
Abstract
Persistent human papillomavirus (HPV) infections can cause cancer (e.g., cervical/vaginal/penile/anal/oropharyngeal). The HPV vaccine prevents cancer, yet U.S. vaccination rates remain low. We explored sociopolitical factors in the adoption of Puerto Rico’s HPV vaccine school-entry requirement. Multiple streams framework explains how the intersection of problems, policy, and politics streams influence policy adoption. Policy entrepreneurs work on joining these streams. Interviews (n = 20) were conducted with stakeholders (e.g., physicians/researchers/nonprofit organizations’ leaders). Data were analyzed using applied thematic analysis. High incidence of HPV and HPV-related cancers in Puerto Rico were indicators of problems. Focusing events included Rhaiza’s case and the HPV-Advisory Panel Report. During summer 2017, a policy window opened; the Department of Health (DOH) adopted the requirement in summer 2018. Stakeholders discussed policy initiatives. Political turnover positively influenced the process. Policy entrepreneurs created an extended period of intersection resulting in the adoption of the requirement. Findings can inform policy initiatives to improve HPV vaccination rates and reduce HPV-related cancers.
Keywords
Persistent infection with high-risk types (e.g., 16 and 18) of the human papillomavirus (HPV), the most common sexually transmitted infection in the United States (Satterwhite et al., 2013), can cause cancers such as cervical, vulvar, vaginal, penile, anal, and oropharyngeal (Forman et al., 2012), while infection with low-risk types, HPV 6 and 11, can cause anogenital warts (Garland et al., 2009). Currently, the HPV vaccine is recommended as a primary prevention strategy targeted for adolescents 11 to 12 years old, due to a better immune response occurring before children become sexually active (Centers for Disease and Control Prevention [CDC], 2019). Despite research demonstrating the safety and effectiveness of the HPV vaccine (Petrosky et al., 2015), HPV vaccination rates among adolescents remain far below the Healthy People 2020 goal of 80% completion among adolescents aged 13 to 15 years old (U.S. Department of Health and Human Services, 2015). As data from 2019 show, only 54.2% of adolescents aged 13 to 17 years had completed the HPV vaccination series in the United States (Elam-Evans et al., 2020).
School entrance immunization requirements are a recommended evidence-based strategy to increase vaccination rates (Averhoff et al., 2004; Guide to Community Preventive Services, 2019). However, HPV vaccine mandates have encountered resistance in part due to the intersection between vaccine safety, parental rights, and adolescent sexuality (Barraza et al., 2016; Colgrove et al., 2010). Currently, in the United States, there is variability in HPV vaccine policies; some states have created legislation in favor of educational campaigns, while others require health insurance to cover the HPV vaccine (Abiola et al., 2013; Keim-Malpass et al., 2017; Laugesen et al., 2014). Only Virginia (Pitts & Tufts, 2013), Rhode Island, Washington DC (Barraza et al., 2016; Hoss et al., 2019), Hawaii (State of Hawaii Department of Health, 2020), and Puerto Rico (Departamento de Salud, n.d.) have adopted an HPV vaccine school-entry requirement. Lack of widespread adoption of the HPV vaccine school-entry requirement has led to a public health need to understand the contextual factors impacting the adoption of this policy (Keim-Malpass et al., 2017). Therefore, the purpose of this study was to understand the sociopolitical factors that influenced the adoption of the HPV vaccine school-entry requirement in Puerto Rico.
Methods
Theoretical Framework
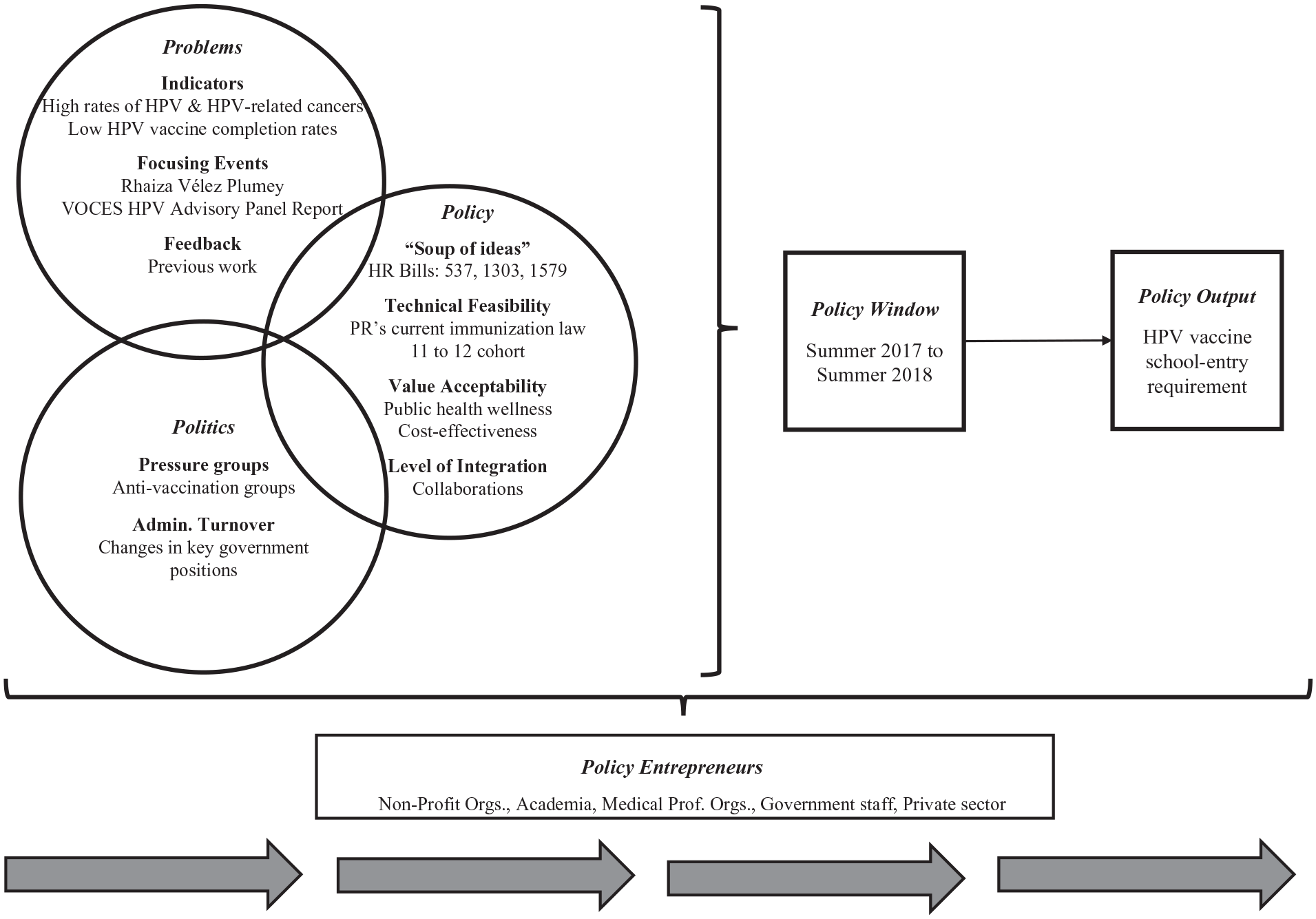
Multiple streams framework (MSF) considers macro-level factors and the process by which a policy is adopted. The MSF posits that the problems, policy, and politics streams will converge, influenced by the policy entrepreneurs, to create a window of opportunity resulting in a policy output (Kingdon, 1995; Zahariadis, 2007, 2014).
