
Abstract
Depression has been the subject of increased awareness and concern in Australia, but there has been little research into how depression is constructed on mental health websites, which have become a major resource for mental health information among the general public. In this study, critical discursive psychology was employed to analyse the informational content of eight major Australian mental health websites concerning depression. Four interpretative repertoires were identified – a biomedical, a self-optimization, a normal-natural and a societal-structural repertoire. The biomedical and self-optimization repertoires were the most prevalent, constructing depression as an illness within an individual occurring as a result of a biological or psychological deficit. Whilst previous studies have identified the predominance of a biomedical repertoire of depression on official websites, this study highlights the growing prominence of a self-optimization repertoire alongside the biomedical. Whilst it appeared that the aim of the websites was to challenge stigma and encourage help-seeking, it is argued that this way of understanding depression may have counter-productive effects in that the problem is located within the individual rather than with society, and individuals may be positioned as responsible for managing their own mental health, under the guidance of experts. The implications of understanding depression in this way, and not in alternative ways, are discussed.
Keywords
Introduction
According to the World Health Organization (‘WHO’), depression is a ‘common mental disorder … characterized by persistent sadness and a lack of interest or pleasure’ in previously enjoyed activities (WHO, 2020). Depressive disorders are now the single largest contributor to disability worldwide, and are likely to be the leading cause of disease by 2030 (WHO, 2017). In Australia, the current prevalence of diagnosable depression in the general population is around 6–7% (ABS, 2018; Lim et al., 2018), and lifetime prevalence is around 15% (Slade et al., 2009). Depressive disorders result in the largest number of days of reduced functioning of any mental disorder (Slade et al., 2009). As such, depression is considered to represent a significant proportion of the burden of ill health in Australia.
Since the 1980s, concerns have risen in Australia about the impact of depression. Since it was found that depressive disorders were common, and that most people with depression went untreated, efforts focused on closing the ‘treatment gap’ (Jorm, 2014). Antidepressant consumption and the provision of psychological therapy have steadily increased since that time (Jorm et al., 2017; Whitely et al., 2020; Jorm, 2018). This has been supplemented by educational measures to improve the ‘mental health literacy’ of the population (Jorm, 2012). A key aim of such campaigns has been to encourage the public to view depression as an illness just like a physical illness (Jorm, 2000). Mental health literacy campaigns in Australia since the mid-1990s have led to a marked increase in the prevalence among the public of medical and biological explanations for depression (Pilkington et al., 2013). Yet despite this, rates of depression have either stayed the same, or have increased (Jorm, 2014, 2018).
The medical model of depression has been subject to critique on a number of fronts. Critical and feminist scholars have argued that biomedical and psychological theories of depression strip distress of its political, economic and discursive context and instead locate depression as a problem or deficit within the individual (Boyle, 2011; Moncrieff, 2014; Ussher, 2010). Rates of depression are consistently found to be higher among women, and those living in disadvantaged areas (e.g. ABS, 2018). Feminist writers have questioned whether higher rates of depression among women really reflect higher rates of biological dysfunction or psychological deficit in women (Ussher, 2010); or whether women’s feelings of distress might more usefully be understood as ‘public feelings’ entangled with the conditions of women’s lives (Fullagar et al., 2019). Depression is theorized as the result of complex interactions between multiple forces including discourses, embodied experiences, power imbalances and institutional practices (Flore et al., 2021).
Another common critique is that depression is a Western cultural construct for which there is often no equivalent term in other cultures (Ussher, 2010). The symptoms of depression as per the DSM are often not considered problematic in other cultures. Whilst the DSM includes a list of ‘culture-bound’ syndromes, these do not include any Western disorders – yet globally the Western construct of depression is atypical (Marecek, 2006). As Maracek (2006, p. 303) argues, the Western disorder of depression is not a universal entity, but is, like many other culture-specific syndromes, ‘a set of practices authorized by the culture through which people express to others that they are suffering’.
How the problem of depression is represented and understood is important because the way we construct the nature of a problem determines the nature of our response to it, and whom we see as responsible for responding to it (Burr, 2003).
