
Abstract
This autoethnographic research utilizes reflexivity as a method to explore my self-experience of Lyme disease while holding co-occurring identities as a researcher, health professional, and mother. Awareness of self is central in psychotherapy so that therapists do not adversely impact their clients. This is similar for researchers who are ethically required to acknowledge and reduce any potential risk(s) of harm to their participants. In this study, I describe and systematically analyze my experiences as a patient with symptom-persistent Lyme disease, contextualized through co-occurring identities as a mother, a regulated (mental) health professional, and a scholar investigating the embodied experience of being a Lyme disease patient in the Canadian context. The central research question guiding this study is: “What are my experiences with symptom-persistent Lyme disease?” The results of this study suggest reflexivity is an important practice in both health research and healthcare. Relationships with health professionals have a significant impact on patients’ healthcare experiences, and engaging in reflexive practice may improve the responsivity of healthcare professionals toward patients’ needs and embodied experiences and serve as a check on pre-existing power relations in healthcare. Further, this research contributes to the current academic knowledge on symptom-persistent Lyme disease by offering a reflexive representation of my experiences as a researcher who is also a health professional and a patient within the Canadian healthcare system. Representations of patients’ experiences are critical in advancing health research and ensuring equitable care for patients. Autoethnography offers important insights into patients’ disease experiences.
Introduction
Autoethnography is a well-established methodological approach in qualitative social science research (Bochner, 1997; Edwards & Bess, 1998; Ellis, 1993; Forber-Pratt, 2015; Pathak, 2010; Priddis, 2015; Spry, 2006; Wall, 2008). This methodology allows researchers to be “deeply immersed in self-experience” (Edwards, 2021, p. 1). Prior to this point, positivist and modernist perspectives dominated research methods and practices (Wall, 2008). Feminist and postmodern scholars increasingly drew attention to the western-centric research practices which valued objective knowledge over embodied knowledge (Pathak, 2010; Spry, 2006). Essentially, autoethnography “provides an approach for studying yourself” (Creswell & Poth, 2018, p. 263), which is to say, it is a written, autobiographical account that involves a researcher as a research subject in a cultural context (Ellis & Bochner, 2000). Although there are many ways to conduct research using autoethnography, Forber-Pratt (2015) stresses the importance of the researcher finding one’s voice, while being honest and vulnerable. As Priddis (2015) explains, “autoethnography arises from a combination of an autobiographical approach and ethnographic methodology, which focuses specifically on reflexivity and self-consciousness” (p. 2). An emphasis on self, reflexivity, lived experience, and patient-centeredness are the central focus in this study.
Although perspectives on how to conduct an autoethnographic study range vastly, scholars who have engaged in this research methodology point to the emotional and transformative aspects of the approach (Bochner, 1997; Ellis, 1993; Forber-Pratt, 2015; Pathak, 2010; Priddis, 2015; Spry, 2006; Wall, 2008), including documenting experiences of grief, loss, trauma, and patient-centered care (Baarts et al., 2000; Breen, 2022). “Autoethnographers vary in their emphasis on auto- (self), -ethno- (the sociocultural connection), and -graphy (the application of the research process)” (Wall, 2008, p. 39). Bochner (1997) explores self-experiences of grief; whereby, he poignantly declares: “I realized as never before that I was a human being” (p. 2). Spry (2006) outlines self-experience of an “embodied,” “performative turn” through grief and loss and explains, “there was a bizarre and profound comfort in admitting to and describing this feeling of dismemberment and fragmentation … I am thankful for the disciplinary wisdom to view lived experience through theories of embodiment” (p. 341). Priddis (2015) describes self-experiences of medical trauma in childbirth and subsequent hope to “inspire reflection in health professionals to create change within themselves and the health services within which they work” (p. 2). Likewise, Breen (2022) describes her lived experience as a patient (and researcher and mother of young children) who almost died after receiving inadequate medical care. In modern, positivist traditions, academic rigor has highlighted the role of researcher objectivity; however, postmodern and feminist scholars have challenged this stance (Wall, 2008). To this point, Bochner (2000) expresses: Traditionally, we have worried much more about how we are judged as “scientists” by other scientists than about whether our work is useful, insightful, or meaningful—and to whom. We get preoccupied with rigor, but are neglectful of imagination. We hold on to the illusion that eventually we will unanimously agree on the culture-free standards to which all evidence must appeal, so that we won’t have to rely on our own “subjectivity” to decide. Criteria pose as something beyond culture, beyond ourselves and our own conventions, beyond human choice and interpretation when, of course, they are not. (p. 267)
Researchers are not bias-free (Pathak, 2010), and this research challenges positivist traditions of objectivity as I explore my own subjective position as a patient while conducting research with other patients who have had similar experiences. As Yanos and Ziedonis (2006) assert, clinically trained researchers can make important contributions to health research.
Reflexivity: Safe and Effective Use of Self
Reflexivity is a key instrument in qualitative research. “Reflexivity in qualitative research—where researchers engage in explicit self-aware meta-analysis—has a long history spanning at least a century” (Finlay, 2002, p. 209) and serves to bring introspection, and self-scrutiny, with attention to issues of privilege and power (Whitson, 2017). Arising from a range of disciplines with roots in feminist philosophies (Doucet, 2018a, 2018b), reflexivity explores how “qualitative research … relies on those who conduct it” (Charmaz, 2014, p. 15). Doucet (2018a, 2018b) describes situated knowledges, through which all knowledge must be understood from the viewpoint of the researcher and the researched. Arguably, “within … diverse forms of ‘reflexivities’ one can identify how reflexivity is practiced and adopted: who practices ‘it’; what the research is ‘on’; and what the researcher’s agenda ‘is’” (Subramani, 2019, p. 1). Research is a socially constructed experience, whereby power must not remain unexamined (Finlay, 2002). Aronowitz et al. (2015) argue: Discourses of culture can work to justify and maintain health inequalities when actors in positions of power and authority—researchers, politicians, public health advocates, physicians—designate and take for granted their own social practices as legitimate, natural, or healthy while labeling the practices of other groups, particularly those that are marginalized, as illegitimate, unnatural, or unhealthy. (Aronowitz et al., 2015, p. S403)
In response to this, they advocate for “culturally reflexive scholarship … to improve health research and practice” (Aronowitz et al., 2015, p. S403). Reflexivity can contribute to safe and effective use of self for health professionals and could serve as a check on power relations within health systems.