The problem stream is composed of the concerns and conditions that policymakers and citizens believe need to be resolved (Zahariadis, 2007). Policymakers become aware of these concerns through the following factors: (a) indicators or data that describe the problem, (b) focusing events—events that call attention to the problems and are usually pointed out by the media or policy entrepreneurs, (c) feedback from previous experiences, and (d) load or the number of problems the policymaker needs to attend to (Zahariadis, 2007, 2014). The policy stream includes the “primeval soup” of ideas or all the potential solutions presented by the experts. Not all ideas will receive consideration by the policymakers (Kingdon, 1995; Zahariadis, 2014). Thus, MSF posits that there are criteria that guide the policymakers’ selection process (Zahariadis, 2007, 2014). These criteria include technical feasibility, value acceptability, and the level of integration. If a solution seems challenging to implement, does not align with the values of the policymaker, or seems too costly, it has a lesser chance of approval (Zahariadis, 2007, 2014).
The politics stream refers to the broader political context and includes the pressure-group campaigns, the national mood, and the administrative or legislative turnover (Zahariadis, 2007). The way groups of people think, the changes in members, positions, and political parties in power, and the influence some groups have over policymakers all impact the chance that an idea is set on the agenda (Zahariadis, 2007, 2014). The policy windows are moments in time when the three streams intersect. As Kingdon (1995) defines it “is an opportunity for advocates of proposals to push their pet solutions, or to push attention to their special problems” (p. 165). These moments tend to be short, and MSF assumes that the policy windows open one at a time (Zahariadis, 2007, 2014). These windows are critical because they provide context to the policymaking process. Finally, the policy entrepreneurs are the people and institutions who work on joining the three streams when the policy window opens (Kingdon, 1995). They are described as the manipulators of the policymakers, and those with the strategies, time, and resources to invest in their problem of interest (Zahariadis, 2007, 2014).
Thus, guided by the MSF, the research questions were (a) How did the problems, politics, and policy streams intersect to inform the adoption of the HPV vaccine school-entry requirement in Puerto Rico? and (b) Who were the policy entrepreneurs involved in the adoption process and what were their roles?
Study Overview
The study consisted of two sequential phases. Here we present Phase 1, which consisted of interviews with stakeholders from Puerto Rico. Phase 2 entailed a content analysis of newspapers from Puerto Rico (Vázquez-Otero, 2019). The study was approved by the University of South Florida—Institutional Review Board.
Research Setting and Context
Puerto Rico is an island in the Caribbean with an estimated population of 3,411,307 residents (United States Census Bureau, n.d.). In 2015, the Puerto Rican median household income was $18,626 with 58% of children living in poverty (Krogstad et al., 2017), and an unemployment rate estimated to be at 13% (Government Development Bank for Puerto Rico, 2016). Spanish is the most commonly spoken language on the island. The Governor, at the moment of the adoption of the HPV vaccine school-entry requirement, was from the “Partido Nuevo Progresista” (PNP) party, which advocates for Puerto Rico to become a state of the United States.
Puerto Rico’s Department of Health (DOH) administers the vaccination funds available from the Vaccines for Children program to vaccinate low-income groups 0 to 18 years old (Departamento de Salud, n.d.). The “Centros de Salud Primaria 330” (primary care clinics) provide vaccination services to uninsured or underinsured groups (VOCES, 2015). There are vaccination centers in hospitals that accept private health insurance. Also, but less common, there are providers, such as pediatricians, who provide these services (VOCES, 2015). Of note, Puerto Rico’s economic situation is like that of other low-income countries; however, Puerto Rico is not part of GAVI. Law 25 of 1983 is Puerto Rico’s current vaccination law. It authorizes the DOH Secretary to decide which vaccines will be required for school entrance. Opt-out mechanisms include a sworn declaration indicating religious reasons or certification indicating medical reasons. The DOH Secretary must announce the required vaccinations every year, 3 months before the beginning of classes (“Ley de Immunización,” 1983).
Among U.S. states and territories, Puerto Rico has one of the highest incidence rates of HPV-associated cancers (including anal, cervical, oropharyngeal, and rectal cancers), with a rate of 13.10 cases per 100,000 people (CDC, 2016). Moreover, Puerto Rico has the highest incidence rate of HPV-associated cervical cancer in the nation, with rates of 11.70 cases per 100,000 women (Viens et al., 2016). In 2016, initiation and completion rates of the HPV vaccine in Puerto Rico were reported to be 75.8% and 52.8%, respectively (Walker et al., 2017). In 2018, Puerto Rico adopted the HPV vaccine school-entry requirement.
