
Abstract
Developing safety interventions using patient feedback is valuable for creating safer systems of health care. A qualitative process evaluation of a patient feedback on safety intervention was undertaken in six primary care practices. The purpose was to theorize factors mediating with the implementation of the intervention using existing theories. The intervention required practices to obtain patient feedback on safety using a validated tool and respond using quality improvement methods. Multiple methods of qualitative data collection were used, including interviews and overt observation. Abductive reasoning informed the iterative process of analysis that examined theories relevant to the intervention and setting. A theoretical framework was developed, which encompassed mediating factors grouped under three concepts: practice readiness, utilization of problem-solving skills, and agency. Theorizing mediating factors was necessary to understand the complexities of primary care practices, and to identify the essential components for implementation of the intervention on a larger scale.
Keywords
Introduction
Engaging patients in the prevention of harm and error is imperative for the development of safer systems of health care (World Health Organization, 2009). Evidence supports the acceptability and feasibility of obtaining patient feedback on safety for system learning and improvement (Kiran et al., 2019; Lawton et al., 2015, 2017; Wright et al., 2016), in addition to responding to clinical incidents (The Health Foundation, 2013; Hernan et al., 2014, 2015; Vincent & Davis, 2012), modifying health professional behavior (Kirkman et al., 2015; Reeves et al., 2017), and improving delivery of evidence-based health care (Pronovost et al., 2008; Taylor et al., 2013). Interventions engaging patients have demonstrated a reduction in adverse events and risks relating to falls, pressure ulcers, and medication errors (Park & Giap, 2020).
Patient safety research has predominately been based in the hospital context, with a small but growing consideration of the primary care context (Lawati et al., 2018; Lawton et al., 2017; Ricci-Cabello et al., 2016; Wright et al., 2016). In many health systems, primary care practices serve as the first point of contact for people seeking health care and have an important role in improving patient safety (Department of Health, 2013). Patient feedback has the potential to transform primary care systems, contribute to quality improvement (QI) interventions and improve patient safety (Hovey et al., 2011; Kiran et al., 2019). Developing approaches to obtaining patient feedback on safety and constructing interventions based on this feedback are emerging areas of health research (Giles et al., 2018; Hernan et al., 2016; Wright et al., 2016).
A specific patient feedback tool, the Primary Care Patient Measure of Safety (PC PMOS) tool was developed and validated (Giles et al., 2018). The purpose of the PC PMOS tool was to obtain patient feedback on the contributing factors to safety incidents in the primary care environment (e.g., communication, team factors, and timely access of care), rather than relying on the identification and analysis of incidents retrospectively. The PC PMOS tool was trialed, with a corresponding intervention that utilized QI methods to respond to patient feedback, in the Australian primary care setting (Giles et al., 2018; Hernan et al., 2019, 2020). The trial was informed by other patient safety research that used QI methods as a key intervention component within the hospital setting (Lawton et al., 2017; O’Hara et al., 2016; Sheard et al., 2017a, 2017b). Results of the trial demonstrated that the intervention was feasible and patient safety scores indicated improved safety (Hernan et al., 2020). Safety interventions developed and implemented by practices included strategies targeting specific components of the PC PMOS tool (i.e., reduce waiting times and increase the availability of appointments to improve service accessibility) and strategies to respond to patient-reported safety incidents (Hernan et al., 2020).
Alongside the trial, a qualitative process evaluation was undertaken. The purpose was to theorize factors mediating with the implementation of the intervention by examining existing theories pertinent to the intervention and setting (Kislov, 2019; Oakley et al., 2006). Similar approaches have been used in other patient safety research to develop explanatory theories to capture the relationship between intervention components and system complexities (Louch et al., 2017; Sheard et al., 2017a, 2017b). More broadly, theorizing processes have been used to explain the intended and unintended effects of implementing QI interventions in the health care setting (Dixon-Woods et al., 2011).
Due to the complexity of the patient feedback on safety intervention, considering multiple theories prospectively was inherent to the theorizing process as there was not one single theory that provided sufficient breadth and depth to examining contextual factors mediating with the implementation of the intervention by participating primary care practices (Davidoff, 2019; Dixon-Woods et al., 2011; McIntyre et al., 2018). Examining existing theories pertinent to the primary care setting, the utilization of QI methods as a key intervention component, and the characteristics of exemplar practices were required.
In this study, the primary care setting was theorized through a lens of complexity science. Primary care practices, like other health care systems, are complex adaptive systems (CASs) that are multifaceted, subject to competing clinical and nonclinical demands, and uncertain (Braithwaite et al., 2017). As a CAS, primary care practices also comprise different organizational structures and behaviors at multiple levels, which change and evolve over time (Braithwaite et al., 2017). Embedded in this understanding, there were many system and contextual variables that required close examination when implementing a novel intervention across multiple primary care practices.
Intervention complexity in this study was also compounded by the utilization of safety and QI methods as a key intervention component (Hernan et al., 2019). Multiple theoretical frameworks exist, which explore factors thought to influence the success of QI interventions in the health care setting. Two frameworks pertinent to the study included the Model for Understanding Success in Quality (MUSIQ) and Informing Quality Improvement Research (InQuIRe) in primary care framework (Brennan et al., 2012, 2013; Kaplan et al., 2012). The MUSIQ framework was developed from a review of the literature and expert consensus (Kaplan et al., 2012) and captures the relationship between 25 contextual factors organized at three levels: microsystem (e.g., QI leadership and motivation), organization (e.g., QI culture), and environment (e.g., external motivators; Kaplan et al., 2012). Similarly, the InQuIRe conceptual framework identifies contextual factors mediating with the implementation of QI projects in primary care at the organizational (e.g., capability for QI leadership), team (e.g., team composition, attitudes), and individual (e.g., knowledge, skills, and efficacy for QI) level (Brennan et al., 2012, 2013). Both the MUSIQ and InQuIRe frameworks provided a foundation for understanding system complexities. However, these frameworks offered very little guidance to understanding the inputs and processes that practices used to implement new interventions using QI methods (Davidoff, 2019). Although specific to primary care, the InQuIRe framework provides a limited explanation as to how contextual factors interact with each other during the QI process, when compared with the MUSIQ framework, which illustrates the relationships between different system levels and their influence on outcomes (Brennan et al., 2012, 2013; Kaplan et al., 2012).