Online Depression Information
The internet is widely used by the public to source health and mental health information (Torous et al., 2019; Wong et al., 2014). This is especially so for commonly stigmatized illnesses including depression (Berger et al., 2018; Gowen, 2013). Since 2000, mental health websites and online resources have proliferated in Australia. In 2017 the Australian government launched Head to Health, an online ‘mental health gateway’, designed to link professionals and consumers to online resources of high quality (Sturk et al., 2019). Websites providing information about mental health are therefore recognised by government as an important influence upon discourses around depression in Australia. The Beyondblue website was one of the first of these and has been a key platform for the dissemination of information around depression (Jorm, 2012). Exposure to Beyondblue messages has been found to influence public attitudes toward mental health (Jorm et al., 2006).
Although discussion of mental health is now common on social media, many users are still reluctant to make themselves personally visible in online conversations around depression, reflecting ongoing stigmatisation (Chan et al., 2016; McCosker & Gerrard, 2021). Accessing mental health information via websites has advantages in terms of convenience and cost as well as anonymity and privacy (Chan et al., 2016). Perhaps for this reason, internet searches and websites remain a key site for the public to access information regarding mental health, including younger people (Lupton, 2021). After friends and family, the internet is the next most frequently accessed source of support for young people seeking help with important issues in their lives – ahead of social media or health professionals (Tiller et al., 2021). Whilst peer mentors and influencers play an increasingly important role in online mental health support via forums, blogs and social media (McCosker, 2018), in the online environment centralized health information from official or government websites still tends to be seen as the most credible (Lupton, 2021). Such sites are usually affiliated with academic or clinical experts, and may provide a space of relative certainty and clarity amidst the multiplicity of narratives and counter-narratives around mental health encountered on social media (Chan et al., 2016). Thus, government-endorsed mental health websites carry epistemic weight and are important sites for the education of the public and the cultural production of the constructs of mental health and mental illness.
The Present Study
In this study, the content of eight major Australian mental health websites was analysed, looking specifically at how the concept of depression was constructed in the information provided. Reviews of Australian mental health websites exist, but most have appraised sites chiefly in terms of the evidence-based nature of the information presented (Griffiths et al., 2005), or their effectiveness in reducing stigma and increasing mental health literacy and help-seeking (Griffiths et al., 2004). Whilst such reviews are valuable, they do not question the epistemological underpinnings of depression websites and how they might serve to construct depression in particular ways, nor what other discourses might be excluded (Fullagar, 2008).
Discourse analytic research has been carried out in respect of the portrayal of depression in the mass media (Clarke & Gawley, 2009; Rowe et al., 2003), and in government policy documents (Fullagar & Gattuso, 2002; Teghtsoonian, 2009). However, few studies have analysed the information presented on mental health websites using discourse analysis. Young et al. (2004) deconstructed six Australian depression websites from a critical feminist perspective, and Fullagar (2008) critically analysed the discursive construction of depression on the Beyondblue website. It was found that biomedical accounts predominated, and, except in the case of post-natal depression, power relations, social roles and structural inequalities were not addressed in any detail (Fullagar, 2008). Given that over 10 years have passed since this research was conducted, the present study extends this research by providing an updated analysis of major Australian depression websites; and by analysing a larger data set of eight websites.
Method
The data for this study are comprised of the content of the eight websites which are linked to the Australian Government’s Head to Health mental health gateway in its section on depression. These sites are all major, well-known Australian mental health websites. All receive government funding but are independently administered. Given that these are the resources which users are directed to by the Australian Government, these websites can reasonably be considered to be representative of the discourses around depression that are institutionally sanctioned in Australia currently.
To manage the large amount of website material, analysis was restricted to web pages or fact sheets which addressed the questions ‘what is depression?’ ‘what causes depression?’ and ‘what should be done about depression?’ Personal narratives were included if these were part of the informational content the websites provided to answer these questions; but discussion forums, message boards and other interactive resources were not included. This project did not require ethics approval as the material was in the public domain and accessible to anyone.
Summary of Websites Selected for Inclusion in Analysis.
