
Abstract
Patient trust is positively related to health outcomes, but there remain barriers to patient trust in physicians. This narrative study analyzed patient experiences and highlights barriers to patient trust underlying communication with physicians in acute care. Snowball sampling was used. Informants were 12 participants, in poor physical health, upon discharge from a 3-week hospitalization in an acute-care setting at an Israeli public general hospital. Two narrative interviews were conducted with each participant upon and after discharge. Findings suggest presurgery barriers to trust (lack of acknowledgment of patient’s crisis, underrating patient’s autonomy, and use of unique empathy) and postsurgery barriers to trust (lack of attentive listening, lack of medical professionalism, and delegitimization to patients’ self-alienation). Two common narrative identities emerged linking trust with self-worth. To build trust, physicians are called upon to extend their dedication from dedication to improve clinical outcomes to dedication to improve clinical outcomes and preserve patients’ self-worth.
Keywords
Introduction
Patient trust in physicians is central to health promotion (Feo et al., 2016; Kitson & Soerensen, 2017). Trust is positively related to better disease markers, higher adherence and higher utilization of health services, higher well-being and life quality, and better health (Gabay, 2015; Haywood et al., 2014; Wiechula et al., 2016). Trust is the acceptance of a vulnerable situation in which one party believes that “at the moment of truth,” the other party will care for its interests (Rousseau, Sitkin, Burt, & Camerer, 1998). This widely accepted multidisciplinary concept of trust was characterized as only partially mature for application in patient relationships with clinicians (Hupcey, Penrod, Morse, & Mitcham, 2001; Morse, 2000; Morse, Hupcey, Mitcham, & Lenz, 1996). To advance the concept of trust toward maturity, Hupcey et al. (2001) conducted a concept clarification process using the method described by Morse (2000). The clarification process developed a more refined, pragmatic, and higher-order concept of trust that is adequate for relationships in health care (Hupcey, 2002; Hupcey et al., 2001). Finally, based on a grounded theory study with adult patients in acute care, a scaffold of trust was generated (Hupcey, 2002).
The scaffold included a patient’s need that could not be met by self, congruence between expectations and actual behaviors of others, an assessment of risk, and a willingness to depend on someone else (Hupcey, 2002). This conceptualization of Hupcey and Morse (2000) proposes that patients have expectations for care and are willing to place themselves in a relationship that establishes or increases vulnerability with reliance upon the clinician to perform as expected (Goudge & Gilson, 2005; Hupcey et al., 2001). Meeting patient expectations was a theoretical core that linked all categories of trust (Hupcey & Morse, 2000). In critical medical situations, the vulnerability of patients is high, and their need to trust the physician is overwhelming (Hupcey, 2002). If expectations are met or exceeded, trust is formed. If patient experience is short of meeting expectations, distrust results. I adopt the above conceptualization of trust established by Hupcey and Morse (2000) and Hupcey (2000).
Trusting patients expect their physician to perform her or his responsibilities competently and to assume responsibility rather than inappropriately defer it to others (Hupcey, 2001). Patients also expect physicians to make their welfare the highest priority (Goudge & Gilson, 2005). Finally, patients expect physicians to use communication that promotes their health (Gabay, 2015). These expectations relate to outcomes and needs of clinical care. This study explores barriers to patient trust underlying patient expectations regarding physician–patient communication in acute care. This study identifies elements of communication that may be embedded into everyday practice to meet patient expectations and build trust.
Patients enter the hospital with expectations based on their needs of care and on the hospital’s reputation (Hupcey & Morse, 2000). Their assessment of the congruence between their expectations for care and their actual encounters with physicians takes place through repeated interpersonal interactions during the hospitalization process shaping their trust or their distrust in a physician (Hupcey & Morse, 2000). Although trust was originally regarded as a dichotomy, with trust and distrust as separate constructs, some researchers studied the concept of distrust and reversed the score of trust to represent distrust (Fulmer & Gelfand, 2012). With no empirical evidence for separate constructs, I also adopt the continuum theory of trust, with trust and distrust at the ends of the same continuum (Schoorman, Mayer, & Davis, 2007). Next, trust-building communication in critical care is discussed in the following section.
Trust-Building Communication in Critical Medical Situations
Patients who reported that they experienced lack of respect and dignity had low trust in clinicians (Lattimer et al., 2010). In acute-care settings, clicking on a personal level and having a sense of humor promoted patient trust in clinicians (Hupcey & Morse, 2000). Cancer patients who felt validated, worthy, reassured, and comforted had positive psychosocial outcomes (Hack, Degner, & Parker, 2005; Hupcey, Penrod, & Morse, 2000). Several behaviors facilitated patient trust in clinicians: knowing the details regarding the patient’s condition, advocating for the patient, taking action, and being responsible for going the extra mile (Hupcey & Morse, 2000).
Patient-Centered Communication and Patient Trust
The Institute of Medicine determined that patient-centered care is an element of high-quality care related to patient worthiness (Baker, 2001). Patient-centered care is defined as respecting and responding to patients’ wants, needs, and preferences so that they can make choices that best fit their individual circumstances (Baker, 2001). Patient-centered care focuses, among others, on clinicians’ sensitivity to patients’ unique physical, psychosocial, cultural, and emotional needs, which are routinely overlooked (Feo & Kitson, 2016). Patient-centered care positively impacts clinical outcomes (Levinson, Lesser, & Epstein, 2010). Compelling evidence shows that patient-centered communication (PCC), described below, increased trust (Levinson et al., 2010).
