
Abstract
Empathy is one of the important components in the patient–nurse relationship. The aim of the study was to explain the culture of empathic care in intensive care unit (ICU) nurses. The present focused ethnographic study was conducted in the cardiac surgery ICU in Tehran. Three methods of observation, interview, and review of existing documents were used to collect data. From data analysis, three cultural models, “Predominance of task-based care over emotion-based care,” “Empathy and lack of empathy, two ends of the spectrum of the nurse–patient relationship,” and “Empathy, an interactive and reciprocal process,” were extracted. The results showed that empathy creates a caring environment where nurses not only understand their patients but also relate to them, and both are affected by it. Policymakers should consider removing barriers as a means of empowering nurses to provide empathic care.
Introduction
Clinical nursing is associated with complex interactions that represents the nurse–patient relationship, and in this complex form of communication, each person brings his/her historical and cultural background to the nursing situation, so that the cognitive, emotional, and attitudinal components of each person are revealed (Sumner, 2001). Studies have shown that in situations where nurses and patients communicate and understand each other in a better way, the patient’s quality of care increases and the cost of care decreases (Khodabakhsh & Mansoori, 2011). However, the quality of the nurse–patient relationship has been reported to be poor in many studies (Gilmartin & Wright, 2008; Jangland et al., 2009; McCabe, 2004), and unfortunately patients complain about a lack of appropriate communication and a lack of attention and empathy and friendly communication from nurses (McCabe, 2004).
Empathy means “standing in the patient’s shoes” (Unit, 2006), and it has behavioral, moral, emotional, cognitive, and relational components (receiving empathy from the client) (Morse et al., 1996). Emotional empathy is higher and more effective than sympathy and compassion (Khodabakhsh & Mansoori, 2011). Empathy clearly involves imaginative involvement, and although both sympathy and compassion may be mediated by imaginative involvement, these terms typically refer to reactive and unreflective responses whose characteristics do not require psychological acumen. Empathy is a skilled response, whereas sympathy and compassion are reactive (Maxwell, 2008).
Integrating empathy into caregiving leads to supportive functioning and assistive behaviors (Bowers et al., 2001). First, emotional involvement leads to the caregiver’s desire to attend to the client’s feelings and needs, increasing the quality of their relationship and the quality of care provided, and finally, the interpersonal interaction between the caregiver and the client leads to the formation of “empathic care.” Empathic care is a multidimensional phenomenon that includes emotions as well as behaviors (Lamberton et al., 2015).
The consensus in the literature is that empathy can help patients to understand and cope with the disease and help the provider to respond more accurately to the patient’s needs, thus indirectly leading to improved outcomes (Neumann et al., 2009), patient satisfaction, compliance with treatment, reduction of anxiety and stress, better diagnosis and outcomes, and also patient empowerment (Derksen et al., 2013; Hojat et al., 2009; Lelorain et al., 2012; Menendez et al., 2015; Rakel et al., 2009; Uitterhoeve et al., 2009). Empathy can improve the nurse’s relationship with the patient and family and help the nurse gather more accurate information and incorporate it into effective patient care (Moghaddasian et al., 2013). However, a lack or absence of empathy can lead to disruptions in the diagnosis, treatment, and care process (Williams et al., 2012). Folbre describes empathy as an integral part of quality care for adults, arguing that it is the empathic component of care that essentially distinguishes it from other service work (Folbre, 2012). In a 2018 study, Yang also found that patients with lung cancer who were cared for by nurses with higher empathy had greater cellular immunity (Yang et al., 2018).
One area where empathy and empathic care are essential is the intensive care unit (ICU) (Koukouli et al., 2018). In this ward, patients are mechanically ventilated (Hoonakker et al., 2011) and receive tranquillizers (Jakimowicz & Perry, 2015), which makes it impossible for patients to communicate verbally with ward staff and relatives (Hoonakker et al., 2011) and it is not an easy task for nurses to perceive patients’ feelings and needs (Shalaby et al., 2018). Therefore, communication with patients is a challenge for ICU nurses (Hoonakker et al., 2011). Thus, in this ward, empathy forms the core of the nurse–patient interaction and makes nurses to understand patients’ conditions, needs, and feelings when providing ICU care and to take steps to address them (Hoonakker et al., 2011).
However, the researchers believe that while there have been great advances in physical care in ICUs, holistic care, which includes the psychological care of patients, is being ignored (Loghmani et al., 2014). Although the empathic component of care is as important as the instrumental component in terms of overall quality of care, relatively little research has been conducted on the aspect of care delivery (Lamberton et al., 2015) and on nurses’ empathy in ICUs (Moghaddasian et al., 2013; Van Mol et al., 2015). Although qualitative approaches are invaluable for discovering conceptual areas or identifying the factors that strengthen or inhibit empathy, they have been very little used (Charlesworth & Foëx, 2016; Jones et al., 2016; Monks & Flynn, 2014; Strube et al., 2018). The phenomenon of empathy, more as a hidden concept, is extracted among other nursing concepts in the fields of communication, aesthetics in nursing, and nursing care (Banerjee et al., 2016; Díaz et al., 2015).
From the researcher’s perspective, personal and professional experiences during 10 years of working as an ICU nurse have highlighted the role of empathy in improving the quality of care and the need for analysis in different cultural contexts. While studies have shown that empathy can strengthen therapeutic relationships with patients, improve clinical outcomes, reduce burnout, and even reduce complaints against healthcare workers (Gleichgerrcht & Decety, 2013; Howick et al., 2018; Riess, 2010), it is necessary to consider the cultural contexts in which these observations are made (Eichbaum et al., 2022). As Atkins showed in his study, empathic responses to the emotional states of others, as a subcategory of the cultural context, can have different manifestations (Atkins et al., 2016). Okougha found in his study that communication needs and ways of expressing emotions differ in different cultures and rituals (Okougha & Tilki, 2010), and Kelly reported that empathy can be influenced by situational and cultural factors (Kelly, 2007).
According to studies, empathy depends on the cultural situation, so an interpersonal approach to the study of empathy requires recognition that such interactions take place within a larger socio-cultural context (Main et al., 2017). In this study, we aimed to find out what the culture of the ICU is in terms of providing empathic care and what factors contribute to the implementation of empathic care by ICU nurses. We also aimed to identify the factors that facilitate and hinder the implementation of empathic care by ICU nurses. To conduct this research, an inductive and flexible design was required to facilitate movement between emic (local/participant) and etic (foreign/researcher) perspectives; therefore, this study was designed using a qualitative method of focused ethnography (FE).
Focused ethnography allows researchers to explore cultural contexts that cannot be studied using traditional ethnographic methods (Wall, 2014) and allows the researcher to examine emic and etic perspectives to gain a deeper understanding of the target culture. Anthropological researchers use both perspectives to participate in experiences (Chen, 2010; Roper & Shapira, 2000).
Focused ethnography involves carefully observing the participant in a real place, asking questions to understand what is happening, and using other available sources of information to fully understand the people, place, and events in question. By collecting data in real places and using multiple sources of data and flexibility in sampling strategies, the research process leads to the discovery of cultural knowledge (Speziale et al., 2011). This method is usually concerned with a particular problem in a specific context and is carried out in a subculture. Focused ethnography is primarily used in practice-based disciplines, such as nursing, as a pragmatic and efficient way of capturing culturally specific perspectives and putting this understanding into practice (Wall, 2014). Given that this study focused on a specific issue, that is, the culture of empathic care, in a specific setting, that is, the ICU, and also on the relationship between nurses and patients, a focused ethnographic approach was the best method to guide us toward the aim and research question.
We aimed to explore the culture of empathic care among nurses in the ICU. Using a focused ethnographic study and the experiences of nurses in this unit, we tried to uncover unknown aspects of this phenomenon.