The practice of reflexivity in qualitative research is well-documented (Doucet, 2018a, 2018b; Etherington, 2017; Finefter-Rosenbluh, 2017; Finlay, 2002; Subramani, 2019; Whitson, 2017). To be reflexive, a qualitative researcher is required to locate, position, or situate themselves in their work. Through this process, an important discussion arises regarding the personhood of the researcher, as well as their membership role in the group being studied (Dwyer & Buckle, 2009). Doucet (2018a, 2018b) argues that “most approaches to reflexivity are informed by representational ways of knowing that give little attention to how values within our research practices are part of how we define, approach, and negotiate the making of evidence, data, and narratives” (p. 302). Researchers must attend to their own values, biases, and beliefs with respect to research practices including data analysis and presentation of results. Taking this into account, I will reflect on my experiences with insider research by locating myself as a patient and regulated health professional.
Purpose and Central Research Question of This Study
This research utilizes autoethnography methodology (Bochner, 1997; Creswell & Poth, 2018; Ellis, 1993; Forber-Pratt, 2015; Pathak, 2010; Priddis, 2015; Spry, 2006; Wall, 2008) and reflexivity as a method (Doucet, 2018a, 2018b; Etherington, 2017; Finefter-Rosenbluh, 2017; Fook, 1999; Hemmings, 2012) to tell my story. In this study, I describe and systematically analyze my experiences as a patient with symptom-persistent Lyme disease, contextualized through co-occurring identities as a mother, a regulated (mental) health professional, and a scholar investigating the embodied experience of being a Lyme disease patient in the Canadian context. This research study is guided by the central research question: “What are my experiences with symptom persistent-Lyme disease?” Utilizing reflexivity as a method provides greater depth of critical reflection and data collection (Etherington, 2017; Finefter-Rosenbluh, 2017; Fook, 1999; Hemmings, 2012).
Ethical Issues in the Disclosure of Health Status
With awareness of ethical issues, I confirm that I received ethical approval from the Brock University Research Ethics Board (REB #21-144-MOORE) and provided written informed consent prior to commencing this research. Studying oneself involves a level of vulnerability; thus, “autoethnography is not for the faint of heart” (Forber-Pratt, 2015, p. 822). Researchers using this methodology are subject to considerable examination from peers in ways that intersect both the personal and professional realms. Other researchers such as Della Porta and Ingrao (2022) have documented similar anxiety around “sharing real experience” (p. 4) in their work. Admittedly, I have approached autoethnographic research with hesitancy. I am concerned that my legitimacy as a scholar will be more heavily scrutinized if I acknowledge my experiences with symptom-persistent Lyme disease given the contentious debate in academic literature regarding the disease (see also Ali et al., 2014; Auwaerter et al., 2011; Bamm et al., 2019; Boudreau et al., 2018; Cameron, 2010; Dumes, 2020; Gaudet et al., 2019; Lantos, 2015; Oliveira & Shapiro, 2015; Shapiro, 2014; Tracy & Baumgarth, 2017). Through reflexive practice, I grappled with the following questions: How much do I share? What are the risks of sharing my story? How will I know if I am sharing too much? What about not sharing enough? I struggled with the possibility that I would receive personal versus professional scrutiny. It is one thing to receive feedback on my work, and it is another to receive feedback on how I express my embodied experiences.
Conceptual Framework
This research utilizes reflexivity through a transdisciplinary theoretical orientation (Bai, 2008; Choi & Pak, 2006; Klein, 2015; Leavy, 2011; Mitchell & Moore, 2018; Montuori, 2013; Moore & Ciotti, 2021; Robinson, 2008). My scholarly background and professional practice have exposed me to a range of perspectives including sociology, criminal justice, public policy, couple and family therapy, and child and youth studies. Historically, reflexivity is bounded in disciplinary traditions, variable in their epistemology (Subramani, 2019). Transdisciplinary research is a reflexive approach, developed in response to the dominant model of knowledge production (Popa et al., 2015). Ontologically oriented toward transformative social justice (Moore, 2018), transdisciplinarity seeks to address complex social issues (Leavy, 2011; Montuori, 2013). Social justice “is an ongoing practice of analysis, action, and striving … constantly ask about social worlds … the identities and positionality of all those who are involved, and the horizons of hope and possibility for rendering freedom, justice and equality” (Kouri, 2020, p. 69). Fundamentally, I believe research should seek to improve social conditions, particularly, for those traditionally marginalized, underrepresented, and socially excluded.
Advancing Health Equity: Reflecting on the Social Determinants of Health and Intersectionality
Health researchers (see also Fisher & Kalbaugh, 2011; Hay et al., 2019; Nelson, 2002; Smedley et al., 2003) have drawn attention to the importance of addressing health disparities. It is important that health researchers and clinicians consider the social determinants of health (World Health Organization, 2008) and intersectionality (Crenshaw, 1989, 1991) to advance equity in public health research and policy. The social determinants of health recognize the ways in which human health is impacted by social conditions (World Health Organization, 2008). Intersectionality-informed approaches to health research: … have their antecedents in feminist and anti-racist traditions in the USA, and start from the premise that people have multiple identities. They seek to understand the ways in which patriarchy, class oppression, racism and other systems of discrimination create inequalities among women and men, placing some at relative advantage or position of power as compared to others. (Ravindran, 2017, p. 1322)
This approach encourages health researchers to critically analyze pre-existing power structures that contextualize and impact human health. By reflecting on their backgrounds, social locations, and internal biases, health researchers and professionals maintain professional boundaries and ethics. My social location involves intersecting identities of power, privilege, and exclusion. My identities as a woman and a person with a disability have contributed to my experiences of exclusion; however, my other identities (racial, professional, socio-economic, and educational) have afforded me greater access to systems. For example, as a health researcher and a health professional, when I access healthcare as a patient, for the most part, health professionals seem to treat my symptoms with sincerity and view my health complaints with credibility. I have some ability to articulate my knowledge of health research and understand the professional practice standards of regulated health professionals (e.g., consent and confidentiality).
Intersectionality is an important interpretive and analytical framework for public health (Bowleg, 2012) and aligns with the social determinants of health framework (World Health Organization, 2008). Representation and awareness of intersectionality in health research are imperative in advancing health equity for individuals and groups who have been traditionally underrepresented including racialized persons, women, and children (Fisher & Kalbaugh, 2011; Hay et al., 2019; Spencer et al., 2020). As Bowleg (2012) asserts: Acknowledging the existence of multiple intersecting identities is an initial step in understanding the complexities of health disparities for populations from multiple historically oppressed groups. The other critical step is recognizing how systems of privilege and oppression that result in multiple social inequalities (e.g., racism, hetero sexism, sexism, classism) intersect at the macro social-structural level to maintain health disparities. (p. 1267)
Further, according to Kapilashrami and Hankivsky (2018): There is no single way to approach intersectionality and no preferred method. However, there are some fundamental questions that researchers could ask at each stage of the research process. Researchers need to also be self-reflexive throughout, by considering how their own social positioning shapes how they approach the examination of any research question in global health. (p. 2590)
Reflexivity as a method allows health researchers to formulate greater critical engagement and awareness of intersectionality within their work. Throughout my research on patients’ experiences with symptom-persistent Lyme disease in Canada, I continued to engage in self-reflection and reflective journaling simultaneously.