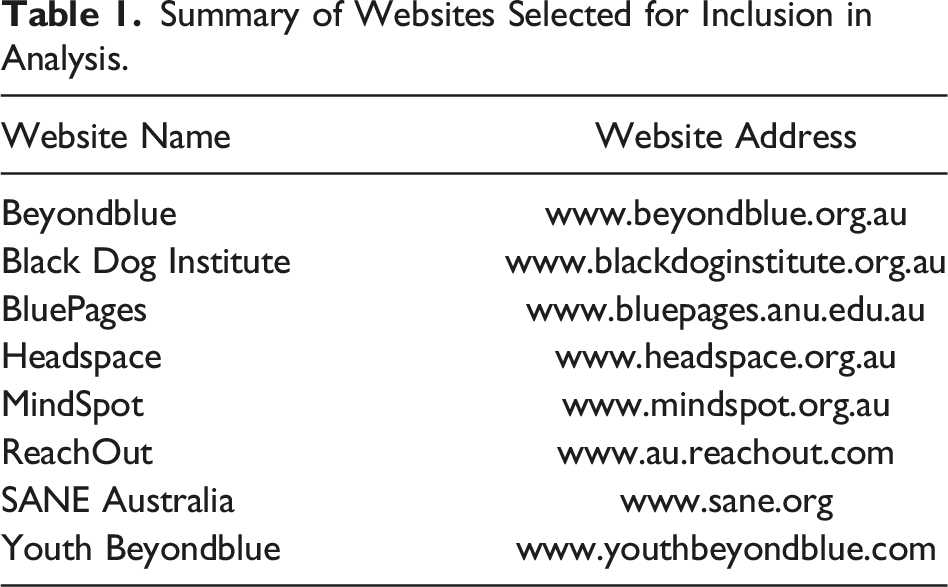
The websites above were all visited on one day, 31 March 2020, by the first author and all data analysed in this project was captured as at that point in time.
Analysis in this study drew upon the methodology of Discursive Psychology (Edwards & Potter, 1992; Potter, 1996; Potter & Wetherell, 1987), a form of discourse analysis grounded in a social constructionist epistemology. In this study, we use in particular the ‘synthetic’ approach to Discursive Psychology known as ‘Critical Discursive Psychology’ developed by Wetherell (1998) and Edley (2001). This approach combines the fine-grained analysis of text and talk with consideration of the wider historical, cultural and political context in which talk occurs (Locke & Budds, 2020).
Key concepts in critical discursive psychology are interpretative repertoires, ideological dilemmas and subject positions (Edley, 2001). These central analytic concepts were used to guide the analysis of the data in this study, and are briefly outlined here.
Interpretative repertoires have been described as ‘coherent ways of speaking that form over time, becoming easily recognisable arguments, assumptions, metaphors, figures of speech, and images’ (Van Der Merwe & Wetherell, 2020, p. 230). Interpretative repertoires are closely related to discourses, but focus less upon the abstract workings of power and more upon how the content of discourse is organized and used by people to perform actions in social situations (Wetherell & Potter, 1992).
Ideological dilemmas informed the analysis in this study, as it was anticipated that there would be likely to be different ways of thinking and talking about depression. Billig (1991) has argued that a culture’s common sense or lived ideology is by nature ‘dilemmatic’. Given that descriptions are generally chosen and constructed against alternative, ‘could-have-been-otherwise’ accounts (Edwards, 1997, p. 8), attention was paid to dilemmas within the data; and also to what was absent from the websites (Potter, 1996).
Subject positions are the identities produced and constructed for people by particular discourses or ideologies (Edley, 2001). Different subject positions will come with different roles, responsibilities, rights, obligations, possibilities for action and degrees of agency. As distinct ways of talking about social objects, interpretative repertoires will often provide or make relevant certain subject positions for participants (Edley, 2001).
Analysis in this study was carried out by the first author in several stages similar to the steps outlined by Locke and Budds (2020). Firstly, website data was read repeatedly and carefully by the first author to build familiarity. Whilst reading, systematic patterns were searched for in language, terminology, images, metaphors or figures of speech (Edley, 2001; Potter & Wetherell, 1987). Hypotheses were formed as to the functions and effects that might explain the patterns observed, including what potential alternative versions of reality may have been countered. Themes and patterns were coded and refined with each successive re-reading, and these were organized in the final analysis into four main interpretative repertoires, along with associated subject positions. Extracts considered most representative of each repertoire were purposefully selected, and a finer-grained analysis of these was carried out (Goodman, 2017). Lastly, findings were considered in light of the wider social, economic and ideological context, and what the most common repertoires around depression might achieve in that context. Analyses and results were reviewed by the second author and minor adjustments were made.
