
Abstract
Little is known about the experiences of frontline professionals in Kazakhstan. Although studies of frontline workers have been conducted worldwide, it is imperative that caution should be exercised when extrapolating findings from disparate societies and generalizing them to Central Asian countries. As such, the purpose of this study was to explore and describe the firsthand experiences, perceptions, and knowledge gained from the experience of Kazakh frontline physicians and nurses during the COVID-19 pandemic. An exploratory-descriptive qualitative (EDQ) study was conducted over the course of a year in COVID-19 hospitals in Kazakhstan, with physicians (n = 23) and nurses (n = 7). Each participant was interviewed three times between May 2021 and May 2022. Braun and Clarke’s six-step method was used for the thematic analysis. Three overarching themes and subthemes were identified: (1) Longitudinal Journey (“Nobody knew, nobody understood, nobody was ready”; “It’s just life”); (2) Facets of Professionalism (“In my lifetime this is something unique”; “Who else if not us”; “We survived the war and the enemy”); and (3) Facets of Resilience (“God’s providence”; “A good word heals too”). In light of the lack of research that has previously been conducted in Kazakhstan, the results of this study offer important new insight into the experiences of medical professionals during the COVID-19 epidemic.
Keywords
Introduction
When the COVID-19 pandemic hit, Kazakhstan’s healthcare system was already very fragmented. Since December 26, 1991, when the Soviet Union ceased to exist as a sovereign state, Kazakhstan became an internationally recognized independent state, and with the new Constitution of Kazakhstan officially ratified on January 28, 1993, Kazakhstan has made significant efforts to revamp its post-Soviet health system. The National Programme for Health Care and Development 2005–2010 and the State Health Care Development Programme for 2011–2015 “Salamatty Kazakhstan” were both developed in the 2000s and represent substantial reform initiatives.
However, and despite substantial progress in recent years, the country still faces major challenges, such as an inequitable distribution of financial resources across regions, inconsistent use of medical services, and varying health indices. Even though there have been efforts to raise the quality of service, Kazakhstan’s healthcare system still has a way to go in terms of accessibility, equity, and efficiency (OECD Reviews of Health Systems: Kazakhstan 2018; OECD, 2018). Furthermore, little is known about Kazakhstanis’ beliefs on mental illness because so little research has been conducted in the subject of mental health. Hence, assessing and comprehending Kazakhstani frontline workers’ attitudes toward mental health during a pandemic is crucial.
The pandemic posed problems to the already struggling healthcare system of Kazakhstan (Kitamura et al., 2022). The lack of medical personnel, the lack of preparedness, and the lack of knowledge about the coronavirus caused a pervasive sense of helplessness and fear among Kazakhstani frontline workers. At first, there was not enough personal protective equipment (PPE), and frontline workers did not know how to use them. Subsequently, incidents of occupational exposure were reported, and frontline workers were inevitably infected (Kitamura et al., 2022). With the steady rise of new cases throughout 2020/21, the primary healthcare service in Kazakhstan was exponentially burdened. What would normally have been “essential” healthcare services, such as planned hospitalizations and healthcare for chronic illnesses, were halted as COVID-19 became the priority (Menlibayeva et al., 2022).
Although there is consistent evidence of a rise in symptoms of anxiety, depression, insomnia, and psychological distress among frontline workers during the COVID-19, there is a lack of published data on frontline workers in Kazakhstan during the COVID-19 pandemic (Lai et al., 2020; Wańkowicz et al., 2020).
Given the variability of healthcare services in Kazakhstan and the extent to which the pandemic exacerbated this, it is important to examine the experiences of Kazakh frontline workers, especially since this may not be the last pandemic and there is need to be prepared for future challenges.
Aim and Objectives
The purpose of this study was to explore and describe the firsthand experiences, perceptions, and knowledge gained from the experience of Kazakh frontline professionals, during the COVID-19 pandemic over the course of one year.
Methods
Study Design
This study used an exploratory-descriptive qualitative (EDQ) design. EDQ has been recognized as a useful theoretical framework for investigating under-researched facets of health research (Hunter et al., 2019).