Methodology
This qualitative research study utilizes autoethnography methodology (Bochner, 1997; Creswell & Poth, 2018; Ellis, 1993; Forber-Pratt, 2015; Pathak, 2010; Priddis, 2015; Spry, 2006; Wall, 2008) to tell my story. This approach has been associated with various disciplinary traditions including health sciences, disability studies, sociology, and anthropology (Bochner, 1997; Creswell & Poth, 2018; Ellis, 1993; Forber-Pratt, 2015; Pathak, 2010; Priddis, 2015; Spry, 2006; Wall, 2008). Transdisciplinary research and its anticolonial focus (Moore, 2018; Moore et al., 2005) align well with autoethnography. As Pathak (2010) asserts, autoethnography is not merely “me-search,” but rather, this is a misguided perspective that represents a “deeply colonialist position,” which privileges western “intellectual” knowledges over “embodied” knowledges (pp. 3–4). Researchers who have used autoethnography as a methodology have expressed the intention to facilitate meaningful change in academia and beyond (Bochner, 1997; Ellis, 1993; Forber-Pratt, 2015; Pathak, 2010; Priddis, 2015; Spry, 2006; Wall, 2008).
Methods
Wall (2006) suggests “autoethnography is less of a method and more of a philosophy, theoretical underpinning, or paradigm, aimed at restoring and acknowledging the presence of the researcher/author in research, the validity of personal knowing, and the social and scientific value of the pursuit of personal questions” (p. 6). I utilize reflexivity (Doucet, 2018a, 2018b; Etherington, 2017; Finefter-Rosenbluh, 2017; Fook, 1999; Hemmings, 2012) and reflective journaling (Sealy, 2012) as methods in this autoethnography. I use memory as data, by writing a personal narrative (Ellis & Bochner, 2000), and systematically analyze multiple relevant data sources (i.e., photos, social media posts, medical documents and records, medical expenses, and email) using thematic analysis (Braun & Clarke, 2006, 2012; Ciotti et al., 2022; Glaw et al., 2017; Vaismoradi et al., 2013). These additional sources of data were included as a method of checking my memories and addressing potential concerns regarding academic value in my work. Although, as a methodology, autoethnography is rather unconventional, these methods are conventional in qualitative research. Pathak (2010) asserts autoethnography “disrupts the traditional academic voice” (p. 1) and, as a result, presents specific challenges including ensuring academic value. However, Bochner (2000) asks “what is it we are not talking about when we are talking about criteria? Instead of asking, how can this be true? we could ask, what if this were true? What then?” (p. 267). This question was central in my decision to tell my story through this autoethnography—my voice will contribute to knowledge on patients’ experiences in research.
One way I attempted to address potential concerns about academic value and truth in my work was to engage in member-checking. Member-checking is “the method of returning an interview or analysed data to a participant” (Birt et al., 2016, p. 3). Forber-Pratt (2015) argues this can build validity to the “non-traditional approach” (p. 821) of autoethnography. In this study, member-checking occurred in dialogue between myself and others. To guide me in this process, I utilized the questions outlined in Forber-Pratt (2015): Does It Make Sense to Me? Does It Make Sense to Someone Who Knows Me Really Well? Does It Make Sense to Someone in My Family? Does It Make Sense to an Academic? Does It Make Sense to a Non-Academic? Does It Make Sense to Someone Who Does Not Know Me Very Well? (p. 834)
Additionally, I used member-checking as a tool to evaluate my data which was checked by me, my partner, and all members of my dissertation committee. This process allowed me to reflect on my experiences more deeply and subsequently articulate them for others who might read my work. Figure 1 illustrates the methods utilized in this study: Methods.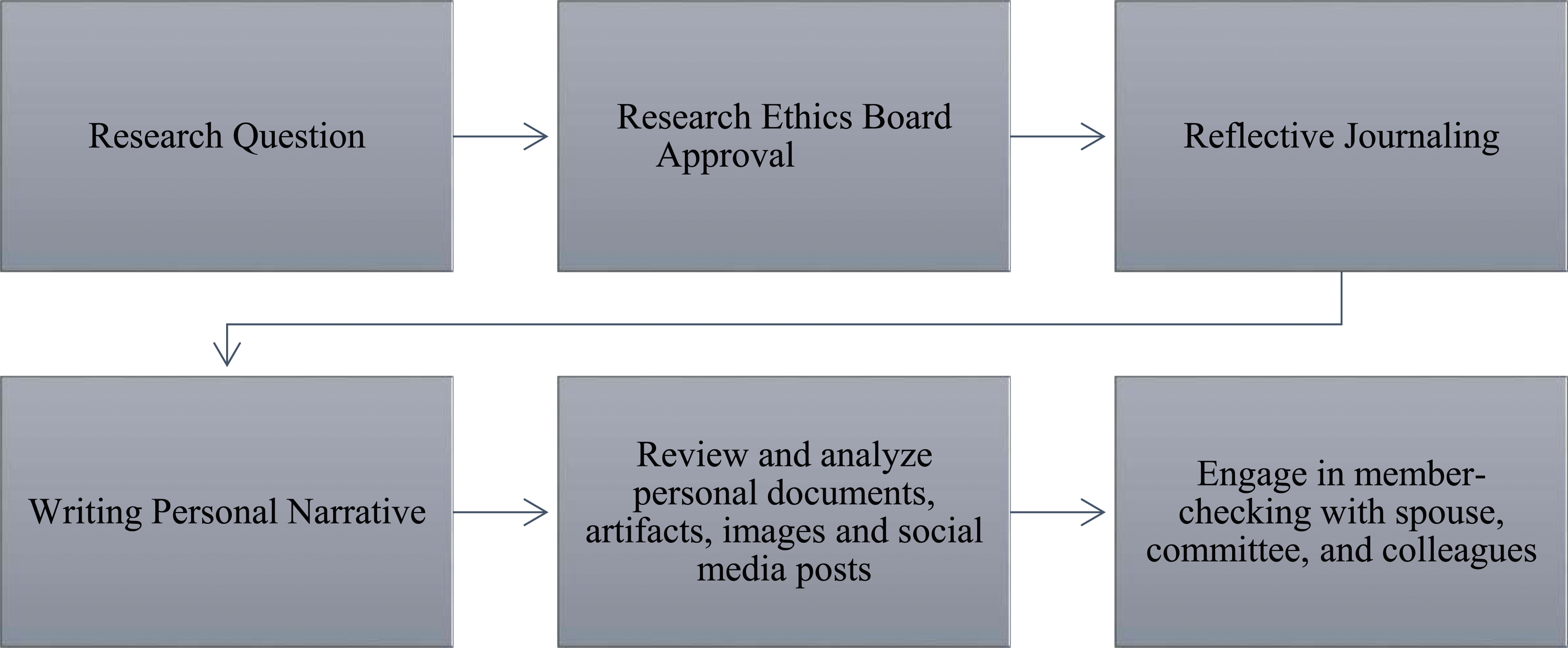
My Data
