
Abstract
Autistic adults have higher health needs compared to most, yet they continue to experience barriers to accessing appropriate healthcare. Presently, no qualitative research exists exploring these barriers which impact overall physical and mental health. We conducted a qualitative analysis in Victoria (Australia) of the perceived experiences of healthcare access for autistic adults (n = 9) and primary caregivers of autistic adults (n = 7). Specifically, a three-staged phenomenological approach was applied involving: (i) a communicative checklist, (ii) a health status survey and (iii) face-to-face interviews. Elements such as support, responsibilities and protective factors exhibited by caregivers, may impact healthcare access for autistic adults. Results indicate the need for further research exploring interdependent factors that impact healthcare access by caregivers, so evidence-based interventions can be developed to support caregivers in the future.
Whilst autistic adults represent only 0.8% of the Australian population, this data should be viewed with caution as this is rapidly increasing (Hand et al., 2019). Approximately 205,200 people had a diagnosis of autism spectrum in Australia in 2018, an increase of 25% over 3 years, compared with 164,000 in 2015 (Australian Bureau of Statistics (ABS) (2018). Previously, many people received their diagnosis prior to the age of 18, however, with refined diagnostic criteria, increasingly people are diagnosed after the age of 18 (Huang et al., 2020; Leedham et al., 2020; Tan, 2018). Many autistic adults experience worse health in comparison to the general population and therefore access to appropriate healthcare for this group is even more critical (Croen et al., 2015; Fortuna et al., 2016; Hwang et al., 2019). This study aims to explore perceived health, communication difficulties and healthcare access experiences of autistic adults and primary caregivers.
Compared to the general population, autistic adults experience a higher prevalence of co-occurring conditions such as seizure disorders (11.9% compared to 0.73%), hypertension (25.6% vs. 15.6%) and allergies (Croen et al., 2015). Research also suggests that mental health conditions are also more commonly experienced amongst this population. Conditions such as anxiety, bipolar disorder, depression and schizophrenic disorder are all more prevalent amongst this group (Baldwin & Costley, 2016; Croen et al., 2015; Fortuna et al., 2016; Hofvander et al., 2009; Mattys et al., 2018).
Even less is known about the impact of caregiver support access or barriers to healthcare (Brewer, 2018). The healthcare system in Australia is complex and the autistic community experience multiple barriers in accessing appropriate support (Raymaker et al., 2016). These barriers include communication difficulties, limited specialized knowledge and a lack of support from health clinicians (Mason et al., 2019; Nicolaidis et al., 2015). Behaviours of concern such as aggression, property destruction, disruptive and self-injurious behaviour have been frequently reported among autistic people (Fitzpatrick et al., 2016; Kats et al., 2013; Smith & Matson, 2010). Thus, further impacting the ability to access appropriate healthcare.
Preventative care and screening are important, even more so in a vulnerable population, who experience poor levels of health and multiple barriers accessing appropriate care (Croen et al., 2015; Fortuna et al., 2016; Hwang et al., 2019). Healthcare screening for health conditions such as cervical cancer, for example, is far lower for autistic adults than in the general population (Nicolaidis et al., 2013; Zerbo et al., 2018). This suggests that the health needs of autistic adults are not being met. The cause for this may be due to the poor access to relevant and/or appropriate healthcare services (Murphy et al., 2016). Primary caregivers have expressed their concerns in caring for an autistic person and evidence highlights many caregivers experience stress and anxiety due to the complexity of autism (Adib et al., 2019; Brewer, 2018; DePape & Lindsay, 2015; Nicholas et al., 2015; Parker & Killian, 2020; Robinson & Weiss, 2020; Sun et al., 2013). Dependent on the autistic person’s needs, undertakings such as routine check-ups, further investigations and applying for funding all whilst managing the rest of other family member’s needs, can negatively impact caregivers’ wellbeing and in turn further impact their level of care (Brewer, 2018; Parker & Killian, 2020).
As research suggests, further exploration into this area of health is critically required as whilst much is known about the barriers of healthcare delivery for autistic adults, it is evident that this group of people do not have good health outcomes nor appropriate healthcare access (Dern & Sappok, 2016; Nicolaidis & Raymaker, 2014; Nicolaidis et al., 2013).