Study Setting and Study Participants
In Kazakhstan, the first cases of the COVID-19 infection were confirmed on March 13, 2020, immediately followed by a nationwide state of emergency declared on March 16, 2020, that lasted until mid-April 2020. Following that, however, different lockdown and quarantine measures were still strictly imposed and remained in most parts of the country with these restrictive measures later on alternating between being re-established and eased. Throughout Kazakhstan, several hospitals were designated as COVID-19-specific facilities.
Twenty-three frontline physicians and seven nurses (total 30 participants) working in these main COVID-19 facilities throughout the country were recruited for this study. Participants were recruited from a preceding large-scale online quantitative survey examining the mental health experiences of Kazakhstani frontline HCWs during the pandemic. After completing the anonymized survey, participants were invited to forward their contact details to the research team to indicate interest in participation.
Inclusion Criteria/Exclusion Criteria
Physicians and nurses who worked at the frontline during the COVID-19 pandemic, were aged over 18, and were able to converse in Russian and/or Kazakh were eligible for inclusion. The exclusion criteria for this study included being <18 years old and not having direct contact with COVID-19 patients.
Data Collection Procedure
Three interviews were planned for each participant. Our aim was to repeatedly interview the participants using serial interviewing (26 May 2021–23 May 2022), to investigate how their experiences and perceptions changed and/or varied over time considering the rapid evolution of the pandemic situation. Change over time may indicate it is not that the interviewees themselves change but rather that various circumstances highlight different facets of their experiences or perspectives. In using serial interviewing, we believe that the researcher establishes familiarity and trust via repeated interactions, is enabled to investigate a variety of important subjects from many perspectives, examines various dimensions of participants’ experiences, and gains knowledge from incidents that occur while conducting the interviews.
We made a practical decision regarding the interview time points considering the changing situation in hospitals in Kazakhstan with regard to the pandemic and the length of the funding for the project. We decided upon three time points with a minimum of four months between each time point (T1, T2, and T3). In contrast to the longitudinal qualitative research (LQR) in the social sciences, where issues such as identity changes from childhood to adulthood are studied for years, many studies involving patients’ health only last a year or two at the most (Calman et al., 2013).
Semi-Structured Interviews
The initial (T1) topic guide and the interview schedule developed by the research team were inspired by a priori topics from the existing literature and previous research and included the following preliminary topics and themes: frontline challenging events; exposure to treating COVID patients and working circumstances; aspects of feeling prepared for the pandemic; attitude to work, job role, and professional values; patterns of emotions and feelings; support, resilience, and coping; positive experiences and self-reflexive thoughts; transforming experiences and insights; changes after one year; and concerns and needs.
With experiences from the earlier interviews noted, topics addressed in the subsequent interviews (T2 and T3) included questions and probes, such as “How have you been feeling emotionally these past months?”, “How are you feeling now?”, “What has changed since the last interview?”, “How has it changed?”, “How have your feelings changed?”, “How have things changed at work within this period?”, “How did the situation change?”, “How does coping change?”, “How do you manage this change?”, “Do you feel adequately supported within your workplace?”, “Do you feel your needs are being considered?”, “Looking back, what support do you feel you need for your emotional well-being?”, “Did you seek psychological support, and from whom?”, and “What have you done so far to try to stay psychologically well?”.
In serial interviewing, the goal was to keep focus on longitudinal elements and track changes in each participant’s experiences. To prepare for the next interview and to cross-check, what prior points merit follow-up, and what new material or questions to offer, the interviewer reviewed transcripts and notes from previous interactions in order to prepare for each session.
A short summary was written with key issues to consider in each subsequent T2 and T3 interviews, which started by providing a short summary identified prior to the session that each participant can reflect upon before moving on. Thus, capturing and assessing themes for the presence in the subsequent interviews as well as taking a moment to discuss and reflect on such interview summaries with each study participant contributed to the credibility of data focusing on changes over time. Thus, such a systematic approach enabled us to analyze changes and transitions across three time points within each case and between cases.