It is important to note that on September 20, 2017, Hurricane María hit Puerto Rico as a category 4 storm with winds of 155 mph, moving across the island and producing catastrophic flooding (National Weather Service, 2017). Due to this atmospheric event, the island lost power/electricity and access to potable water causing significant damages to the health care system.
Participant recruitment and data collection
Purposive sampling was used to recruit participants identified from online sources (e.g., Puerto Rico’s DOH and newspaper websites), by consulting local experts (i.e., gatekeepers), and using the snowballing technique. Using these different strategies, the potential of recruiting participants from the same network was reduced (Hennink et al., 2011). Inclusion criteria included being of legal age and involved in Puerto Rico’s HPV vaccine school-entry requirement adoption process. Interviews were conducted in Spanish by a Puerto Rican native Spanish-speaker. Participants had the option of being interviewed in-person or by phone.
The interview guide consisted of open-ended questions adapted from an instrument used by Abiola et al. (2013) which was guided by MSF. The guide was translated into Spanish and shared with two local experts for feedback. The main topic areas included previous work (e.g., strategies or policies) related to the HPV vaccine, barriers and facilitators for the adoption of the requirement, and people in favor of and against the requirement. Interviews were conducted until meaning saturation was reached (Hennink et al., 2017); which was achieved when there were enough data to fully understand the codes and inform the constructs of MSF. The process to determine saturation was iterative, and considered thematic areas that needed more information and clarity, participant recruitment (e.g., considering the point during the snowballing process when participants recommended others who were already scheduled for an interview or had been interviewed, and following guidelines from Guest et al., 2006), and the breadth and depth of the data collected. Interviews were audio-recorded after obtaining informed consent from the participants. Participants were offered a $20 gift card for their time.
Data analysis
All interviews were transcribed. A codebook was developed using a priori codes that were based on the interview guide and MSF constructs, and emergent codes derived from the data. All data were imported to MaxQDA and were analyzed in Spanish. The primary researcher and a second coder, both proficient in Spanish and trained in qualitative data analysis, independently coded four interviews, and discussed issues that arose during the coding process. A final Kappa score of 0.89 was achieved. The remainder of the interview data (n = 16) were coded by one researcher (Vázquez-Otero). Data were analyzed using applied thematic analysis (Guest et al., 2012). During the data reduction phase, qualitative matrices were created by code. This facilitated the use of a cross-case comparison technique to identify patterns by comparing a code across all interviews (Guest et al., 2012; Hennink et al., 2011). Categorization of the data was done to create summaries. These summaries were linked back to the theoretical framework by conceptualizing the data at the abstract level (Hennink et al., 2011). Exemplary quotes were translated to English (Vázquez-Otero) and reviewed by a second Spanish speaker.
Results
Sample Description
Twenty interviews were completed between May and August 2018. Seven interviews were conducted in person and 13 over the phone. Interviews lasted an average of 46 minutes (range: 20:30–72:30 minutes). All participants were in favor of the HPV vaccine school-entry requirement. Participants were categorized into five groups based on how they identified their primary role: (a) “Non-profit,” e.g., leaders and members of nonprofit organizations (including coalitions) or public corporations, n = 5, (b) “Professional Organization” (e.g., leaders of professional medical and dental organizations, n = 3), (c) “Government” (e.g., DOH employees and policymakers, n = 5), (d) “Researchers” (members of academia, n = 4), and (e) “Other” (e.g., physicians, attorneys, pharma representatives, n = 3).
Overview
Stakeholders noted the high incidence of HPV and HPV-related cancers in Puerto Rico (e.g., cervical, oropharyngeal) as indicators of problems to be solved. Social factors such as the publishing of the VOCES HPV Advisory Panel Report and the case of Rhaiza Vélez Plumey, a Puerto Rican mother who died of cervical cancer in 2015, served as focusing events. During the summer of 2017, a policy window opened when the DOH announced that the HPV vaccine was going to be required for school entrance for fall 2018. The HPV vaccine school-entry requirement was adopted in the summer of 2018. Stakeholders discussed policy initiatives, such as changes to the immunization law. The political turnover in key government positions positively influenced the adoption process; however, pressure groups reacted by advocating against the requirement. Policy entrepreneurs from multiple sectors worked to get the HPV vaccine school-entry requirement adopted (Figure 1). These findings are discussed further below.
Problem Stream
Stakeholders talked about problems, including health-related indicators and focusing events (social conditions), which they thought served as catalysts to the adoption of the HPV vaccine school-entry requirement. Among the indicators, the most frequently mentioned were the high HPV-related cancer incidence and prevalence in the island’s population. Stakeholders noted the high rates of cervical cancer and the increasing rates of oropharyngeal cancer, as well as concerns regarding how common HPV is in Puerto Rico, as evidenced by studies conducted on the island. For example, a member of a professional organization stated, I think that the fact that cervical cancers have been dramatically increasing, and as a matter of fact, in the press conference that we did, the statistics about the increase in cervical cancer were shown. Also, we have not been able to decrease oral cancer, not because we are not decreasing smoking incidence, but because we have an increase of HPV related [oral cancers].
Participants noted that Puerto Rico had a relatively high HPV vaccine uptake (first dose) but mentioned the need to increase HPV vaccine completion rates, as another problem that needed to be solved. As depicted in the following quote, Puerto Rico has always had good coverage of the first dose; it is said to be 85%. Now, where it has declined is for the second and third doses, which fall under 50 [%], and now with it becoming a requirement, I suppose that percentage . . . we estimate it will go up too.—Professional Organization
Stakeholders mentioned two focusing events affecting the adoption of the HPV vaccine school-entry requirement, (a) the case of Rhaiza Vélez Plumey and (b) the publication of the VOCES HPV Advisory Panel Report (Report). Rhaiza took part in an interview, shared on social media, that narrated her cancer story, and made a call for all women to get screened for cervical cancer. A member of a nonprofit organization mentioned, “Rhaiza’s story helped us a lot too. For me, Rhaiza’s story was a complete turning point.”