Results
On the eight websites analysed, depression was constructed through the use of two main interpretative repertoires, which will be referred to as the ‘biomedical’ and the ‘self-optimization’ repertoires. A third interpretative repertoire, which will be referred to as the ‘normal-natural’ repertoire, was explicitly argued against. A fourth interpretative repertoire, which will be referred to as the ‘societal-structural’ repertoire, had a relatively minimal presence.
The Biomedical Interpretative Repertoire
The biomedical repertoire was the most prevalent interpretative repertoire on the websites analysed. Under this repertoire, depression was constructed as an illness occurring in an individual, and requiring intervention by medical experts to diagnose and treat. Depression was spoken of as an entity separate to the individual, which invaded their mind or brain and caused changes to their usual mood and behaviour. Depression was constructed as being unrelated to the individual’s character or choices, and thus outside of the bounds of personal responsibility.
When it came to the question, ‘what is depression?’ depression was commonly explained as an illness, as exemplified in Extract 1.
1. Clinical depression is an illness, a medical condition. It significantly affects the way 2. someone feels, causing a persistent lowering of mood. 3. Depression is often accompanied by a range of other physical and psychological 4. symptoms that can interfere with the way a person is able to function in their 5. everyday life. The symptoms of depression generally react positively to 6. treatment. Extract 1 begins with a categorical assertion that depression is an illness or medical condition. The lack of any qualification, modality or hedging around this assertion serves to build factuality by conveying the impression that the statement is certain, undisputed and self-evident (Latour & Woolgar, 1986; Macdonald, 2002). Yet, despite the certainty expressed about depression being a medical condition, the description of the symptoms that follows is vague, ambiguous and hedged – ‘often’ (l. 3), ‘a range of’ (l. 3), ‘can’ (l. 4) and ‘generally’ (l. 5). This was a pattern that occurred repeatedly across the websites, revealing a high degree of ‘fuzziness’ (Lane, 2020) to the category of depression, despite the rhetoric of objective science. This pattern is indicative of what Lafrance and McKenzie-Mohr (2013) have described as a ‘fundamental epistemological disjuncture’ between objective science and subjective experiences of distress. Unlike the physical illnesses it is often compared to, depression has no biological markers, meaning it can only be defined through social processes of authority and consensus. When explaining the difference between depression and normal sadness, the websites appeared in most cases to rely upon DSM diagnostic criteria such as number and severity of symptoms and a duration of longer than 2 weeks. However, these criteria have themselves been criticised for their arbitrary nature (Kutchins & Kirk, 1997). In Extract 1, vagueness arguably functions to augment the factuality of the initial assertion, by removing the opportunity for the reader to scrutinize the detail for contradictions or errors (Potter, 1996). Carefully adjusted combinations of vagueness and detail may perform the ‘delicate rhetorical work’ of rendering a claim difficult to question, whilst providing just enough information to lead the reader to arrive at the desired understanding (Augoustinos et al., 1999). Unsaid or glossed over on the websites was the socially constructed and contested nature of the category of depression. In Extract 2, depression is reified as a disease entity separate to the individual.
1. Are you finding it difficult to reach out for help? Perhaps your depression is making you 2. feel withdrawn and unable to cope with talking to a doctor. You might be feeling 3. embarrassed, or that your problem is not important enough to ‘bother’ a doctor. Perhaps 4. you imagine that depression is something you should be able to handle and fix yourself. 5. You might even think that you are not suffering from a real illness. If so, you are not 6. alone. Many people don’t seek help for depression. However, depression is a serious 7. illness and you deserve help. 8. Depression is a serious illness. 9. Not convinced? Well, just consider this. Panels of experts have found that moderate 10. depression disrupts a person’s life as much as multiple sclerosis, severe asthma or 11. deafness. Imagine not seeking help for multiple sclerosis or severe asthma because you 12. didn’t want to bother the doctor! In Extract 2, metaphors likening depression to physical illness are drawn upon (ll. 10–12); a common feature of the biomedical repertoire on the websites. Illness metaphors serve to build the physical reality of the abstract construct of depression by suggesting a similar (if yet unknown) physical etiology (Read, 2007). As illustrated in this Extract, the biomedical interpretative repertoire constructs a subject position for the depressed person as a ‘patient’ who may legitimately occupy the sick role, but who is also expected to seek out and comply with medical treatment to expedite a return to ‘normality’.