To begin, framing questions were centered on the contexts and conditions that affect changes considering the shifting conditions inside of COVID-19 hospitals. These questions typically generated descriptive information regarding the types of changes that have taken place, such as questions about PPE, management styles, number of COVID-19 beds, and so on, after which the researcher was able to dig further into the “experience” of the participants by asking more probing questions, such as “How is this affecting you.” With the use of these queries, the researcher was then able to analyze (and interpret) the participants’ perspectives in “these changing pandemic times” at a deeper level.
One of two researchers conducted each interview remotely. Both interviewers are Kazakh natives with extensive expertise conducting qualitative interviews in both Russian and Kazakh. One has a master’s degree in public health and is pursuing a doctorate in global health, while the other is a professional physician from Kazakhstan with a master’s degree in public health. For consistency, each subject was interviewed by the same researcher at all three time points. An English-speaking assistant professor of behavioral medicine completed the research team. The entire team participated in the analysis. The entire team consists of women.
Analysis
Thematic analysis, based on the six-stage, step-by-step methodology of Braun and Clarke (2006), was selected as the method of data analysis for this EDQ study.
The datasets are extensive and intricate. It was challenging to do in-depth analyses of each interview before moving on to the next, a difficulty that has been highlighted in previous research (Wray et al., 2007). In this case, we opted to first analyze and summarize the interview so that the future interview might begin with a repeat of what was discussed earlier. This more targeted interviewing technique limited the amount of data collected, making it simpler to evaluate and less intimidating for the researcher. Typically, follow-up interviews were shorter than the initial interview, lasting between 20 and 30 minutes. This helped the subject and the researcher focus on longitudinal elements like what has changed since the prior time and why this happened.
To ensure rigor, transcripts were prepared by the interviewer, and the entire study team validated them. Once the codebook was generated for all interviews at each data collection point, themes and subthemes were further developed. Moving unrestrictedly across the transcripts of interviews collected over three time points helped to gain a thorough understanding of the participant account(s), analyze interviewees’ perspectives, and track changes within each individual case as well as across cases over different time periods. All data were examined by the whole data analysis team. Regular team meetings were organized to share individual interpretations of participant accounts and reach a consensus regarding themes and subthemes and their relationships via rigorous discussions.
Results
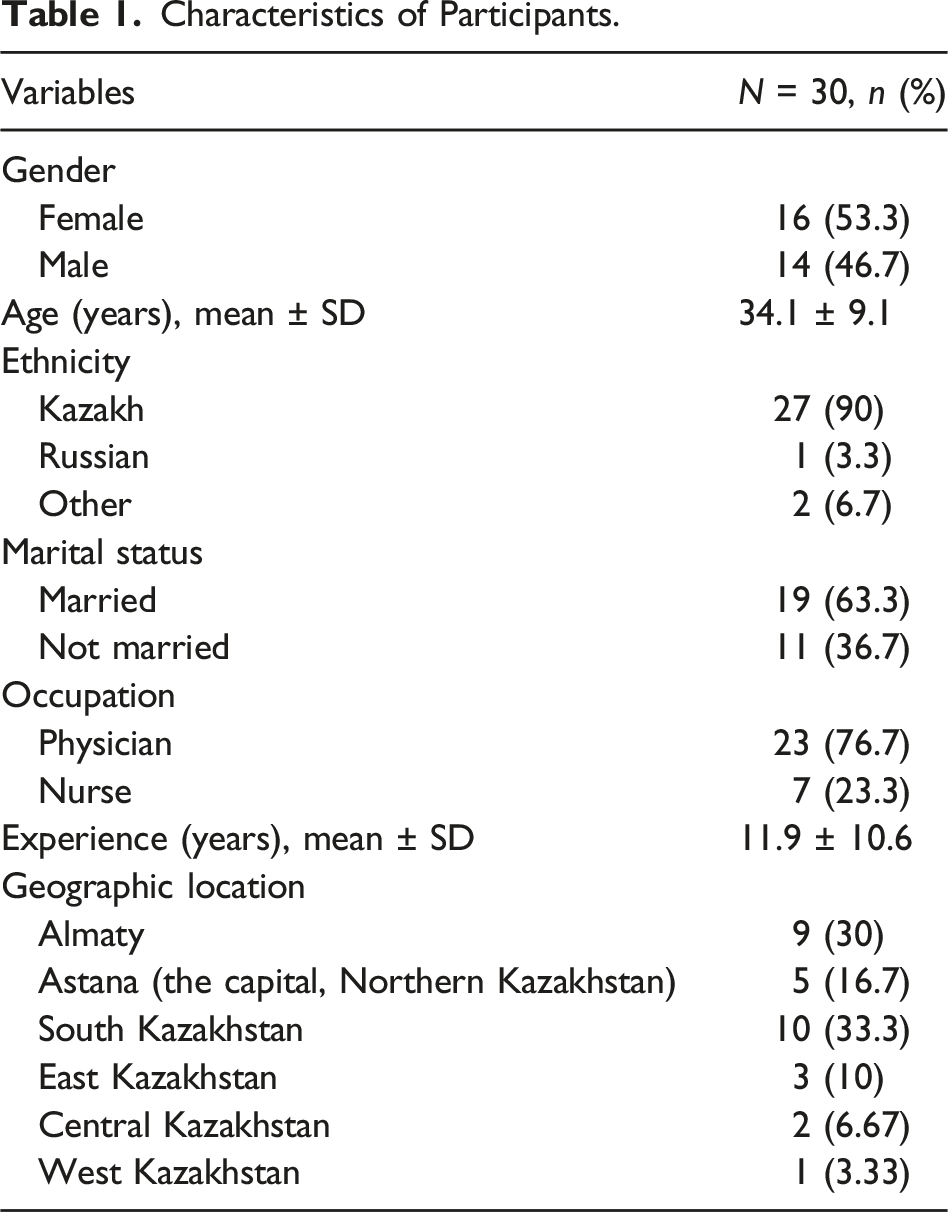