Methodology
This study was conducted in the cardiac surgery ICU of a teaching hospital in Tehran, Iran. The governmental nature of the hospital (due to the lack of specialized services for patients), the presence of a cardiac surgery ICU, obtaining university approval to conduct a study, the cooperation of hospital officials for the long-term presence of the researcher in the field, and better access to information were some of the reasons for choosing this hospital. The fact that there are both conscious and unconscious patients in the cardiac surgery ICU, and that the researcher wanted to observe the interaction and empathy of the participants with all types of patients, as well as the experience of cardiac surgery itself, led to the choice of this unit. Our study was approved by the Research Ethics Committee (approval number IR.IAU.TMU.REC.1400.069). Written informed consent was obtained from all participants prior to enrollment.
This ward has 12 active beds and each nurse is responsible for two or three patients on each shift. The nurses work in morning, evening, and night shifts. Nurses with more experience usually work in the morning shift. They come from different religious, ethnic, and linguistic backgrounds and have different levels of nursing competency and ICU working experience. The charge nurse or the shift manager assigns the nurses according to their competence and the condition of the patients.
The selection of participants in this study was not pre-determined and was adapted from the outset to the theoretical framework that underpinned this research. According to the purpose of the study, the main focus was on nurses, but as all actors in the field have a role in shaping the culture of empathic care in the ICU, the participants in this study included all informants in the field who were directly or indirectly involved in the care of patients. These included bachelor and master level nurses, patients, cardiac surgeons, anesthetists, and paramedics. The experience of the nurses ranged from newly recruited nurses to nurses with more than 20 years’ working experience. In total, there were 27 nurses, six nurse’s assistants, and one cardiac surgery registrar in the cardiac surgery ICU. Patients were admitted to the ICU after open heart surgery or were referred and readmitted to the ICU for postoperative complications. The most common procedures were CABG, AVR, MVR, and TVR.
Data were collected through observation, interviews, and review of available documents from November 2021 to March 2023 (with a total of 1500 hours of observation). The data collection process started with the presence of the researcher in the ward. Observations were made in different shifts (morning, evening, and night). Observations were made by purposefully observing events and the people involved and then making decisions based on these observations. Listening to the patient (to understand the patient’s feelings); explaining the procedure to the patient; standing next to the patient; describing the patient’s condition to the patient (gives the patient a sense of trust); taking measures to relieve pain, reduce anxiety and fear, and calm the patient down; touching the patient; smiling at the patient; saying something to make the patient feel better (Stavropoulou et al., 2020); providing clear information; being understandable and honest with the patient’s family; family members being with the patient; and family members meeting some of the patient’s needs (Koukouli et al., 2018) were examples of behaviors that were considered to be empathic toward the patient and the patient’s family.
In ethnographic studies, there is a continuum of observation as a complete observer, partial participant, observer as participant, and complete participant. In focused ethnography, the method of observation is often the type of observer as participant (Higginbottom et al., 2013). In this study, the researcher used a number of the above methods of observation to gain a better understanding of the phenomenon under study and mostly used participant observation. This gave the researcher the opportunity to closely observe the interactions between people and, if necessary, to question them to clarify their thinking and, if the patient was conscious, to observe the patient’s behavior and response. In addition to observing verbal behaviors, the researcher also tried to observe non-verbal behaviors.
In ethnographic studies, observations are made in a descriptive, focused, and selective way. The process of observation is not linear, but cyclical between descriptive, focused, and selective observation, and all three are interrelated (Roper & Shapira, 2000). Descriptive observations are made without a specific question (Speziale et al., 2011). They are followed by focused observations, which are derived from the questions the researcher asks during the initial descriptive observations, and finally by selective observations, which are based on the focused observations (Knoblauch, 2005).
In order to get a clear and accurate picture of the environment and what goes on in it, descriptive observations were made in this study to find out about the different parts of the ICU, the routines, and the current activities of the ICU. Examples of the descriptive questions asked of the researcher in this study are as follows: What are the parts of the cardiac surgery ICU? Who enters and leaves the unit? What are these people like in terms of education and clothing? What activities are carried out in the unit? What are the interactions between people in the unit?
Once the descriptive observations were completed, the focused observations were used. In line with the purpose of the study, the focused observations in the study process were derived from the questions that came to the researcher’s mind during the initial descriptive observations (Higginbottom et al., 2013). If the researcher had a question during the focused observation, he or she would be doing a selective observation. Selective observation usually focuses on a specific feature of the activity. For example, if the researcher had questions about how nurses dealt with an agitated patient, he or she would follow them to observe closely. If at the time of the interview some cases were raised where the researcher felt the need to confirm, selective observation was made. Observations continued until data saturation was reached. Saturation is when the research questions have been answered and it means the researcher can leave the field (Roper & Shapira, 2000). When necessary, the researcher also conducted informal interviews in the form of friendly conversations in line with the research objective.
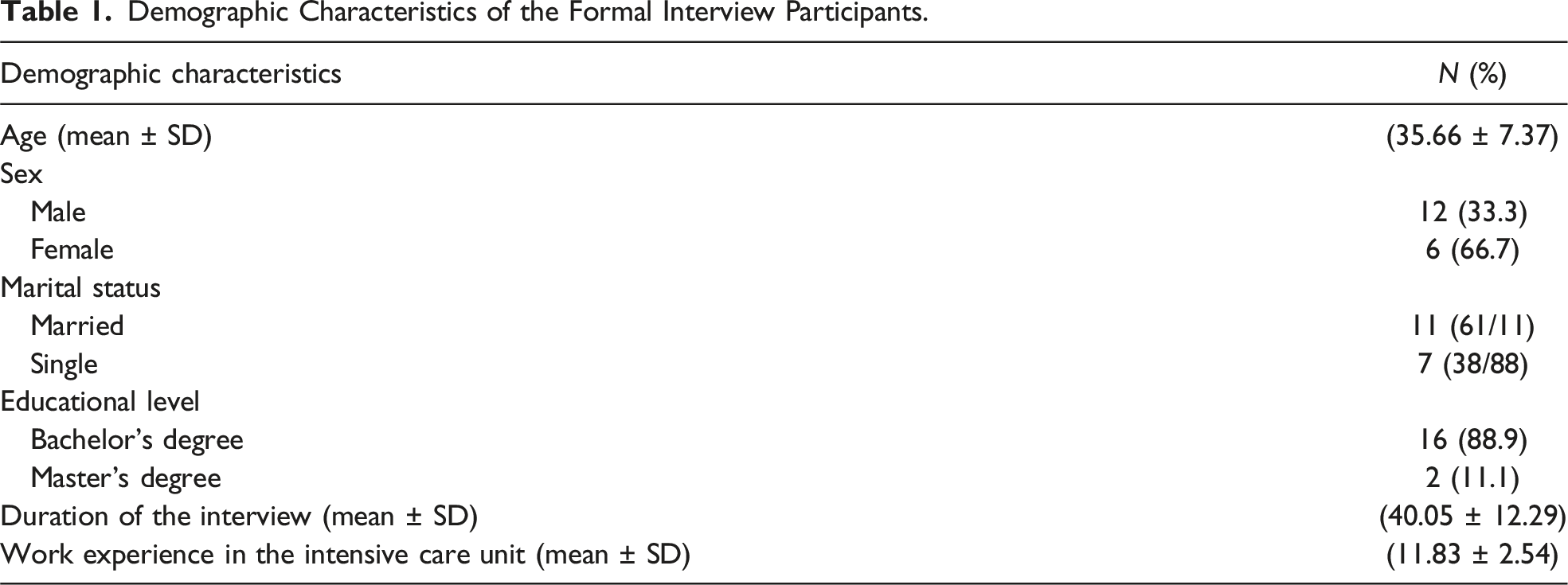
Demographic Characteristics of the Formal Interview Participants.