VOCES, founded in 2013, is a nonprofit organization and coalition dedicated to the promotion of vaccines in Puerto Rico. Participants highlighted the importance of the Report, made possible by VOCES’s initiative, and noted how it was informed by a panel of experts. The Report stated the need for comprehensive HPV-related education for parents, providers, religious leaders, and the press. Additionally, the Report documented the need for increased HPV vaccination on the island due to the high prevalence of HPV and HPV-related cancers and provided recommendations for action, one of which included making the HPV vaccine a requirement for school entrance. As illustrated by the following quote, There was a unanimous consensus of all participants, that in Puerto Rico the use of the vaccine should be promoted and that, eventually, if we wanted to lower our virus incidence rates, we should also promote that it be one of the requirements for school admission—Other
Participants highlighted the work (i.e., policies and strategies) that was accomplished before the HPV vaccine could be required in 2018 and described how it served as feedback to the adoption (Table 1). These efforts to increase HPV vaccination rates date back to the years when the vaccine was first recommended by the Advisory Committee on Immunization Practices and Puerto Rico’s DOH included it on the vaccination schedule as a recommended vaccine.
Timeline of Policies and Strategies Leading to the HPV Vaccine School-Entry Requirement in PR.
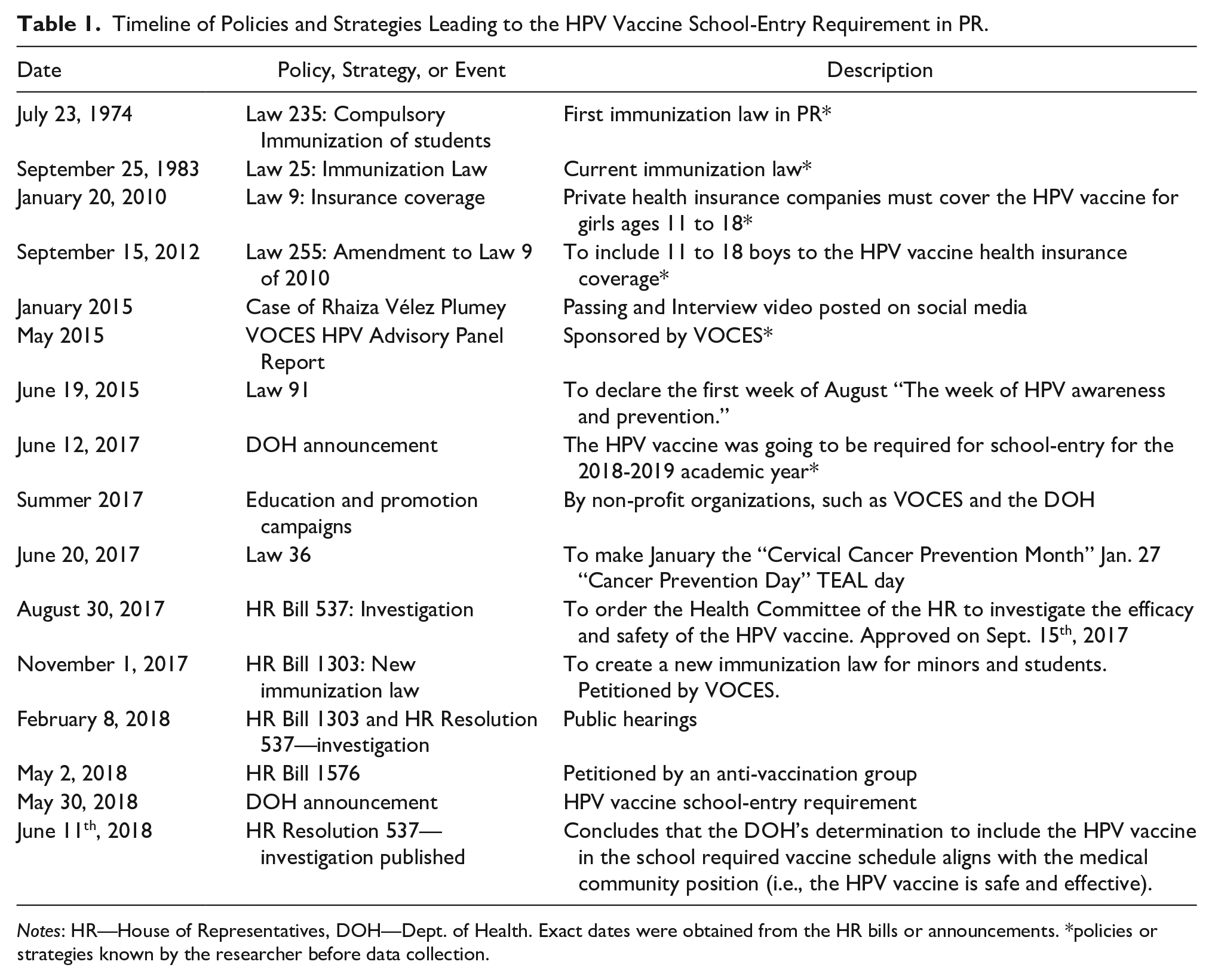
Notes: HR—House of Representatives, DOH—Dept. of Health. Exact dates were obtained from the HR bills or announcements. *policies or strategies known by the researcher before data collection.