Twenty-three frontline physicians and seven nurses (total 30) participated in this EDQ study. In Kazakhstan, most responsibility for patients lies with doctors rather than nurses, which could explain the higher prevalence of physicians than nurses in our study. Participants were frontline professionals of different specialties, for example, cardiac surgeon, general surgeon, CAT MR-imaging radiologist, junior and senior nurses, intensive care physicians, pulmonologist, anaesthesiologists, neonatologist, paediatrician, infectious disease doctors, neurosurgeons, and general practitioners.
Characteristics of Participants.
Theme 1: Longitudinal Journey
The participants’ narratives suggested that the early stages of the COVID-19 pandemic were associated with heightened levels of distress, as well as depression and anxiety symptoms. Participants spoke retrospectively about reduced sleep, increased irritation, or hostility, crying, self-harm, sensitivity to shock, and a desire to avoid work. Everyone had some kind of terrible depression. At the end of the year when “everyone” was dying, I was so depressed, I think I even wanted to commit suicide, I was so sick of it. I pushed myself all the time like “go-go-go,” but I no longer wanted to go there, and it is like I am forced to. (Doctor 8, second time point) I was isolated from family and friends. I could only think about the patients and the work. The patients were so severe that I had a depressive state. (Nurse 2, first time point)
Subtheme 1.1: “Nobody Knew, Nobody Understood, Nobody Was Ready” (Doctor 19, First Time Point)
Participants’ recollections of the beginning of the pandemic were accompanied by a wide range of sentiments, including fear about being infected, dying, infecting loved ones, losing patients, the unknown, helplessness, a lack of resources, and an inability to stem the spread of the disease. Not feeling psychologically prepared at the beginning; it seems like something which is far away, something which will not reach us, until one of the relatives gets infected; many colleagues passed away .... (Doctor 15, first time point) Helpless, due to a rapid inflow of patients and a lack of staff, they literally died ... They might have perished in the future ... but they died here ... in our hands ... right here ... when you lacked time. There was a moment when I was connecting one patient to a ventilator and the other patient began dying. I had to choose. That was a dilemma, and this creates a feeling of incompetence. (Doctor 23, first time point)
Subtheme 1.2: “It’s Just Life” (Nurse 5, First Time Point)
A change in perspective emerged after struggling through the first year of the pandemic. The toll of the epidemic contributed to a worsening of mental health at the outset, but participants remarked about emerging more resilient and feeling more emotionally and practically prepared for the workplace problems caused by the pandemic. Not feeling emotionally prepared in 2019-2020, but more prepared now. (Doctor 23, first time point) The uncertainty scared in the beginning, but then we got used to it. Yes, got used to it. (Nurse 2, second time point)
Although not verbalized in the interviews, participants’ feelings at this point were perhaps bolstered by the fact that effective March 1, 2021, Kazakhstan relaxed its quarantine policies (Kazinform, 2021), and WHO had delivered medical supplies to Kazakhstan with financial support from the European Union (EU) (WHO delivers EU-funded medical supplies to Kazakhstan to protect healthcare workers against COVID-19, 2021).