To theorize the characteristics of exemplar practices involved in this study, a positive deviance approach was used, which requires a close analysis of high-performing organizations and health care teams by studying “positive deviants” or effective practices pertinent to the phenomena of interest (i.e., What works?) (Lawton et al., 2014). One component of this was identifying the characteristics of agents of change in health care teams and how the implementation of new interventions was facilitated. The Institute for Health Improvement’s (IHI) Psychology of Change (Hilton & Anderson, 2018) was identified as a useful framework to understand the theoretical underpinnings of how agency is activated in individuals and teams in the context of implementing a novel intervention. Using these aforementioned theories pertinent to the primary care setting and intervention, the purpose of this study was to theorize factors mediating with the implementation of the patient feedback on safety intervention through a qualitative process evaluation.
Method
Study Background, Setting, and Intervention
A study protocol detailing the design, sampling frame, and intervention has been published (Hernan et al., 2019). Six primary care practices located in Victoria, Australia, were purposively sampled based upon their experience in participating in previous QI projects. Due to previous QI and patient safety research undertaken in the region, some of the participants were known to members of the research team. The intervention required practices to distribute a patient feedback on safety survey—the PC PMOS—to patients at two time points (T1 and T2). The PC PMOS is an internationally validated tool that prospectively collects data concerning contributory factors to potential safety incidents in the primary care setting such as communication, access to care, task performance, and information flow (Giles et al., 2018; Hernan et al., 2016). It is an anonymous 28-item survey, covering nine domains of safety (Giles et al., 2018; Hernan et al., 2016).
PC PMOS data were then pooled and provided to practice teams at T1 to use as a basis for developing and implementing practice-specific safety interventions. Developing and implementing safety interventions was facilitated through application of the Model for Improvement (MFI) QI framework (Langley et al., 2009). Practice Safety Intervention Teams (SITs) received training and education about QI from expert facilitators at two structured workshops and a practice-specific action planning meeting (APM) during the intervention period (6 months). The findings of the T2 survey were then used to measure any changes in patient feedback on safety. The results from the trial have been published elsewhere (Hernan et al., 2020).
Type of Process Evaluation
The use of process evaluations to understand the implementation of complex interventions in health care has increased in prominence (Bunce et al., 2014; McIntyre et al., 2018; Mills et al., 2019; Oakley et al., 2006; Sheard et al., 2017a). Engaging with theory during process evaluations of health interventions is reported to be widespread, yet few process evaluations aim to extend existing theory or create new theories (McIntyre et al., 2018). Furthermore, researchers are encouraged to theorize using qualitative data and move beyond narrative approaches to qualitative research (Morse, 2004). An abductive approach to theorizing was utilized to critically examine existing theories in the context of new qualitative data and to understand how, for whom, and in what context the patient feedback on safety intervention worked (Langley, 1999; Mills et al., 2019; Tavory & Timmermans, 2014). Theorizing through a process evaluation was an essential step to considering opportunities to scale the intervention for wider adoption and translation into clinical practice (Dixon-Woods et al., 2011; Kislov, 2019; Mills et al., 2019).
Data Collection
Multiple methods of data collection were used (Figure 1). Sources were triangulated to capture various aspects of the implementation process (Flick, 2007; Reeves et al., 2014) (Online Appendix I). Triangulating data collection methods and sources ensured that findings were embedded in the context of inquiry and able to capture multiple variables across the different levels of primary care practices (e.g., individuals, SIT, and organizations), rather than be reflective of a single voice (Hammersley & Atkinson, 2007). A longitudinal qualitative approach to data collection also captured contextual changes over time (i.e., interviewing the same participants at different time points during the intervention and following the intervention; Calman et al., 2013). A plain language statement (PLS) was provided to all participants, which explained the study components, duration of the study, and time required for participation. Written organizational and individual consent was obtained from participants for the duration of the study.