The Self-Optimization Interpretative Repertoire
The self-optimization repertoire was also prevalent in the data. Under this repertoire, depression was constructed as an illness resulting from a lack of skills and education, and/or an unhealthy lifestyle. Therefore, the appropriate treatment for depression was to learn new skills, educate oneself and improve one’s lifestyle. Under this repertoire, depression was still characterized as an illness, but an illness which individuals can prevent and manage, potentially introducing a moral aspect.
Extract 3 provides an insight into how causation is understood differently under this repertoire.
1. People suffering from depression, particularly 2. ‘non-melancholic depression’, will often have an 3. ongoing negative view about themselves and the 4. world around them. CBT shows people how their 5. thoughts affect their mood and teaches them 6. to correct faulty negative thinking. In Extract 3, faulty, negative thoughts are said to affect a person’s mood, implying that negative thinking causes depression. This is a different understanding of causation than the biomedical interpretative repertoire, where the illness of depression was said to cause negative thinking. Under this repertoire, a person is able to change how they think, so as to avoid becoming depressed in future. Rather than the goal being to restore one’s old self, the goal is to create a new, improved self. When it came to the question of what should be done about depression, under the self-optimization interpretative repertoire the appropriate ‘treatment’ was learning skills and making lifestyle improvements. Extract 4 shows how responsibility for mental health is returned to the individual.
1. Practical steps to help yourself 2. There are lots of things you can do to fight back against the symptoms of 3. Depression. 4. Understanding makes all the difference 5. A good example of this is the flow of negative thoughts into the mind, a 6. common feature of Depression. Sometimes we are hardly even conscious of 7. these thoughts, which may cause us to feel that things will always turn out for 8. the worst or that a task is completely beyond us. 9. Once we understand why this happens, however, we can start looking out for 10. and tackling these thoughts. They are often unjustified or irrational. They are 11. often negative about things that are just as likely to turn out well. 12. There are often alternative, more practical and positive ways of dealing with 13. these concerns, which can be discussed with the treating doctor or other 14. health professional. In Extract 4, the metaphors of ‘fighting back’ (l. 2) and ‘tackling’ (l. 10) reify depression as a separate entity, but rather than the individual being helpless, they are depicted as having the power to fight back. In this account, health professionals are primarily dispensing education rather than medication (ll. 12–14), signifying that responsibility is being passed from expert to patient. Rose (1990) observed that the ‘disease model’ of mental illness is being supplemented or supplanted by an ‘educational and skills’ model. ‘Treatment’ for depression now includes the individual being trained by experts in how to think in more rational, positive and useful ways. As illustrated above, the subject positions made available to a depressed person under the self-optimization interpretative repertoire are simultaneously that of patient, and that of responsible, instrumental individual, reflecting the observation of Greco (1993) that ‘the duty to get well’ formerly associated with the sick role has now been transformed into ‘the duty to stay well’. Thus, there is potential scope for moral blame of a person who does not responsibly act to optimize the self and prevent depression, although this was never stated explicitly.
The Normal-Natural Interpretative Repertoire
Another interpretative repertoire which appeared on the websites analysed will be referred to as the ‘normal-natural’ repertoire. According to this repertoire, depression is a normal part of life and usually not an illness requiring medical treatment. This repertoire was typically negatively evaluated on the websites as resulting in harmful moral judgements of people with depression, and was usually only mentioned in order to be refuted. The conflict between the biomedical and self-optimization repertoires, and the normal-natural repertoire, was the main ideological dilemma evident on the websites.
