportunity for cooperative operations in care practices (Colon-Emeric et al., 2006). This notion is applicable here in that there was no two-way communication among the multidisciplinary care teams reported by our participants.
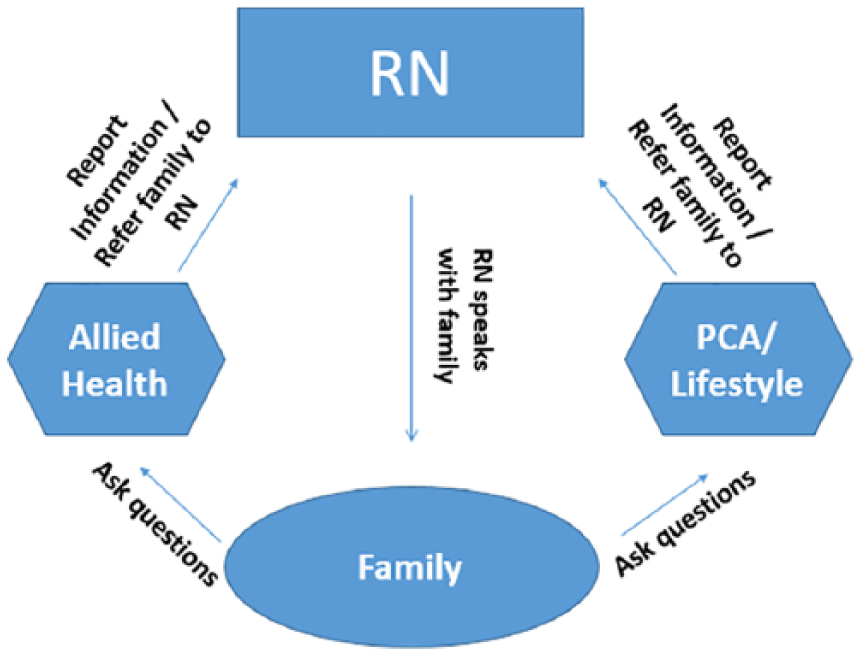
Family communication through hierarchical communication structure within multidisciplinary teams.
Allied health professionals and PCAs work at the frontline of care: interacting with residents directly on a daily basis. Both allied health staff and PCAs discussed the difficulty in sustaining the hierarchical communication style by which they are not encouraged to have care-related conversations directly with families. They considered this to be a significant barrier to achieving effective overall communication with families. Although all staff witness families struggle to understand their loved ones’ health conditions that fluctuate on a day-to-day basis, only RNs (and GPs where necessary) can provide direct assistance due to the hierarchical policy. PCAs at Facility O explain,
. . . a lot of them (families) don’t understand what their loved ones are going through, even down to personal care, what their needs are . . . as a carer we’re not really meant to explain to them as to why . . . It’s the families that really struggle with dealing with “why is mom not looking good today, why is she in a wheelchair today, why is she not walking, what’s wrong with her, why is she in bed?” . . . they don’t understand but that’s the part of the decline or her condition . . . They (families) want the answers from us.
Because we are their carers. They (families) don’t go to nurses. They come to us and want more from us but we can’t give them. That’s hard because they want our opinions.
Don’t you have those conversation [with families] if they want?
We can’t.
That’s what I mean. That’s what makes it hard for us because we can’t say anything to them even though we deal with them day in/day out. We know that has been going downhill because he’s had a cold or whatever . . . We can’t say anything. Then, when you say “you need to speak to a nurse,” they panic. “Why? What’s wrong? What’s happened?” Yes, it’s hard.
Families understand that PCAs tend to have closer relationships with residents than nurses do and so want to hear what is happening to their loved ones from their perspectives. PCAs can converse with families regarding residents’ general wellbeing, however face a dilemma when it comes to health communication as all health or care related queries must be referred to RNs.