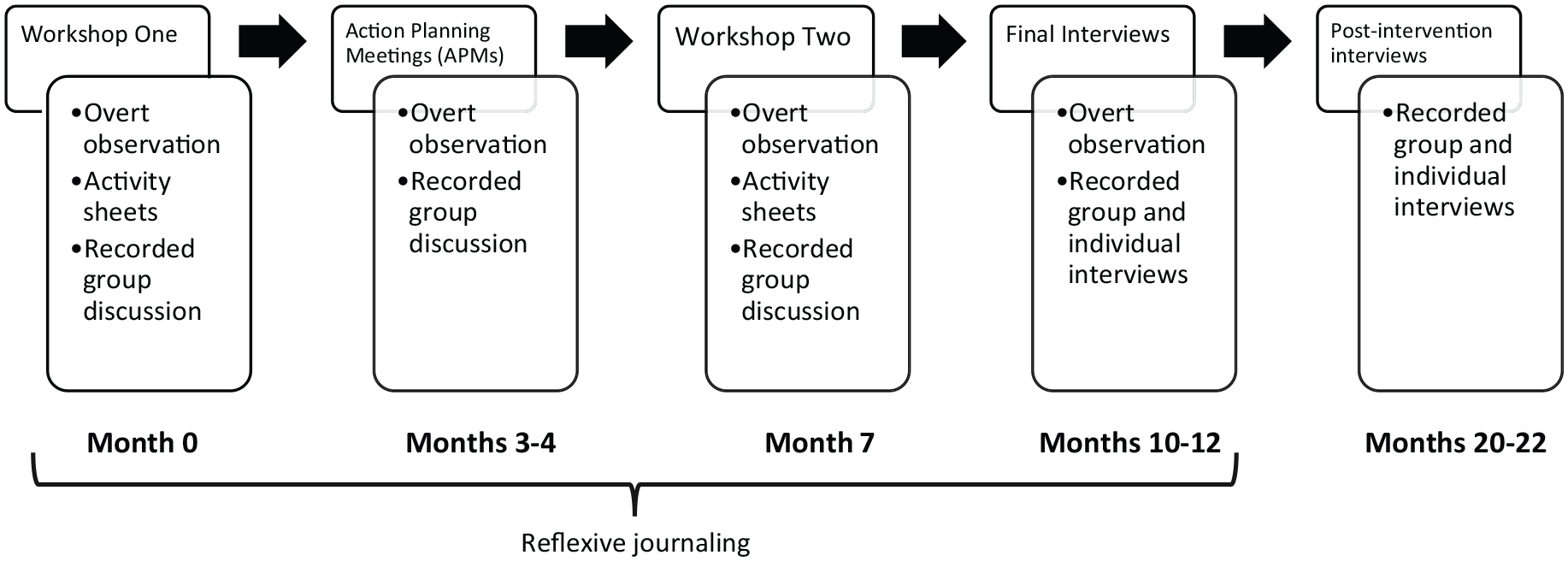
Data collection methods.
Participant observation
Overt participant observation was undertaken during workshops and APMs. All sessions were audio-recorded for analysis. A template was developed for each event (Online Appendix II) and used to document observations in real time, which included visual observations, such as room layout, nonverbal communication, and interactions between participants. Descriptive contemporaneous field notes were written by the researcher conducting observations, whereas other researchers facilitated workshops and APMs.
Reflexive journals and researcher debrief
All researchers involved with sessions participated in a verbal group debrief following workshops and APMs. Engaging multiple field researchers was an important component of a thorough qualitative process evaluation. These debriefs were audio-recorded and transcribed, with the purpose of identifying emerging issues from the sessions and sharing theoretical insights. Debriefs were also used to facilitate reflexive practice by providing an opportunity to critically reflect on the role of the researchers in presenting or facilitating sessions and any observed power imbalances. Two researchers maintained a reflexive written journal, which considered how the role of the researchers interacted with data collection and analysis, in addition to the documentation of emerging issues (Finlay, 2002; Higginbottom et al., 2013).
Interviews
Individual semi-structured interviews and practice group interviews were conducted at the conclusion of the study and post-intervention by two female researchers involved in delivering the intervention and four other female researchers not involved in the intervention delivery (Figure 1). All researchers had experience in conducting qualitative interviews. An interview guide was developed from the preliminary analysis of trial data and review of the relevant literature, including theoretical frameworks and other patient safety research (Brennan et al., 2012, 2013; Hilton & Anderson, 2018; Kaplan et al., 2012; Langley et al., 2009; Lawton et al., 2017; Sheard et al., 2017a), focusing specifically on emerging concepts that required further explanation (Online Appendix III). A second interview guide was used for interviews conducted post-intervention, which was developed from key themes emerging from analysis at the conclusion of the intervention period (Online Appendix III).
Data Analysis
Abductive reasoning shaped the analysis of qualitative data and process of theorizing. As a pragmatist qualitative approach, abductive analysis develops or extends theory through an iterative and recursive process of engaging with established theories and new research data (Kislov, 2019; Tavory & Timmermans, 2014). This was selected as an appropriate analysis method to critically extend the aforementioned theories in the context of inquiry. In approaching the analysis with multiple perspectives and hypothesis (theoretical triangulation; Braithwaite et al., 2017; Brennan et al., 2012, 2013; Hilton & Anderson, 2018; Kaplan et al., 2012; Lawton et al., 2014), a broad range of factors mediating with the implementation of the patient feedback on safety intervention were able to be identified and explored (Denzin, 1989). Analysis was focused on the microsystem (i.e., participant and SIT) and organization level (i.e., primary care practice), with particular attention to the interplay of contextual factors between these levels (Kaplan et al., 2012).
Two researchers independently conducted first cycle coding of transcripts and documents from the workshops, APMs, and researcher debrief sessions, using elemental methods such as descriptive and In Vivo coding (Saldaña, 2009). NVivo™ (V. 11, QSR International Pty Ltd) was used to store and manage data sources during the process of coding and to support analysis. Codes from independent first cycle coding were compared through discussion between the researchers and were grouped into categories. The aforementioned theories were then discussed by the two researchers in the context of the developed categories. Through a visual and iterative mapping process using a whiteboard, relationships between the aforementioned theories and categories were mapped. This process involved discussion between the two researchers, reorganization of categories, and critical examination of the aforementioned theories to develop a merged coding framework in NVivo (Saldaña, 2009).
The merged coding framework was then reviewed by a third researcher involved in the study and was used to guide the second cycle coding of the interviews and other study documents (e.g., observations, field notes) using focused coding methods (Saldaña, 2009). This relied heavily on the reflexive triangulation of all data sources, including field notes and researcher debriefs, to inform the development of concepts and attributes of these concepts, and to enhance the trustworthiness of findings (Hammersley & Atkinson, 2007). Concepts were then critically reviewed by all three researchers and mapped to existing theories to develop a theoretical framework examining the phenomena of interest.
Ethics
Ethical approval for the study was obtained from Deakin University Faculty of Health Ethics Advisory Group (HEAG 175_2017).