Methodology
When it comes to developing interventions and/or improving the management and treatment of clinical problems, autistic people and their families have firsthand expertise. Their voices and perspectives matter. During the development of the study, grounded theory was explored as a possible methodology that could be used. But upon consideration, this study expected to understand the outside world and the impacting factors of healthcare access by and through human consciousness rather than generating theories from the emerging patterns (Neubauer eta l, 2019). Therefore, a phenomenological approach best suited this study to ensure the findings could be valued and used within healthcare settings and future evidence-based interventions (van Wijngaarden et al., 2017). Gathering data from autistic adults and their primary caregivers increased the credibility of the study, as it provided different ways of looking at the phenomenon of healthcare access (Al-Busaidi, 2008; Lindsay, 2019; Starks & Brown Trinidad, 2007). By incorporating semi-structured descriptive interviews, the method of semi-structured interviewing was employed to hear the voices of the participants (Supplemental File) (Bevan, 2014). The step-by-step process informed by literature guided the application of phenomenology in this study (Howard et al., 2019; Smith et al., 2009). This is presented in (Supplemental Table).
Methods
Study Description
This is a qualitative study guided by a phenomenological methodology. Semi-structured interviews were completed, a perceived health status survey and a communication checklist was employed to screen the overall current perception of health from the autistic adults’ point of view (Creswell & Poth, 2016).
Study Sample and Technique
Data were collected from a sample of autistic adults (n = 9) and primary caregivers/close family members (n = 7) from 2019 to 2020. The phenomenon of interest was healthcare for autistic adults and caregivers who frequently provide support for autistic adults when accessing healthcare (Brewer, 2018). Our sample primarily represented a group of people without intellectual disability (n = 8) but continued to require caregiver support. For this reason, including caregivers was vital to this study as each layer of individualized challenges increases the limitations when accessing appropriate healthcare (Green et al., 2018).
Autistic adults and primary caregivers were included in this study if they (1) were aged 18 years or older, (2) they lived in Melbourne Australia and (3) have a diagnosis of autism. Autism diagnoses were classified using the Diagnostic Statistical Manuel (fifth edition: DSM-5) (American Psychiatric Association (APA), 2013).
Sixteen participants were included in the study using a convenience sample. The participants were recruited via two Australian autistic organizations, paper advertisements in centrally located areas (such as local health services and libraries) and through social media. We decided against recruiting only through a health service as this would have biased the sample because certain people would have been seeking treatment.
Data Collection Methods
Semi-structured interviews
Semi-structured interviews allowed for a more open dialogue with the participants, which allowed them to discuss health-related issues that they may have experienced or other life changes that have impacted their access to healthcare, without a direct question needing to be asked (McIntosh & Morse, 2015). The interdependent factors relating to health and healthcare were guided by participant responses. However, due to the intersection of disability and healthcare, some questions asked in the semi-structured interviews were not directly related to accessing care (Singh & Bunyak, 2019). The Model of Health Disparities and Disability (MHDD) helped guide and develop the semi-structured interview questions, as the framework conceptualizes how the mismatch between personal and environmental factors can reduce healthcare access and quality, and in turn impact community participation (Meade et al., 2015). Interviews ranged in length from 20 minutes to 2 hours and 10 minutes. The descriptors – Communication Checklist – Adult (CC-A) and the Short form-36 (SF-36)
Identifying strengths and weaknesses in communication was important to understand, as past and current research has demonstrated that there are communication translation barriers between healthcare providers and autistic people (Nicolaidis et al., 2015). The Communication Checklist – Adult (CC-A) validated and provided information on how the participants in this study communicate and was then was compared to general census data. The CC-A is a tool that measures communicative weaknesses and strengths within populations (Whitehouse et al., 2010). The 70-item questionnaire was completed either by the participant or by a respondent who had regular contact (3–4 days per week) with the individual. Scaled scores of seven or above indicated that the person is unlikely to have communicative disorder and those with two or more composite scaled scores of six or less suggested that the person has communication difficulties (Whitehouse & Bishop, 2009). Data were scored and stored in SPSS (IBM SPSS Statistics, 2020).
The Short Form-36 (SF-36) (Ware & Sherbourne, 1992) was used to measure perceived health of autistic participants. The SF-36 is a standardized health assessment and is used amongst multiple populations, including the autistic population, to describe current physical and mental wellbeing (Asztély et al., 2019; Ezzat et al., 2017; Li et al., 2018)).