Participants’ change in perspective was described as resignation to the circumstances: There is resignation with this, that is, earlier it was not such resignation. I wanted to fight to the end for a patient. To prove something ... Maybe to try some more medications, etc., etc. Now you are already resign[ed] this situation and say: “Yes, this patient will probably pass away.” So somehow ... probably wrong, cynicism has appeared. (Doctor 14, second time point)
Participants also talked about no longer being as afraid of contracting the infection in the hospital because “people can get infected anywhere…” (Doctor 10, second time point) and “if you are meant to get infected with COVID-19, you anyways will, no matter where you are, at home or outside” (Doctor 2, first time point). They spoke about how following the safety measures reduces their perception of risk. We study all orders, the Sanitary Rules and Norms, all requirements. We try to protect ourselves from this infection. We follow all the rules about a clean zone and a dirty zone as well as about changing clothes, sanitation, as it should be, because we are professionals and also need to avoid getting infected, to protect our loved ones, our family members. (Doctor 12, first time point)
By the third round of interviews in mid-2022, the pandemic was far from over in Kazakhstan; the Healthcare Ministry initially projected daily positive cases to reach 13,000 after a new wave of illnesses (Vlast.kz, 2022). Nonetheless, as the number of confirmed cases rose, the Ministry raised its daily infection estimate to 17,500 and advised Kazakhstanis to wear masks and to avoid holding or attending large-scale recreational events, social gatherings, personal visits, and hosting guests (Vlast.kz, 2022). Interestingly, despite the situation with the pandemic, participants did not speak of the uncertainty and fears that had predominated at the start of the pandemic; instead, participants spoke of having grown accustomed to the pandemic, with a better understanding of the infection and treatment tactics. By this point, acceptance had become a recurring topic. Difficulties do and will happen with people, with doctors. We simply do our work and have to continue doing our best, strive, adapt, and learn quickly … and despite the hard work, poor sleep, stress and missing family gatherings, I try to benefit from it. I think it is worth it and this is what people need now. (Doctor 5, third time point)
Theme 2: Facets of Professionalism
Participants’ experiences of working with the pandemic over time not only led to “acceptance” of COVID-19 but also boosted their own sense of professional obligation and motivated a desire to study as much as they possibly could about the virus and the variants. Their newly acquired knowledge had a direct impact on how they saw professional duties. And we among ourselves after reading a lot of literature on COVID-19, aseptic and antiseptic, we began to draw our own lines, where to pass, where the red zone to-be–lined, where they will pass, where employees would change their clothes. (Doctor 1, second time point)
Subtheme 2.1: “In My Lifetime This Is Something Unique”
In fact, several of the respondents used phrases like “I felt professional excitement” (Doctor 6, first time point) and “It was exciting to me” (Doctor 1, second time point) to describe their level of interest. They described how, in the face of the professional challenge posed by the pandemic, they adapted to their new normal as they gained more clinical experience and knowledge of COVID-19. I was just curious, first of all, as a doctor, and then I developed my own treatment tactics, diagnostic tactics, and tactics for interrelationships in that field online. And it was just a very interesting experience for me as a doctor. (Doctor 5, third time point)
Subtheme 2.2: “Who Else if Not Us” (Doctor 9, Second Time Point)
Even before this epidemic, healthcare professionals in Kazakhstan were struggling with an already very fragmented healthcare system. We are used to working in this regime, we are used to working with seriously ill patients, the only thing that is worthy of note is the fact that it was morally difficult, of course we were tired, of course there could be pressure somewhere, but to say that directly ... well, yes, in general, several people got sick, nursing staff actually all got sick, doctors got sick, but I had suffered all this before. (Doctor 12, first time point)