Having limited access to the HPV vaccine, due to both availability and cost, was mentioned as a barrier to adoption. Therefore, previous work included the support of policies that made it mandatory for private insurance to cover the cost of the HPV vaccine for girls (2010) and boys (2012). As indicated by the participants, Vaccines for Children and the insurance provided by Puerto Rico’s government covered the vaccines for the public sector. Stakeholders also noted the importance of different policy strategies used to increase awareness and education efforts about cervical cancer (2016) and the HPV vaccine. They explained that these efforts seemed to have helped increase HPV vaccine rates in Puerto Rico. For instance, participants indicated that in 2018 the CDC awarded Puerto Rico’s DOH a recognition due to high adolescents’ overall vaccination and HPV-specific rates. As exemplified with this quote, In recent years, despite that the vaccine mandate was still not accomplished, the campaign promoting the vaccine, educating people and all professionals achieved significant increases in the vaccination rates against HPV in Puerto Rico.—Government
Policy Window
Stakeholders explained that the HPV vaccine school-entry requirement became official when the DOH secretary announced it in the summer of 2018, but a previous announcement was done in 2017. The purpose of the 2017 announcement was to provide an entire year for additional education and promotion of the HPV vaccine, and for parents to have time to begin the HPV vaccine series for their children. This timeframe was described as follows, In the past year [2017] a determination was made to make it [HPV vaccine] mandatory for this year [2018], to give a year of orientation to those that did not want to get vaccinated. [. . .] it was presented to the Secretary of Health, and the Secretary signed it now [2018].—Other
Policy Stream
After the DOH announcement during the summer of 2017, other policies that were part of the policy soup were considered by policymakers. The policies mentioned included the House of Representatives (HR) Bill 537 and HR Resolution 537, HR Bill 1303, and HR Bill 1576 (Table 1). The purpose of HR Bill 537, initiated by the policymakers, was to investigate the safety and efficacy of the HPV vaccine after concerns were raised by antivaccination groups. Public hearings were conducted in early 2018, and in June 2018 HR Resolution 537 concluded that the DOH’s determination to include the HPV vaccine on the school-required vaccine schedule aligned with the position of the medical community (i.e., HPV vaccine is safe and effective). Some stakeholders talked about HR Bill 1303, a project that was petitioned by VOCES and supported by the DOH, which intended to change the immunization law to make mandatory the use of the Puerto Rico Immunization Registry and continue to require that health insurance companies pay for vaccinations. Later, during the summer of 2018, as a reaction to the HPV vaccine school-entry requirement, antivaccination groups promoted Bill 1576. This bill proposed an amendment to the immunization law to add the philosophical exception to the available vaccination opt-out options.
The Puerto Rican immunization law authorizes the DOH Secretary to decide which vaccines should be added to the list of required vaccinations for school entrance. This authority was mentioned by the stakeholders as a facilitator for the adoption (technical feasibility). As a participant described, Law 25 in Puerto Rico, which is the Immunization law [. . .] established that the secretary of health is the one that has the responsibility to look out for public health in terms of preventable diseases. Law 25 gives that authority to the secretary.—Non-profit
Another aspect that made the HPV vaccine school-entry requirement technically feasible, was that it targeted 11- and 12-year-old adolescents. The stakeholders thought this was important for two reasons (a) the economic savings of only having to provide two doses, and (b) the better immune response children have to the HPV vaccine at these ages. The following quotes illustrate these reasons.
The current chosen age requirement for school-entry by the Department of Health is 11, 12 years of age. We know that the CDC extends it until 26 years, but it has been proven scientifically that the younger the person is, the higher the response [. . .] his/her immunological system that person will have.—Other In this case, what the administrative order is going to say is the cohort from 11 to 12, and an additional group will be added each year. We are going to ensure that those girls and boys receive just the two shots, which will represent an immediate economy in vaccine doses because if you wait until 14, then [he/she] will need three.— Non-profit
The HPV vaccine school-entry requirement aligned with the following stakeholders’ values (value acceptability): protection of the public’s health, reduction of the HPV-related cancer health disparities, and long-term economic savings due to the prevention of HPV-related cancers. As the following quotes demonstrate, It is still a public health issue because if you look historically, if you look at the data, cervical cancer and many of the HPV-related cancers tend to occur on patients from low socioeconomic positions.—Researcher With a study done by the Comprehensive Cancer Center, we showed that if Puerto Rico achieves the vaccination of 80% of the girls and 67% of the boys by 2020; we will have saved almost $88 million in diagnosis and subsequent cervical cancer treatments.—Non-profit
Stakeholders agreed that the adoption process of the requirement was successful due to the level of integration of different sectors, such as the government (including the DOH and the Department of Education), academia, and nonprofit organizations. These sectors collaborated to create a consistent message with a defined purpose, as this quote shows, “We had a clear objective and right now that is to reduce HPV related cancers through an 80% rate increase of immunization among adolescents for the HPV vaccine.”—Other.
Politics Stream
When the HPV vaccine school-entry requirement was announced by the DOH Secretary in the summer of 2017, pressure-groups, for the most part antivaccination groups, reacted and resisted the policy. These groups included an online religious group, a Catholic priest, a feminist organization, an autism organization, and a group of parents. From the participants’ perspectives, the views against the HPV vaccine school-entry requirement included concerns about the sexual transmission of the virus, worries related to the HPV vaccine (i.e., safety and side effects), the connection between religious values and the idea that children would become sexually active if they get the HPV vaccine, and concerns about the lack of education and information about the HPV vaccine. Despite the varied composition and views of these groups, all shared concerns toward making the HPV vaccine mandatory for school entrance. As illustrated with this quote, “Obviously, the main barrier is always the anti-vaccine movement which reacts and starts doing public policy around the hallways and making noise in the press and television, and provided parents with incorrect information regarding the supposed harms.”—Non-profit.
Stakeholders mentioned changes in key government positions (administrative turnover) as facilitators of the adoption of the HPV vaccine school-entry requirement. They mentioned how the current DOH Secretary made the HPV vaccine one of his priorities, and the importance of the person named to occupy the position of Sub-secretary of Health (i.e., a pediatrician strongly in favor of vaccinations). However, participants noted that if a new secretary is named, he or she could remove the HPV vaccine from the list of required vaccinations for school entrance. A member of a professional organization described this concern as, The legislative [process] is the most difficult, obviously, because you have all these religious and naturalistic groups that lobby strongly against, and that made it [the process] slower. It was done; it is not permanent, it does not have a lot of sustainability, but at least it solved the problem, and it helps that the DOH adopted it by creating awareness. The problem is that if the secretary of health changes, the next secretary does not need to do it [require the HPV vaccine]. We have to make this into a bill.