The SF-36 is a self-report tool which includes a set of generic, coherent and easily administered questions based on health status, to evaluate individuals’ perceived health outcomes (Ware & Sherbourne, 1992). The higher the percentage score identified a more favourable health state (Ware & Sherbourne, 1992). The tool has been widely used for autistic people to collect health-related quality of life measures (Lee et al., 2009; van Heijst & Geurts, 2014). Data were scored and stored in SPSS (IBM SPSS Statistics, 2020).
Analytical strategy of the qualitative data
Crafted stories provided glimpses of phenomena and by using in-depth analysis techniques, hidden narratives were uncovered (Crowther et al., 2017). Analysing the lived experiences of participants via an interpretive phenomenological research approach was therefore applicable (Howard et al., 2019; Matua & Van Der Wal, 2015). Highlighting the single cases and examining the individual perspectives within their own unique concepts was important during the coding of the data to share participant’s own story (Pietkiewicz & Smith, 2014; Smith, 2017). The qualitative data were thematically analysed and coded by the whole research team to highlight the developing themes and essential aspects within the data (Braun & Clarke, 2019). Interrater reliability was employed throughout the data analysis phase.
The use of reflexivity was used to understand the social position, personal experience, political and/or any professional beliefs the researchers may have had when conducting the face-to-face interviews and/or during the data analysis (Berger, 2015). By using reflexivity, the researcher did not use any leading questions based on previous participant’s responses (Howard et al., 2019; Pietkiewicz & Smith, 2014; Smith, 2017). This study was approved by Swinburne University of Technology ethics committee (Ethics ID: 2018/354). All participants received information on this study and signed consent forms before the collection of data.
Results
Demographic Data – Autistic Adults
The demographic information, CC-A and SF-36 results for autistic adults is provided in Supplemental Table (Supplemental Table). The male to female ratio was 5:4, the mean age was 25.5 and the age range was between 18 and 37 years old. Whilst only one participant had a diagnosed intellectual disability, other co-conditions were recorded within the group such as Attention Deficit Hyperactivity Disorder (ADHD), Post-Traumatic Stress Disorder (PTSD), Depression, Anxiety Disorder and Scoliosis. Noted within our study, one participant was married, one participant had children, two participants were studying at the time and four participants were in paid employment. Seven of the nine participants presented with low scaled scores overall (a scaled score of six or below), suggesting that most have a communicative disorder and six displayed overall communicative difficulties. Few participants (2 of 9) indicated a lack of engagement (scaled score of six or under for social engagement with seven or above for language structure). One participant showed a higher scaled score in language structure and social engagement (a scaled score of seven or more on language structure but lower in pragmatic skills) but a lower scaled score in pragmatic skills.
One participant scored almost 100% for all the categories for the SF-36 but on average, most participants did not experience physical functioning issues/conditions and did not have limitations due to physical health. Five participants experienced emotional limitations and poorer energy/fatigue levels. All except two participants had exceptional functioning, yet most participants felt that they experienced an increase in their overall health change over the past year. This included their overall physical and emotional performance and participation levels. When linking the data from the CC-A and SF-36, three participants presented with a communicative disorder, but mainly self-rated their health to be good to very good.
Demographic Data – Caregivers
Of the seven primary caregivers that participated in the study, the male to female ratio was 1:6. The caregivers in this study represented most of the autistic adults who also participated in this study (n = 5). Two participants identified as paid caregivers and five participants identified as family members.