Results
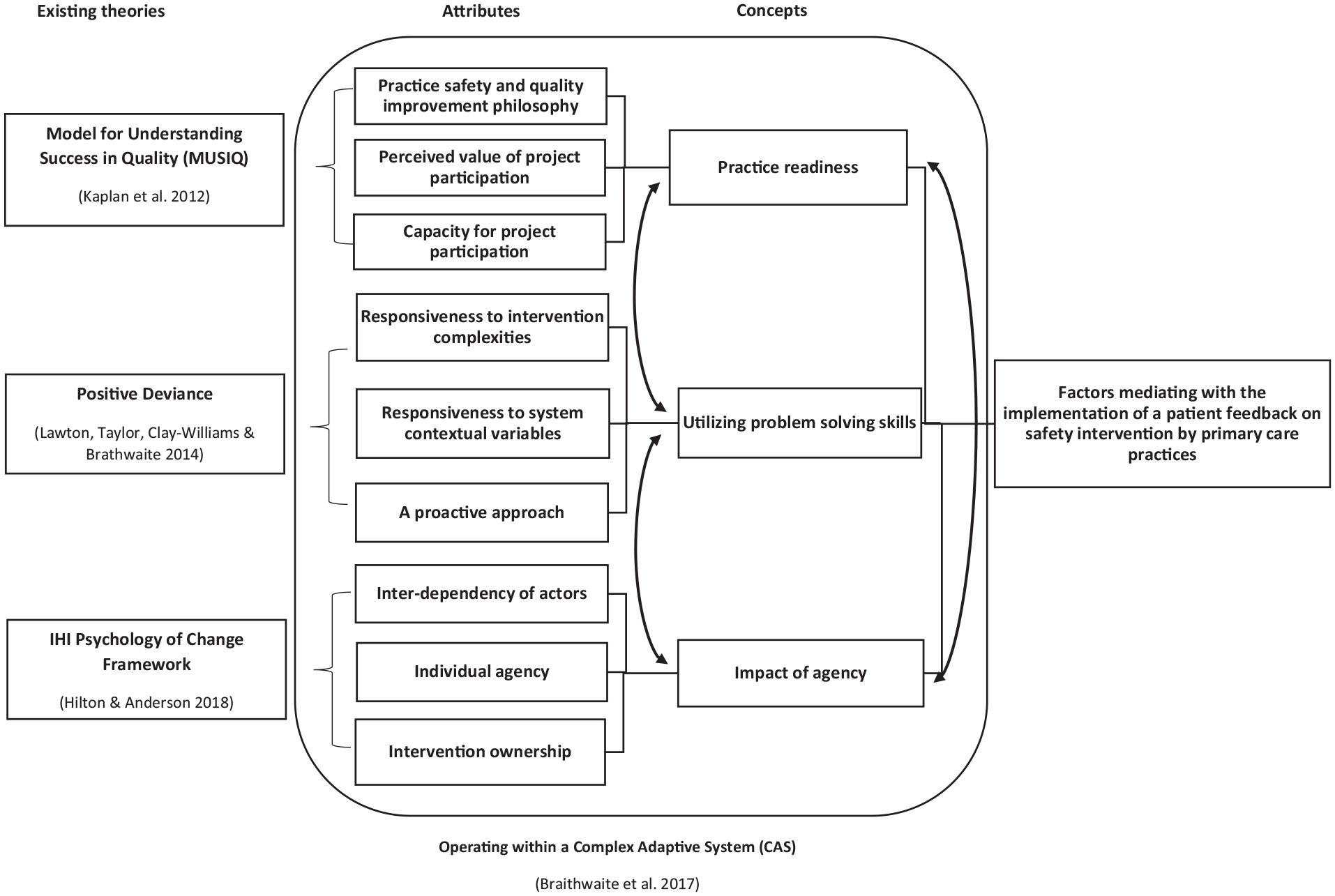
A total of 25 participants from the six practices were involved in the study. Of these, 21 (84%) had been involved in previous QI initiatives (Online Appendix IV). Three concepts, encompassing nine attributes identifying factors mediating with the implementation of the patient feedback on safety intervention, were developed through the analysis process (Figure 2). Concepts included practice readiness, utilizing problem-solving skills, and impact of agency. These concepts were an extension of existing theories (Hilton & Anderson, 2018; Kaplan et al., 2012; Lawton et al., 2014) relating to the context of inquiry, within the understanding that practices were operating within a CAS (Braithwaite et al., 2017). Intervention implementations were dependent on relationships between these three concepts and nine attributes, forming a theoretical framework. This theoretical framework was used to explain how the patient feedback on safety intervention worked, for whom, how, and under what conditions.
Patient feedback on safety intervention theoretical framework.
Practice readiness
Practice readiness was a multifaceted concept, encompassing both the ability and willingness of participants to implement a patient feedback on safety intervention. This was shaped by the attributes of having an underlying quality and safety improvement philosophy, perceived value of project participation, and capacity for project participation. Individual participants and practice teams exhibited varying degrees of practice readiness. Practice teams exhibiting readiness at both the organizational and microsystem level at the commencement of the study, were better placed for successful implementation of safety interventions and QI success. The degree of readiness shifted for some teams through the course of the study as they responded to competing priorities at the organizational level (e.g., computer software issues, structural changes) and microsystem level (e.g., unplanned leave, changes in roles). For some practices, this directly impeded the ability to fully implement safety interventions (Practices A and D).
A shared practice philosophy, concerning the importance of patient safety and QI at the microsystem level, served as an enabler for the initial uptake of the intervention across all practices. Philosophy encompassed underlying beliefs and attitudes. Inherent to this was a commitment to building a QI culture at the organizational level with the purpose of creating a safer health care service. Participants with QI experience also verbalized a personal and professional investment in developing a QI culture at the microsystem level to improve the quality of health services delivered.