The negation of the normal-natural repertoire was accomplished on the websites through the rhetorical device known as a ‘contrast structure’ (Potter, 1996) or ‘concession/criticism’ format (Wetherell & Potter, 1992). This typically involves an initial description of an activity or an argument with a limited concession to its legitimacy, followed by a description which undermines the activity or argument as unjustified or illegitimate. In Extract 5, the factuality of the category of depression as an illness is built up in this way.
1. Many people feel sad after they have gone through stressful or 2. difficult times. This could be a relationship break-up, trouble 3. with friends or family, changing schools or exam times. 4. It’s normal to feel down from time to time, and it can actually 5. help you to figure out what’s important to you. 6. The word ‘depression’ is often used when people are 7. talking about moments when they’re feeling sad or 8. down. Depression and feeling depressed is more than 9. ‘feeling sad’. 10. Different people will experience depression in different ways. 11. It usually includes these signs and symptoms – for a period of 12. at least 2 weeks – without improvement. The above extract begins by acknowledging that there is such a thing as sadness in response to adverse life events (ll. 1, 4), but this limited concession is followed by a refutation of the idea that these experiences of sadness are the same as ‘depression’ (ll. 6, 8–9). Critical scholars have for some time raised concerns that the category of ‘depression’ has become more capacious over time, resulting in increased scope for ‘normal’ sadness and grief to be regarded as disordered (Horwitz, 2011; Horwitz & Wakefield, 2007). Perhaps to counter such ‘medicalisation’ critiques, the websites in this study frequently worked to demarcate a clear boundary between the ‘illness’ of depression and ‘normal sadness’, as in Extract 5. The effect was to create a binary in which a person either has the illness of depression, or does not. On the websites, the normal-natural repertoire was said to create a subject position for the person who is depressed as someone who is irresponsible, weak and lazy. This account was referred to in Extract 6.
1. Symptoms may seem hard to describe. Fear of being shrugged off as ‘neurotic’ or 2. not listened to, can make people reluctant to talk to a doctor, or to describe 3. symptoms fully. 4. The stigma attached to having Depression can also discourage some people from 5. seeking help. They may feel that admitting to having a mental illness is somehow 6. shameful or labels them as a ‘failure’. This makes it all the more necessary to 7. understand that depression is a medical condition, is no one’s fault, and - 8. importantly – is treatable. In Extract 6, people with depression fear others seeing them as ‘neurotic’ (l. 1), ‘shameful’ and a ‘failure’ (l. 6). Such beliefs were seen to deter people from seeking and receiving medical help (ll. 4–5). The suggested alternative to viewing depression as a sign of shameful failure is to view depression as a medical condition which is no one’s fault (l. 7) and is treatable (l. 8). These are the only two interpretations mentioned, implying that there are no other possible constructions of the situation that can be made. According to this account, the solution to the problem of stigma is universal acceptance of the biomedical approach to depression, and prompt medical treatment of depressed individuals. Indeed, one of the main rationales behind the promotion of the medical model of depression has been that, if depression is seen as an illness outside of the control of individuals, this will reduce stigma and encourage help-seeking (Barney et al., 2009; Jorm & Griffiths, 2008). However, whilst increases in biomedical explanations for depression among the public have been found to reduce blame and perceptions of dangerousness, they have not resulted in increased social acceptance (Schomerus et al., 2012; Sarbin & Mancuso, 1970). A biomedical explanation of depression is often welcomed by sufferers as it means that their distress is socially legitimized as ‘real’, and moral blame is avoided (Lane, 2020; Lafrance & McKenzie-Mohr, 2013). Yet there is also frequently ambivalence towards a diagnosis of depression, with many patients resisting biomedical explanations and preferring to focus on social context and the need for change in their lives (Kokanovic et al., 2013; Conneely et al., 2020). Whilst the uptake of a biomedical explanation of depression may have some benefits within a particular historical and cultural milieu, its focus on individual pathology simultaneously serves to erase the social, political and economic context in which distress occurs. For example the assertion that depression ‘is no-one’s fault’ (l. 7) ignores the history of oppression and marginalization experienced by certain groups in society. This then obscures the need to address the root causes of distress through social change.