PCC is more than simply being courteous and honest with patients; it is, in fact, a sophisticated process. PCC processes seek to build trust through increasing clinicians’ understanding of patients’ individual needs, perspectives, and values; exchanging information; fostering healing relationships; responding to patients’ emotions; providing support; managing uncertainty; making informed choices; and patient enablement (Levinson et al., 2010). Furthermore, communication that enhances the patient’s sense of worth was found to confer meaning, motivation, and energy as an essential psychosocial outcome of health (Feo & Kitson, 2016; Levinson et al., 2010). Success in helping patients to preserve their sense of worth, however, is difficult in the current chaotic work environment of clinicians and may, therefore, fall outside the boundaries of clinician–patient relationships (Street, Makoul, Arora, & Epstein, 2009).
The Current Study
Despite the agreement that trust in physicians is essential to health promotion and is driven by PCC, only a few studies explored trust-building communication in clinicians in acute care. Furthermore, hardly any studies focused on trust-building communication that physicians use in acute care (DeLemos et al., 2010). Previous studies called to extend our understanding of how to improve physician–patient relationships to reduce risky, early self-discharge (Haywood et al., 2010). Furthermore, Street et al. (2009) called to explore communication elements that may shape successful well-being outcomes. This narrative study responds to these calls seeking to fill the gap in the literature and explore specific elements of PCC that are important to patients in acute care and that physicians may embed in their daily work while communicating with patients to preserve their self-worth and avoid distrust.
This study is based on patients’ experiences. Qualitative methods that explored patients’ experiences mostly focused on negative attitudes and distrust of clinicians in patients rather than on distrust of patients in physicians (Haywood et al., 2014). Insights based on patients’ experiences are unavailable from other sources and can be useful for quality improvement because meeting patient expectations is an important component of trust (Hupcey & Morse, 2000; Levinson et al., 2010).
The Theoretical Perspective and Research Questions
The theoretical perspective that I borrowed for this study to explore self-worthiness of patients and barriers to trust in communication of physicians with patients is Emanuel Levinas’s ethical philosophy of the responsibility for another (Levinas, 1981, 1993). Levinas focused on repetitive face-to-face encounters that are applicable to face-to-face encounters between patients and physicians. Levinas viewed face-to-face encounters as an inter-subjective relation of being called by another and responding to that other. Levinas contended that, when one adopts responsibility to another, emotion is expressed in light of the suffering of one human when another human has power that is greater than the other can contain. The responsibility for another person’s self-worth is the essence in asymmetric relationships (Levinas, 1981). Because patients are vulnerable and have much less power than do physicians, it is adequate to characterize this relationship as asymmetric. This study seeks to focus on this asymmetric relationship and identify elements of PCC that physicians may use in their encounters with patients to preserve their self-worth and build trust. Research questions are as follows:
Method
Recruiting Participants
A maximum variation approach was employed to recruit participants, enabling the inclusion of a wide range of perspectives (Lincoln & Guba, 1985). Participants were 12 Jewish secular Israelis (six men and six women), ages 29 to 81, with diversity in participants’ age, gender, geography, illnesses, profession, and work status. Ten were married, 1 single, and 1 divorced. Participants were hospitalized in a large hospital (1,202–3,200 beds) or medium hospital (300–700 beds). Narratives provided adequate information power (Malterud, Siersma, & Guassora, 2016). Table 1 presents demographics and health attributes by group (Morse, 2007). Participants were hospitalized due to cancer, heart disease, neurological disorders, or accidents that put them in mortal danger.
Participants’ Sociodemographic Data by Group, Type of Disease, and Profession.
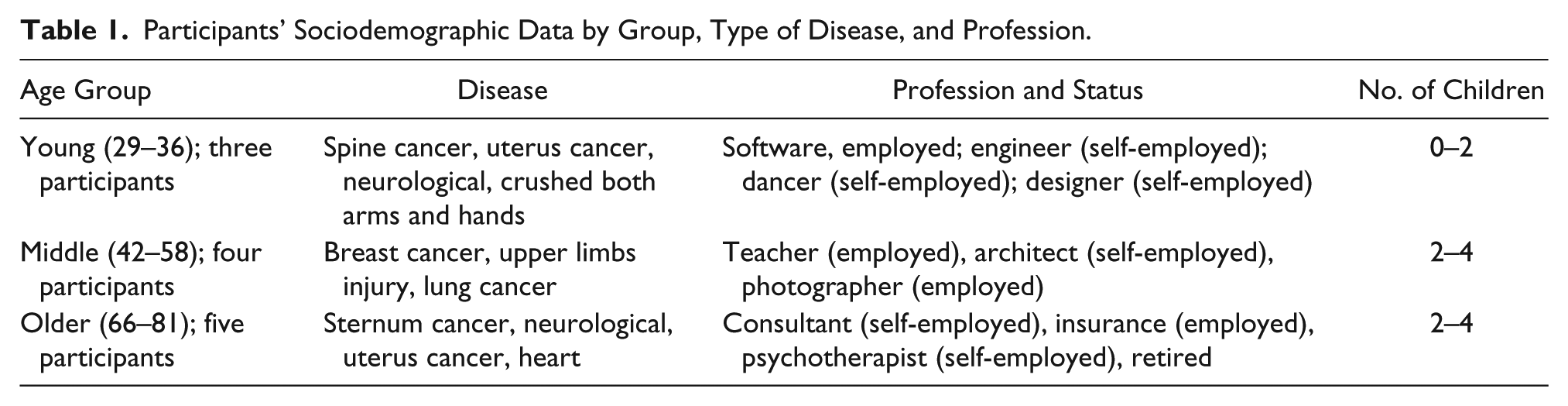
A snowball sampling was used to locate subjects in their initial recovery process upon discharge from acute-care setting in a public general hospital. While the average hospitalization lasts 3 to 4 days, participants were hospitalized for about 3 weeks. Interviews were audio-taped, transcribed verbatim, and translated into English.
