
Abstract
Pakistan has extremely poor breastfeeding indicators: fewer than half of infants under 6 months are exclusively breastfed, only 20% of infants are breastfed within the first hour of life, and nearly half are never fed colostrum. The country’s high infant morbidity and mortality is in part due to this suboptimal infant feeding. A network of lady health workers (LHWs) employed by the government facilitate maternal and child health programs, including breastfeeding support in their communities. This study describes LHWs’ perspectives and experiences regarding breastfeeding. We conducted semi-structured interviews with 14 LHWs and used thematic qualitative analysis to code and analyze the data. Our research revealed that LHWs use their role as members of the community and involve influential members of the family to build trust. Frequent home visits beginning prenatally help them address misconceptions about infant feeding. While they have strong knowledge about the benefits of breastfeeding and the importance of colostrum, they demonstrate gaps in their knowledge regarding breast conditions, the safe preparation of human milk substitutes, the physiology of milk production, and supporting mothers who are separated from their baby. Future training should address these areas where LHWs lack knowledge to help mothers facilitate early and exclusive breastfeeding. With adequate training, LHWs are uniquely positioned to use their role as trusted members of the community to effectively counsel families on the importance of breastfeeding and support the clinical needs of women during the perinatal time.
Keywords
Introduction
In low-resource settings where water quality and dietary diversity are poor, breastfeeding is particularly important for child health as it ensures infants receive key nutrients and protects them from lethal infections such as diarrheal disease (Daud et al., 2017; Mansuri et al., 2018; Shahid et al., 2015). However, Pakistan has low rates of breastfeeding initiation and exclusivity contributing to the highest neonatal mortality rate in the world, estimated at 42 per 1000 live births. Nationally, fewer than half (48%) of infants under 6 months of age are exclusively breastfed, and only 20% are breastfed within the first hour of life (National Institute of Population Studies Islamabad, 2019).
Within the first three days of life, nearly three-quarters (74.2%) of infants in the Punjab province of Pakistan are fed liquids other than breastmilk, including liquids such as honey (37.3%), milk (other than breastmilk, 34.5%), and infant formula (19.6%), and only 9.5% are breastfed within the first hour after birth (Bureau of Statistics Punjab (BSP), 2018). Late initiation (up to several days after birth) and prelacteal feeds are related to traditional beliefs against feeding babies colostrum, while concerns that a mother’s milk can be poisonous or that there is low milk supply reduce exclusive breastfeeding (Ahmed et al., 2018; Asim et al., 2015, 2020; Qureshi et al., 2017; Zakar et al., 2018). Prelacteal feeds given in Pakistan commonly include honey, ghutti (a herbal mixture), dates, water, and teas (Asim et al., 2015, 2020; Fikree et al., 2005; Pirzada et al., 2021), which are given because families believe they will act as a laxative and reduce colic, and because colostrum is considered to be old milk that has been in the breast throughout pregnancy (Asim et al., 2015, 2020; Fikree et al., 2005). Furthermore, through this traditional practice, families believe that the baby will take the personality characteristics of the person who gives them the sweet prelacteal feed (Akhtar & Shaikh, 2019; Asim et al., 2015, 2020).
Infant formula is heavily marketed across the globe as an alternative to breastmilk (WHO, 2020), often through the use of emotionally evocative and misleading marketing (Hastings et al., 2020). Infant formula is readily available in the markets in Pakistan where it does not require a doctor’s prescription; however, infant formula is not an affordable option for most families such that cow or buffalo milk is often used as a substitute for breastmilk (BSP, 2018). Infants who are fed formula or animal milk or are given water-based prelacteal feeds have higher rates of morbidity and mortality than those who are breastfed (Victora et al., 2016).
The purpose of this study was to explore the perspectives of lady health workers (LHWs) on breastfeeding in their communities (perceived effectiveness, beliefs, and practices).
Participants, Ethics, and Methods
Research Design
We used a basic qualitative research design to investigate LHWs’ perspectives on infant feeding training, experiences, and care practices in their communities. We used the constant comparative approach (both inductive and deductive) to analyze data and develop themes through an iterative process. We chose this design to gain understanding from participants’ perspectives and experiences (Merriam & Tisdell, 2015). Duke University’s Institutional Review Board granted this study exempt from a full board review on 23 February 2020 (protocol number 2020-025), because it was considered to have minimal risk to participants.