Evaluation of Study Rigor
Morse’s (2015) strategies were used to increase the validity of the study, including long-term presence, observation, and thick and rich description of the findings. To this end, the researcher used several strategies, including prolonged presence and interaction in the place; continuous observation and comparison; writing out comprehensive, accurate, and clear notes; thick and rich description; integration of data collection methods; searching for analysis of negative cases; and accurate recording and copying of participants’ statements in the stages of data collection and generation, data coding/analysis, and presentation of findings. In addition, once the initial general structure of themes and sub-themes emerged, the strength and stability of the data, the application of the findings at the bedside, and their appropriateness/relevance were reviewed, clarified, and audited by presenting these findings to a number of peers, participants, and external observers. In order to reduce the influence of her personal values, the researcher recorded his thoughts in a diary before the start of the study and during data collection and analysis. Reflexivity in qualitative research is one of the most important quality criteria and a basic requirement in all qualitative research, and it is particularly important in focused ethnography. It makes it possible to confirm the validity of the phenomena under study and is a form of validity called “reflexive accounting” in qualitative research (Cruz & Higginbottom, 2013). In relation to this characteristic, the researcher can clearly describe her historical and cultural background and how it has influenced the research.
Data Analysis
Data analysis was carried out concurrently with data collection. For this purpose, observations, conversations, and field documents were converted into fieldnotes, and recorded interviews were transcribed and analyzed using qualitative data organization software. Roper and Shapira’s (2000) analytical framework was then used to analyze the data: (1) Coding for descriptive labels: To carry out this step, the researcher transcribed all the fieldnotes and interviews word for word, and a separate text file was created for each interview. For better management, the data was entered into MAXQDA version 11 software. All observations and interview texts were read several times to gain a general understanding. The texts were then analyzed word by word, line by line, and paragraph by paragraph. The data was broken down into small pieces and words or groups of words were identified and coded. (2) Sorting for patterns: At this stage, similar codes were placed in a group or category called sub-sub-themes and then these concepts themselves were placed in a category according to similarity and formed sub-themes. From the combination of the sub-themes, the main themes were obtained. (3) Identification of outliers or negative cases: At this stage of the analysis, negative cases that did not correspond to the findings of the study were identified and taken into account in the data analysis. (4) Generalizing with constructs and theories: At this stage, the findings were related to and enriched by other studies and theories. To generalize the findings, the link between participants’ internal meanings (emic) and insights and the researcher’s mental interpretations (etic) of these meanings was established. Finally, the findings were compared with existing studies and theories. (5) Memoing including reflective remarks: Memos are the researcher’s ideas and help the researcher to find the connection between pieces of information, and they can be questions the researcher asks himself/herself or short conceptual insights that lead to the emergence of theoretical concepts (Higginbottom et al., 2013; Roper & Shapira, 2000). All types of memos were used at all stages of the research, that is, data collection and analysis.
Findings
From the analysis of the data collected using different approaches such as participant observation together with descriptive, focused, and selective observation, formal and informal interviews, and document review, three cultural patterns were extracted: “The predominance of task-based care over emotion-based care,” “Empathy and lack of empathy, two ends of the spectrum of the nurse–patient relationship,” and “Empathy, an interactive and reciprocal process.” This section contains an analysis of events that occurred frequently in the care provided by the cardiac surgery ICU nurses.
Cultural Pattern I: The Predominance of Task-Based Care Over Emotion-Based Care
Task-Based Care
Due to the requirement for nurses to be accountable to the organization and the regular checking of cases by supervisors, nurses had to carry out the tasks listed in the unit’s accreditation, and perhaps this requirement and the time-consuming registration work for the nurses meant that they did not have time to empathize with the patient, although the items that were checked out focused more on the physical care of the patient. The nurses in this unit were also very competent in providing treatment and physical care to the patient. This issue was very prominent in the setting under study, so even when the patient’s condition deteriorated, the nurses were able to deal with the condition without wasting time and quickly. Fieldnote on day 56: • The patient’s heart rhythm went into atrial fibrillation after walking … The nurse immediately went over his head and informed the anesthetist … Doctor: “Give him amiodarone” … Nurse: “I did it, let’s see if it works” … Doctor: “What can I say, you know how to use it yourself.”
Often, seeing the nurse’s skill at work would amaze others, and sometimes this skill was so tangible that others acknowledged it. Fieldnote on day 121: • The anesthetist visited the patient in bed 5 who was 100 days post-op, had a tracheostomy and was on a ventilator. He turned to the nurse and said: “If it wasn’t for your care, this patient would have died a long time ago. Even now it is very strange that he is alive. No one can believe that this patient survived. All this is the result of your good care. I have said it in other places. The nurses here are really good ….”
ICU care was highly dependent on equipment. In fact, the care was a kind of technological care and required high knowledge and expertise of nurses in working with equipment, so that if someone did not have this expertise, he could not be a special nurse.
Some nurses felt that the atmosphere of care in this unit was soulless and mechanical. Observations also showed that in many cases, care was given without communication with the patient and that the care was mechanistic. Nurse number 5 said: • I myself have learned that I have to do the work of the sick … it is sick anymore … it is like a car that comes to the pit of the repair shop and you have to change its oil and its periodic service must be done and return to normal work. I don’t know why the companions of the patient cry when their parents or loved ones are here or when they are dead … now they are dead … but when I stand in this position that they are human beings like us, I think it will be much easier to understand this issue ….
Another important aspect of the care was that most of the care was on the shoulders of the nurse’s assistants and they actually did much more care and communication with the patient than the nurses. This care was non-specialized care. Fieldnote on day 26: • The patient wanted fruit juice … the head nurse told the assistant nurse: “Give him fruit juice, give him a bedpan as well. The assistant nurse said: If they stay here too much, they give orders all the time. He should be discharged.” He grumbled under his breath and picked up the bedpan and went to the patient ….
Of course, in many cases the high level of interaction and intimacy of the nurse’s assistant with the patient led to greater trust in the patient, and the patient was more inclined to express their needs with the help of the nurse. It seemed that they were more empathetic than the nurse, despite more physical work.
In fact, the nurse’s priority was the routine work and the physical needs of the patient that needed to be followed up. Even when everyone was at bedside of the patient to hand over the shift, they may have missed a simple greeting with the patient, and all their focus was on the words of the colleague from the previous shift, and the one who looked at them with concern and curiosity (the patient), and surely all these things were to help him, they saw less.
According to some nurses, paying attention to the patient’s feelings is not very important; what is important is the physical recovery of the patient and saving his life. Nurse number 3 said: • In my opinion, empathy and communication with the patient is not a priority. Whatever it is, it will pass. When the patient leaves the hospital and goes home to his family, he forgets. A nurse may not feel like talking to the patient, but his technical work is correct.
Emotion-Based Care
After being in the field for a long time and carefully observing and discarding preconceptions, the researcher found that nursing is an amalgam of knowledge, duty, performance, feeling, patience, fatigue, etc., and it is true that in the cardiac surgery ICU, duty-based care was prioritized, but there was also empathy, although perhaps not everywhere and all the time, although it may have faded under the influence of circumstances, but it was still there.
The nurses were sometimes very patient and kind, taking time to communicate with the patients, taking care of their feelings, and when they saw them suffering and sad, they tried to perceive and reassure them. They did not hesitate to support the patient when the ward was quiet and less busy, or when they felt that the patient was in an unfavorable physical or emotional condition. Fieldnote on day 17: • The patient was a 60-year-old woman on a ventilator … The nurse changed the dressing with the help of the assistant … The nurse looked at the patient and said I want to suction her too … She put her hand on the patient’s head (who had been extubated a few days ago and was intubated again and had sepsis) and put her face close to the patient’s face and looked at her and said: “I'm so sad. She became so agitated and uncooperative that she had to be intubated again.