These narrow communication boundaries can be understandable as PCA’s professional knowledge and skills are not medically and clinically informed. A PCA at Facility E noted, We don’t really want to step out of our scope of practice. So basically, to communicate with family is like a 3 way conversation really because you’ve got the RN. If we are confronted with relatives and we’re not quite sure in ourselves, you know, out of our scope, we basically kindly speak to them and we notify the DIV I (Division I nurse) and it’s dealt with through that way. (J)
Health/care-related questions can be beyond PCAs’ knowledge and so referring everything to RNs may be an appropriate practice. As seen in G’s comment earlier, families do understand that they have to find the “right staff” to direct questions to although this is often difficult to do.
Allied Health staff were found to have similar experiences to PCAs. Despite their professional knowledge and practice as physiotherapists and occupational therapists, they too were required to adhere to the same chain of command and report everything to RNs. They demonstrated an understanding of the necessity of this communication style to prevent families from obtaining inconsistent information from various care professionals, which can be a source of staff–family conflict (Caron et al., 2005). However, Allied Health professionals felt that their specific care practices are unable to be effectively explained to families through this process of communication.
. . . it is challenging because we obviously have specific things that are directly relevant to what we are dealing with and we are the best person to that contact, which we do anyway even though we’re not supposed to. It’s all supposed to go through the RNs but that’s not practical for them when they are emailing us going “can you please call us about this?” (L [Physio, Facility N])
Although RNs and physios work as a team, the latter is situated below the former in the hierarchical communication structure. This arrangement, according to Allied Health staff, is impractical and frustrating as their communication with family members is restricted and their professionalism is overlooked. More importantly, this structure affects families’ ability to receive a timely and accurate response to their queries as discussed by the family participants.
Our findings revealed that Allied Health professionals and PCAs believe that they are effective mediators for communication between residents, families and care staff. Many PCAs demonstrated their pride by stating that they know residents better than nurses do. However, the organizational structure determined that all professional communication must be passed through RNs, which inconveniences both parties. The hierarchical communication structure is a significant barrier to harmonious communication among care staff and effective staff–family communication. This structure was also found to reinforce communicative boundaries among all groups of care professionals. With this, some staff experienced a dilemma between professional conduct and bureaucratic rules. In the next section, we explore patterns of day-to-day staff–family communication and discuss the issues and obstacles this entails.
Day-to-Day Staff–Family Communication Patterns
Our findings confirmed that the RNs believed that communication with families is an important part of their care practice. When asked if they regularly communicate with families, the common answer was, “yes, all the time” (D, RN, Facility O). RNs’ responses to further questioning were unanimous regarding how and when staff and family communicate: “it’s more of when there’s a change with the residents’ care” (J, RN, Facility O). The other RN followed: After GP reviews [of care] and if there was any medication changes, we actually have to let them (family) know because we had a problem that family wasn’t informed in time and later they came and asked “why is my mom on such and such medication?,” so we do that now. Also if there’s any incident family needs to be notified or any alternation in the condition of their loved ones we let the family know. (E [RN, Facility O])
The communication style staff engaged in, as described above, comprised incident briefing and informing of amendments to care after they had occurred. Based on E’s comment, briefing phone calls are necessary and strategic actions that help prevent family conflict with staff as family members are always informed of any issues or changes. As family’s experiences of receiving these briefing calls were consistent across all focus groups and sites, this suggests that this practice is formally structured within the organization.
It was clear from family feedback that the frequency of these phone calls varied considerably depending on residents’ health conditions and vulnerability to incidents or other health issues. Thus, some families receive frequent phone calls, where others are rarely contacted:
They do give us phone calls pretty regularly because mom has a lot of falls. So we’ve had a lot of communication about falls.
If there’s an issue they do call you.
Yeah absolutely, even if there’s a slight scrape or something, they’re straight on to you but also just conversation too when you’ve had someone in here a fair while you get to know the most of the staff. They are very open that way.