Participants described how the COVID-19 pandemic increased their workload and time commitment, requiring them to juggle the shifting demands of their job while also prioritizing the health of their own loved ones. Oh, there were tough conditions. We literally lived there 24/7. There were very tough conditions, we lived in the hospital, days and nights, basically, we did not have a rest. (Nurse 7, third time point)
Participants, on the other hand, stressed the inherent responsibility that comes with their profession and indicated a true desire to fulfil their professional obligation and aid those in need. This is the doctor’s mindset … Growing a seed of humanity and taking responsibility for the life and health of others. (Doctor 4, third time point)
In other words, the participants believed that they had a higher level of responsibility than the ordinary person because of the nature of their profession. They described how medical professionals have an even greater duty to help because of the special knowledge and skill they hold. Most participants said they either volunteered to the frontline and/or worked extra hours and took on extra responsibility during the pandemic because they wanted to, not because they had to.
There was one participant who stood out as an exception; this person objected to the use of what they perceived as coercive management methods that lacked ethical standards. It was terrible, we were outraged, they told me, no one will go on vacation, no one will go on leave of absence, even on sick leave, only pregnant women leave from 12 weeks, and before 12 weeks they said—it’s desirable to have an abortion, all doctors, all of them. (Doctor 8, first time point)
This individual ultimately adjusted and stated as much in a follow-up interview: Somehow the COVID-19 situation stabilized, everyone no longer began to pay attention to it, that’s when I calmed down. People became indifferent to COVID-19. Well, come what may! (Doctor 8, third time point)
Subtheme 2.3: “We Survived the War and the Enemy” (Doctor 18, Third Time Point)
Many of the participants, echoing the preceding sentiment of inherent responsibility because of their professional status, equated the pandemic scenario to that of war, portraying themselves as soldiers whose duty is to protect the motherland: “It was mostly considered as a war, and we were soldiers who should protect their motherland; it was our duty” (Nurse 2, first time point). I understood that this was our moment and who else except us. It was considered as a war mostly, and we were soldiers who should protect their motherland, it was our duty. (Doctor 10, first time point)
Theme 3: Facets of Resilience
Subtheme 3.1: “God’s Providence”
Religion and faith were fundamental to many participants’ resilience, and they spoke of how their belief helped them accept the situation, not be afraid of contracting the virus, and, to some extent, release the burden of responsibility for what was going on around them in terms of patient deaths. Furthermore, having inner faith enabled them to find some respite and inner fortitude to work under pressure while also not being fearful of acquiring the virus. First of all, you have Allah first, Allah sees everything, Allah knows everything. If I’m going to get sick, I will get sick. If that is not my destiny, I won’t get sick. (Nurse 6, second time point)
Subtheme 3.2: “A Good Word Heals Too” (Doctor 24, Third Time Point)
Family and friends were cited frequently as sources of strength. Participants described how family and friends were able to provide both practical and emotional support by providing meals or simply being there to listen and show empathy. They support me with warm words. As I told you before, I had three children, they need clothes, food and care, my relatives helped me to provide care to my children. (Nurse 5, third time point)
Likewise, a consistent theme across all interviews was the value placed on support from colleagues: “If the team is good, you can work in the most difficult conditions” (Doctor 24, third time point). Participants also stated that they made every effort to provide a helpful, reassuring, and encouraging environment for their coworkers during this trying time. Well, we had employees when they were stressed. They’d come off their shift straight and they’d cried to me. They were crying, screaming. They were in tears. And I had to deal with them gently. (Nurse 2, first time point)
In terms of social recognition and appreciation, participants on the one hand expressed their gratitude for support from the public, but they also spoke about wanting to receive more social recognition, acknowledgment, and appreciation for their hard work. I treated lots of patients in the ICU, worked on the frontline and achieved big results, and no one expressed gratitude on the Doctor’s Day. Others received all the medals and certificates, while we simply continued working. We would be pleased to receive at least a certificate, not even medals, which we deserved… (Doctor 10, first time point)