Empathic response was a skill that was seen in the work of some nurses. It had different manifestations, for example, trying to meet the patient’s needs in different ways, giving hope and information to the patient, making the patient’s companion take part in the care, and so-called anything that could improve the patient’s condition in any way. In fact, what was done in response to the patient’s needs was to try to meet the patient’s needs in any way possible, even with the help of the patient’s companion.
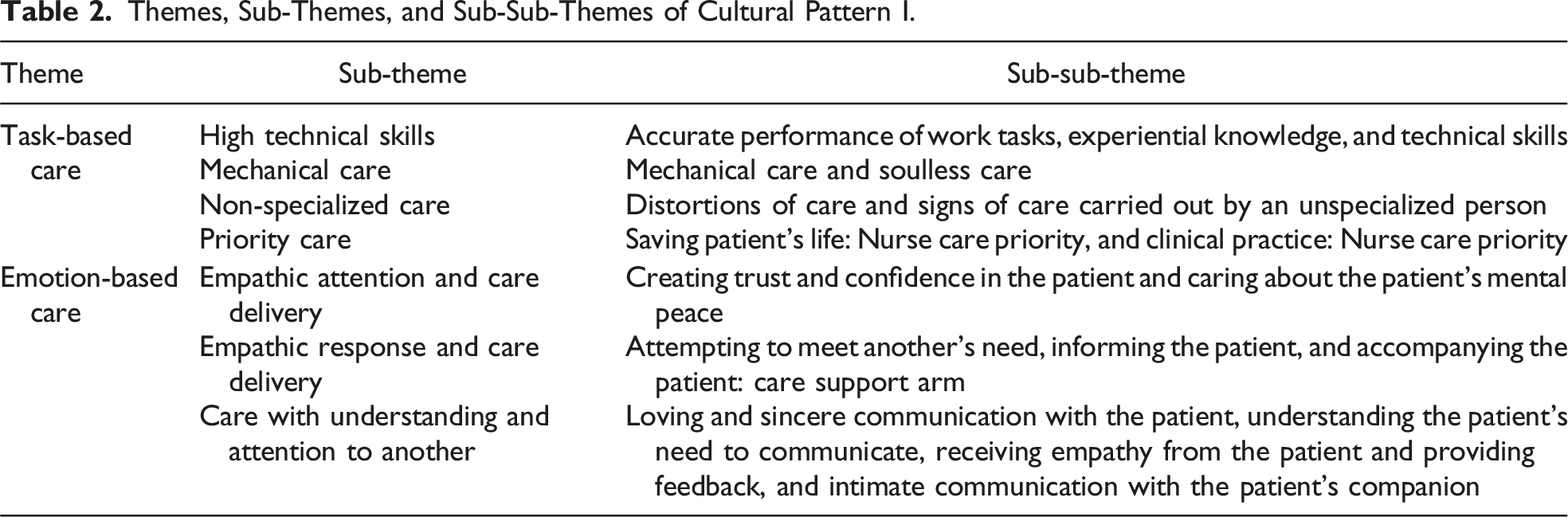
Themes, Sub-Themes, and Sub-Sub-Themes of Cultural Pattern I.
Cultural Pattern II: Empathy and Lack of Empathy, Two Ends of the Spectrum of the Nurse–Patient Relationship
From the beginning of the fieldwork, the researcher tried to find a pattern of interaction between nurses and patients. Gradually, he came to the conclusion that in a situation where two people with different cultures, personal conflicts, views, capacities, and roles are confronted with each other, a number of factors are involved in creating different behaviors. The researcher asked people in the field to give a definition of the concept he was looking for, that is, empathy or empathic care. What most of them included in their definitions was communication with and support for the patient, and according to them, this communication depended on various factors. They had different understandings of this concept, and most of them actually considered empathy as support and communication with the patient. Nurse number 9 said: • I think empathy is the highest level of communication. Is it possible that there has been no communication and then there is an expectation of empathy? not really. The two are inseparable. In my opinion, when communication reaches a high level, empathy, love and now everything else can be included in this category ….
The inclusion of the concept of communication in their definitions led to a greater focus on it. In fact, the formation of the nurse–patient relationship was influenced by various factors such as culture, personality of the person, environmental conditions, and previous experiences of the individual, and based on this, the relationship was either full of empathy and understanding of the other and giving importance to the other or it lacked empathy. It was irresponsible and indeed emotionless.
Empathy, the Key to a Successful Therapeutic Relationship
According to the participants in this study, empathy was communicating with and understanding the patient, and they believed that this communication would lead to better support for the patient. It was the ability to put oneself in the patient’s shoes that led to a better understanding of the patient. What stood out in the nurses’ discussion was that in many cases their empathy was dependent on their previous experiences, and if they had experienced this situation, they were better able to put themselves in another situation. In many cases, participants used the patient’s perspective to understand the patient better and even to provide better therapeutic interventions for the patient. They put themselves in the patient’s shoes and tried to understand how they might feel in that situation. Nurse number 12 said: • “My mom also has cancer … I put myself in the place of a sick girl … I constantly thought about how I would feel if I lost my mom?”
In addition to incorporating feelings into situations, the nurse’s information about the patient’s condition and the nature of the disease or procedure was effective in helping them to put themselves in the patient’s shoes and understand the patient’s feelings. Perhaps, the nurse’s familiarity with the condition, type of procedure, and experience of caring for people with these conditions would make it easier for them to see from the patient’s perspective and help them to understand better. Participants also mentioned their previous familiarity with the patient, saying that the long period of hospitalization made them feel better about the patient and made it easier for them to understand him/her by remembering him/her. In fact, the nurse understood the patient by relating the patient’s condition to his/her own previous experiences, but this did not remain at the level of a feeling and made him/her try harder to help the patient, and this is the concept of empathy. Nurse number 11 said: • Of course, I have to say that if this problem does not happen to us, we cannot identify with each other … For example, if my father is not ill, I don’t know what will happen if my father is ill, or if my father or mother dies, or …! This vision can help me in my work to see the patient as my family.
A number of nurses also felt that previous experience did not always lead to understanding of the other party (the patient) and felt that other factors, including the personality of the person and the impact of the experience on the person, were involved in this understanding. Nurse number 15 stated: • One of our colleagues has experience and still has a hard time with patients. It is different. People are different.
Empathy, the Missing Key to Communication
In the cardiac surgery ICU, there was a lack of understanding between nurses and patients and their family members. This had created a challenge in the relationship between them. Patients expected immediate attention from nurses, and sometimes the condition of the ward and the condition of the patients did not allow for patients’ needs to be met as quickly as possible. Nurses felt that some of the patients’ demands were excessive and beyond the scope of their duties. It seems that in most cases, the different views of the patient, their visitor, and the nurse about the illness caused these problems, and each of them was right from their point of view. It can be said that in many cases, the lack of awareness caused by the lack of adequate and correct training of patients and carers caused such problems. As the discharged patient said: • I was happy with everything, but I wish they had told me what they were going to do for me on the first day I was admitted. I know they did it so I wouldn’t be stressed, but I would have liked to know. They tell us everything that is going to happen. They tell us where we are going, what the law is, for example, my wife came to see me, they had a fight with her. So they should tell us what the law is soon?! what do we do?!
Many nurses considered the physical condition of the ward and the lack of space for patient family members to meet the patient as the reason for this confrontation and unprofessional treatment, but the behavior of some nurses with the patient’s carers indicated a sense of complete ownership of the ward and a lack of mutual understanding. In most cases, they did not understand the patient’s feelings. Fieldnote on day 126: • The patient visitor who had brought fruit juice for his patient and was not allowed to see his patient stopped when he saw me and said sadly: “When can I see my patient? Why is no one here giving us an answer? I have been sitting behind this door since last night. They don't answer people”.