The Societal-Structural Interpretative Repertoire
A fourth interpretative repertoire around depression, which will be referred to as the ‘societal-structural’ repertoire, was referred to on some websites but was not discussed by the majority of websites. As such, this repertoire was notable for its minimal presence. Under this repertoire, depression was constructed as the result of experiences such as abuse, oppressive societal norms and structures, or a political and historical context of inequality. According to this repertoire, depression is not an illness but a reasonable and understandable response by individuals to distressing experiences.
Extract 7 illustrates what the discourse around depression can look like when a societal-structural interpretative repertoire is adopted. Notably, this repertoire of depression was deployed when accounting for depression in marginalized groups such as Aboriginal Australians.
1. These higher rates of depression need to 2. be understood in the historical context of 3. intergenerational trauma. Since colonization, 4. individuals and communities have shown 5. resilience through the many hardships and 6. experiences of grief arising from the loss of land, 7. children, culture, community, identity and pride. 8. Trauma from these losses has been passed down 9. from one generation to the next and can be 10. compounded by new experiences of racism (the 11. systematic oppression through society and its 12. Institutions) and hardship. 13. These experiences can contribute to Aboriginal 14. and Torres Strait Islander peoples’ experiences of 15. anxiety, depression, suicide and attempted suicide. 16. Culturally safe and trauma-informed services, that 17. recognise the role of trauma in depression, may 18. be particularly important for Aboriginal and Torres 19. Strait Islander peoples. In Extract 7, the direct contribution of racism and discrimination to depression is recognised. The depression of Aboriginal and Torres Strait Islander (‘ATSI’) people was referred to elsewhere in the same section as ‘psychological distress’. The use of language such as ‘distress’, ‘hardship’, ‘loss’, ‘grief’ and ‘trauma’ functions to construct the depression of ATSI peoples as a meaningful and rational response to oppression, rather than as an illness or dysfunction. In the same section, the help that ATSI peoples could access through community health services was referred to as ‘support for depression’ rather than as ‘treatment’. There was a noticeable lack of biomedical or self-optimization language – there was no talk of illness, of medical treatment, of chemical imbalances, of brains, of genetics, of ‘triggers’, of faulty thinking patterns, or of cognitive behaviour therapy. There was no talk of depression occurring for no reason, or being ‘no-one’s fault’. Whilst Extract 7 discusses the social, economic and historical context surrounding ATSI peoples’ experiences of depression, ordinarily such considerations were largely absent from explanations of depression in the data, except for passing mentions of groups who have a ‘higher risk’ of depression. The different language used in this section indicates that, ordinarily, website information assumes a universal white, male, middle-class subject ‘for whom feeling bad is frequently a mystery because it does not seem to fit a life in which privilege and comfort make things seem fine on the surface’ (Cvetkovich, 2012, p. 132). In such cases, brain malfunctions and faulty thinking styles explain otherwise unexplainable depression. Yet, as Cvetkovich (2012) argues, histories and structures of inequality and exclusion ‘haunt’ all members of a society.
Discussion and Conclusion
In this study it was found that depression was constructed in two main ways on the websites analysed – as a medical illness (the biomedical interpretative repertoire); and as an illness resulting from a lack of skills, education or healthy lifestyle (the self-optimization interpretative repertoire). Two other interpretative repertoires were alluded to but were less prevalent – the societal-structural, in which depression was seen as distress stemming from a context of structural inequality; and the normal-natural, in which depression was seen as a normal and expected part of life. Whilst previous studies have identified the dominance of the biomedical interpretative repertoire of depression, this study adds to previous research by identifying the growing role of the self-optimization repertoire in official sources, in which individuals are positioned as responsible for managing and preventing their own depression.
Overall, it appeared that the primary concern of the authors of the websites was to promote help-seeking; and that societal stigma around depression was seen as the major barrier to this. This appears to be why the websites emphasized the biomedical discourse in particular, as depression is constructed as an illness which is not within the control of the person affected. Meanwhile, the self-optimization repertoire appeared to be a preventative health measure through education and skills training. Arguably, both repertoires are likely to have some productive effects in reducing stigma and encouraging help-seeking.