Study Setting
The National Programme of Family Planning and Primary Health Care administers Pakistan’s LHW program, which was rolled out across Punjab in 1994 and has wide outreach in the province: 56% of women who reported a birth in Punjab’s 2018 Multiple Indicator Cluster Survey (MICS) received information or services from an LHW (BSP, 2018). Per government guidelines, Punjab’s LHWs should be between 20 and 50 years old, preferably married women with children, have at least 8 years of schooling, and reside in the communities that they serve (Oxford Policy Management, 2019). They provide home-based clinical services (breastfeeding support, children’s growth monitoring, and maternal iron and folic acid supplementation) and health education (nutrition, family planning counseling, and vaccination counseling) (Health Information Service Delivery Unit, 2020). LHWs are based out of their home, also known as the Health House, which is dedicated as an open space for women in their catchment area to visit for advice and to receive medicines and supplies (Global Health Workforce Alliance Task Force, 2009; Oxford Policy Management, 2019). They work an average of 6 days in a week, conducting home visits, seeing patients in the health house, and accompanying patients when they are referred to a healthcare facility (Oxford Policy Management, 2009a). LHWs rely primarily on verbal communication in the native language as only 40.8% of women are literate in the rural areas of Pakistan (Government of Pakistan Ministry of Planning, Development & Special Initiatives Pakistan Bureau of Statistics, 2022). As per the recent population census in 2017, there is a 98% Muslim majority population in rural Punjab with an average family size of 6.46 people per household (Pakistan Bureau of Statistics, 2017). Female participation rate in the labor force is 21.4% (Government of Pakistan Ministry of Planning, Development & Special Initiatives Pakistan Bureau of Statistics, 2022). Since women typically live with their husband’s family, when LHWs conduct home visits they also interact with the mother-in-law and other female household members.
A lady health supervisor (LHS) is appointed for every 20–25 LHWs, and she is based at the Basic Health Unit or a Rural Health Center (RHC). Basic Health Units are the primary-level healthcare facilities where LHWs refer patients for primary healthcare services. They often accompany the patients to the health facility during their working hours; further referrals to secondary care facilities are made by the Basic Health Unit staff as necessary (Oxford Policy Management, 2009b).
Participants
We recruited a purposive sample of 14 LHWs in the rural area around Lahore. Inclusion criteria were that participants had to be currently active adult LHWs who serve women and families in the rural communities in the Punjab Province of Pakistan. A list of potential participants was created by members of the research team in collaboration with local health department collaborators. In addition to the purposive sampling, we used snowball sampling where some interviewees helped to connect us with other people who met the eligibility criteria. The research team determined sample size by saturation, meaning no new themes emerging during analysis (Merriam & Tisdell, 2015). Saturation was reached after 11 interviews; we conducted additional interviews to verify saturation and ensure that LHWs from different Basic Health Units were included to account for potential regional differences.
Data Collection
ZWF conducted semi-structured in-person interviews between December 2019 and January 2020. At the time of the interviews, ZWF was a master’s level researcher from Pakistan. She is fluent in Urdu and English. NS is trained as a qualitative researcher and an International Board Certified Lactation Consultant with clinical lactation experience; the other members of the research team are development economists.
The research team developed the study interview guide collaboratively after a thorough literature review to identify current knowledge gaps regarding infant feeding in Pakistan (Supplemental material: interview guide). ZWF conducted a pilot interview with a representative local participant before conducting the interviews. We revised the study guide to incorporate feedback received during the pilot.
ZWF traveled to the Basic Health Units to interview LHWs, following the interview guide and using general probes to prompt for more information or for clarity. Participants provided verbal consent after the researcher informed them of their voluntary participation and the confidentiality of the interview. ZWF audio recorded the interviews with consent of the participant; interviews ranged from 22 to 35 minutes in length and were conducted in Urdu. During the interview, the researcher provided gifts of sweets as is customary in the area. She took notes and wrote debrief memos for each interview. She assigned each participant a unique identifier, and the links between the data and the participants as well as the de-identified audio files and transcripts were stored on password-protected computers.