This lack of understanding was mutual between the nurses and the family members, and the family members felt it was their right to see the patient and to know about the patient’s condition, and they often tried to get into the ICU by circumventing the rules or by asking the doctor. Again, they were treated harshly by the nurses, and in some cases, when these rules were not followed by the patient’s companion, it disrupted the nurses’ work and the patient’s treatment. Disregard for the nurses’ warnings and disregard for the rules of the unit led the nurses to deal with them harshly. Non-observance of the rules by the companions sometimes angered the nurses and led to sharp verbal confrontations between the parties. Fieldnote on day 98: • The patient in bed 4 was agitated and wanted to throw himself off the bed. The patient’s companion came into the ward with the nurse’s permission to talk to the patient and calm him down. He walked over the patient’s head and started taking pictures of the patient. The nurse suddenly noticed him and said angrily: “What are you doing? You have no right to take pictures here” … She went over to him and asked him to delete the pictures ….
Perhaps, in many cases the harsh encounters and verbal and non-verbal abuse that sometimes occurred not only between nurses and patients but also between members of the treatment team were the result of a lack of empathy. It was the lack of empathy that made the person unable to understand the other person and to see from their point of view. This made the person irresponsible and caused the person to be irresponsible and short with the patient and his colleague, and what the researcher witnessed many times was the complaints, dissatisfaction, and fatigue of nurses and sometimes even patients due to this irresponsibility.
It seems that one of the things that made the nurse feel bad or callous toward the patient and the patient’s family members was that they were judging them. In fact, they were judging them on the basis of their own assumptions about the cause of the patient’s behavior and what the patient’s family members had said on the phone, and they were treating them on the basis of those assumptions. Fieldnote on day 106: • The phone rang. The nurse answered it. He said: “He’s fine, he’s been taken off the ventilator and he’s fine.” He hung up and laughed and said: “bed 1’s son is an addict. His sons want to get rid of him … I also said it was fine on purpose and he laughed!!!”.
By piecing together observations, interviews, and notes from the field, the researcher found factors that may have been involved in the lack of empathic care and empathy, including individual factors, personality, workload, gender, and culture. It turned out that one of the most important reasons was the organizational issues and problems that led to a lack of motivation for nurses to do their work and in many cases even to differences between staff. The implementation of empathy in the care environment requires a suitable platform, and many field informants felt that this platform did not exist. They argued that organizational and environmental barriers prevent the integration of empathy into patient communications and also stated that organizational support is a key factor in supporting patients, meeting patient needs, communicating effectively, and enabling empathy to be integrated into practice. Although many of them stated that the existence of these problems in the performance of their duties did not affect the patient, it was evident that the quality of work was reduced. One of the things that were often mentioned in their conversations was the difficult working conditions in the ICU and the low income, and by comparing it with other settings, they expressed that this important issue might cause a person to behave differently in two settings. Nurse number 18 said: • Look, there was a time when I did the work with enthusiasm, but there was also a time when I was hurt. Well, it will definitely have a negative effect. I can’t hide it … organizational problems or any incident can have an effect on a person’s mind … these problems made me fall back, but the fall back was compensable. There was nothing that could harm the patient.
Another thing that seems to be a long-standing problem of nursing in different organizations, and has been said many times and everyone is aware of it and its consequences, is the problem of the nurse–patient ratio and the high workload of nurses. In this department, lack of time and heavy workload were factors that prevented the nurse from communicating with the patient and therefore neglected the emotional support of the patient. Nurses also said that administrative demands can lead to limited time and no opportunity to experience empathy. Nurse number 16 said: • Anyway, the workload is too much. ICU work is very hard. If I get very tired, it definitely affects my behavior. Maybe the work is not done with the quality I want to provide. I have to do all the paperwork. I don’t have time to listen to the patient.
Other reasons include different cultural patterns. In some cases, communication or physical contact was difficult for some nurses because of the gender of the patients. Nurse number 14 said: • I really can’t communicate with men. Or, as you say, I empathize and try to keep my distance. Because you hear something that is not good ….
Some nurses withdrew from the suffering of patients in order not to hurt themselves. In fact, they saw their lack of empathy as a shield for themselves.
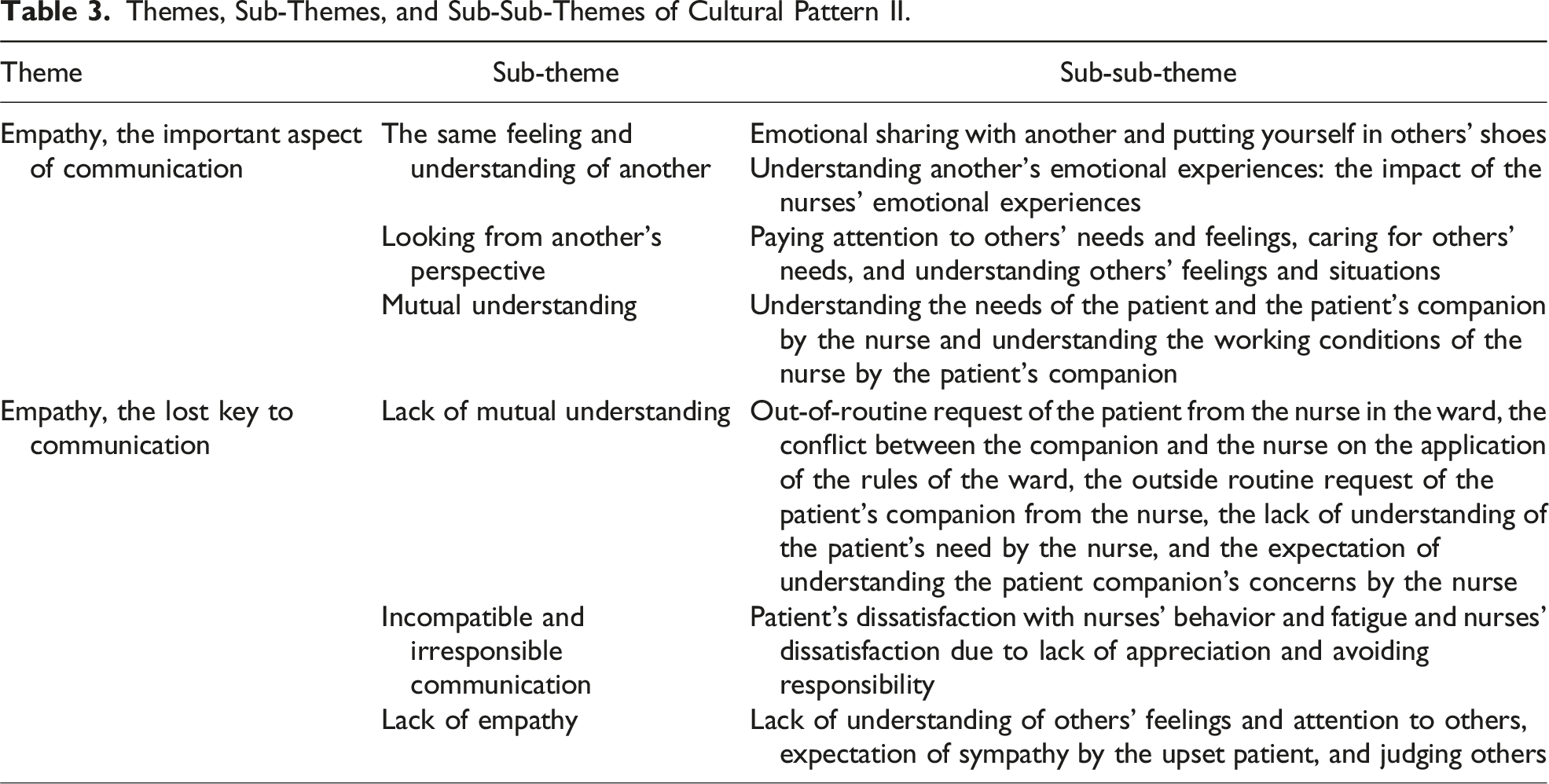
Themes, Sub-Themes, and Sub-Sub-Themes of Cultural Pattern II.