Study Procedures
This study was approved by the ethics board at COLLMAN, Israel (IRB #099, September 2017). Following ethics approval, participants were recruited. I assured participants that their participation would have no influence on their future treatments at the hospitals and informed them that they could stop the interview at any point they choose. I asked participants to sign a written statement of informed consent regarding participation in the study and publication. Participants acknowledged their understanding that parts of their narrative will be published (Morse, 2007). All identifying demographics at the individual level were omitted from the findings section to promote anonymity and confidentiality (Morse, 2007). After transcribing the interviews, each participant received a copy of the interviews and approved their content. Two participants asked to omit a paragraph from the interview due to high exposure that made them feel uncomfortable.
A total of 24 interviews were conducted. Two interviews were required for each participant to share the hospitalization experience with me. I conducted interviews at participants’ homes upon discharge at the initial phase of recovery. The first interview was conducted within the first 2 days after discharge, and the second interview was conducted about 3 weeks thereafter. Interviews ranged in length from 90 minutes to 2 hours; two interviews lasted 3 hours and one interview lasted 4, due to considerations of physical discomfort or emotional distress that required breaks. I presented myself as a researcher from academia studying the experience of hospitalization. I presented the goal of the study as education and improvement based on patients’ experiences. I also presented the study methodology. Participants stressed that although it was very challenging for them to meet me in their poor physical state so soon upon discharge, they had a purpose to improve the experiences of others. I thanked them for their willingness to contribute to our understanding.
In the narrative interview, I presented one general open question aiming at generating a deep, unstructured narrative (Josselson, 2013; Josselson & Lieblich, 2003): “Please tell me, how did you arrive at the hospital and what did you experience there?” From then on, participants, who vividly remembered their hospitalization, shared their experience from the first appearance of symptoms until discharge. I actively listened and made no attempt to comment on, ask questions, or judge what participants said. All interviews were emotional. During the interviews, participants had flashbacks, cried, and expressed anger. They said they felt insulted and degraded by what they remembered that had happened in their encounters with physicians. I suggested breaks when I sensed that participants needed them. To allow participants to express themselves freely throughout the emotional interviews, I intended that my body language would send a message of comfort even when it was emotionally difficult to contain the narratives due to both the sensitivity of the issues and personal trauma previously experienced (Dickson-Swift, James, Kippen, & Liamputtong, 2008; Kumar & Cavallaro, 2018).
Research Quality Criteria
I maintained general quality standards of qualitative research (Lincoln & Guba, 1985). I acknowledged my own theoretical positions and values regarding the research issue; I acknowledged my shared experience with the participants requiring examination of my critical reflections (i.e., having undergone a long hospitalization in acute care; Hunt, 2009), and my privileged position as an academic researcher and as a native Hebrew speaker from the same culture. Similar to participants, I enjoy a progressive middle-class standard of living.
To support the transferability of the findings, I described the methodology of the study in detail and provided dense descriptions of participants’ points of view, within their life context. Preliminary results were exposed for a qualitative peer debriefing to seven specialists: three qualitative academic researchers, two physicians, and two hospital directors, asking each one separately for feedback. Based on physicians’ comments, I corrected several medical terms. Narratives were told in the present, at the time of the interview, at the initial phase of healing, at home. Narratives were anchored within three contexts that affected the choice of the narrative by the participant: the broad context, the micro-context, and the immediate context (Spector-Mersel, 2010a).
The broad context of the narratives was the Israeli universal health care system providing all residents broad health services (Segel, 2009). While Israeli hospitals are equipped with modern facilities, high-quality medical technology, and well-trained medical personnel, similar to other health systems in the Organisation for Economic Co-operation and Development (OECD), the Israeli health system exposes its patients and clinicians to difficulties of balancing needs with resources (Israel Guide, 2014). There is a shortage of clinicians and a decreasing rate of beds per population (Crisp & Chen, 2014). Since 2013, Israeli hospitals have been emphasizing patient-centered care as the cornerstone of quality health care.
The micro-context was each participant’s phase of life and career cycle (peak vs. retirement). Finally, the immediate context of the “here and now” may have also affected the narrative: the way I defined the study, my academic identity as an audience for their story, and participants’ wish to participate in the study. Thus, the narrative is the story each participant chose to tell rather than everything that happened during the hospitalization (Hewitt, 2007).
Data Analysis
Data were analyzed by the narrative method based on the perception that narratives are a main cognitive scheme in human development and attribute meaning as a basis for interaction (Gergen & Gergen, 1988; Polkinghorne, 1991, 2014). Repeated elements across narratives reflect the authentic narrative as was expressed by participants. The analysis was guided by the holistic principle that views narratives as whole experiences whose parts are related to each other, openings are related to the endings of narratives, pivots of content are interrelated, and episodes that seem unrelated may be revealed as linked to one another (Bruner, 1991; Josselson & Lieblich, 2001; Polkinghorne, 1988; Riessman, 2008). The wholeness principle draws upon constructive ontology and epistemology (Spector-Mersel, 2010b, 2011).