A general belief that practices should engage in safety and QI to improve patient outcomes was shared by participants. The embedded organizational philosophy, coupled with recent QI exposure (QI maturity), placed some practices in a more advantageous position for implementing the patient feedback on safety intervention, particularly when all participants involved in the intervention had some degree of QI exposure. Through the course of the intervention period, it was clear, through the documentation of plan–do–study–act (PDSA) cycles and responsiveness to results from the PC PMOS tool, that practices with these characteristics were well positioned to transfer skills gained from previous QI projects (i.e., using PDSA cycles) for the development and implementation of the patient feedback on safety intervention (Practices B, C, and E). This included identifying QI leaders within the practice to support intervention development and implementation: I think the model for improvement, and I think the process and I think the PDSAs, it is a good process and it’s simple but sometimes we complicate it by making it bigger than what it is . . . I think if you’ve got a leader in charge of the group that can oversee that and bring everyone back to base, I think it’s a good process.
Practice readiness for developing a patient feedback on safety intervention was also influenced by the perceived value of participating in the study, at both the microsystem and organization level. Perceived value at an organization level included using study participation as evidence of obtaining patient feedback data for external accreditation requirements and generally improving service delivery (i.e., workforce focus on QI). At a microsystem level, participants perceived that the project had value in the potential to improve the safety of patient care through identification of process inefficiencies and potential risks encountered within their respective roles (i.e., capability for improvement and motivation for change). Furthermore, most participants valued patient feedback obtained either through formal (e.g., written survey) or informal mechanisms (e.g., opportunistic conversations). However, some participants were reluctant to accept some patient feedback they perceived as irrelevant or inaccurate.
Although all six practices exhibited readiness through a commitment to the uptake of the intervention at the commencement of the study, the capacity to implement all intervention components varied. Capacity was the ability for practices to implement planned interventions and was determined by factors across the organization (e.g., supportive management and general practitioner [GP] lead, adequate staffing), external environment (e.g., university support), and microsystem level (e.g., protected time for study participation, unplanned leave, and staff resignation). Barriers at the organization and microsystem level impeded the ability for participants to implement all components of the intervention. For example, Practice A experienced staffing issues, including unplanned leave and staff turnover during the intervention phase, which impacted their intervention fidelity.
The provision of support to practices from the external environment (including financial reimbursement for travel and time in addition to workshop facilitation) by the research team served as an enabler for practice capacity to participate in the study. Although all practices valued patient safety, QI external support was identified as a driver for practice capacity and a necessary component for implementing a patient feedback on safety intervention: . . . external support is good because it makes you do the tasks. Whereas we all get bogged back down in our everyday tasks which are quite huge. So, I think some degree of external contact and support probably would keep a lot of the projects going.
An additional form of external support was the facilitation of face-to-face workshops for all practices. This served as an opportunity for participants to network and share their knowledge. Workshops and APMs enabled a cross-pollination of potential solutions (e.g., how to streamline administrative data) between participants, practices, and researchers. Workshops also served as a platform for participants to discuss challenges relating to capacity to implement interventions and various other barriers experienced.
Utilizing problem-solving skills
Through the intervention period, participants utilized various problem-solving skills and approaches to respond to patient feedback on safety, develop safety interventions, and to traverse system contextual variables. Practices able to successfully implement safety interventions demonstrated a collectively proactive approach to problem-solving during the intervention period. This generally involved identifying areas of negative feedback on the practice-specific PC PMOS feedback tool and developing a safety intervention based on this feedback. This differed from problem-solving skills used outside of the intervention (i.e., in everyday practice), which were more reactive in nature and responded to incidents that had taken place. The ability for participants to be proactive in their problem-solving, following the intervention, was dependent on other contextual variables affecting practices (e.g., staffing levels, competing clinical and administrative demands): We’re still at the stage where we’re having to be more reactive, rather than proactive, towards the issues, because of the bigger picture at the moment. Working towards the bigger picture is a proactive one. We know it’s going to be better, longer term. At the moment, we’re just trying to get through the days.
Utilizing the MFI QI methodology to develop a safety intervention, in response to results obtained from the PC PMOS tool, was a challenging task at the microsystem level. This was voiced by participants with and without prior QI experience. Participants without prior QI experience required additional external support from research facilitators during the early phases of the study (Workshop 1 and APMs) to develop a safety intervention. The process for developing a safety intervention goal, measures, ideas, and PDSA cycles, was generally undertaken as a collective exercise within each team and enabled participants to exchange and discuss their ideas. A combination of individual and collective PDSA conceptualization and comprehension was evident during the workshops, particularly when safety interventions were more dependent on specific individuals (e.g., administration leads). Conceptualizing what constituted a PDSA cycle and what measures of change were required, was regarded as problematic by participants, even by those with QI experience. External support was often requested by staff to assist with formulating a measure. However, those with QI experience were more able to work through the process for developing measures: I always found with those things the goal and the ideas are really easy, the measuring of the . . . the measuring is really hard, but I guess I can do . . . like I can go in and go, “Whoa, hang on,” you know, “In the previous 12 months how many health assessments did we do as opposed to in . . .” like, yeah. So, I guess I can measure that, it’s just having the time to go in and pick up that information and put it into something.
The need for critical thinking skills to be harnessed at the microsystem level was evident during workshops and APMs. This was necessary for safety interventions to be developed while factoring in responsiveness to other system contextual variables (e.g., staffing and administrative processes). Examples of these variables included both clinical and nonclinical competing priorities (e.g., involvement in other projects, recent clinical incidents, and new computer systems), structural changes (e.g., practice rebranding) and intra-practice cultural dynamics (e.g., relationship with GPs). To work through navigating system complexities, problem-solving in the context of developing safety interventions was mostly a collective process, involving an exchange of ideas and discussion before reaching consensus on the most appropriate course of action. Dialogue was generally inclusive of all participants within the team, allowing for a sharing of diverse perspectives and clinical backgrounds, which considered how safety interventions would impact the broader practice. It was observed during Workshop 2 that there was a general preference to use brainstorming methods to problem solve and work through PDSAs rather than other approaches, such as root cause analysis and process mapping.