However, as discussed above, the biomedical discourse may never be fully effective in reducing stigma due to the inherent differences between depression and physical illnesses. Those diagnosed cannot show any tangible evidence of a physical condition out of their control, meaning that their moral identity is perpetually shaky (Lafrance & McKenzie-Mohr, 2013). Furthermore, the biomedical model of depression creates a binary between those who have the illness of depression and those who do not; and binary constructs tend to be closely associated with stigmatising processes, given that they divide people into groups with different labels, creating an ‘us and them’ situation. In contrast, understanding depression as a continuum is associated with lower levels of stigma, likely because depression is understood as a more severe version of experiences that we all have, and people who are depressed are therefore recognised as ‘someone like us’ (Peter et al., 2021). Moreover, the self-optimization repertoire may counteract efforts to reduce stigma due to its moral overtones and emphasis on ‘fighting back’ and self-help, which may imply that those who remain depressed are lazy or irresponsible.
One of the key questions asked by critical discursive psychologists is why certain discourses or versions of reality become dominant in a culture at a certain point in history (Edley, 2001). Critics of the dominance of the biomedical model of depression have previously noted its compatibility with neoliberal ideology (Moncrieff, 2014; Sugarman, 2015; Cosgrove & Karter, 2018; Tseris, 2017), in that the problem is defined as a defect within the individual, rather than as a problem with society. However, biomedical explanations also tend to create a subject position for the depressed person as a somewhat helpless victim of their biology. The self-optimization repertoire, on the other hand, creates a subject position for the depressed person as an active, agentic, responsible citizen; which may account for the growing prominence of this account, as observed in this study. In recent times, the ever-increasing cost of providing mental health treatment has caused governments to turn attention to preventative measures in the hope that these will be more cost-effective long-term. This requires that all citizens be equipped to take on the responsibility of maintaining their own mental health (Parker, 2007).
Under both the biomedical and self-optimization repertoires, the distress that results from social, political and economic injustice is de-coupled from its context and de-politicized; reconstructed as a disorder or deficit within an individual (Cosgrove & Karter, 2018; Mulder et al., 2017; Lewis, 2006). By normalizing an individualized, deficit-based interpretation of depression, and by positioning individuals as responsible for their own mental health, contemporary medical discourses of depression play an important role in preserving the neoliberal status quo (Adams et al., 2019; Tseris, 2017).
The purpose of this research is not to argue that there is no place for biomedical and psychological understandings of depression, or that these approaches should be completely rejected. We believe that these approaches play an important role in helping many people suffering from depression. Nor is it our intent to criticize messages encouraging help-seeking for depression or to devalue the important work done by the mental health websites analysed. Rather, we aim to contribute to an understanding of the multiple ways in which depression may be constructed; and to draw attention to the political conditions which may have contributed to certain constructions becoming more prevalent than others.
In this study we focused on the analysis of text in official online sources; however, depression is shaped through a complex meaning-making assemblage involving many entangled forces including bodies, affects, objects, places, relations and practices (Fullagar et al., 2019). Narratives and discourses around depression therefore have been studied utilizing a wide range of qualitative methods. This research does not aim to provide a complete picture but to sit alongside analyses drawing upon other methodologies and focussing on other contexts and mediums such as social media. We were not able to examine how website advice was evaluated, interpreted or acted upon by its audience, or to what extent the information provided ‘cut through’ into public discourse beyond the websites. As mentioned above, the data for this study did not include any content from the websites’ discussion forums, message boards or interactive resources, which could help provide a fuller picture of how official discourses are taken up by the public; and these are potential areas for future study.
Depression is an issue of concern for societies worldwide, but current medical approaches to the problem may have limited effectiveness. This research has demonstrated that individualized biomedical and psychological conceptualizations of depression remain dominant on the major mental health websites in Australia. In order to fully address the problems of depression and stigma, there is a need for more prominence to be given to other ‘languages of suffering’ (Brinkmann, 2014). Ideally this would involve a paradigm which places the social and political realities of people’s lives front and centre rather than as an add-on consideration; and one in which the aim is not just to help people adapt to external circumstances, but also to work towards social change (Lafrance & McKenzie-Mohr, 2013).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.