Results
Thematic Analysis
Autistic adults and caregivers supporting autistic adults reported barriers to healthcare. This was irrespective of low or high physical functioning and/or their communicative strengths and weaknesses. The four themes included (1) overall health needs, (2) being ignored and disempowered, (3) autonomy and future planning and (4) the caregiver perspective. Figure 1 presents a thematic model based on the impact of qualitative responses from participants. Thematic model based on the impact of qualitative responses.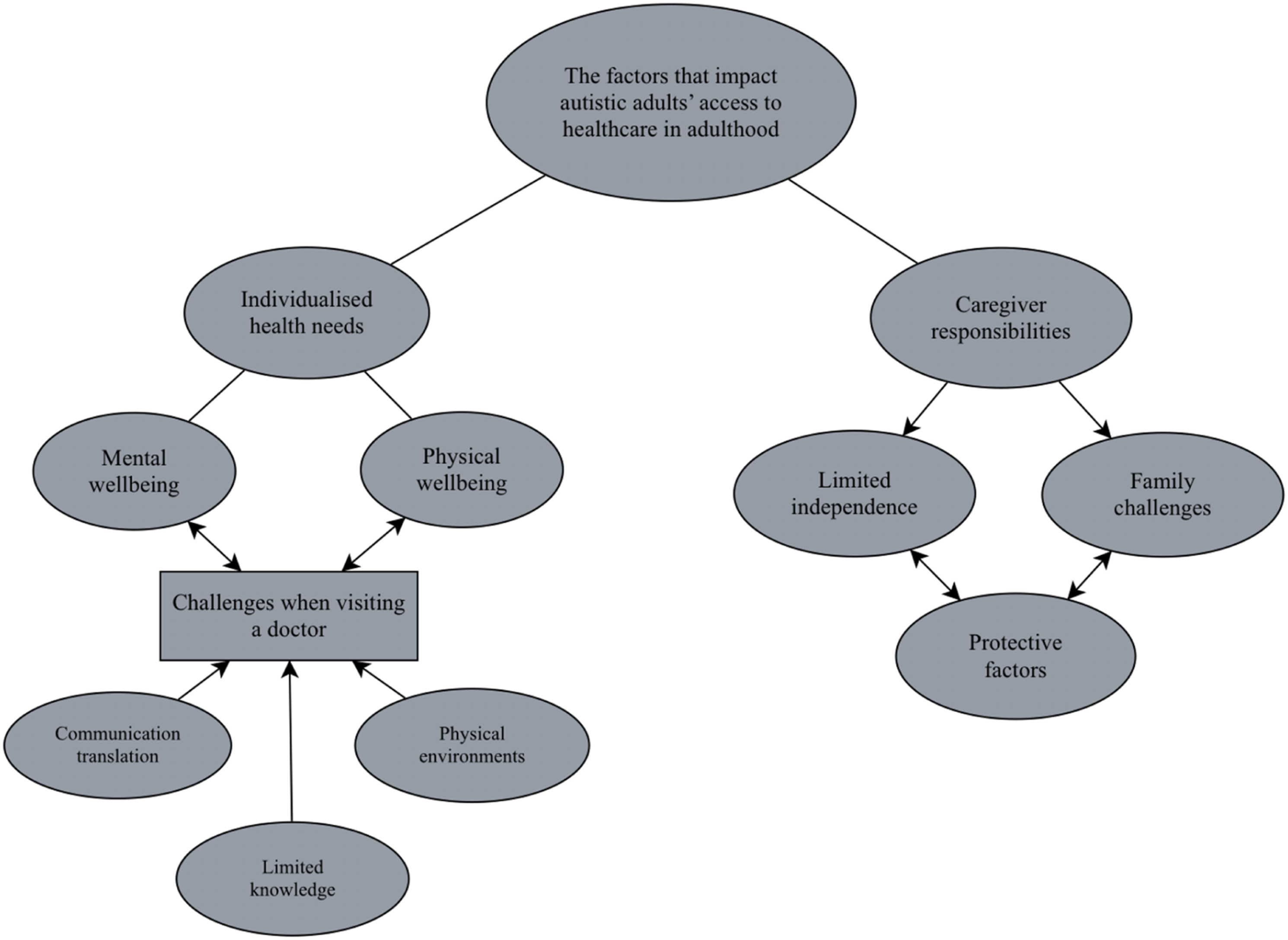
Overall Health Needs
Understanding health and health needs was of importance for autistic adults. Addressing mental health concerns, physical wellbeing, sexual health needs and visiting a general practitioner were amongst the main points discussed.
Mental and physical wellbeing
Many autistic participants described how their need for support varied over time, but mental health was a priority throughout all the interviews, but they did not have access to this. Seeing health practitioners for other conditions such as stomach issues, routine vaccinations, lung collapses, diet control, allergies and sexual health, was expressed throughout. One of the main concerns of caregivers was the dental health of autistic adults. Behaviours of concern were discussed and were linked to the fear of dentists and the physical pain that would be felt through the experience.