Data analysis is based on four distinct analytical steps. The first three steps of the analysis draw on the method of selection mechanisms (Spector-Mersel, 2010a, 2011, 2014). The fourth step of the analysis draws on the Bricolage approach (Kincheloe, 2001, 2005a, 2005b). The selection mechanisms method aims at a tight correspondence between narrative epistemology and methodology by interpreting narratives in a way that reveals the narrative identity which each interviewee claimed via the narrative (Spector-Mersel, 2010a, 2014). Each narrative consists of six selection mechanisms, elaborated below, through which biographical facts are chosen, filtered, and sorted to organize events and confirm an endpoint of the narrative. I, therefore, sought to identify the six selection mechanisms and the endpoint in each narrative.
The Bricolage approach examines phenomena from multiple perspectives enhancing rigor, richness, and depth of making meaning in a single study (Denzin & Lincoln, 1999; Kellner, 1999). In the fourth step, I added the group perspective to the analysis. Kincheloe’s Bricolage approach (2001, 2005a, 2005b) embraces complexity by viewing subjects not only as detached-in-themselves, but also as connected between them, exploring the role of power in shaping narratives. Adopting Kincheloe’s approach, I analyzed commonalities in narratives of subgroups of participants, which entailed dimensions of power relating to interactions with physicians.
In the first step, each transcribed interview was read and reread as a whole unit. Initial themes were identified for each participant. In the second step, each narrative was analyzed using six selection mechanisms that describe what participants unconsciously chose to tell and what they chose not to tell, in the content and form of the narrative (Spector-Mersel, 2010a, 2014). The following selection mechanisms were identified: inclusion—relating to facts and experiences reported and a common motive among them (e.g., detailing everything that had happened from admission until discharge); sharpening—relating to events that participants highlighted (e.g., lack of privacy as the nurse yelled to other nurses, “Bring me a bedpan”); omission—relating to events that participants viewed as irrelevant to the desired endpoint (e.g., disregarding the dynamics with one’s significant other); silencing—relating to events that participants perceived as conflicting with the desired endpoint (e.g., stories of other patients with whom a participant had interaction); flattening—relating to the minimization of events that participants perceived as unimportant (e.g., a participant’s distress as a young father who has not seen his children for about a month); and attribution of appropriate meaning—relating to meaning attributed to events that participants found to accord with the endpoints, although they may not necessarily fit their original meaning (e.g., attributing meaning to the degrading attitude of the staff).
In the third step, the endpoint of each interview was identified, as it emerged from the analysis using selection mechanisms (e.g., “Although I am dependent on the staff and although I am seen as part of a collective of patients rather than as an individual, I will represent my-self by not signing the informed consent form”). In the fourth and final step, common themes in narratives of participants by subgroups were analyzed stressing the impact of communication on patient trust and self-worthiness throughout the trajectory of building trust in acute care.
Results
Patients mostly related to one treating physician, by name, when they described the communication that resulted in either trust or distrust. Participants processed their experiences through the evaluation of congruency between their expectations from the physician and the actual communication. There was no change in attitude toward physicians between the two interviews. Due to the high reputation of Israeli hospitals and patients’ assessment of their care needs, participants expected good clinical outcomes. Although all participants were discharged from the hospital with improved outcomes, six themes of barriers to patients’ trust in physicians emerged from the analysis. Themes that were articulated in 20% to 100% of the interviews and that entailed potential for improvement of the patient experience were marked. Barriers were folded within the narratives, appeared by phase of the hospitalizations, and were related to physician–patient communication.
One phase was admission and presurgery, and the second phase was postsurgery through discharge. Presurgery barriers to trust were lack of acknowledgment of the patient’s sense of crisis, physicians’ determination to save life at all costs despite patients’ right for autonomy to choose or refuse treatment, and unique, rather than universal, empathy. Postsurgery barriers to trust were mistaken attempts to communicate with patients to alleviate their loneliness rather than providing legitimacy for their self-alienation in processing their feelings, patients’ expectation for medical professionalism, and lack of attentive listening by physicians. At the subgroup level, commonalities among experiences of participants illustrate links between trust, distrust, and self-worth post-discharge.
Presurgery Barriers
Lack of acknowledgment of patients’ crisis in the routine of physicians (emerged from all narratives)
Patients expected physicians to explicitly acknowledge their transition from routine to crisis. The perceived insensitivity of physicians to the unique crisis experience that patients were undergoing, from routine to crisis, increased patients’ self-withdrawal and created an encounter beset by anxiety, lack of cooperation, and distrust. One participant shares her observation and feeling of being transparent instead of receiving acknowledgment for her crisis: I noticed that they are coming and going and talking about the surgery like a regular person would talk about their flower arrangement.