Wall (2008) suggests “for the most part,” data used in autoethnography follow the tradition of ethnography including “interviews, participant observation field notes, document and artifact analysis, and research diaries” (p. 44). While noting in her autoethnographic study, she largely “relied on the memories of [her] lived experience” (p. 45). For this autoethnography, I accessed my personal photographs, social media, medical documents and records, artifacts (supplements and medications), emails, and medical expenses. An example of a data source (which was incorporated in my analysis) is taken from one of my Private Instagram/Facebook posts, dated August 25, 2019, and presents a tearful image of me, along the following caption: This was a very vulnerable moment. Perhaps I captured it because I was in such despair I wondered if anyone would believe me. I am sick. In the past 9 months or so I have seen over a dozen doctors and about the same amount of other health professionals. I have a long list of symptoms including vertigo, migraines, eye issues, tinnitus, vestibular issues, sinus pain, migrating sharp stabbing pains, joint pain, numbness and tingling, hormonal sensitivity, concentration issues, and gastrointestinal issues that make daily living unbearable at times. I have had many tests and paid thousands out of pocket to treat and manage symptoms (not covered by OHIP). In June, I tested positive for Lyme.
This post captured the most distressing and difficult time in my illness.
In addition, I engaged in critical reflexivity through conversations with my family, friends, acquaintances, health providers, colleagues, and committee members about my self-experiences and co-occurring identities. This data was utilized in addition to the reflexive journals I wrote while conducting research with patients with symptom-persistent Lyme disease. Like Wall (2008), I incorporated my own memories, to my story as a patient, along with my co-occurring identities as a mother, researcher, and health professional. Importantly, “the significance of memory in the process of ethnography has been acknowledged” (Wall, 2008, p. 45). I was challenged to explain my use of memory as data by my dissertation committee, including how I chose to use this data to tell my story. Through writing a personal narrative (Ellis & Bochner, 2000), I describe and systematically analyze my experience of having co-occurring identities while investigating patients’ experiences with symptom-persistent Lyme disease in the Canadian context. My story is not presented chronologically; instead, I chose to write about my co-occurring identities (while emphasizing how these identities intersect) as I believe this best captures the gestalt of who I am in this moment. Figure 2 illustrates the data analyzed in this autoethnography: Sources of Data.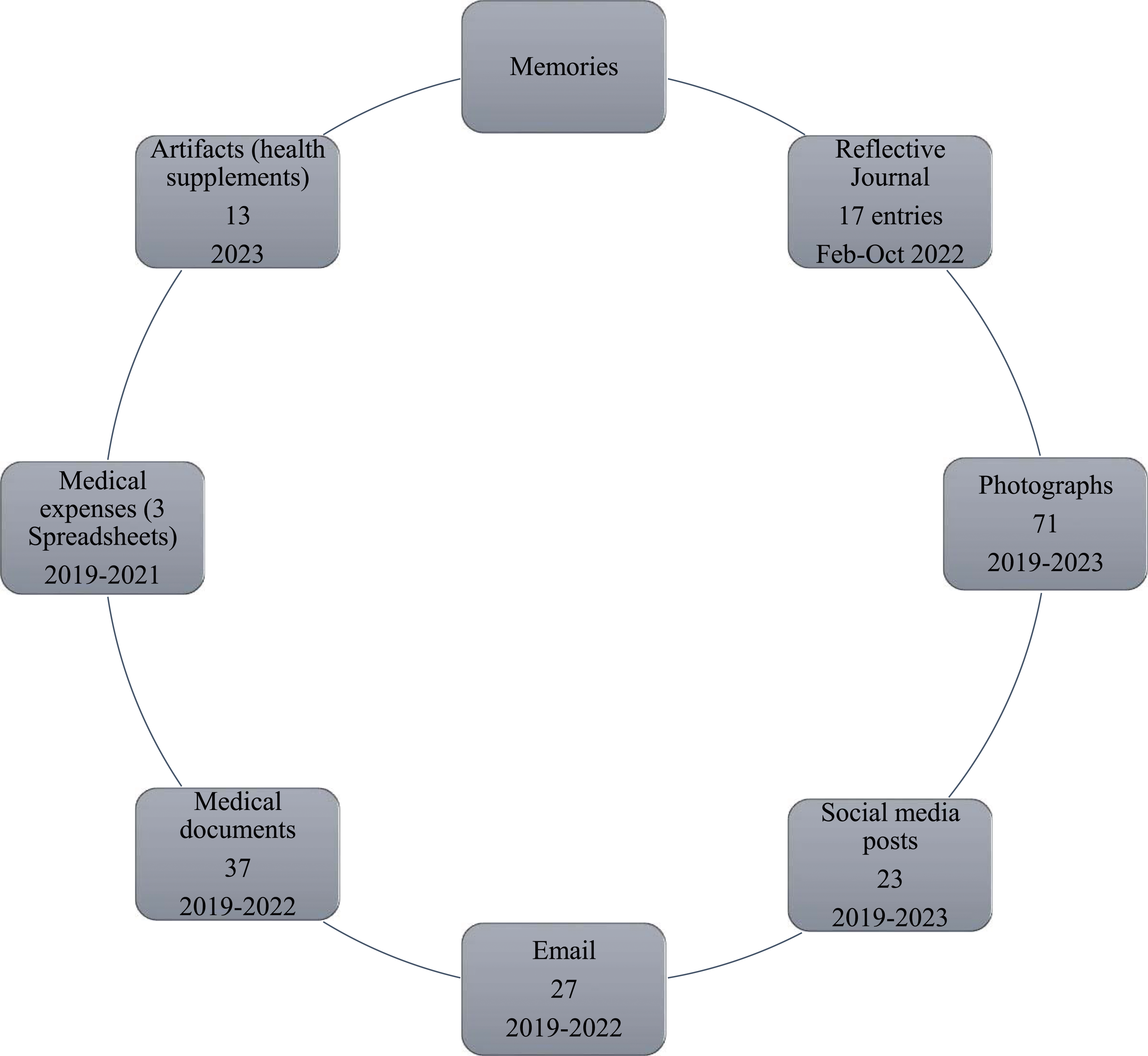
My Process of Analysis
In qualitative research, data analysis is most frequently presented through codes and themes that emerged through interpretative analysis. In my review of autoethnography literature, it is not always made explicit how the analysis unfolded, while at the same time, choices are made. For example, Spry (2006) and Forber-Pratt (2015) do not mention analysis in their work. Moreover, Bochner (2000) argues “it is impossible to fix a single standard for deciding the good and right purposes, forms, and practices of ethnography. This has been tried before without notable success” (p. 268). There appears to be some ambiguity in the literature regarding the methods of data analysis applied in autoethnographic research. As Wall (2008) points out, “autoethnography has been used as a way of telling a story that invites personal connection rather than analysis” and “explicitly links to concepts from the literature to the personal narrative” (p. 39). I am drawing on this autoethnographic tradition by describing my story with examples from my embodied experience (personal connection) and literature (academic connections) to arrive at my conclusions.