Here, appreciation of staff commitment to their communication with family, even for minor ailments, is expressed. Most families considered briefing calls important to keep up to date and informed of their loved one’s experience and condition. The call also give families opportunity to see whether or not, staff took appropriate actions in accordance with the types of incidents.
In contrast, some families were critical of this type of communication and did not find it valuable:
I would say there’s probably a regulation that if they (residents) have a fall, the next-of-kin must be notified. That sounds like that’s part of the procedure of the institution . . . I got a call at quarter past 12 one night saying that my husband had been taken to hospital because he’d had a fall and my reaction was, “What do you want me to do?” sort of thing and I’m not going into the hospital at 1 o’clock in the morning and try to find a car park in the dark alone as an elderly woman . . . But part of the procedure at the organization is the incident reporting and they have to do it.
The incident reporting style utilizes one-way communication with family members taking on the receiver role. Some relatives were critical of the automatic way staff report to families in the event of an incident, particularly when no action is required.
I had one (a call) for my daughter where they said, “she fell out of the bed but she’s laughing and she’s all right.” And I said “Well, what can I do if she’s fine?” So, that was a stupid call. She’s up and she’s fine. Why ring me?
So do you want them to ring you when . . .
Not when it’s silly, no. Urgency, yeah, “you’re fine,” something like that. I just thought it was a bit silly.
It was clear that the “incident report” style of communication was adhered to by care staff at all facilities; however, this framework treats families as passive information recipients only and does not allow for their involvement or input. Furthermore, some families experienced less frequent staff-initiated communication because their loved ones’ conditions are relatively stable compared with other residents within a residential aged care facility.
Families Hope to be Involved in Decision-Making Discussions Around Care
When families were asked how frequently they have an opportunity to discuss care planning or decision making for their loved one in conjunction with staff, they commonly answered that this was a rare occurrence. According to feedback from our participants, there seemed no institutional obligation for staff to involve family in care-related decision making. Therefore, families tend to be informed of changes in care by staff after they are implemented, as seen in the “incident reporting” style of communication discussed earlier. At facilities, where families noted higher levels of satisfaction in communicating with staff information sharing tended to be more informal and frequent with families able to have honest dialogue with staff regarding their loved one’s health and care journey. Some families experience supportive emotional relationships with care staff which assists in facilitating bi-directional open communication; however, these positive experiences were not the norm for most families.
There was a discrepancy in perceptions between what staff believe they provide to families and what families expect to receive. As discussed earlier, RNs’ regular style of communication with families was reactive in that contact was often initiated in response to an incident and the sole purpose was to inform. However, families generally expressed wishes to be active participants in care-related discussions rather than being a passive information recipient. Many families in our focus groups mentioned that RNs are too busy to spare sufficient time for a one-on-one discussion with them; heavy workloads imposed on staff were regularly described in the discussions: “The workload is really difficult. To look after over 70 residents and manage everything is quite difficult” (S, RN, Facility E). Understandably, this affects staff-family interactions, particularly when RNs are the designated information providers. J, a husband of the resident at Facility L whose wife is diagnosed with Parkinson’s disease said the following:
Although I come in virtually every day, none of the staff have come to me and said “now this is what’s the next stage is.” I’m not at loss but I certainly don’t know, well, I know she’s going to get worse, never going to get better, but I don’t know what the next stage is.
Do staff tell you day to day information about care?
Well not really. The staff, when I come they all seem to be rushing around the place, very busy and you know, no one have said, you know, take me to one side and said “this, that and other things.”
There’s nothing to stop you from asking.
Yes I know, now I realized that, but I suppose, you know, because they’re rushing around and I don’t want to disturb them.