In a similar vein, another participant adds his reflection, “Physicians distance themselves from us, from our fears, our needs and our feelings. They don’t know how it
Physicians’ determination to save lives at all cost despite patient’s right for autonomy (emerged from half of narratives)
Patients new to the disease felt insecure and accepted the physicians’ treatment decisions. As patients became more familiar with their disease, learned about possible treatments, and consulted with others, they realized that despite their lack of medical knowledge, they have a right to choose whether or not to receive treatment and which treatment to receive. Blurred boundaries between the autonomy of participants and the limits of medical authority created tension and distrust. One participant describes this realization: “I did not agree and they cannot make me . . . otherwise they would not ask me to sign . . . If they cannot do that without my signature, then the authority is mine.” Another participant explains his rationale for refusing treatment: I am an educated patient at this point, I can stop any procedure at any phase and they can legally do nothing.
One participant compares himself with other patients and shares his thoughts: Patients without a strong character don’t know how to fight them—their healing will not be complete. I’m half a paramedic, I understand things, and they can’t do whatever they want with me. I pity those who have no one to represent them.
Participants felt that physicians believed they understood their condition better than they did, and to save their lives or to be more efficient, they dictated treatment rather than held a dialogue with them, thereby, breaching their trust.
Physicians’ use of unique rather than universal empathy (emerged from a quarter of the narratives)
Crisis, pain, and expectations for high-quality care create high emotional complexity among participants who were affected by layers of thoughts, doubts, and behavior. By mapping the emotional state of patients, physicians may choose how to express their empathy. One participant judged the style of empathy: “Physicians don’t always have interpersonal communication that goes well with who you are and what you need. They are completely dry. They have no energy to fuss with you.” Another participant was irritated by the physician who approached her with a genuine intent to help her but projected his world on to hers, demonstrating paternalism and disrespect toward participant’s preferences: After several hours in acute-care, I needed something for the pain again. The physician said, “I understand that you are in great pain. Take your pain to a positive place, think Zen” . . . So condescending! . . . I was furious with him.
If communication skills of physicians do not fit the complex emotional state of patients, they may perceive physicians as being condescending and disconnected, thereby creating distrust.
Postsurgery Barriers
Physicians’ delegitimizing patient’s self-alienation while confusing it with loneliness and encouraging communication (emerged from all narratives)
Even when physicians communicated with participants and when participants had visitors who came to support them, participants experienced self-alienation (distancing oneself from one’s own feelings due to emotional stress). This may seem like loneliness or isolation but it is not: Their self-alienation emerged due to their perception that others, including physicians, are unable to know what they were experiencing. When physicians confused self-alienation with loneliness, it was burdensome. One participant offered a glimpse into his inner dialogue: You lose yourself from day one. It hurts so much. My spirit is broken. . . . [Quiet] . . . but I chose to alienate myself . . . I don’t know why . . . I need it . . . maybe it’s because when I shut my world from the outside I don’t feel like a cripple . . . I don’t know . . . I have a concealed hate towards anyone who can move their legs and no one can understand that but the doctors kept encouraging me, once I was out of the ICU, to invite my friends to visit but I was not ready to talk about books and movies as if everything is the same.
Another participant describes his self-alienation as a way of processing and coping with the disruption that cancer created in his life: Not everyone can stand this. You are actually moved to a different planet, to a parallel universe in which routine life is pushed into a corner. What would I gain from sharing it with anyone? I just wanted my simple day-to-day routine back. I felt an urge to take my kids, get into my car and run away to someplace nice . . .
Physicians who listened attentively and expressed compassion for the self-alienation that participants felt, without pretension to know how they feel, maintained trust and facilitated healing relationships with participants. Participants’ self-alienation is mixed with fear, disappointment, and a sense of betrayal by the body as well as an anxiety that the illness is severe. Alienation is felt within the patient’s self and is part of the grieving period due to loss of health and functionality (Younger, 1995).
Lack of medical professionalism (emerged from 10 out of 12 narratives)
Findings stress that lack of medical professionalism creates distrust. Medical professionalism entails integrity, compassion, altruism, excellence, and working in partnership among team members (Working Party of the Royal College of Physicians, 2005). Participants expected medical professionalism and observed that competent physicians may be challenged by medical professionalism. Participants categorized their physicians on two axes: clinical competence and medical professionalism. Based on these axes, participants formed their perception regarding their physicians: clinically competent but no medical professionalism, medical professionalism but not high clinical competence, no medical professionalism and no clinical competence, and, finally, clinically competent and strong medical professionalism.
One participant shares his impression of the gap between his expectations for medical professionalism and the communication he experienced: “They have no time for us patients and no patience or energy whatsoever.” Another participant added his similar observation, attempting to explain the physicians’ attitude: “They send you a message that there is no room for sensitivity towards you, that it’s not part of medicine, and it’s not their responsibility.” One participant shares an illustration of the lack of professionalism: The anesthesiologist was digging to find a vein and connect the tube, it was so painful, I was screaming my lungs out but he kept going and said nothing. At some point, my surgeon stepped in, heard me and scolded at him to immediately stop: “Why don’t you do that when she is sedated?!”
A young participant also expressed the gap between professional values she expected to experience in communication with physicians and her actual experience: I wanted to ask the physician: “Why did you choose to become a physician?” He had no compassion . . . And he talked about me over my head as if I were not there, as if I were a museum exhibit. It was so degrading . . . [Tears in her eyes].