I apply thematic analysis (Braun & Clarke, 2006, 2012; Ciotti et al., 2022; Glaw et al., 2017; Vaismoradi et al., 2013) as a primary method to analyze multiple data sources (i.e., photos, social media posts, medical documents and records, medical expenses, and email) in this autoethnography. I used photo elicitation and autophotography which are commonly used techniques in ethnographic research (Glaw et al., 2017). I analyzed my personal archival photos to explore my emotions, thoughts, and memories and generate a narrative discussion of my experiences as a patient. Multiple data sources (photos, social media posts, medical documents and records, medical expenses, and email) were chosen as a method of checking my own memories as expressed in my memory (narrative account) of my illness experiences before I began my research with patients with symptom-persistent Lyme disease. I engaged in reflective journaling during the research process, and these journals were used as textual data to tell my story of co-occurring identities. Textual data was prioritized, and supplemental data in the form of spreadsheets, photographs, and personal artifacts were applied to contextualize my story.
As both a researcher and a research subject, I made conscious choices on which data to include based on my ontology and epistemology and ethical considerations around my own confidentiality as a human subject. For example, I chose to withhold detailed and specific aspects of my personal health information. This is not outside of the ethical standards in research—there are always boundaries on the process including protecting participant data with confidentiality. In this way, I made ethical decisions not to share beyond what I need to as a scholar, and this is the point at which member-checking became significant in my work. I sought feedback on what to add and what to subtract in relation to my story.
My knowledge in this area is built upon my previous research where I utilized thematic analysis, content analysis, and critical content analysis (Ciotti et al., 2021, 2022; Ciotti & Moore, 2022; Moore & Ciotti, 2021). This insight has informed my approach to finding and identifying the key excerpts in my memories that clustered together (codes) to form the identification of parts of my story (themes) that became my story (the key results). Some examples of codes that developed into themes include: disease (i.e., impact on daily life and overall functioning), mothering (i.e., expectations and limitations due to illness), symptoms (i.e., initial and ongoing in addition to management and treatment), conventional healthcare (i.e., formal diagnostics and treatments such as serological testing and prescribed medications), unconventional healthcare (i.e., naturopathic care, herbal treatments and supplements, and dietary/lifestyle changes), and emotions (i.e., fear, grief, sadness, and anger).
My Story (Results)
My story (the results of this study) is a representation of my self-experience of having co-occurring identities as a patient with symptom-persistent Lyme disease, a mother, a regulated health professional, and a scholar investigating the lived experiences of patients with symptom-persistent Lyme disease in the Canadian context. I explore the tensions I experienced in conducting this autoethnographic study. I experienced some consternation around sharing my innermost experiences of health and illness so publicly (and in a professional capacity). Upon reflection, and through discussions with peers, my supervisor, and those close to me, I realized that my apprehension around sharing my story of illness has been largely shaped by professional experiences to date. As a regulated health professional, I have been able to effectively separate my personal experiences and emotions from my professional practice. For example, in one instance, I found out about the death of a family member immediately before a session with a client—I dissociated from my feelings of shock, sadness, and grief during the session to focus on my professional responsibilities as a therapist. During the session, I set aside my emotions and focused on my work, but afterward I questioned if dissociation could be possibly dangerous to my humanity, as this makes me an empathetic and compassionate therapist—my ability to deeply and authentically feel. Upon deeper reflection, I noticed how my co-occurring identity as a mother has also allowed me to practice setting aside my own feelings and needs to focus on meeting the needs of my children (I am sure many parents can understand the sleep deprivation that comes along with a newborn feeding schedule). This is an example of how my identities intersect and subsequently shape my perspectives and reactions in both personal and professional experiences.
Themes and Source of Data.