Policy Entrepreneurs
Participants described different societal sectors that contributed to the adoption process of the HPV vaccine school-entry requirement. These sectors were categorized into nonprofit organizations, medical professional organizations, academia, government staff, and the private sector. Each had a distinctive role based on their expertise. See Table 2 for exemplary quotes.
Composition of Policy Entrepreneurs’ Groups and Exemplary Quotes.
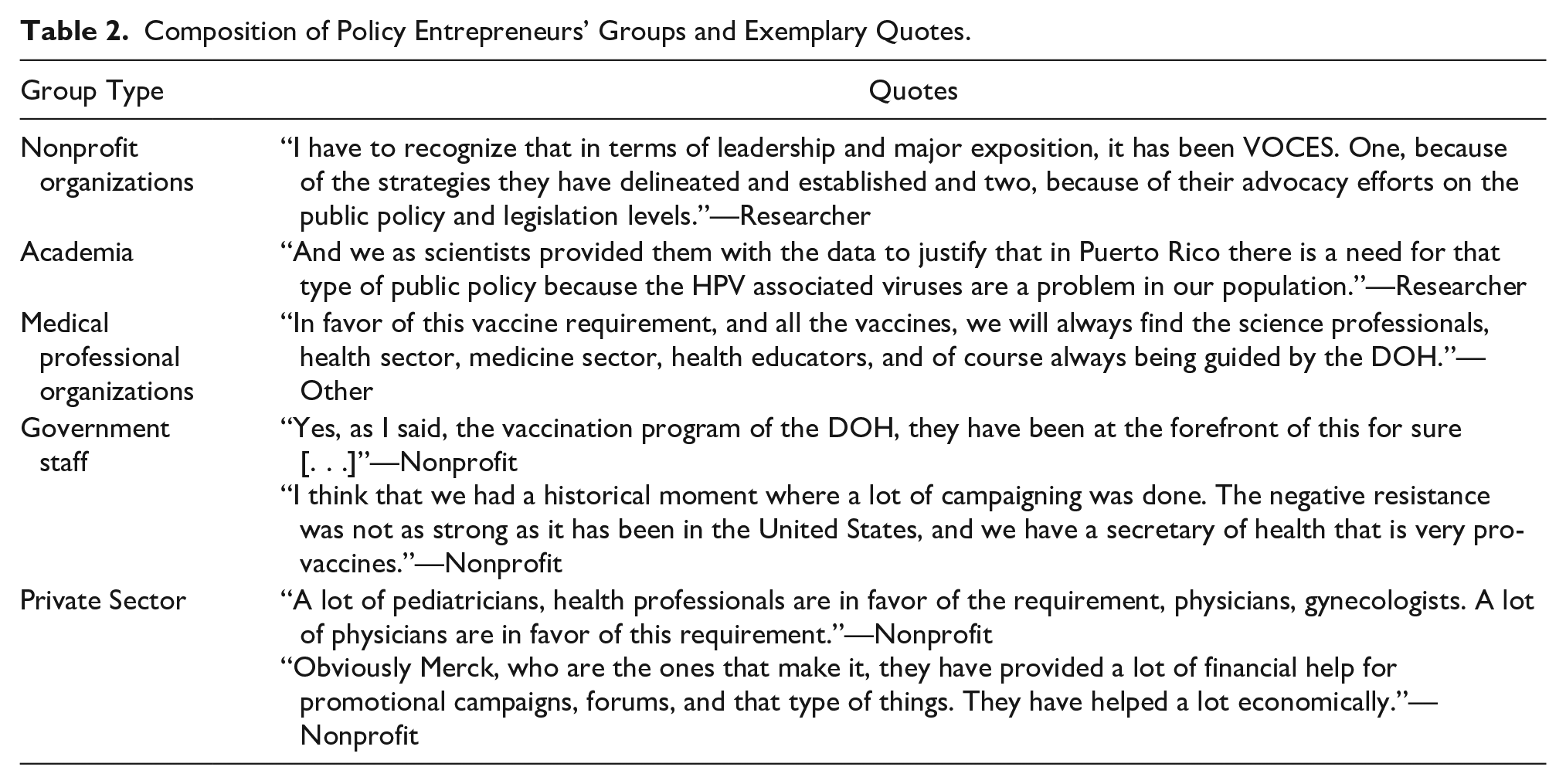
Participants agreed that VOCES was fundamental in the adoption of the HPV vaccine school-entry requirement. VOCES is a coalition that includes medical professional organizations, other cancer prevention coalitions, and members of the private sector. This coalition created awareness and provided education about HPV and HPV-related cancers. VOCES actively advocated for the HPV vaccine school-entry requirement. Other nonprofit organizations mentioned included the American Cancer Society, which mainly supported education, the Head and Neck Coalition, and the Puerto Rican Cancer Coalition. Another sector included the medical professional organizations that supported the requirement by providing education and advocating using their expertise. Medical professional organizations mentioned included the Puerto Rico’s Pediatricians Society, Academy, and ACOG chapter, as well as the Dentists Society. Members from academia included researchers from the University of Puerto Rico (UPR), the UPR Medical School and Public Health School, as well as Puerto Rico’s Comprehensive Cancer Center. They provided scientific evidence (e.g., data on the incidence and prevalence of HPV and HPV-related cancers) from studies conducted in Puerto Rico to the community, the DOH, and the Legislature.
The main actors in the government were the DOH secretary, the DOH subsecretary, and the vaccination program employees who facilitated the adoption process. From the stakeholders’ perspectives, the position of the DOH vaccination program was always on par with the current scientific guidelines. Finally, the private sector included organizations such as hospitals, pharmacies, physicians from private practice (e.g., a private group of gynecologists), and Merck, the vaccine manufacturer. This sector collaborated by providing information about the HPV vaccine and indicating their support for the HPV vaccine school-entry requirement. Merck primarily provided information about the HPV vaccine to key decision-makers, and funding, via grants, for organizations to develop educational materials.