Lack of attentive listening by clinicians (emerged from 10 out of 12 narratives)
Participants who felt that their physician did not really listen to them as they answer questions regarding their physical symptoms, allergies, and medication sensitivity tended to feel frustrated with physicians, anxious, and insecure about physicians’ ability to meet their clinical needs. One participant repeatedly reported pivotal medical information to the physician, hoping that he would be attentive to the implications of the information while treating him: “I exhaustingly detailed the meds I am allergic to but it didn’t prevent him from prescribing me exactly some of those meds before the procedures.” Another participant described a similar experience: “In the internal ward they treat you like meat, I kept saying things over and over but they kept at it. As if patients are their guinea pigs . . .” Another participant shared similar observations: “They did not listen when I said that I am sensitive to iodine.” One participant shared an observation that the lack of attentive listening extends beyond failure to listen to what patients said to lack of attention to the condition of the patients and its implications: They needed to stop the treatment that caused my hyperglycemia and heart palpitations but the anesthesiologist belittled me and didn’t listen. He was still going to take me into surgery. My primary care physician rushed to the hospital and prevented the surgery. I could have died!
Two participants concluded, “Physicians don’t listen any more, they don’t listen”; “They don’t listen to us. I can’t even fathom what they do to old people or to people who don’t think straight.” Principle anecdotes across narratives of participants highlight PCC elements that physicians may adopt not only to construct significant care relationships (Peltola, Isotalus, & Åstedt-Kurki, 2018) but also to preserve the self-worth of patients in acute care. Elements of PCC were acknowledgment of the patients’ crisis, attentive listening while according face and body language to context and content, realizing patients’ authority to choose treatment, applying universal empathy, and avoiding communication messages that further decrease patients’ self-worth by medical professionalism. Participants viewed the dialogue regarding treatment choices as pivotal to their trust in a physician. Through the presurgery phase and hospitalization, physicians who assisted patients to sense that they have control by clarifying and assuring understanding of the process and the procedures, even if they are not the ones making treatment decisions, created trust. Figure 1 presents a summary of barriers to trust.
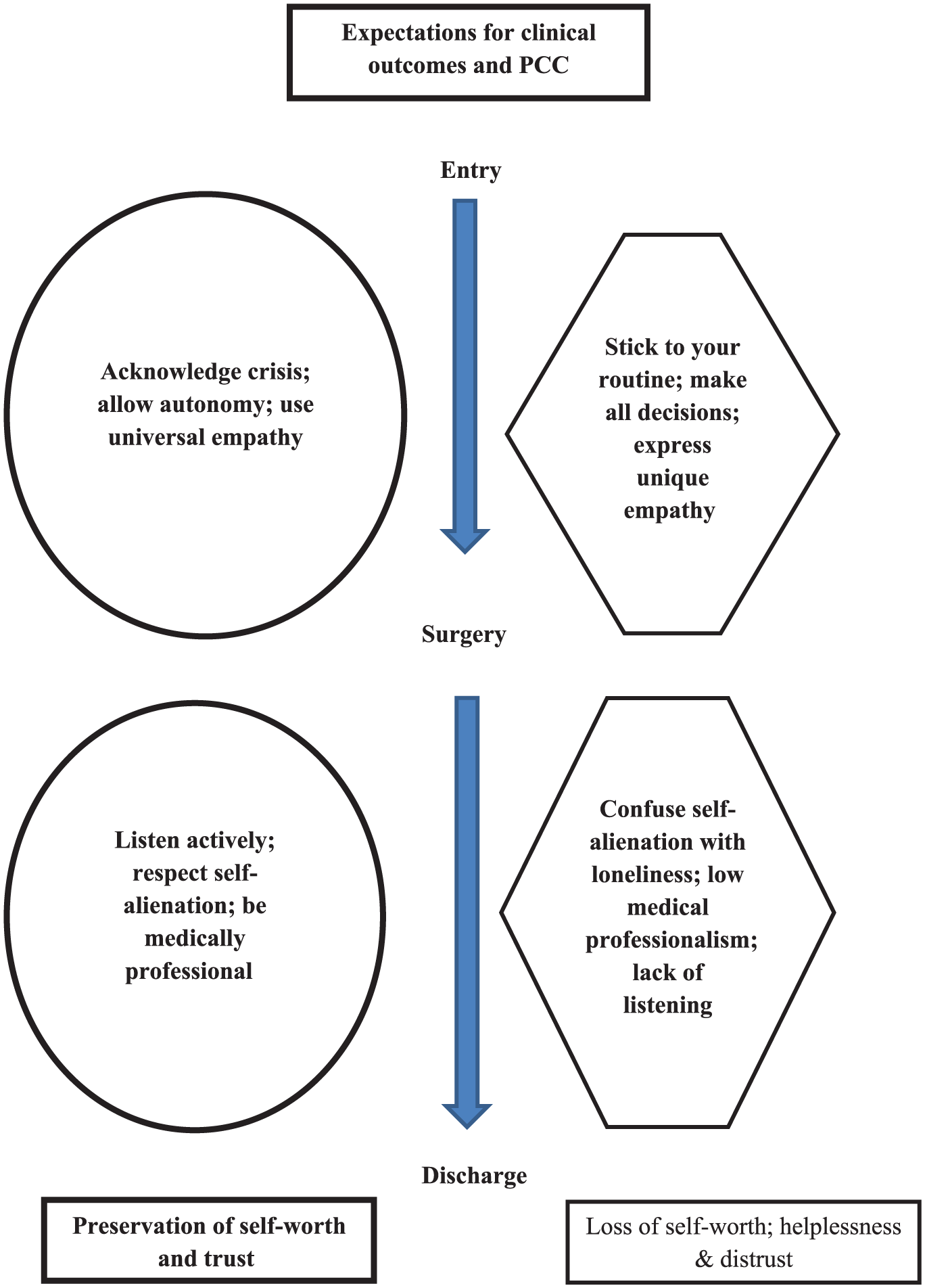
Physician–patient communication and trust.