Cultural Pattern III: Empathy, an Interactive and Reciprocal Process
It seems that the effects of empathy and empathic care go beyond what has been said so far. The researcher witnessed the effect of empathy both in the empathic person and in the situation they created and found that empathy can affect both the empathic person and the person who receives that empathy. Empathy is a process that gradually grows and penetrates a person over time and through personal experience and work, and the person benefits from this feeling. Also, one of its effects was to create satisfaction in the patient due to the improvement in clinical outcomes and being understood by another as a person who received care from this empathetic person. Therefore, the intrapersonal and interpersonal consequences of empathy formed the main elements of this pattern.
Intrapersonal Consequences of Empathy
The researcher’s observations showed that the most obvious effect of empathy was the feeling of inner satisfaction in the empathic person and the pleasant and positive feeling that the person got from this empathy. Nurse number 5 said: • I believe that if this patient is satisfied with me, whatever I have done for him can have an impact on my life, and at least it creates a mental satisfaction for me … and it can definitely be reflected in my life ….
What was seen as a result of the crystallization of empathy in an empathic person was that he accepted the patient in any condition, regardless of social class, race, addiction, and unconditionally, and felt obliged to provide complete care to the patient in any condition. Nurse number 2 said: • I never misbehave with these patients (addicts) … I don’t hate them … The guys always tell me that you treat them well too …! But I think that whether the patient is an addict or a homeless person, we should understand him … I don’t care who the patient is and what he does ….
Whether or not they were responsible for the patient, the empathic persons considered themselves responsible for all patients and their problems and conditions. Fieldnote on day 70: • The doctor came to the ward to visit the patients. They arrived at the patient in bed 7, a woman who had a tracheostomy and was on a ventilator. The patient was coughing and there was a lot of secretions from the trachea. The nurse left the visit and said excuse me, doctor, can you continue the visit yourself? I have to help this patient and he immediately started suctioning the patient.
Gaining a deeper insight into the person was a beneficial inner change brought about by empathy. In such a situation, the nurses experienced feelings such as “concern for the patient” and “compassion for the patient” and had concern for the patient. Working beyond the duty was also clearly evident in these people, and the nurses themselves acknowledged that they had done so. Although the nurse knows that what she is doing is beyond what is expected of her by the organization, sometimes she even feels tired of doing it, but in the end this sense of inner satisfaction from doing the work and the institutionalization of the sense of empathy in the person make her work beyond her duties. Nurse number 1 said: • I often get tired … when I go home I say to myself that I will retire … then I say no! I still want to work … or I say that I won’t be upset if I leave tomorrow … or that I won’t work more than I can … you know? I’m working here much more than my ability and responsibility, but I can’t help it … When I come back, I won’t be able to see it again ….
The person tries not to let workload, personal, and organizational problems affect the way they communicate with the patient and tries to give the best care to the patient. However, as mentioned earlier, organizational problems affect the quality of the person’s work and the quality of their communication with colleagues and patients.
Interpersonal Consequences of Empathy in Nurses
One of the most obvious interpersonal effects of empathy is an improvement in the patient–nurse relationship. The patient had more trust in the empathic nurse; empathy made the patient feel understood and more relaxed, and even according to the nurses, it reduced the patient’s mental problems and the patient participated more in the treatment. Nurse number 2 said: • Regarding extubating the patient … because the patient is already awake anyway … when you explain to him, for example, tell him that I want to do a certain thing … you do these collaborations. You will be better and easier and faster to get off the machine, otherwise we will have to give you medicine and it is possible that we will keep you under the ventilator again … I saw that this communication was so effective that it made my job easier and how much the patient cooperated more ….
Perhaps one of the most important and well known of these effects is the improvement in the patient’s clinical outcome, both physically and psychologically. The interpersonal effects of empathy also include creating satisfaction in the patient through the improvement in clinical outcomes and being understood by another person as a person being cared for by that empathic person. Nurse number 2 said: • Sometimes I have seen patients become psychotic … I saw that the patients I talked to and communicated with were much better psychologically. If we didn’t communicate with the patient, his problems would have increased … he would have become psychotic and had to take antipsychotic or anti-hallucination medication, and some patients even had to be reintubated. The effects of empathy with the patient were good in terms of work, the patient felt positive and satisfied, and I was also satisfied ….
Many nurses said that empathy with patients, in addition to the positive psychological effects, also reduced the physical problems of patients and led to a sense of satisfaction that was understood by both parties. As mentioned earlier, this sense of satisfaction led to tolerance of difficult conditions and had long-term positive effects for the nurse. Nurse number 13 said: • I could see that the patients I was communicating with and understanding were much better mentally and even physically. Both the patient felt positive and I was satisfied myself ….
Patients also found the close nurse–patient relationship very useful and effective and felt that the nurses’ kind treatment of them was morally uplifting and energizing.
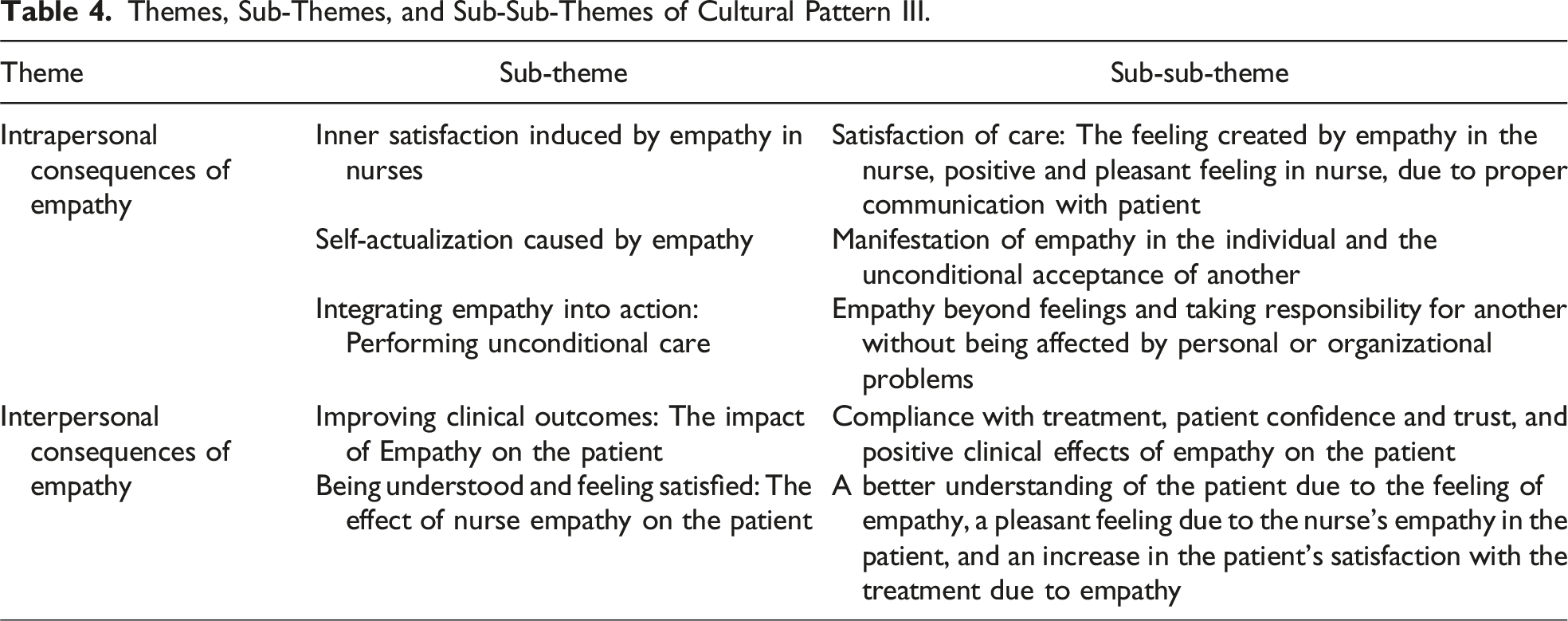
Themes, Sub-Themes, and Sub-Sub-Themes of Cultural Pattern III.