An active role undertaken by some of the policy entrepreneurs was taking part in public policy advocacy. Members of nonprofit organizations, medical associations, and academia talked about their support for not only the requirement as a public health prevention strategy but also for policy changes that were needed to increase education and access to the HPV vaccine.
Aftermath of Hurricane María
Participants were asked if they thought that the passing of Hurricane María could affect the implementation of the HPV vaccine school-entry requirement. All agreed that hurricane María affected vaccine availability, and the operation of the vaccination clinics and private medical offices. However, most stakeholders did not anticipate any major barriers to HPV vaccine availability. Only a few stakeholders seemed unsure about the current situation of the health care/vaccination system but sounded optimistic about the implementation process.
Discussion
This study, guided by the MSF, examined the sociopolitical factors that influenced the adoption of the HPV vaccine school-entry requirement in Puerto Rico. During the summer of 2017, a window of opportunity opened; ultimately, the policy output was produced in the summer of 2018, when the DOH Secretary officially announced that the HPV vaccine was going to be required for school entrance (Figure 1). However, before the policy window opened, policy entrepreneurs worked on issues that needed to be addressed to clear the way for the adoption of the requirement. For instance, participants mentioned the policies that were put in place (e.g., health insurance coverage) and the education campaigns that took place in Puerto Rico years before the adoption of the requirement. These educational campaigns created awareness of the HPV, HPV-associated cancers, and the HPV vaccine as a cancer prevention tool. This finding is similar to research showing that the idea of preventing cancer was the primary driver for the decision to adopt such a policy (Abiola et al., 2013; Colgrove et al., 2010).
The policy entrepreneurs were instrumental in the adoption process of the HPV vaccine school-entry requirement in Puerto Rico. Their actions date to many years before, and continued even after, the policy window opened (Figure 1). Thus, despite the MSF’s assumption that each of the streams runs independently from one another and converge for short periods (Kingdon, 1995; Zahariadis, 2007), findings show how continuous, integrated, and purposely carried out efforts from the policy entrepreneurs created an extended period of intersection that resulted in the adoption of the HPV vaccine school-entry requirement (noted by the crossover of the circles overtime in Figure 1). Research has noted the key role of the policy entrepreneurs in the adoption of HPV vaccine policies. When studying the case of Virginia’s mandate, Abiola et al. (2013) found how Senator Janet Howell and Delegate Hamilton were the policy entrepreneurs who achieved consensus in the legislature and support from stakeholder organizations. In contrast, policy entrepreneurs in Puerto Rico were from a variety of sectors. For example, VOCES played an important role in unifying all the sectors to advocate for the HPV vaccine school-entry requirement with the scientific evidence needed to convince the secretary of health. Similarly, in the case of Washington DC’s mandate, the American Cancer Society provided a statement in support of the legislation (Barraza et al., 2016). Moreover, in international settings such as India, research shows how integrated political will, guided by community engagement, can enable the implementation of vaccine programs (Dutta, 2019).
Specific health factors, or indicators, contributed to the process of adoption of the HPV vaccine school-entry requirement. The high rates of HPV and related cancers, particularly cervical and oropharyngeal cancer, were among the problems that stakeholders thought needed to be resolved by the requirement. This finding is similar to Virginia’s HPV vaccine school-entry requirement, where concerns regarding cervical cancer were noted as a health issue by the proposed legislation passed in 2009 (Abiola et al., 2013). Additionally, stakeholders described the relatively high uptake of the HPV vaccination in Puerto Rico as a facilitator; however, the low completion rates were an indicator that was considered for the adoption of the requirement.
Two focusing events facilitated the adoption process of the HPV vaccine school-entry requirement in Puerto Rico: (a) the death of Rhaiza and (b) the publication of the VOCES HPV Advisory Panel Report, both occurring in 2015. From the participants’ perspectives, Rhaiza’s case was a catalyst that impacted the Puerto Rican population and brought awareness to the issue of cervical cancer and the HPV vaccine. Moreover, this case contributed to making people receptive to the HPV vaccine and facilitated the adoption of the policy when the window of opportunity opened. The report was meaningful because it included local epidemiological and cost-effectiveness data, and supported the requirement. Having these local data and the case of Rhaiza facilitated the adoption process by pointing to the relevance of the problem in Puerto Rico.
An important finding from this study is that stakeholders thought that Puerto Rico’s current immunization law, which authorizes the DOH Secretary to require vaccinations for school entrance, made it technically feasible to adopt the HPV vaccine school-entry requirement as a policy. This regulatory approach may have facilitated the HPV vaccine school-entry requirement adoption because convincing the members of the legislature, whose decisions are highly influenced by voters, can be difficult. This approach is similar to the case of Rhode Island, where the DOH also established the requirement via its rulemaking powers (Barraza et al., 2016; Washburn et al., 2016). On the other hand, both Virginia and Washington DC created mandates through the legislature (Barraza et al., 2016). Another aspect of technical feasibility was that the requirement only includes the 11 to 12 years old cohort. This meant that the government and public health system would only spend money on the cost of two vaccine doses, which is the number of shots required for the targeted cohort in alignment with current HPV vaccine recommendations (CDC, 2019). Moreover, findings support that there were value considerations regarding this policy approach. The values captured by the HPV vaccine school-entry requirement included the protection and overall wellness of the island’s population by preventing the physical, emotional, and economic implications of HPV-related cancers in the long term. In Virginia, for example, research with parents of girls noted how the requirement brought their attention to HPV as a public health concern (Pitts & Tufts, 2013).
From a political perspective, the anti-vaccination sector actively exerted pressure on the policymakers. These pressure groups posed a direct resistance to the adoption of the HPV vaccine school-entry requirement. Findings show how, in an attempt to weaken the reach of the HPV vaccine school-entry requirement, pressure groups petitioned Bill 1576 to include an opt-out option to the immunization law based on personal beliefs (the bill was not discussed during summer 2018). In other scenarios, such as in Virginia, the passing of an HPV vaccine mandate encountered less resistance; here, a quick passing of a bi-partisan bill did not provide enough time for an anti-bill campaign to form and be a barrier for the passing of the policy (Abiola et al., 2013). Similarly, members of the Rhode Island DOH noted minimal opposition to the addition of the HPV vaccine to the school entrance requirements in 2014 (Washburn et al., 2016). However, actions through the legislature have been taken to limit Rhode Island’s DOH powers related to its authority to establish vaccine requirements, particularly requirements related to diseases not contagious in the school setting (Barraza et al., 2016).