J is reluctant to take the initiative to seek information because staff appeared busy. Clearly the culture of “if you don’t ask, you receive no information” was established at some facilities. A daughter of the resident at Facility E spoke of her experience: “We get no information at all. We only get what we ask for, probably about a twentieth of that as a response.” There was a general consensus among family members at these facilities that “communication to us here only happens when we initiate it” (D, Son-in law, Facility O). In such circumstances, families feel the need to actively insert themselves in care-related activities to know what is happening, which is well illustrated by S’s (Wife, Facility L) experience:
I suppose because I’m in here so often and also I take my husband to all his appointments, really active in knowing exactly what’s going on, I’m sort of telling staff what’s going to happen really.
S collects information from external sources by accompanying her husband to appointments. She actively involves herself in care which, she believes, is the way that she can know “what’s going on” without relying solely on unpredictable staff communication. Some families revealed that they have frequent and thorough communication and updates from external specialists involved in their loved one’s care; thus, they reject the role of passive information recipient assigned to them by the hierarchical communication style and their reliance on care staff to provide information is lessened.
Without active involvement in information seeking, families tend to express uncertainty about what the future entails for their loved one. This is evident through comments like, “I’d like to know a bit more of what’s going to happen in the future” (L, Husband, Facility H). Brashers (2001) notes that “uncertainty exists when details of situations are ambiguous, complex unpredictable, or probabilistic; when information is unavailable or inconsistent; and when people feel insecure in their own state of knowledge” (p. 478). This statement nicely summarizes the experience of families with regard to the care of their loved one. According to the majority of our participants, adequate explanation of their loved one’s health journey has not been provided to them by staff. Hence, there is significant uncertainty for families around the overall care plan and the anticipated changes to care as the resident’s disease or illness progresses. This situation often drives family members, particularly younger ones (including adult children and a grandchild), to engage in self-directed research using various sources to inform themselves of the condition their relative has and what that means for the future of their care. Family members seeking information from external sources reduce their experience of uncertainty and it allows them to become a more active participant in determining outcomes of care. Although beneficial for families, these behaviors were perceived as causing difficulties for the staff participants in our study.
J, a RN at Facility O, mentioned challenges when dealing with families, “The majority of dealings with family is conflict resolution.” Here, the RNs at Facility O discussed their experience of being confronted by families about the care changes for their loved one.
Some family try to control everything that goes on with their parents and they don’t like it when doctors make changes without talking to them about it and quite often we have to bear the brunt of that in trying to explain why medications have changed or why care directives have changed and a lot of the families get very annoyed about it.
. . . a lot of them use Dr Google. That’s one of our biggest problems.
You’ll get a resident who has had their medications changed so the family will go home and Google and then you’ll get “oh but doesn’t that interact with this and won’t this make mom or dad this?” and you have to explain to them why the doctors has suggested the changes to these medications and hope they understand what you are trying to say.
The RNs viewed family self-directed research as trespassing on their clinical domain and professional boundaries. Family members’ challenge to the professional knowledge was perceived unfavorably. As described in the introduction of this article, clinical staff are protective of their professional boundaries and our findings supported this in that the RNs largely viewed equal family input as an interference to care and moreover, violation to their professional boundaries. Within aged care settings, this can be a source of staff–family conflict (Nelson & Cox, 2003). The findings coincide with existing research that Internet-informed lay individuals are often viewed as a challenge to medical authority, and medical professionals engage in boundary work to reinforce the conventional doctor–patient relationship (Broom, 2005).
Families in all focus groups stated that they wish to be involved in care and they feel responsible for the care of their loved ones, to varying degrees. Often, their information seeking behavior was driven by a desire to act as an advocate for their loved ones who have little capacity to speak up for the care they receive, which supports previous findings (Bauer et al., 2014; Cohen et al., 2014; Konnert et al., 2017).
It’s our job to take the responsibility for Mom. A staff member- some are great and some are not so great, and I don’t want to leave those sorts of decision up to other people and particularly sometimes because I know that they don’t make the type of decision that I would make.
. . . we know what they want, what they need and I spend the most amount of time with him (my husband) . . . I still know my husband better than anybody else here including the doctors and I want the opportunity to say yes or no to be involved.