Discussion
The present focused ethnographic study provides valuable insights into the unknown aspects of behaviors and interactions in the ICU. The aim of the current study was to explain the culture of empathic care in the ICU. Three cultural patterns were identified in this study, and the findings are discussed based on the cultural patterns and their main respective themes.
According to the research findings, task-based care was a priority for nurses. Although most of them emphasized the importance of patients’ emotions, in reality, the nurses’ priority was to perform the work tasks correctly rather than to emphasize patients’ emotions. Confirming this finding, Kruijver et al.’s study showed that nurses rarely consider patients’ emotional aspects or feelings (Kruijver et al., 2001). Of course, this issue is a familiar issue in many nursing studies, and other studies confirm this finding that nurses focus more on performing technical tasks and interpersonal communication is left on the sidelines (Aein et al., 2008; Salmani et al., 2016; Sepehri Nia et al., 2013). However, these cases do not seem to be indicative of all conditions, as patient communication does not require extra time and good communication not only does not take nurses’ time but also helps save it (Chan et al., 2012). Nevertheless, it is important to note that more nurses, less stress, and proper training can go a long way in helping nurses develop empathy and communicate effectively.
One of the interesting findings in this study was mechanistic care. Other studies have shown that nurses describe task-based care as mechanistic and unemotional, leading to a cold and inhospitable environment rather than humanizing care (Albinsson & Arnesson, 2019; Gray, 2010). This, perhaps, has something to do with the nature of medical education, where patients are seen as objects and tools for learning. It is interesting to note Feo and Kitson’s findings that the focus is on the patient as a body to do things rather than as a person (Feo & Kitson, 2016).
One of the characteristics of ICU nurses was a high level of scientific and technical competence, and other studies also confirmed that specialist nurses had a high level of practical competence (Fotohi et al., 2019; Mokhtari Nouri et al., 2015), but in terms of theoretical knowledge, this finding contradicts the findings of Fotohi et al. (2019) and Gardulf et al. (2016). Perhaps, working in a highly specialized unit and the seniority of most nurses in that unit created this atmosphere. However, confirming the insufficiency of knowledge without empathy, Stephany’s book states that even if the members of the healthcare team have sufficient technical knowledge, the lack of empathy in the care process reduces the level of satisfaction with the care received (Stephany, 2022).
One of the findings of the study was that ICU care is dependent on technology. The reliance on technology in patient care is a requirement of the ICU due to the structure and nature of the department, and is a common theme in many studies, both positive and negative. Almerud et al. (2008) in their study see this technology as both an important tool and a barrier to patient-centered care. On the other hand, a number of researchers believe that technology can facilitate and improve care and allow nurses to spend more time with their patients to reduce anxiety and address their concerns (Price, 2013; Tunlind et al., 2015). However, despite its benefits, technology can never replace the empathic care, and technology cannot dominate the art of nursing and patient empathy.
The term non-specialist care refers to care provided by nurse assistants. It would seem that having less responsibility for recording and reporting, or being accountable to the system for the life of the patient, would enable them to empathize better with patients. Importantly, it is curious that this group of healthcare workers has received less attention in studies, given the important role of nursing assistants in patient care, particularly in ICU.
In line with Eriksson’s view, care should be based on an understanding of the person in terms of an indivisible unity of body, mind, and spirit (Eriksson, 2002). The study showed that the ability to understand others results in appropriate responses, the empathic response. Silverman, Kurtz, and Draper came to the same conclusion in their study and defined empathy as “a two-step process: (1) understanding how others feel and (2) transferring this understanding to the sufferer in order to support him/her” (Kurtz et al., 2017), and this transfer of understanding to the patient can be an empathic response. Empathic responding was a skill that had different manifestations, for example, trying to meet the patient’s needs with different forms of love, giving hope and information to the patient, using the patient’s companion in caring, and so on. Hojat et al.’s (2004) study considers empathy as a skill, stating that empathic response shows understanding of another’s perspective and requires integration of knowledge, skills, and attitudes taught during academic education.
In general, what has been said about the predominance of task-based or physical care over emotional or empathic care has been confirmed in many studies. One of these was the study by Feo and Kitson, which showed that all nurses were concerned about patients’ well-being and responded kindly when patients were unwell or distressed, and some nurses showed more empathy, compassion, and active listening. However, in his study, most nurses focused on getting the job done and providing physical care (Feo & Kitson, 2016). In general, emotion-based care was overshadowed by task-based care in the cardiac surgery ICU, and the task-oriented atmosphere was more pronounced in this unit.
The results of the study showed that the relationship with the patient is influenced by a multifactorial background and moves along the spectrum of “empathic relationship—relationship without empathic feeling and action.” When describing empathic care, most of the participants in this study mentioned the issue of connecting with and supporting the patient. As in Stavropoulou’s study, the concept of communication and the concepts of support and achieving the best outcomes for patients were mentioned by participants when describing empathic care (Stavropoulou et al., 2020).
The study also found that carers were able to relate their own past emotional experiences to the symptoms they were experiencing. The relationship between similar past experiences and the ability to accurately predict the emotions and cognitions of others has received limited support in a number of studies (Gibbs & Woll, 1985; Hodges, 2005; Kitano & Chan, 1978). In contrast, some studies have supported the link between similar past experiences and empathic and emotional responses (Barnett, 1984; Barnett et al., 1986, 1987; Hodges et al., 2010; Stotland & Dunn, 1963). Perhaps, it is possible to argue with this finding that, as the results of this study also showed, although past experiences can be effective in people’s understanding, other factors such as people’s personality, gender, and cultural background are also effective. Similarly, the results of the Batson et al. study showed that women showed more empathic responses (such as empathic concern, sympathy, and compassion) than men when exposed to another similar experience (Batson et al., 1996).
The nurses stated that they tried to identify with the patients in order to understand them better. In contrast to these findings, other studies have shown that nurses were careful not to identify too much with clients by shifting psychological locations or relating their experiences to their own (Davis et al., 2004; Gerace et al., 2013). This may reflect nurses’ efforts to distance themselves from negative emotions (Zaki, 2014) and a defense mechanism to prevent the damage they cause, which can be a barrier to empathy.
At the other end of the nurse–patient relationship spectrum was a lack of empathy. A frequent example of this is a lack of mutual understanding, both between staff and patients, and particularly with their family members. One of the main challenges in the ICU was the encounter between nurses and patients and the encounter between nurses and patients’ family members, and, as described, the family members’ non-compliance with ward rules sometimes led to nurses’ anger and harsh treatment, unprofessional behaviors, and sharp verbal conflicts. Parizad et al.’s study mentioned some of these unprofessional nurse behaviors, such as belligerence, harsh and inappropriate encounters, retaliatory confrontation, or incitement (Parizad et al., 2018). Patients and their relatives expected the nurse to be caring, understanding, and friendly. Similarly, in Loghmani’s study, empathy and consolation were important to families (Loghmani et al., 2014). However, as mentioned, this lack of understanding could be due to the different views of the parties and lack of training.
It is safe to say that one of the most important factors influencing the culture of empathic care was organizational issues, which were mentioned in observations, quotes, and interviews. Participants considered organizational support to be an important factor in patient care, meeting patients’ needs, effective communication, and the ability to provide empathic care. Stavropoulou also found in his study that organizational support, incentives, training, and teamwork help to overcome existing organizational barriers and increase the provision of empathic care by ICU nurses (Stavropoulou et al., 2020).