Common narrative identities of self-worth, trust, and distrust after discharge
Assessment of gaps between expectations and interactions with physicians continued as participants processed their hospitalization experience post-discharge and expressed trust or distrust in physicians. Due to the high reputation of the hospitals at issue, prior to entry, patients expected good clinical outcomes, and their life was, indeed, saved, meeting their expectations for care. Their expectations for PCC, however, were either exceeded or unmet. A strong linking theme across gaps in the expectation for PCC was the participant’s self-worth. Looking closely at how physician–patient communication reflected on the self-worthiness of patients, I identified the narrative identity for each subgroup of participants (Kincheloe, 2001, 2005a, 2005b).
Two common narrative identities as patients who are hospitalized in acute care were found: preservation of self-worth and trust and loss of self-worth, helplessness, and distrust. Nine out of 12 participants shared themes of loss of self-worth, helplessness, and distrust. They not only felt helpless and frustrated with physicians but also felt they depended on them and therefore had no way out. They did not want to upset their physicians and helplessly accepted the reality of hospitalization. Three participants experienced a deep loss of self-worth and expressed distrust in physicians and hospitals: “Being hospitalized is like a roulette-wheel . . . you never know how physicians will treat you and what care you will get”; “It’s best to stay away from all physicians”; “I still have flashbacks from the degrading conduct of my doctor during those three weeks.” Another participant, in a quiet, sad tone, sums up her insights: Hospitalization is a bad experience, you can’t decorate it. It’s bad. You can’t win. I felt as if I was the little kettle that needs fixing in the huge plant. Had I sensed that the doctor sees me, I may have felt better. Physicians are supposedly involved with our diseases and diagnoses but they turned into technologists, they totally forgot to be healers. I asked my girlfriend to come take me home. She convinced me to stay but I wanted to leave the hospital.
Some participants described the tension and conflict they experienced: I refused to let them permanently connect the IV to my veins. They wanted to do it so they can comfortably and swiftly reach my heart through a main vein with a catheter. It would have been convenient for them . . . but I refused. He pressured me again and again. . . . Until I said out loud, “Stop bothering me, it’s my choice.”
The communication that nine out of 12 participants experienced contrasts the value of responsibility to self-worth of another. They experienced communication that weakened their self-worth and resulted in distrust in the physician despite positive clinical outcomes. They lost trust not only in their attending physician but also in all physicians and in hospitals. For them, the hospitalization remained a traumatic experience.
Three participants shared the common narrative identity of preserving self-worth and trust. They received support through the acknowledgment of their crisis, medical professionalism, and attentive listening of their physicians. They were aware that they belong to a collective of patients, but perceived themselves as different from other patients. Based on information they received, they felt they are in control despite their dependence on physicians who made the decisions. They structured the time during their hospitalization to learn about the disease and treatments in a manner that maintained their prehospitalization self-value: Some doctors make every effort possible to ignore eye contact with you, especially in the corridor. Not my doctor. He would easily make eye contact and stop to ask how I was doing today and if I have any questions. Sometimes when I wanted to ask a question he said “I don’t have time to talk about it right now” . . . but he would not forget and come back to my room later to continue to talk about it . . . [Quiet]. I felt that I am respected and for me that is the power of the sense of calling, of his caring, of being humane. My doctor was great. Courteous, stern at first, but the minute he started treating me, it was clear he was very professional. Even on the weekend he came to see how I was doing, he fixed my catheter after my heart surgery by himself although he is a senior doctor. He changed everything very gently and wanted to assure I was in good spirits. He is a good person. He demonstrated a lot of accountability. The doctor was so sensitive to me, was filled with caring and compassion, and encouraged me through those horrible days. His mere positive presence meant a lot to me, he gave me a lot of strength and hope. His dedication to my well-being shows what sacred work doctors do.
These results indicate that the prominent biomedical approach to care resulted in depersonalization, poor patient experiences, and distrust in physicians not only pre- and postsurgery but also after discharge, compromising participants’ self-worthiness.
Discussion
This narrative study explored patients’ perception of their interactions with their physicians while in an acute-care setting due to cancer, cardiac disease, neurological disease, or accidents. The contribution of this study is threefold. First, theoretically, this study expands our knowledge of specific PCC elements that are important, from the patients’ perspective, to building patient trust in physicians and of communication elements that created patient distrust in physicians. Second, this study elaborates on the relationship between the preservation of patient self-worth and patient trust in physicians in acute care. Third, the suggested recommendations may raise awareness among physicians, allowing them to embed specific PCC elements in their practice, preserve patients’ self-worth, reduce distrust, and improve quality of care. Three presurgery barriers to trust were lack of acknowledgment of the patient’s sense of crisis, physicians’ determination to save life at all costs despite patients’ right for autonomy to choose or refuse treatment, and unique, rather than universal, empathy. Three postsurgery barriers to trust were mistaken attempts to communicate with patients to alleviate their loneliness rather than providing legitimacy for their self-alienation in processing their feelings, patients’ expectation for medical professionalism, and lack of attentive listening by physicians.