S and A are among those who believe they know their loved ones better than care staff and thus they hope to participate in care-related decision making. Families expressed desires to be regarded as valued members of the care team, however, care staff were not seen to acknowledge or recognize family members as co-carers but rather as mere visitors of the resident (Konnert et al., 2017; Petriwskyj et al., 2014). Significant changes in perceptions of roles appears necessary for staff to recognize the importance of family involvement in decision making regarding care. For such a shift to occur, more frequent two-way communication between the parties and a greater understanding of different perspectives of care is required (Bauer et al., 2014; Pillemer et al., 1998).
In summary, our findings revealed how communication patterns within these residential aged care facilities were structured in such a way that promotes and maintains hierarchical systems and professional boundaries. Families were prescribed the role of passive information recipients rather than active participants in care discussions. Incompatibility between the care-roles staff and family want to fulfill, led to frustration and conflict: Families aspired to have greater input into their relative’s care and staff wished to maintain control over their professional domain.
Critical Reflections
We took a critical interpretive approach and viewed the facilities as providing a unique organizational culture, which leads to a particular form of action (Deetz, 1982). Nolan (2013) argues that the organizational culture has a significant impact on shaping the experiences of staff, residents, and families at aged care settings. Presumably, care professionals as organizational members and families as non-members may have different understandings and expectations regarding communication and care. Effective communication has been explored as a way that different professions can build harmonious, collaborative team environments where quality care is provided (Colon-Emeric et al., 2006; Ong et al., 1995; Poole & Real, 2011). Our findings suggest communication can also foster professionalization of care. In other words, through communication, care professionals can draw and maintain the boundaries between professional and nonprofessional care providers. This creates barriers to informal caregivers’ (i.e., family) involvement or collaboration in the care of the resident. The rigid communication style operating within these facilities preserves the professional hierarchy where all communication must be directed to the RNs and distribution of information to families is solely at their discretion. This narrow pathway of communication is generic and one-directional to maintain and control professional care boundaries, however was found to be a major cause of frustration and discord among some groups of staff (such as PCAs) and the majority of family participants. There were no relational practices in place to assist staff and families to develop meaningful interpersonal relationships based on shared values and goals to facilitate care cooperation (Nolan, 2013). Overwhelmingly, conflicting care expectations and incompatibility of responsibilities between the two parties seemed to underscore the staff–family dynamic and the power struggle around communication.
The predominant style of communication engaged in by care staff is the incident report where families are contacted by the RN in relation to an event or change in care concerning their loved one. There are two problematic features of this style. First, frequency of contact for families varies depends on how stable their loved one’s condition is. Second, families are not expected to take further action based on the information they receive—the phone call is for the sole purpose of reporting. Staff utilize this type of communication for strategic conflict avoidance; families are less likely to be confrontational or disruptive if they feel that they are informed of any changes or incidents. This practice appears to be prevalent across all facilities in this study and may serve to protect staff from accusations made by uninformed families thus avoiding stressful and anxiety provoking conflicts with family (Walker & Jane, 2001).
The communication practice of incident reporting does not value the family as an important contributor to care practices or decision making. This is problematic as families expressed their wishes to be involved in meaningful communication as joint caregivers for the resident rather than relegated as a passive recipient of information who takes a backseat to professional clinical staff once their loved one is admitted to care. Many families face uncertainty about their loved ones’ future because they have not been provided with enough opportunity to discuss concerns and care plans with staff. Families wanted communication with staff to consist of discussions around the resident’s health journey, what to expect in the future and what their care involves. Families are thus unsatisfied with the current style of staff communication and so often choose to engage in uncertainty management by actively seeking health information from external sources including specialists (with whom the residents have regular consultation) and the Internet (Brashers, 2001). The improvised lay knowledge, particularly through the Internet, has become a source of conflict between staff and families as the former feel that their professional knowledge and boundaries are being challenged and overstepped (Broom, 2005). Frequent bidirectional staff–family communication may help to alleviate family uncertainty and anxiety and thus prevent these tensions from arising.