Sexual health
Some primary caregivers expressed that sexual health was a priority and an area that they want increased support and access to appropriate services and information. As explained by one caregiver they wanted support for their son to be informed and be able to discuss sexual health with a trained health professional: “My son is 22 years old and an adult now. I want somebody to be able to discuss with him about his sexual health. I don’t know if he has sexual desires or not. It would be good for him to have a service that he can talk to, where he feels comfortable. But I am not aware of these services.”
A caregiver expressed the process of discussing sexual health and relationships with those they supported as being confronting, ‘she doesn’t like talking about her body’. It was noted that by understanding and explaining what a sexual health appointment would entail for the autistic adult that this would be beneficial because they lacked appropriate health literacy on this topic. This was further shown when a caregiver also expressed concerns that ‘she wouldn’t go to the gynecologist, (as) nobody explained what the gynecologist would do’.
Visiting a general practitioner
The needs and concerns to visit a general practitioner were discussed frequently. Some caregivers mentioned general practitioner support was not required at this current time, whilst others noted they only sought further support for vaccinations and further investigations were not performed. This lack of accessibility to general practitioners was highlighted by an autistic adult who stated: “I only go to see the local general practitioner for something simple, for example, a medical certificate. Or vaccinations. I have another general practitioner, who is more specialized and understands the condition, my psychologist is incredible too, but was hard to find. I have seen many practitioners in the past and I was tired of repeating my story every time.”
This lack of access to medical care leading to the perception of poor health; both mental and physical and was identified as an overarching theme. Even with these perceived poor health beliefs autistic adult participants are very concerned with their own health but lack the communication skills required to convey or express these concerns to others.
Being ignored and disempowered
Even though most participants in this study could verbalize or communicate their needs, they did not feel that their voices were heard by healthcare practitioners. An autistic adult described this by saying that they ‘have bad experiences in hospital, because when I say I have had enough, it means I have had enough’ and that ‘the doctors talk (to my mum) as if I am not there’. In this theme, the communication barriers and the impacts of physical environments are discussed by autistic adults and caregivers.
Communication barriers
Many participants expressed they were made to feel that it is always a struggle to receive and access appropriate healthcare or diagnosis. An example of this was explained by a caregiver who stated, ‘I didn’t get any assistance for my children because they were diagnosed later in life’. The communication between the person and provider was of concern with participants feeling that the health professional had little knowledge about autism. A participant when seeking a diagnosis was told by a general practitioner, ‘I don’t think you’re autistic because you’re self-aware’ (Autistic Adult). This perceived lack of knowledge and communication participants believed led to misdiagnosis and poor support. Additionally, explanations were not provided when seeking medical help, ‘the general practitioner I use to see, sent me to a dietician and just told me I was fat. That’s basically it’ (Autistic Adult). Again, from this quote we can ascertain that participants felt like they were being stereotyped which led to them not receiving appropriate services.
The needs of the autistic participants were not always communicated by them and instead were expressed solely by caregivers. This was expressed in frustration by one autistic adult who when going to a general practitioner stated, ‘I go, and they [GP] ignore me, and they talk to my mum’. Additionally, the questions that were being asked by the health professional were sometimes not clear ‘when asked questions they expect people to answer the exact question. I never understood what I should or shouldn’t be saying’ (Autistic Adult). This led an autistic adult to feel they were being dismissed, ‘I know nursing can be hard, I just felt that they weren’t very sympathetic or empathetic, and it made it hard for me when I was experiencing a lot of pain and they were dismissive’. Primary caregivers showed concerns in this area regarding communication between themselves and healthcare workers and were made to feel unable to have full involvement in health decisions with regards to the autistic adult they were supporting.
The physical environment
The physical environment can relate to physical touch and/or sound and light leading to further sensitivities for some autistic people. For some study participants, recognizing the environment as a factor was important, as unfamiliar environments can cause people to feel ‘frantic’ (Caregiver), because the person may be sensitive to the light, sound or movement within the area. It was noted, however, that ‘health professionals may perceive an autistic person to be anxious due to other reasons, but it may just be due to the smell and noise’ (Caregiver). The hospital environment can also be of concern for autistic people as past experiences may cause one to feel ‘afraid’ (Caregiver). Ending up in hospital isolation when they did not need to be, was a concern for one participant as this had happened before and lead them to have a ‘horrible experience’ (Autistic Adult). This was discussed in the following passage by an autistic adult: “My first lung collapse was when I was 19 or 20. Then I had a few more after that year…The nurses were dismissive…. They weren’t very sympathetic or empathetic and that made it hard for me when I was experiencing a lot of pain.”