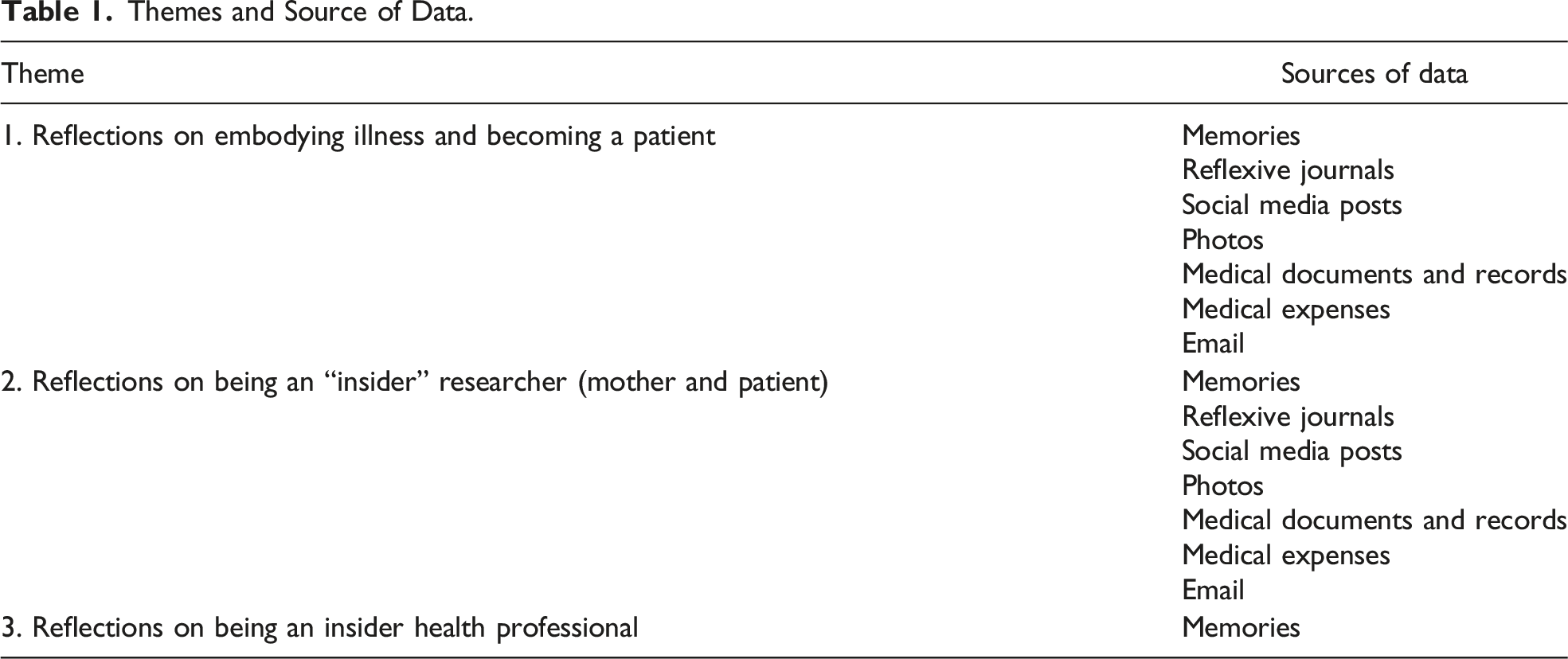
Reflections on Embodying Illness and Becoming a Patient
I understand chronic pain and illness. I have experienced a range of symptoms including vertigo, vestibular migraines, stomach pains, neck pain, shoulder pain, jaw pain, knee pain, ringing in the ears, visual disturbances, newly acquired allergies, nausea, physical exhaustion, and symptoms of anxiety and depression. I understand the fear of living with progressive pain and disability. For example, while conducing this research, I had an experience of severe pain which led me to the emergency room. In an excerpt from my journal, on June 22, 2022, I describe an emergency medical experience while I was in the data collection and analysis stages of my research: Following my most recent interview I struggled with a major health issue that landed me in the emergency room for 13 hours. After several tests including blood, urine, ultrasound, and CT scan I found out that I have inflammation in the bowel and perhaps Crohn’s disease? Or an infection. I have to follow up with a GI specialist in August. I am told this is rather fast in the current healthcare climate in Ontario.
This example points to the unpredictability of embodying chronic illness. At times, managing symptoms of illness can be overwhelming and disruptive. At that time in my life, I was experiencing significant stress, which I have found can lead to a symptom flare-up. These flare-ups can impact my capacity to work, parent, and care for myself, and at times, they stop me in my tracks. Medical appointments occupy a great deal of my time in addition to managing my symptoms.
To an outsider, it is exceptionally difficult to describe the kinds of emotions that can be stirred up when you get sick. You wonder whether you will survive and begin to ponder what the end of your life will be like. Since getting sick I have experienced what at times felt like never-ending worry about my remaining quality of life; I wondered how I would survive the pain and suffering, and admittedly, there were dark times I had fleeting hopes for a painless end. In my experience, it is one thing to intellectually understand chronic illness, and it is another to embody chronic illness. For example, of course a cancer doctor or cancer researcher would understand cancer, but a cancer patient intimately understands cancer by facing it—living it every day, going to bed with it every night, and waking up with it every morning. But Lyme disease is not cancer, and the experience of not being believed or having physicians say it is all in your head can be particularly challenging for patients. In my own experience, I was referred to a psychiatrist by my GP who repeatedly told me that my symptoms were caused by anxiety. Subsequently, I visited a psychiatrist who referred me to a specialized women’s health (outpatient) clinic in a hospital. After I completed the initial assessment process, I was told that I did not have a mental health issue. I debated sharing this last point, but I think it is critical to voice that I as a patient/health researcher and regulated mental health professional met the same scrutiny when engaging with the health system.
I was initially referred to a psychiatrist after I visited my general practitioner (GP) crying and begging for help. In this situation, my long-time partner came with me to the visit (as a family, we have shared the same general practitioner for over a decade) because he directly witnessed my struggles with illness and was concerned about the level of distress I was experiencing. Later, he attended my psychiatrist appointments at the hospital to offer me support. This experience was paternalistic and demoralizing, and I felt like my voice had been muted. At the same time, I felt that I needed my partner to speak out on my behalf and lend credence to the fact that I was not making up my illness. This was a very vulnerable and desperate time in my life. I would have vestibular migraines that were so severe I could barely function; my sleep was adversely impacted, and I was unable to practice yoga (which was an important stress management technique for me). I recall crying alone during the day hoping for some relief.
I share this story to emphasize the desperation and despair I was experiencing at the time and to highlight the challenges I faced negotiating the power dynamics involved in the doctor–patient relationship. This is supported by Greenhalgh (2001) who explores patients’ experiences with chronic illness/pain and subsequent power relations within the doctor–patient relationship. Upon reflection, I ask myself: Did my chronic illness/pain impact my mental health? My answer: unequivocally yes. Those who have embodied knowledge of chronic illness/pain are aware of the mental suffering this can cause. However, despite this, according to my healthcare providers, I did not meet the diagnostic criteria for a mental disorder. In some ways, this was both validating and invalidating. Validating in that my illness was not deemed psychological (i.e., it was not simply “all in my head”) and invalidating in that even my mental suffering was not diagnosable.
My self-experiences of illness had both good days and bad days. At times, the bad days disrupted my daily living to the point where I was unable to function but merely had to cope with the pain. This experience mirrored some of those shared by my research participants. For instance, one young person I interviewed shared this exact experience of coping with pain, not being able to live fully the way he once did, taking the pain day by day, praying for recovery. I know from my own experiences of disease, when symptoms are severe enough, illness can consume one’s daily life and adversely impact one’s mental health. Findings from Fallon et al. (2021) support this assertion—patients who had previous Lyme borreliosis infections had higher rates of mental health disorders and suicidal ideation. In my clinical work, as a somatic-oriented trauma therapist, I understand how physical/somatic pain and emotional pain are deeply connected. I have worked with many trauma survivors who shared stories of chronic physical pain and health anxiety; the association between post-traumatic stress disorder (PTSD) and somatic symptoms has been documented in academic literature (Afari et al., 2014; Gupta, 2013; McCall-Hosenfeld et al., 2014).