The afore-mentioned hierarchical communication process in effect within the facilities hinders the existence of a harmonious, collaborative team environment for all involved in care (Colon-Emeric et al., 2006). This policy, as explored above, effectively informs families of any issues relating to their relative from a single source, ensuring that information is streamlined and filtered. This one-way reporting system is also in place for all care staff within a facility but might not be the best for multidisciplinary care team communication. Some PCA and Allied Health participants expressed their frustration with this system as all information must be directed through the RN. RNs are therefore burdened to manage all family inquiries that may be beyond their clinical knowledge such as information related to physiotherapy or the day-to-day care of a resident. This communication method limits opportunities for the multidisciplinary teams to discuss care plans with families based on their professional input on a regular basis. Doing so under this hierarchical framework might negatively affect collegiality within the teams (Anderson, Corazzini, & McDaniel, 2004). To maximize benefits derived from multidisciplinary care teams, extensive revision of this communication form may be necessary to optimize function of the multidisciplinary care team (Fleischmann et al., 2016).
There was a lack of recognition among care staff that families are valued members of their care team, providing important care-related information. This supports previous findings (Reid & Chappell, 2015). Perceptual change is necessitated to create a care environment where both formal and informal caregivers can be involved in care planning. The findings suggest that malleable boundaries allow more room for negotiating roles, ultimately providing a strategy for more effective communication. This may be of particular relevance to the current trend within care services where the traditional bio-medical care-model is shifting to a person-centered or consumer-directed framework. It is now recognized in aged care that the involvement of families is one of the best guarantees of a resident’s wellbeing. This welcomed shift toward a holistic person-centered model of care will require quality staff–family communications as these relationships are integral to quality of care provided (Bauer et al., 2014). Policy changes may be required to provide workers with time and flexibility in their schedule to build cooperative relationships with residents and families as the issue of short-staff impacts how communication is carried out and, moreover, care is planned and delivered (Bowers, Lauring, & Jacobson, 2001). It is important to note here that families’ dissatisfaction with the levels of communication with staff did not indicate that they were also dissatisfied with the quality of care their loved ones were receiving.
Limitations and Future Directions
The limitations of the present study should be noted. All family participants showed high levels of dedication and commitment to the care for their loved ones, therefore, our findings that families desire to be involved in communication and decision making at a greater level than they currently are may not be generalizable. Our study was conducted within one Australian service provider, and therefore, the families’ experiences might be organization-specific. Further study would be required to determine whether these findings are applicable outside an Australian residential aged care context. As noted in the research design section that this study was a small part of a larger study that involved the development of TMs, which was created aiming to improve quality of communication between staff and families/relatives. A future study may explore how TMs could address the communication issues alleviating tensions between the two groups derived from the structured communication styles.
Conclusion
The aim of this study was to explore levels of family involvement in the care of their loved one residing in an aged care facility. In particular, we focused on patterns of communication staff and families engage in and explored communication styles and structures that create barriers hindering family’s active involvement in care. Despite family members’ high aspiration to be an advocate for their loved ones to support their best interest in care planning, in reality, there are numerous structural obstacles and barriers that limit opportunities for their involvement in care decision making. The findings from our focus groups revealed that communication within residential aged care facilities embodies complex dynamics of care expectations and responsibilities held by care staff and families. Protecting professional boundaries may be perceived by care professionals as necessary to maintain the hierarchical clinical structure. Communication was a powerful tool to protect or promote professional boundaries between formal and informal caregivers. However these boundaries may require negotiation to shift to an individualized, person-centered care model from the predominant clinically oriented culture of care. Our findings suggest that institutionalized care may need flexibility and perceptual change that allow care professionals to understand relational care practices.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Dementia and Aged Care Service (DACS) Fund provided by Department of Health, Australian Government.