Finally, the political turn-over in key government positions facilitated the HPV vaccine school-entry requirement adoption process in Puerto Rico. In 2017, changes in the political party of Puerto Rico’s government led to new individuals occupying positions in the governor’s cabinet. However, political turn-over was also raised as a concern. Changes in political parties could mean that whoever is named to occupy the position of Secretary of Health may decide to remove the HPV vaccine from the list of required vaccinations. This is a limitation of the regulatory approach taken to create the HPV vaccine school-entry requirement in Puerto Rico.
The contextual political nuances are important to consider because they can impact the policy outcome as it happened in the cases of Texas, Indiana, New York, and California (Abiola et al. 2013). In Texas, Governor Rick Perry issued in 2007 an executive order to require the HPV vaccine for sixth-grade girls (Colgrove et al., 2010, Abiola et al. 2013). This action was followed by a strong backlash when donations from Merck to his campaign were made public (Mello et al., 2012). The Legislature overrode the order by arguing that the governor was “overreaching” his constitutional powers, and only approved the distribution of HPV vaccine information in schools (Abiola et al., 2013; Colgrove et al., 2010). Another failed attempt to require the HPV vaccine which ended with a similar outcome occurred in Indiana when, in 2007, Senate Bill 327 was introduced. Again, Merck’s influence, coupled with the conservative profile of the state, resulted in a difficult political landscape that was not receptive to the mandate (Abiola et al., 2013; Mello et al., 2012). Nevertheless, in 2014, Indiana passed House Bill 1464 which authorized pharmacists to administer the HPV vaccine (National Conference of State Legislatures, 2020). Other attempts include the states of New York and California where efforts to pass the HPV vaccine school-entry recruitment failed, and no alternative policy outcome was produced (Abiola et al., 2013).
As with any research study, limitations exist. Recall bias may impact the findings, especially participants’ narratives related to work done before summer 2018. However, the documents reviewed (Table 1) and findings from the content analysis (Phase 2) may have served to reduce this limitation via data triangulation (Vázquez-Otero, 2019). Also, the timing of the data collection process was opportune since it took place amid the HPV vaccine school-entry requirement adoption process in Puerto Rico.
Purposive sampling may limit the generalizability of the results. Data presented here are from the participants who supported the requirement. Thus, this study lacks an in-depth exploration of the HPV vaccine school-entry requirement adoption process from the perspective of the groups who were opposed (e.g., antivaccination). Particularly, when research has noted how some of these groups can influence views by spreading misinformation regarding the HPV vaccine (Dutta, 2019). Future research should explore the views of those opposed to the requirement to comprehensibly understand additional social factors that may affect the adoption process of this policy. Other viewpoints that should be explored include those of parents of adolescents, employees from the school system (including school nurses), members from the media, and religious leaders. Moreover, future research should look at the implementation process of the HPV vaccine school-entry requirement taking HPV vaccination outcomes for policy evaluation into consideration.
This study has theoretical implications. MSF assumes that each of the streams runs independent of each other and only converge at short times called windows of opportunity (Kingdon, 1995; Zahariadis, 2007). Nonetheless, in the case of the HPV vaccine school-entry requirement adoption process in Puerto Rico, it was difficult to evaluate the streams in isolation. The data showed that the streams were always in contact with one another. Furthermore, the policy entrepreneurs interacted with the streams at many points in time (Figure 1). Finally, the MSF is “adoption biased” meaning that it favors the evaluation of the policy creation and falls short in looking at the implementation phase (Blackman, 2005). However, this study focused on the creation/adoption process, and the use of MSF was valuable to guide the research questions, inform data analysis, and identify the sociopolitical factors influencing the process.
Implications
This study of Puerto Rico’s HPV vaccine school-entry requirement has public health implications for national and international settings. At the local level, the process that occurred in Puerto Rico (i.e., requirement adopted via the DOH), can serve as an example to states where legislative policymaking options may seem difficult. Moreover, the findings provide insight into the strategies and policies that may need to be in place before the adoption of an HPV vaccine school-entry requirement and serve to highlight the potential barriers that should be considered in national or international settings. Because multilevel and multimodal approaches are recommended to increase HPV vaccination rates (Zimet et al., 2020), public health practitioners and advocates of vaccination policies can use these findings to develop action plans for their communities (i.e., states or countries) to leverage resources, engage the media and the public, and create messages to influence the policymaking process. In sum, by creating awareness of the health issue, educating the population, and considering people in key government positions, the adoption of vaccination mandates can be facilitated. These lessons are useful as we consider requiring existing and future vaccinations, such as a vaccine against COVID-19.
Conclusion
The purpose of this study was to understand the sociopolitical factors that influenced the adoption of the HPV vaccine school-entry requirement in Puerto Rico. Despite the impact of a major hurricane and economic constraints, Puerto Rico was able to adopt this requirement. Policy entrepreneurs created an extended period of intersection that resulted in the adoption of the HPV vaccine school-entry requirement to prevent cancer. This study provides useful information about the adoption process of a population-based intervention that can increase HPV vaccination rates and reduce HPV-related cancers in the United States and internationally.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.M. Daley served on the U.S. HPV Vaccine Advisory Board of Merck Pharmaceuticals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the completion of this project came from the University of South Florida College of Public Health Student Honorary Awards for Research and Practice (‘SHARP’) Award and the University of South Florida Office of Graduate Studies Scholarships and Fellowships. Additionally, Dr. Vázquez-Otero’s time to write this paper was supported by the Cancer Prevention Fellowship from the National Cancer Institute and Harvard T.H. Chan School of Public Health – National Institutes of Health grant number 2T32CA057711-27. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.