While simultaneously ruling out mental illness, I have continued to seek treatments for physiological symptoms. I have tried several different medications to treat my symptoms over the years and have often found their side effects unmanageable. In my experience, taking pills/tinctures/herbal medicines was the primary solution offered through conventional and unconventional medicine. Several medication trials did not provide enough symptom-relief to tip the scale toward benefit versus risk. For example, some of these side effects were severe nightmares and increased anger/volatility. As a mother, a student, and a professional, I made the decision that these side effects had adversely impacted my home and professional life. At the time, I began to explore supplements, lifestyle, and dietary changes that could improve my symptoms. In my research, I read that magnesium could be effective in migraine prevention. When I spoke to one of the neurologists I saw, he advised me that yes, magnesium in combination with CoQ10 and B2 could be effective in preventing migraines, and he offered a suggested daily dosage. Later, I sought advice from a naturopathic doctor who suggested that I add some additional supplements and directed me to specific brands based on their brand quality. I saw a reduction of my symptoms with no adverse side effects (beyond out of pocket costs), so I continued with this regimen. Recently (October 2022), I had my gastroenterologist recommend specific dietary supplements for persistent bowel/stomach pain. Currently, I take less medication than when I was being treated for Lyme disease; however, I continue to take pills (over 20 a day) to help me maintain my wellness and prevent a flare-up of symptoms. Image 1 represents my co-occurring identities before illness. Co-occuring Identities Before Illness.
Image 2 represents my co-occurring identities after illness. Co-occuring Identities After Illness.
My identity as a patient became central after getting sick. Importantly, this identity was not chosen by me, rather was an unexpected and challenging experience that I was tasked with adapting to, compared to my other identities as a researcher, health professional, and mother, which were chosen by me and were deeply impacted by my illness. This experience of illness has taught me how precarious my health is.
Reflections on Being an “Insider” Researcher (Mother and Patient)
The viewpoint of a researcher as a patient offers a unique perspective and contribution to health research; being an insider in research comes with both benefits and challenges. Importantly, my role as a researcher is self-directed, and my identity as a patient is involuntary. For instance, Dwyer and Buckle (2009) assert: … being a member of the group under investigation does not unduly negatively influence the process. Disciplined bracketing and detailed reflection on the subjective research process, with a close awareness of one’s personal biases and perspectives, might well reduce the potential concerns associated with insider membership. (p. 6)
Moreover, insider membership may result in greater candor between the research participant(s) and the researcher, leading to richer data collection. As a qualitative researcher and a trained mental health professional, I am acutely aware that populations are not homogeneous, and shared membership does not equate to shared experience. A closer proximity between the researcher and the group or topic they are studying might make it more difficult for insider researchers to distinguish themselves from their participants, potentially influencing data collection and analysis. As Finefter-Rosenbluh (2017) argues, researchers can influence their research in a variety of ways including participants’ responses in an interview; insider researchers might find it difficult to separate their personal experiences from those of their participants. I argue these are important considerations for all researchers who are studying human participants. Researchers hold awareness that “research is co-constituted, a joint product of the participants, researcher and their relationship” (Finlay, 2002, p. 213). Attending to relational dynamics, including power and communication techniques, ensures researchers uphold strong research ethics. Ultimately, researcher knowledge is informed by their “positionality” (Mullings, 1999), and the same can be said for therapist knowledge.
As a researcher (and health professional) who has witnessed patients’ experiences of pain and suffering, I have reflected on how these parallel my self-experiences. When we are truly suffering, it can be difficult to see where your illness ends and you begin. In other words, it is difficult to answer how do I exist beyond being sick? For many mothers, this is particularly distressing. The participants I interviewed, who were mothers with symptom-persistent Lyme disease, shared stories of self-doubt and sadness around parenting limitations because of their chronic illness. As a mother, I experienced these limitations and struggled to accept that I was no longer able to function as my old self, which led to feelings of grief and loss. I mourned the identity I had once held and had to work on letting go of the possibility that certain dreams will be unrealized. Time and time again, I heard from patients who in the face of this adversity recognized their resilience and strength, pointing to their emergence as a better, stronger, more capable person in the face of this pain and suffering. I recognized this in a February 7, 2022, journal entry that I wrote after interviewing my second participant: I could relate so much to her story including being challenged to find support as well as balancing her responsibilities as a mother with taking care of herself and managing her illness. I remember when I was sick, I wondered what my life would be like whether I would end up in a wheelchair or unable to leave my bed and the fear and anxiety I had about this. I also have been someone who has been high-performing and achieving and when I got sick this really pushed my energy to almost a grinding halt. I still struggle with guilt and shame about feeling sick: the impact that my illness and being in pain has on my parenting. I regularly worry about the long-term effects of my illness on my children’s mental health and well-being. This, combined with the pandemic has been quite challenging and I recognize in this participant’s story the importance of having broader social support when managing such a complex and chronic illness. It’s hard to hear these stories of pain and suffering that are too familiar to me, but I also acknowledge that their story and my story are unique and worth being told.
Here, I describe how this interview reminded me of my own relationship with chronic illness and the subsequent negative impact on my mental health. Through my experiences as a researcher with co-occurring identities as a mother and a patient, I became aware of a kinship I feel with mothers with symptom-persistent Lyme disease. I reflected on the impact my illness has had on my mothering. I am afraid that I will become too sick to be able to care for my children. I feel guilty if I am unable to be as involved or active as I would like to be when I am experiencing a symptom flare-up. On occasion, this has adversely impacted my mood (and possibly healing) because I am frustrated and overwhelmed by my illness/pain and my motherhood responsibilities. Motherhood is a complex identity that I understand more profoundly because I am an insider. Similar to being a patient, it is one thing to understand motherhood conceptually, and it is another thing to be a mother. It is something completely different to be a mother who is also a patient.