The use of brainstorming methods reflected the need for participants to continually adapt and respond to changes within their respective practices. In some teams, this involved developing and evaluating PDSA cycles through an iterative process during the intervention period. For other participants, navigating system contextual variables (e.g., staff leave, computer system issue) prevented teams from completing a PDSA cycle, leading to partial implementation of safety interventions (Participants [PCPs] A and D): The initial idea was to have a nurse working side by side with [name of GP], to, you know, getting [to] his patients and do the paperwork, do the obs [sic.], all of that . . . so that [name of GP] wasn’t spending so long with the patients and getting out at seven o’clock at night. That fell down because the nurse went on long service leave [laughter] . . .
During the intervention period, successfully implemented safety interventions were developed using proactive approaches to problem-solving and responsiveness to both intervention complexities and system contextual variables by the practice team at the microsystem level. An example of this was extracting and analyzing practice data to proactively identify opportunities to optimize clinical appointments with GPs. Instituting protected time to continually address patient feedback on safety and develop further PDSA cycles was also identified as important and acted on by some practices. However, some practices found this particular variable challenging due to competing demands for time (e.g., clinical schedules, nonclinical priorities). Finding a mutually convenient time that suited all participants (particularly those who worked part-time) was also problematic.
A general preference to brainstorm collectively through informal conversations, rather than formally document safety interventions as required by the patient feedback on safety intervention, was communicated as a preferred mechanism of responding to system contextual variables and feedback on safety. Informal interactions included corridor conversations, texting outside of business hours, and writing notes in communication books. These informal approaches to communication as part of the problem-solving process were also employed in a reactive manner to patient safety incidents or other unexpected issues: . . . one of the other girls from the secretary, we probably collaborate a lot [sic.]. We throw ideas around. You know how to do different things. So, we’re probably the thinkers. We then have to go and say, “Okay this is what we thought, can we get clarification, can we do this?” Then if we get the green light or you know go back to the doctors to get their thoughts.
Impact of agency
In addition to practice readiness and the utilization of problem-solving skills, the degree of agency also impacted the implementation of safety interventions. Agency was understood to be a combination of both power and courage exhibited to develop and implement safety interventions. This was evident at the microsystem level (e.g., nurses, GPs, administration staff, and practice managers) and team level (collective agency). Activating agency at these levels was essential for the successful implementation of safety interventions. The ownership of safety interventions also interplayed with these levels of agency and was the degree to which individuals and the team felt they could implement all components of PDSA cycles addressing the safety intervention.
Although the teams collectively developed safety interventions, there were variations in team dynamics and interdependence of actors across the six practices throughout the implementation process. For three teams, a GP actively participated in developing safety interventions but was more distal to the implementation process. For the remaining three practices, GP participation was more distal in the entire process and involved general support or approval of the safety intervention. Therefore, GP involvement in the collective development of the safety intervention and iterative problem-solving processes was not necessarily essential for successful implementation of a safety intervention addressing patient feedback. It was understood that GPs played more of a supportive role in the development and implementation of safety interventions.
With GPs playing a more passive role, leadership of implementing safety interventions was shared among the roles of nurses, practice managers, and administration staff. Participants with QI experience were not always the drivers of implementing intervention components (PCPs C, F, and D). Participants with the relevant skills and expertise pertinent to the context of the safety intervention, along with an intrinsic motivation to enact change, exhibited leadership in implementing the intervention. For example, a participant who was an administration staff member without QI experience demonstrated leadership in implementing a safety intervention that involved modifying administrative processes to mitigate system inefficiencies. It was observed that the intervention directly affected this participant’s administrative role and had benefits in reducing individual workload (rewards); therefore, the participant had a vested interest in taking QI leadership. Similarly, interventions pertinent to a managerial level were overseen by practice managers, whereas clinical interventions were led by practice nurses. Characteristics identified by participants that were inherent to QI leaders within their teams, in addition to QI experience, were the ability to be open, transparent, and create space for dialogue around patient safety issues with other participants: I think it’s [name of PM]’s leadership. Because she’s fairly out there, she’s fairly loud, and she doesn’t mind being loud, and her leadership as well as her management is excellent.
As part of creating a space to elicit dialogue, QI leaders were also generally effective in distributing power among other participants within their respective teams. Power was relational and dependent on the established relationships between participants and rapport built during the intervention period. Although power did shift throughout the intervention period as those with lesser QI experience grew more confident in their skills and knowledge, leadership was generally maintained by the QI leader identified at the commencement of the study. It was observed in one team, where there were unequal power dynamics, that PDSA cycles were not fully implemented as they were dependent on one participant driving change, rather than the team as a whole. This had implications for other participants within the team, particularly when the change driver left the practice.
Successful intervention ownership by participants and teams was also enabled by an organization supportive of autonomy at the microsystem level. Autonomy, in this context, was the ability for participants to freely take action while operating within the rules and regulations of their respective practice and role. Advantages of autonomy described by participants included the ability to freely implement changes, evaluate the impacts of these changes, and adapt in action.
Although autonomous, some teams experienced difficulty in engaging the wider practice in the implementation and sustainability of safety interventions. Some teams had become a sub-practice culture through the course of the intervention period, whereas others had successfully recruited new participants to partake in the study between workshops and in the post-intervention period. Even participants new to the practice QI team had difficulty engaging the broader practice in the implementation of safety interventions at times. For example, a safety intervention developed by PCP C was implemented by a participant who was an administrative lead and was also new to QI. It was found that the participant had very little support from the broader administration team during the intervention period. Despite this, engaging other staff members from the practice was considered important to improving patient safety and identifying new patient safety goals.