Being ignored can impact the need and motivation of seeking healthcare in future circumstances and not having a voice can further impact and lead to a feeling of mistrust. The barriers discussed within this theme highlighted how and why autistic adults may not seek further support and healthcare in the future when needed. Autistic adults expressed their desire to participate in their own health and wellbeing and could see this as the basis for future life goals.
Autonomy and Future Planning
The word ‘independence’ was mentioned by many autistic participants throughout the interviews and the want and need for autonomy and independence led to further discussions around short and long-term goals. A fundamental point made about independence was made by all participants and emphasized by an autistic adult: “Moving out of home is my long-term goal. I want to be close to work and stop playing basketball, focus on housework.”
This independence to control one’s life was helped by support from others. The importance of feeling a part of a community and being employed was a priority for most autistic adults with caregivers supporting this ideal. One caregiver expressed that: “It would be good to have something that could help him with long-term meaningful employment. An employer that knows what autism is and where he can have a long-term employment would be good. Now he just applies for jobs and goes for job interviews, even if he gets work, it is only for a couple of days. Sometimes they politely ask him to go, sometimes they are rude to him and ask him to go away after calling him lazy, or careless.”
The participants could see that priorities such as independent living and employment, helped them to maintain overall health and mental wellbeing.
The Caregiver Perspective
Physical support was identified to be required by most caregivers and was apparent through many ways including support for physical hygiene, cooking, financial support and National Disability Insurance Scheme (NDIS) planning and guidance. Describing care needs was highlighted by a caregiver: “I take care of all tasks, we take care of his daily needs, we shop with him, he cannot financially support himself, although he is high functioning, he cannot care for himself.”
In addition to the physical support, it was found that emotional support was also frequently needed, ‘Emotionally he struggles to cope with a lot of things. He is not stable at times. Sometimes he gets into a shell and won’t speak and share’ (Caregiver). For another autistic adult participant, going into the community can be challenging, ‘sometimes I can’t go to the shops if my girlfriend doesn’t come, I find it difficult to leave the house if I am low-energy’. Caregivers felt they are the biggest support and many autistic adults may ask or seek emotional support from their caregivers, ‘if the task is stressful, then I need mum to talk me down’ (Autistic Adult). Additionally, encouragement was needed to participate in community settings, ‘I need encouragement to get out and do it, I am not confident being out and doing stuff on my own’ (Autistic Adult). Yet, providing emotional support can be challenging for carers and was at times apparent that it took an emotional toll on caregivers, ‘he is a lot to handle. I mean, he doesn’t listen to everyone, he plays up and he knows that too’ (Caregiver). It was noted, however, that emotional support was dependent on individual needs.
Carer responsibilities
Findings highlighted that carers responsibilities involved a multitude of different aspects with safety being of concern. As one caregiver stated: “If I have said no, you’re not going for a bike ride, he says I will go by myself I am a man and then he is gone. I say go to the gym, because it’s in the garage, but then he is gone. And I just panic the whole time.”
In addition to safety, there were several medical responsibilities that are placed on carers as well that was frequently mentioned. This was highlighted by one caregiver who explained ‘he is not able to decide. He will never be able to see the doctor by himself. He never recognizes the need. All his health issues, I look after his health’. Medical advocacy was also a responsibility of the carer within the health care system as highlighted by one caregiver who stated, ‘a lot of the nurses did not listen to me when I explained the same thing, I said, explain to her what you’re going to do, when and how’.
One caregiver expressed that it was their responsibility and requirement to complete their own research to find organizations that may help with specific health needs in the future, ‘I’ve done my own research and came across… [an autism specific organization] and other specialists too, but I really want to see and know about more clinicians that can support him with socializing, because he is very lonely’.
The responsibilities for carers left some feeling that it impacts the family unit. This tension was perfectly articulated by a caregiver who stated ‘we don’t agree with everything as a family, it was best for our son for my husband and I to stay together. You stick at it. Now we are more patient with each other’. The constant stress of the future and who will provide sufficient support was of concern for the caregiver and their families. This was mentioned by one caregiver stating:
“I just think if I am not here to support him in the future, how will he access or communicate. I just don’t know. He doesn’t tell people. I can make a medical appointment for him and observe him, but what happens when parents aren’t here.”