Reflections on Being an Insider Health Professional
I locate myself as an insider health professional. I have built a diverse professional career working with women, children, youth, and families in both the health and social services fields. My career has spanned over two decades across various human and social services sectors including youth homelessness, child welfare, youth justice, children’s mental health, children’s recreation, children’s residential care, transitional housing for women in conflict with the law, and adult mental health. I have witnessed the ways in which large systems manifest power (Gore & Parker, 2019) and reinforce pre-existing structures of oppression and exclusion for traditionally underrepresented groups. For example, I worked for over a decade in the child welfare system in Ontario—this system has been widely criticized for historical and contemporary racism and the overrepresentation of Black and Indigenous children and youth in care (Maynard, 2017; Vowel, 2016). I also worked within the youth justice system which has faced similar criticism (Maynard, 2017; Vowel, 2016; Wiley et al., 2020). Working within these systems, I noticed how much discretion was granted to professionals and became conscious of how the professional relationship became significant in how service users (or clients) experienced the system. My experiences working in these systems solidified for me the importance of acting according to my own values in my professional praxis.
A pivotal point in my career came in 2015 when I registered with the College of Registered Psychotherapists Ontario (CRPO). As a mental health professional, I hold an innate understanding that the therapeutic relationship is centered on the client. My experiences as a therapist who worked for years with children and youth who experienced sexual trauma has led me to be very cautious about self-disclosure and rigorous with my professional boundaries. I was trained that self-disclosure should be used sparingly and only in ways that benefit the client. As outlined by the CRPO, psychotherapists must regularly engage in professional development on safe and effective use of self that often includes ongoing reflexive practice (College of Registered Psychotherapists Ontario, 2022). From my psychotherapy training, I have gained an appreciation for power imbalances in the therapeutic relationship—professionals hold a great deal of power, and therefore, ethically we must attend to this to avoid abuses of power or professional misconduct practice (College of Registered Psychotherapists Ontario, 2022).
My experience working as a psychotherapist within the conventional healthcare system exposed me to the challenges patients face receiving mental healthcare. I witnessed firsthand stigmatization of patients with mental illness within the healthcare system and this was a valuable lesson—there was a hierarchy and the doctors were always at the top. What I could not figure out was: Weren’t the patient’s needs supposed to be above all else? As might be expected, I did not last long within that system. I could not compromise my values, ethics, and professional standards as I saw them. I believe firmly that healthcare should be focused on the patient, and as a practitioner, I strive to work collaboratively with my clients. I do not believe therapy is something that is conducted on but rather is conducted with clients. Those seeking out care for their mental health must maintain their agency. My role as a therapist is to assist clients in working through problems and challenges while prioritizing the client’s voice, choice, and empowerment. As a health researcher, I am even more resolute that healthcare professionals should practice reflexivity. I believe health professionals should be mindful of the ways in which they may reproduce systems of inequity, exclusion, and oppression in their professional practice and actively work toward resisting this. I take the strong position that the client (or patient) is the expert in their own lives and experiences.
Discussion
The findings from this study align with previous health equity research suggesting patients report higher standards of healthcare when their providers acknowledge their self-experiences (Aronowitz et al., 2015; D’Anna et al., 2018; Lantos, 2015; Ocloo et al., 2020), reinforcing Whitson’s (2017) assertions that issues of power and privilege should not remain unchecked in healthcare. How patients experience the healthcare system is directly impacted by how they are treated by the professionals they encounter (Smedley et al., 2003; Sripa et al., 2019). My self-experiences as a patient offer a unique perspective in the study of patients’ experiences of disease. As a patient, I understand that dealing with denial of one’s experiences does not appear to take away the pain but rather amplifies it like a smoke detector alerting you to a fire, but having support and being believed takes the edge off. I know as a patient that support becomes an important aspect of treatment of disease. This aligns with the findings by Lantos (2015) who suggests that patients with symptom-persistent Lyme disease experience feeling disappointment with the level of healthcare they receive. I studied my self-experiences with Lyme disease for this reason: to challenge the traditional academic voices and discourse regarding patients with Lyme disease. In this way, I may advance knowledge on the disease and the adverse impact that it has on patients (whose voices have largely been ignored in the current body of scholarship on this topic). This is not “me-search”; rather, this is patient-search, telling the story of one patient’s experiences.
My experiences as a patient significantly differ from my identities of a researcher and health professional—positions that are empowering. Although “patient empowerment pervades clinical practice, teaching and research: patients are expected to take control over their illnesses or treatments where possible, and doctors are expected to encourage or ‘empower’ them to do so”; however, “in practice, patients are still rarely invited to take full control over aspects of treatment” (Salmon & Hall, 2004, p. 53). But how can they when they do not have the knowledge, expertise, and education to make informed clinical decisions? Patients do not even have control over their own digital health records (further disempowering them) according to Ebeling (2019). This raises questions about the full scope of informed consent in healthcare including: What level of information do patients need to be considered informed? and who decides this? This is where the embodied knowledges of patients must be valued by health professionals.
Finally, the results of this study support previous research which asserts that health professionals and health researchers engage in ongoing reflexive practice and critical self-awareness to effectively challenge their implicit and explicit biases and improve equity (Baarts et al., 2000). Autoethnographic accounts of illness in health research can contribute important perspectives and voices to the academic literature which can advance our understanding of various diseases and the impact on human health and well-being. This research can advance knowledge on patients’ experiences with symptom-persistent Lyme disease and chronic pain more broadly.
Conclusions
In this autoethnographic study, I have demonstrated reflexivity, vulnerability, and use of self by exploring my self-experiences of chronic illness (symptom-persistent Lyme disease) while holding co-occurring identities as a researcher and health professional. I recognize that my entire self-identity is greater than the sum of any one part. Uncovering this gestalt was critical in my choice of topic and research methodology—I believe that all patients who encounter the healthcare system should be understood as whole persons with complex and multilayered identities. To accomplish this, healthcare providers would benefit from awareness of intersectionality (Crenshaw, 1989, 1991) and the social determinants of health (World Health Organization, 2008). This research contributes the voice of one patient with chronic illness (symptom-persistent Lyme disease) and serves as a reminder that the patient should always be at the center in healthcare and health research. Through my self-experience with disease, I have intimately faced the precariousness of human health; every person is vulnerable to becoming sick and thus becoming a patient (despite best efforts to avoid illness). Holding this awareness allows for introspection and greater accountability in health research and healthcare more broadly. As Shahram (2023) argues, “we actually have to be and do differently, as individuals and as institutions of ‘higher learning’ to make meaningful progress towards health equity” (p. 2). I suggest health researchers and health professionals engage in ongoing reflexive practice. Finally, autoethnography as a methodology can add value and depth to health research. My perspective as a researcher and patient offers a unique contribution to current knowledge on experiences of chronic illness.
Footnotes
Acknowledgments
I am very grateful to Dr. Shannon Moore, Dr. Christine Tardif-Williams, and Dr. Dawn Trussell for providing feedback, supervision, and support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.