Medical Professionalism and Trust
Participants complained mostly about physicians’ poor medical professionalism, echoing findings of previous studies (Baillie, 2009; Lohne et al., 2010). Participants associated lack of physicians’ medical professionalism with poor understanding of their mental and emotional state and, therefore, with less humanity and lesser clinical competence, resulting in distrust. Similar to participants in the study of Hupcey and Morse (2000), participants became angry and felt forced to receive care while in a vigilant state of distrust. Furthermore, the agitation and anxiety of participants created complex situations that required physicians to tailor what they said and how they said it to the emotional needs of their patients. In line with previous findings, participants expected physicians to enhance their health literacy by explaining their diagnosis and treatment (Champlin, Mackert, Glowacki, & Donovan, 2017). In line with previous findings, the distrust of most participants in this study extended beyond distrust in their treating physician to distrust in all physicians and hospitals (Hupcey & Morse, 2000). Findings of this study call to integrate the biomedical approach with the psychosocial approaches to care which preserved participants’ self-worth, which is essential to patient trust.
Patient’s Self-worth and Trust
Patient–physician trust in acute care develops, in part, due to a valuing attitude that clinicians reflect toward patients, leading to preservation of patients’ self-worth (Elander, Beach, & Haywood, 2011; Fu, McNichol, Marczewski, & José Closs, 2018; Gabay, Moskowitz, Silcher, & Galanter, 2017). Participants moved from initial trust in physicians to distrust as they felt that physicians mainly related to their disease and organs but neglected their emotions at their time of crisis and did not see them as a whole person. Findings highlight the relevance of Levinas’s philosophy regarding face-to-face encounters in asymmetric relationships.
Responsibility to Another’s Self-worth in Face-to-Face Encounters
Physician–patient communication represents the basics of ethics in health, particularly in complex situations that may be a turning point in patients’ lives: hospitalization, acute care, surgery, bad news, an extended ambiguous diagnosis, organ transplants, and more. In such situations, physicians may view a patient as part of a group, perhaps unconsciously creating alienation and heightening patient anxiety, or view each patient as an individual. An individual with self-worth can also be a partner to decision-making. Most participants, however, felt helpless in the face of the power of physicians.
Applying Levinas’s philosophy on asymmetric relationships, I contend that despite physicians’ excess power in medical situations, physicians have no right to control the patient’s body or soul, but may humbly acknowledge the patient as an individual and even perceive the patient as a teacher. For accurate diagnosis, physicians depend on patients to report accurate information regarding specific symptoms of the disease in their body. Furthermore, Levinas (1961) introduces the concept of “the face of the other” (p. 297). The concept of the “face of the other” may facilitate a balance between responsibility of physicians for the patient and physicians’ respect for the patient’s uniqueness.
By “face,” Levinas refers to a source of meaning that expresses the living presence of a patient. Applying this concept to this study, the face of the patient expresses the patient’s vulnerable individual presence that is undeniable, and, therefore, cannot be reduced to a group image. A focus on a patient’s face may allow physicians to see an individual, go beyond themselves, and regulate their immediate constraints. The patient’s “face” may also set boundaries over the entity of the patient versus that of the physician, avoiding the use of excess power. Following Levinas, who calls to direct excess power toward empowerment, rather than dictating a path, physicians may frame patients’ refusal of treatment as patient centeredness (Machin, Goodwin, & Warriner, 2018).
Practical Recommendations
This study suggests four recommendations to build trust through medical professionalism and PCC. Coaching among clinicians improved their ability to build better relationships with patients (De Haan, Duckworth, Birch, & Jones, 2013; Theeboom, Beersma, & van Vianen, 2014). Therefore, I believe in physicians’ ability to adopt PCC and build patient trust. To build trust, first, physicians are called upon to discuss values that drive their relationship with patients. Hospitals may translate Levinas’s (1981) value of responsibility to another’s self-worth into a professional responsibility to communicate in ways that avoid the patient’s further loss of self-worth.
Second, training aimed at medical professionalism should focus on trust-building PCC. The physicians’ communication style and messages are to be tailored to needs of individual patients (Anderson, Cimino, & Lo, 2013). The adoption of PCC requires genuine engagement and emotional openness as well as congruence between body language and verbal messages of sincere feelings and concern for patients. This emotional labor is part of the physician’s role and responsibility (Larson & Yao, 2005).
Third, hospital managements and clinicians may explore barriers to trust from the patients’ perspective as part of quality improvement processes. Awareness of physicians to the six barriers to trust in their communication with patients may allow physicians to choose wisely among the specific elements of PCC and embed them in their daily routine. Last, but not least, physicians are exposed to emotional risks due to their continuous exposure to trauma, potential lack of interpersonal skills, and potential lack of skills required to establish caring relationships. Hospital managements are, therefore, called upon to explore ways to integrate the value of responsibility for another’s self-worth in the organizational culture across departments and health professions.
Future Studies
Future studies should explore differences in experiences of patients by gender and by age group. Future studies may examine interventions to implement the value of responsibility to the self-worth of patients despite the constraints of an intense work environment. Also, future studies may explore ways to encourage patients to seek information during their hospitalization. Finally, future studies should also examine physicians’ points of view on PCC and trust. What do physicians view as challenges in applying their best intentions regarding the ideal care on a path filled with potholes?
Conclusion
Inspired by Levinas, I contend that to build trust, physicians are called upon to extend their dedication. Physicians are called upon to extend their dedication from dedication to improved clinical outcomes to dedications to improved clinical outcomes and to preservation of patients’ self-worth.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.