In terms of availability of psychological support, a few participants described there being a psychologist available for patients primarily and staff, though this psychological support was perceived to be of little help. This (counselling psychology) is not practiced in Kazakhstan. I just haven’t come across it and I can’t say for sure if it would have helped me, but I think it would have. I have not met (psychologists for HCWs) in Kazakhstan, but I have seen psychologists for patients in some private clinics. (Doctor 17, third time point) I do not know that there was such a psychological support. (Nurse 5, third time point)
Few individuals acknowledged having access to a psychologist, and those who did described the psychologist’s primary role as being to assist the patients. There was a general aversion to receiving psychological support at work. However, one nurse participant emphasized how access to mental health treatment could be beneficial, and two others admitted to getting help from other sources. We are doctors. We are in fact practical; we are the psychologists for ourselves, and we do not need such conversations. (Doctor 12, third time point) I am going to therapy because … I haven’t yet released/accepted the situation. People do not pay a lot of attention to their mental wellbeing. Local people are not used to share/tell everything, but it is indeed helpful. (Nurse 7, third time point)
Discussion
This study sought to explore and describe the firsthand experiences, perceptions, and knowledge gained from the experience of Kazakh frontline physicians and nurses during the COVID-19 pandemic.
While participants in our longitudinal study initially reported negative effects on their mental health and work environments, at the study’s end, their stories reflected acceptance, resignation, and resilience in the face of difficulties.
Umbetkulova et al. (2023) reviewed studies on the mental health consequences of the pandemic on healthcare workers (HCWs). Long-term impacts of pandemics on HCWs’ mental health symptoms were found to be inconsistent; however, the review did reveal a wide variety of relationships between risk and resilience factors and changes in HCWs’ psychological well-being over time. There was a lack of conclusive evidence suggesting long-term harm to HCWs. Our results are consistent with this finding; initially, participants in this study spoke retrospectively of being affected by the pandemic in much the same way as reported by frontline workers around the world (Liang et al., 2020; Santabárbara et al., 2021). When recalling their experiences at the beginning of the pandemic and throughout the first year, the lack of preparedness and the lack of knowledge about the COVID-19 infection initially caused a pervasive sense of helplessness and fear among the participants. Furthermore, participants spoke of experiencing symptoms of anxiety, depression, insomnia, and psychological distress, but as time passed following the COVID outbreak, over the course of the year, there was a noticeable shift in our participants mindset and attitudes toward the challenging work conditions of the pandemic, and their narratives reflected positive psychological adjustment to the situation and conveyed a sense of them developing resilience and an ability to cope with their personal and work-related conditions.
Interestingly, our findings show that rather than personal individual traits or support from workplace interventions underlying participants’ coping and resilience, participants’ drive to overcome adversity arose from their professional identity and aspirations to the highest professional ideals. Thus, the concept of serving for the common good and references to “a doctor’s duty” was frequently expressed in participants’ narratives. This theme is echoed in other studies, too, in which HCWs have been found to regard their work during the pandemic as their moral duty, professional obligation, and an honor to treat patients and serve the country, sometimes akin to soldiers (Kwaghe et al., 2021; Liu et al., 2020; Rao et al., 2021; Saleem et al., 2021; Su et al., 2007).
The “fighting a war” rhetoric was a strong theme in this study, and although it echoed in numerous existing studies (Kwaghe et al., 2021; Liu et al., 2020; Rao et al., 2021; Saleem et al., 2021), the “fighting for the motherland” rhetoric is perhaps characteristic of Kazakhstani post-Soviet identity.