Protective behaviours
The need to provide ongoing care and the responsibilities of keeping the autistic person safe and the family unit together, was present through protective factors. One caregiver was aware that the person they were supporting did not have access to healthcare, but their child was in denial and refused to accept help. An autistic adult described their current health status and said they were healthy, and their carer agreed, saying, ‘he does not need to go to the GP’ (Caregiver). In turn potential health issues were of concern; however, caregivers did not seek further investigations and further tests were not of a priority. Additionally, other protective factors such as safety were of concern and discussed by a caregiver: “He can use public transport for familiar places, but I don’t feel it is safe to let him do it by himself. He can go by transport himself. But I don’t let him. I will go with him. Usually I call his phone, he doesn’t answer all the time. So, when it is time is to come home, I call him many times, sometimes up to 10 times.”
Throughout the study, safety and keeping the person in their care healthy was of great concern and an ongoing stress for many caregivers.
Discussion
Since research has suggested that communication difficulties can negatively impact overall healthcare access/healthcare delivery for this population, exploring the communication difficulties using a standardized measure was essential to understand if communication was the major barrier or if other factors can negatively impact healthcare access for autistic adults (Nicolaidis et al., 2015). The CC-A may be useful for clinicians to understand the communication limitations of their individual clients as it increased the understanding of the autistic participants in our study and we compared the outcomes with the Australian autistic population. The autistic sample for this study compromised of people under 37 years old and therefore did not obtain data from a wide range of autistic people over their lifespan; however, previous research shows similar barriers for ageing autistic adults (Patra, 2016).
When comparing our sample with the general autistic sample in Australia, according to the Australian Institute of Health and Welfare (AIHW), the data collected presents similar results (ABS, 2018). However, it is important to note that our data only presents a snapshot of autistic people at a point in time. Moderate-profound communicative limitations were compared between AIHW and our sample and were found to be similar, 62% compared to 55% (ABS, 2018). Self-care for participants showed moderate to profound limitations (45.2% compared to 44%). In our study, three autistic participants also relied on their partner’s support for social and mental wellbeing (ABS, 2018). Struggling to identify autism is of concern and as presented by Zerbo et al. (2015), some healthcare physicians were not aware that their patients had ASD. Similarly, Hull et al. (2017) and Perry et al. (2020) discussed how camouflaging autistic traits is a common technique used for coping in social situations. This may impact the diagnostic process, ultimately limiting overall healthcare (Hull et al., 2017). Many of our autistic participants presented with low scaled scores in the communicative checklist (CC-A). This was suggestive that many autistic adults in our sample have a communicative disorder and display overall communicative difficulties, which may impact communication translation. The limited health literacy from health professionals was of concern within our sample, for both autistic adults and caregivers. Limited knowledge and a poor understanding of autism is a reported barrier in literature (Nicolaidis et al., 2015). When comparing the results, both studies found that with limited knowledge about autism and poor communication, further challenges may arise. Communicative difficulties may lead to misinterpretations between the patient and the provider, leading to further difficulties in understanding how the autistic person is feeling (Nicolaidis et al., 2015). This can impact on autistic adults lives as communicating for their individualized needs may cause further challenges in accessing appropriate healthcare. Leading back to feeling ignored, disempowered and the stigma relating to these experiences. Further education at a tertiary level, within hospitals and primary care should be considered for healthcare professionals in the future, as when impacting factors increase, health needs are unlikely to be met. Additionally, assumptions are made by healthcare providers when behaviours of concern are visibly present, but it is not often realized that changes in behaviour can be significant indicators of healthcare problems. Healthcare clinicians need to listen to their patients and enhance the autonomy of autistic adults by directly asking them questions about their health needs. Health professionals across all domains need to begin to understand and identify these impacting factors, so that autistic people feel comfortable in accessing care in the first instance (Goldschmidt, 2017). Autistic adults were shown to care about their own health, but interdependent themes may contribute to the barriers in accessing appropriate healthcare. Interestingly, participants perceived their physical health in the SF-36 as good to better than good. These findings in the SF-36, did not equate to their overall health needs during the interviews. This is an important finding, when developing future research projects to ensure the validity and reliability of results are accurate. It is important to note that some interviews were conducted with a