Discussion
A process of theorizing is imperative to explaining for whom, how, and why new and complex health interventions may or may not work (Dixon-Woods et al., 2011). Inherent to this is the prospective examination of existing theories in light of findings from qualitative process evaluations, with the purpose of generating new theoretical insights (Bowen et al., 2009; Kislov, 2019; Langley, 1999; Oakley et al., 2006). Developing theoretical frameworks specific to interventions through the process of theorizing is also valuable to ascertaining the scalability and generalizability of new interventions (Kislov, 2019). The main finding of this study is a theoretical framework, identifying factors mediating with the implementation of a novel patient feedback on safety intervention in the primary care setting, developed through a theorizing process. Existing theoretical frameworks for understanding the processes underpinning safety and quality interventions in health services were extended in the context of inquiry to inform the development of this theoretical framework. To the authors’ knowledge, there has been no such attempt to make sense of the multifaceted complexities mediating the implementation of patient safety interventions in the primary care setting through a theorizing process. There are, however, theoretical frameworks that present factors that mediate with the implementation of QI interventions in the health care setting.
One such framework, which informed the initial process of sensemaking from large volumes of longitudinal qualitative data, was the MUSIQ framework (Kaplan et al., 2012). This framework guided an analysis of the complexities around implementing an intervention using QI methods (Calman et al., 2013; Davidoff, 2019; Kaplan et al., 2012). The hypothesis offered by the MUSIQ framework indicated that the success of QI interventions is directly influenced by the microsystem and QI team factors (Kaplan et al., 2012). The framework highlighted the multifaceted complexities informing practice readiness at different levels and the relationships between these. Specifically, these included having a shared practice safety and QI philosophy, the importance of QI maturity at an organizational level, and the influence of external organizational support (Hespe et al., 2018; Kaplan et al., 2012; Weiner, 2009). A shared practice safety and QI philosophy, concerning the importance of patient safety, was an enabler for the initial uptake of a patient feedback on safety intervention by primary care practices. As identified in other research, understanding the values, beliefs, and attitudes of primary care practices about patient safety is an important step to ascertaining the readiness of practices to implement changes addressing patient safety (Lawati et al., 2018). Findings also supported that practices with high QI maturity, which had the necessary infrastructure, resources, organizational support, QI leadership, and team expertise, were better equipped to engage in a patient safety intervention using QI methods, compared with those with low QI maturity (Singer et al., 2015). The provision of external support and mentoring to practices with low QI maturity, to facilitate the implementation of a patient feedback on safety intervention using QI methods, was an important consideration for broader adoption. This has also been a recommendation of other QI research, including research focusing on patient safety based in the hospital setting (Hespe et al., 2018; O’Hara et al., 2016) and other QI research undertaken in the primary care setting (Parker et al., 2007). It is difficult to ascertain from this study how the intervention would be sustained without external support, which is an area for future research.
Although the MUSIQ framework enabled examination of factors shaping practice readiness, the framework offered little insight as to how participants navigated the complexities of the intervention and responded to contextual system variables. These included practice cultural factors that are well reported in the literature, such as having a part-time workforce, and fragmented communication processes (Grant et al., 2014). This is also the limitation of other conceptual frameworks (e.g., InQuIRe), which seek to provide guidance in measuring the impact of factors, such as teamwork, when evaluating QI research in the primary care setting (Brennan et al., 2012, 2013). The use of these measures provided limited theoretical insight into the complexities underpinning problem-solving and decision-making processes used by practices when implementing new interventions, such as the patient feedback on safety intervention (Braithwaite et al., 2017).
Utilizing a lens of positive deviance during analysis offered insights that have not been captured by other theoretical frameworks (Lawton et al., 2014). A positive deviance approach has been utilized in other research examining safe care practices on medical wards and has produced useful findings indicating where health service leaders should invest resources in, rather than identifying areas of practice that are failing (Baxter et al., 2019). In health care research, more broadly, it is well established that change is dependent on clinicians and, more often than not, clinicians generally do things well (Braithwaite, 2018). Therefore, a lens of positive deviance guided analysis toward examining the problem-solving skills utilized by practice teams to successfully develop and implement safety interventions during the implementation period (Lawton et al., 2014). Those teams able to fully implement safety interventions were proactive in utilizing a range of skills (e.g., analyzing practice data) and approaches to navigating the complexities of the intervention (e.g., collective brainstorming). By doing so, participants also highlighted shortfalls of more linear approaches to problem-solving (e.g., PDSA cycles; Braithwaite et al., 2017). These skills were best demonstrated when participants were required to develop a change measure for their safety intervention as part of PDSA cycles; a key challenge identified in other patient safety research (Lawton et al., 2017). In addition, open communication, a documented preferred mode of communication in practices, was an identified contributing factor to the successful implementation of safety interventions (Grant et al., 2014). Examples included informal opportunistic conversations in the corridor and text messaging after business hours. Practices that were able to exercise more coherent lines of communication, through regular meetings and focused dialogue, were better positioned to implement interventions compared with teams which exhibited more fragmented communication (Grant et al., 2014). This understanding of how exemplar practices approached problem-solving is valuable to informing future adaptations of the patient feedback on safety intervention for broader translation into clinical practice. It is recommended that future interventions be aligned with the problem-solving processes utilized by primary care practices for successful implementation.
When examining these approaches to problem-solving, it was clear that there were participants, within each practice, who were the drivers of change. This required a shift in analysis to critically examine practices by considering constructs from institutional theory (e.g., practice subcultures), to understand the relationship between practice teams, participants, and the process of developing and implementing safety interventions (Grant et al., 2014). Such an examination enabled a more thorough analysis of the cultural and contextual nuances shaping practices and team dynamics (Grant et al., 2014; Lockett et al., 2012). Although there was a general understanding that practices were operating within a CAS, and that individual agents, the interconnectivity of teams, and contextual factors mediated how teams operated (Braithwaite et al., 2017), application of the IHI Psychology of Change Framework enabled a richer analysis of how individual agents navigated the complexities of the intervention and systems by enacting change (Hilton & Anderson, 2018). These change agents, or “institutional entrepreneurs,” were identified as participants or “actors” who demonstrated the ability to navigate the complexities of their practice or system, including the broader policy environment, and could implement changes (Lockett et al., 2012).