In the ICU, nurses were constantly faced with heavy workloads and enormous responsibilities, which affected how they experienced and demonstrated empathy. Baillie has also shown in a qualitative study that nurses show little empathy when they are overworked (Baillie, 1996). Kerasidou states in his study that the reasons attributed to the lack of empathy in the healthcare sector are long working hours, staff shortages, inability to spend enough time with patients, increasing pressure to meet operational targets, and increasing workload (Kerasidou et al., 2020). Even if empathy is recognized as a virtue rather than a skill, if the environment does not support it being expressed, those working in that environment are less likely to get the chance to develop it (Allmark, 2013).
Some of the participants in this study considered empathy to be harmful and avoided it. In Stavropoulou’s study, ICU nurses stated that empathy could be harmful to them, and self-protection was identified by participants as their main personal coping strategy (Stavropoulou et al., 2020). Another basic variable that should be studied in the expression and perception of empathic care is cultural factors (Tsai et al., 2013). In this study, everyone had their own cultural pattern. Bleakley says that empathy is a historical and cultural concept. We cannot assume that “one empathy fits all” (Bleakley, 2014). We need to question the cultural contexts in which these observations are made. One of the other variables that seem important to consider in empathy is personality traits. Shalchi’s study also showed that there is a strong relationship between personality and empathy in nurses (Shalchi, 2018). It seems correct to think of the nurse–patient relationship in terms of empathy as a spectrum because, as we can see, we are faced with a variety of different emotions in each situation.
The third pattern is actually the unique finding of this study, which has mostly been explored in the psychological literature. The researcher’s experiences during this period showed that the development of the sense of empathy and its flourishing in a person can have positive effects on the empathic person and subsequently on the person who receives this empathy, which indicates the interactive and interpersonal nature of empathy. In support of this finding, other studies state that one person’s feelings affect another person’s feelings in a dynamic and bidirectional way (Butler, 2015; Campos et al., 2011; Reeck et al., 2016; Zaki & Williams, 2013) and that one person’s feelings cannot be separated from another person’s feelings in interpersonal contexts. Given the inherent interpersonal nature of empathy, these principles can be applied to theoretical and experimental work on empathy (Main et al., 2017).
The intrapersonal consequences of empathy are, in fact, everything that has developed in a person as a result of this feeling, as if it distinguishes a person from others. By putting himself/herself in the patient’s place, the empathic person is able to understand the patient’s needs even without expressing them. He/she feels responsible for all patients and conditions and tries not to let workload, personal, and organizational problems affect his work and the way he/she communicates with the patient and provides the best possible care. In Stavropoulou’s study, participants emphasized that understanding patients’ needs is an important component of empathy and an essential aspect of patient care and support (Stavropoulou et al., 2020). As mentioned earlier, this understanding is mutual and two-way. Main also suggests that feedback from the person being empathized with, whether explicit or implicit, helps the empathizer to gain a greater understanding of the subject, thereby facilitating the empathic process (Main et al., 2017).
Pleasant and positive feelings and a sense of inner satisfaction were also effects of empathy. Dicker’s studies also discussed that satisfactory and positive feelings arise when nurses feel that they have achieved their goals in caring and that the patient’s needs have been adequately met (Jiménez-Herrera et al., 2020). These positive emotions are beneficial to the professional experience (Hunsaker et al., 2015), prevent emotional exhaustion, and help to prevent low self-esteem (McCullough et al., 2001).
Empathic individuals exhibited extra-role behaviors and accepting others unreservedly. Extra-role behaviors in the workplace are behaviors that are not officially defined in the job description and are not officially rewarded, and activities that are not part of the formal professional role (Van Dyne & LePine, 1998). Perhaps, it can be said that doing extra-role work through empathy satisfies a person’s sense of self, according to nurses’ sense of satisfaction through empathy. Empathic relationship means recognizing and having a friendly relationship with patients as valuable people, regardless of their physical diagnosis (Raudonis, 1993). As with the results of this study, the empathic person accepted the patient in any condition and the patient’s social class, race, addiction, etc. had no meaning to him/her and he did whatever was necessary for the patient.
The interpersonal consequences of empathy included any outcome that resulted from this empathic interaction and affected the nurse and the patient. However, empathy was also influenced by other factors discussed earlier. As mentioned earlier, empathy is a process that grows gradually in an individual over time. In support of this finding, Main’s study noted the dynamic nature of empathy as a process that unfolds over time (Main et al., 2017). Indeed, “empathy” is a dynamic, directed interaction between participants that leads to the construction of a “shared world” of meanings (Broome, 1981; DeTurk, 2001; Gibson, 2014).
The most important interpersonal effects of empathy in patients were satisfaction, improved clinical outcomes, and being understood. Consistent with these findings, similar studies have reported a positive effect of empathy on patient outcomes, patient satisfaction, and adherence to treatment (Derksen et al., 2013; Hojat et al., 2011; Lelorain et al., 2012; Menendez et al., 2015; Rakel et al., 2009; Utriainen & Kyngäs, 2009). Empathic care and communication not only lead to improved patient outcomes but also help patients to cope effectively with their illness (Neumann et al., 2009). This may be because, as a result of the targeted care provided by an empathic nurse and the mutual understanding between a nurse and a patient, the patient’s negative feelings disappear and he or she cooperates with the treatment with a positive attitude. As well as improving the patient’s emotional state, empathy can also improve physical outcomes. Studies conducted in different groups of patients with different health problems have shown positive results in terms of their health progress (Hojat et al., 2011; Rakel et al., 2011). What is clear, however, is that whatever was said and whatever was caused by the effects of lack of empathy with these effects diminish.
Conclusion
We are aware of the complexity of providing effective and efficient holistic care in the ICU. It is well known that many nurses today are inadequately trained to provide this care because much of the research has paid less attention to all aspects of care, including empathy. Our research shows that empathy creates a caring environment where nurses not only understand their patients but also relate to them. Patients feel heard and supported, which leads to a trusting and effective patient–nurse relationship, which leads to better care and patient satisfaction and improvement, and ultimately both parties benefit from this empathy. In this study, exemplary examples of the effects of empathy in the nursing relationship and its barriers and facilitators were identified, according to which removing barriers from healthcare managers and politicians, receiving organizational support and financial support, creating a supportive environment, training, less workload, and more facilities should be considered tools to empower nurses to provide empathic care.
Footnotes
Acknowledgments
The present research is taken from the doctoral thesis of the author of the study in Tehran Medical Sciences, Islamic Azad University. The authors feel it necessary to express their gratitude to the esteemed officials of the Faculty of Nursing and Midwifery, Tehran Medical Sciences, Islamic Azad University. The authors are also grateful to all the study participants in the cardiac surgery intensive care unit of Dr. Shariati Educational-Medical Centre. Many thanks to Professor David Fetterman for his review and comments on this manuscript.
Author Contributions
Marziyeh Mohammadi: conceptualization, data curation, formal analysis, methodology, resources, software, validation, visualization, writing—original draft, and writing—review and editing; Hamid Peyrovi: conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, and writing—review and editing; Nematallah Fazeli: conceptualization, formal analysis, investigation, methodology, project administration, supervision, and writing—review and editing; and Zohreh Parsa Yekta: conceptualization, methodology, supervision, investigation, project administration, supervision, and writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Tehran Islamic Azad University of Medical Sciences., Tehran, Iran.
Ethical Consideration
After obtaining the necessary licenses and ethical code from Tehran Medical Sciences, Islamic Azad University, No. IR.IAU.TMU.REC.1400.069, and receiving the letter of introduction, coordination was done with the managers of the facility in which the data were collected and the officials of the cardiac surgery intensive care unit and the necessary licenses were obtained. Other ethical considerations taken by the researchers to protect the rights of the participants include introduction and brief and clear explanation of the objectives of the research; assurance of confidentiality and non-inclusion of information obtained by the names of individuals; obtaining informed written consent from respondents; assurance of voluntary participation in the study; explanation to respondents of the possibility of non-response or withdrawal from the study at any stage of the interview; and keeping the results of the study at the discretion of the participants.