The importance placed on social networks and family, friends, and colleagues’ support by our participants is in line with the findings of other researchers (Banerjee et al., 2021; Muzyamba et al., 2021; Rao et al., 2021), but unique to this study is the reliance on these sources to the exclusion of the need for psychological support. Participants were not convinced of the personal need for workplace support or interventions.
A plausible explanation may be the historical lack of focus on mental health in Kazakhstan. It is important to reiterate that currently in Kazakhstan counseling is not a recognized profession, so the concept of “workplace counseling/psychological support” is unfamiliar to participants. As such, unlike some Western countries which have incorporated psychological interventions such as workplace counseling into their protocols for managing the COVID-19 pandemic, this has not been the case in Kazakhstan. Throughout Kazakhstan, mental healthcare is not without its difficulties; however, reform is currently underway to improve the overall situation (Tuleussarinova & Altybayeva, 2020).
During the Soviet era, the religious tradition and heritage in Kazakhstan were marginalized. Since independence, Kazakhstan has been a secular nation where people are free to choose and practice their own religion. Religion as a way of coping was therefore an interesting theme, with most participants explaining they had no need of psychological support because their faith in God was sufficient to cope with challenges. Likewise, examples of religious coping were shown in several other studies conducted in Pakistan and Indonesia (Munawar & Choudhry, 2021; Saleem et al., 2021; Tosepu et al., 2021). This theme and religiosity may be explained by the fact that many Muslims in Kazakhstan have progressively resumed their religious activities. In fact, currently, a sizable portion of the Kazakh population identifies as Muslim. There are 3834 recognized religious organizations in Kazakhstan, with 2695 (or 70%) being Islamic and most likely belonging to the Sunni branch, as reported by the Committee on Religious Affairs of the Ministry of Information and Social Development of Kazakhstan.
The next theme of practicing gratitude and appreciation may also be related to a resurgence of Islam practices and beliefs in Kazakhstan, but it is also a finding that has been reported in research from the United Kingdom, where HCWs shared feeling grateful and being comforted by numerous signs of appreciation shown by the public (Liberati et al., 2021; Padros et al., 2020). Our participants spoke more about the importance of practicing gratitude and appreciation from within rather than needing to see it given from external sources; this does not mean our participants were not responsive to the importance of public and or organizational recognition, acknowledgment, and appreciation of their work and sacrifices while “fighting the war!” In fact, they felt gratitude from external sources was lacking.
Strengths and Limitations
There are some strengths and limitations to the given study. In retrospect, a limitation is that we did not collect information about participants’ religious identity.
While sex distribution of our sample is relatively equal, there were more physicians than nurses among participants. Also, to some extent, there could be self-selection bias as interviewees were among those who volunteered to be contacted upon completing a quantitative survey. The effects of this were addressed and, hopefully, overcome with the following means: analyzing each interview before moving on to the next one; developing preliminary codes, ideas, insights, and themes; providing a short summary from the last interview to allow participants to reflect, assess, and interpret data during the follow-up interviews; and, capturing experiences over time.
Conclusion
Participants began our interviews by describing the negative impact the pandemic has had on their working conditions and mental health. However, at the end, participants’ stories reflected a sense of acceptance, resignation, and/or resilience. Participants described the value of maintaining a positive mental attitude and professional frame of mind in order to better manage stresses faced during the pandemic. It is important to reiterate here that Kazakhstani mental healthcare system does not entail the presence of counselors, as distinguished from Westernized countries. Thus, in contrast to the Western system of workplace counseling practices and despite the government’s continuous efforts, the system of psychological support, access, and coverage of psychosocial interventions for healthcare professionals in Kazakhstan still needs much improvement.
Given the existing research gap in Kazakhstan, the findings presented in this study provide an important insight into the experiences of physicians and nurses, by describing the firsthand experiences, perceptions, and knowledge gained from the experience of being frontline workers during the COVID-19 pandemic.
Footnotes
Acknowledgments
We wish to acknowledge all the frontline healthcare workers who dedicated their time to take part in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work (project’s number: SOM2020010) was supported by the funding source within Nazarbayev University and funded by the Faculty-Development Research Grant Program (funder project reference: 280720FD1906).
Ethical Statement
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.