The findings from this study indicated that any person working in a practice (e.g., nurse or administration person) with a more egalitarian than hierarchical structure can implement and have ownership over a patient safety intervention if they have sufficient agency to enact change (Grant et al., 2014). This deviates from more traditional paradigms of QI interventions in the primary care setting, and practice structure more broadly, which identify GPs or practice managers as the leaders and drivers of change (Grant et al., 2014; Hespe et al., 2018). This resonates with other studies examining the constructs of institutional theory, which identifies that institutional entrepreneurs in health care systems, who have low or intermediate structural legitimacy (SL) or position of influence within an organization, are most likely to conceptualize and enact change within their institution (Lockett et al., 2012). This research was compared with persons who exhibit a higher level of SL and who are least likely to implement change as they are more likely to benefit from current institutional structures and processes (Lockett et al., 2012). Ideally, change agents should have enough SL to have power to change systems and sufficient normative legitimacy (NL) or ability to influence others, to have agency to implement change (Lockett et al., 2012). Other theorists have conceptualized this relationship of power and agency, using constructs from motivation theory and social cognitive theory, identifying that persons who value change and exhibit change efficacy are more likely to implement change (e.g., change valence; Weiner, 2009). The findings from this study support the potential agency of persons holding intermediate SL within practices, such as practice managers, senior nurses, and administration leads. The challenge going forward is how to facilitate agency in other staff members working in primary care practices, which is an area for future research (O’Hara et al., 2016).
One such approach to theorizing factors mediating with the implementation of a patient feedback on safety intervention implemented in the primary care setting is described in this study. Findings are useful for informing the translation of this patient feedback on safety intervention into policy and practice. As practices were purposively sampled to have had some QI and/or research experience, these findings may be limited in their transferability to other practices that have no QI or research experience. As members of the participating practices self-nominated to participate in the study, there may be a bias toward individuals who are part of a practice subculture that is more motivated to implement patient safety interventions and/or QI interventions (Grant et al., 2014). Although every effort was made to triangulate data sources, including overt observations and interviews, there is potential for some complexities within each practice (e.g., team dynamics and aspects of workplace culture) to have been overlooked. This includes insights to which the researchers, as outsiders, were not privy. Such phenomena would be best examined through an emic lens and extended time in the field, using ethnographic methodology (Reeves et al., 2014). This approach has been used in other research examining complex interventions within the primary care setting (Bunce et al., 2014; Russell et al., 2012). This would have also enabled the patient safety intervention to be evaluated using theories that examine factors mediating the ability for complex interventions to be embedded into health care systems over time (e.g., normalization process theory; Murray et al., 2010). It is also acknowledged that there are limitations to developing theoretical frameworks through an abductive process of extending existing theories in the light of new process data. Although there has been support for this type of inquiry for some time (Kislov, 2019), it is acknowledged that other theoretical approaches and qualitative methodologies could have been employed.
Conclusion
This study extended the use of existing theories in the context of inquiry and developed a theoretical framework identifying factors mediating with the implementation of a novel patient feedback on safety intervention implemented in the primary care setting. Although there are limitations around the generalizability of explanatory theories of interventions, the findings would be useful to researchers, primary care practices, decision makers, and QI leads seeking to implement new interventions in the primary care setting. Findings provide a starting point for mobilizing practices to become proactive in prospectively capturing patient feedback on safety interventions and building agents of change to advocate for responding to patient feedback. Additional research will need to explore ways of implementing the intervention into policy and practice without the external support of a research institution and in practices with low QI maturity. Understanding the complexities mediating with the implementation of safety interventions is essential to informing the future of patient safety in the primary care setting.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323211028829 – Supplemental material for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting
Supplemental material, sj-pdf-1-qhr-10.1177_10497323211028829 for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting by Hannah Beks, Andrea L. Hernan, Sally Giles, Mary Malakellis, Kevin P. Mc Namara and Vincent L. Versace in Qualitative Health Research
Supplemental Material
sj-pdf-2-qhr-10.1177_10497323211028829 – Supplemental material for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting
Supplemental material, sj-pdf-2-qhr-10.1177_10497323211028829 for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting by Hannah Beks, Andrea L. Hernan, Sally Giles, Mary Malakellis, Kevin P. Mc Namara and Vincent L. Versace in Qualitative Health Research
Supplemental Material
sj-pdf-3-qhr-10.1177_10497323211028829 – Supplemental material for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting
Supplemental material, sj-pdf-3-qhr-10.1177_10497323211028829 for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting by Hannah Beks, Andrea L. Hernan, Sally Giles, Mary Malakellis, Kevin P. Mc Namara and Vincent L. Versace in Qualitative Health Research
Supplemental Material
sj-pdf-4-qhr-10.1177_10497323211028829 – Supplemental material for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting
Supplemental material, sj-pdf-4-qhr-10.1177_10497323211028829 for Theorizing Factors Mediating With the Implementation of a Patient Feedback on Safety Intervention Implemented in the Primary Care Setting by Hannah Beks, Andrea L. Hernan, Sally Giles, Mary Malakellis, Kevin P. Mc Namara and Vincent L. Versace in Qualitative Health Research
Footnotes
Acknowledgements
The authors acknowledge the participants from the six primary care practices and thank them for their time and contributions to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A grant was received from the Western Alliance Academic Health Science Centre to fund the feasibility trial of the Primary Care Patient Measure of Safety (PC PMOS) tool.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.