caregiver in the room and this may have influenced participant responses, however, this was a requirement of the ethical application. The sample in this study was small, however, similar characteristics such as communicative limitations, self-care limitations and caregiver support responsibilities presented with similar data compared to the autistic population in Australia (ABS, 2018). Recent literature suggests many caregivers experience stress and anxiety due to the complexity of autism and supporting an autistic person (Adib et al., 2019; Parker & Killian, 2020; Robinson & Weiss, 2020). Caregiver responsibilities were an interdependent theme that was explored within our study (DePape & Lindsay, 2015). Primary caregivers described how their carer responsibilities can impact other day-to-day factors, such as the stresses of keeping the family together as one unit and how these difficulties can lead to further stresses in life like who will provide sufficient support for their autistic child if they cannot (Brewer, 2018; Myers et al., 2009). The primary caregivers’ protective factors may ultimately impact the independence and autonomy of autistic adults (Hume et al., 2009) and therefore, may impact healthcare access for the autistic population. However, it is important to note that autistic adults do have the right to care for their own health and manage their own healthcare. Participants have shown and discussed various protective factors that can impact healthcare access and these experiences may impact independence and autonomy when autistic adults’ attempt to advocate for themselves. Much of the sample comprised of family members acting as primary caregivers, opposite to paid carers. The findings from primary caregivers may be different, if there was an equal sample of paid or unpaid carers. Future mixed method research is needed to explore the potential barriers and enablers of healthcare access impacted by primary caregivers and what types of support is required for primary caregivers to enhance autonomy and independence for the autistic person they support. This may in turn improve healthcare access for autistic adults. New standardized checklists/surveys could be developed to measure a primary caregivers’ level of support and highlight any areas of concern to better support autistic adults and ensure the person they are supporting receives appropriate healthcare. Since the results of the SF-36 did not equal the health perceptions and health status needs during interviews, research is required to explore what causes health changes over time for autistic adults. Whether of a positive or negative nature, understanding if health has changed due to specific interventions, access to healthcare or significant life events will be of importance when exploring this area. Regarding the reliability of the SF-36 results, a validation study could be employed to measure and recognize what method would be preferred and recognized as a reliable form of data collection. Given that the overall health of autistic adults is less than the general population, it is critical that healthcare services and clinicians continue to review, adapt and improve services for the autistic population.
Conclusion
The health of autistic adults is important to consider, as this enables us to design and understand healthcare access to improve services to meet their healthcare needs. Employment was an essential aspect and priority for many participants, yet their overall health can impact potential employment opportunities and day-to-day activities. Previous research suggests that healthcare access barriers are primarily due to communication, the limited knowledge of autism and healthcare clinicians’ perspectives of the condition, often leading to misinterpretation. Findings suggest that there may be other impacting barriers such as responsibilities, support and protective factors exhibited by primary caregivers affecting the overall healthcare access of autistic adults. This study recommends further research to explore perspectives of caregivers and develop interventions to better support caregivers of autistic adults. As autistic adults continue to experience poor levels of health and access to healthcare, this study was developed and intended for researchers to advance evidence-based interventions for this group and for healthcare professionals to incorporate changes, to address the challenges experienced by autistic adults to improve their services and increase accessibility.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323211050362 – Supplemental material for Barriers to Accessing Healthcare: Perspectives from Autistic Adults and Carers
Supplemental material, sj-pdf-1-qhr-10.1177_10497323211050362 for Barriers to Accessing Healthcare: Perspectives from Autistic Adults and Carers by Shenae Calleja, Jonathan Kingsley, Fakir M Amirul Islam and Rachael McDonald in Qualitative Health Research
Supplemental Material
sj-pdf-2-qhr-10.1177_10497323211050362 – Supplemental material for Barriers to Accessing Healthcare: Perspectives from Autistic Adults and Carers
Supplemental material, sj-pdf-2-qhr-10.1177_10497323211050362 for Barriers to Accessing Healthcare: Perspectives from Autistic Adults and Carers by Shenae Calleja, Jonathan Kingsley, Fakir M Amirul Islam and Rachael McDonald in Qualitative Health Research
Footnotes
Acknowledgments
We are very grateful and would like to thank the participants who contributed to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by an Australian Government Research Training Program Scholarship.
Supplementary Material
Supplementary material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.