Data Analysis
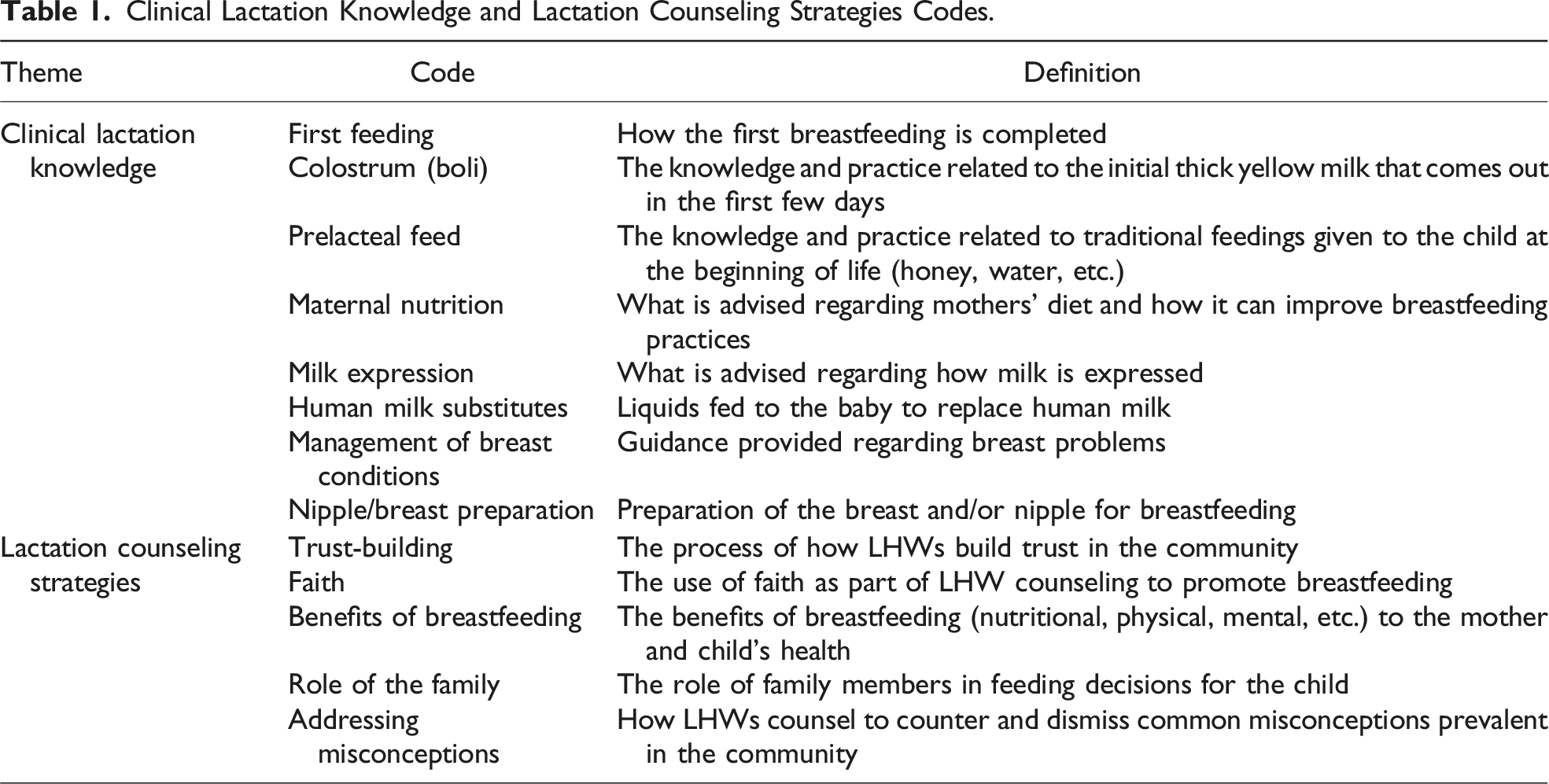
Clinical Lactation Knowledge and Lactation Counseling Strategies Codes.
Results
Clinical Lactation Knowledge
LHW knowledge about clinical lactation management stems from formal training based on evidence-based practices as well as dominant cultural beliefs and personal experiences. Their knowledge of the importance of breastfeeding within the first hour of life and the benefits of colostrum was strong; however, they had misconceptions in the areas of managing breast and nipple conditions, the impact of maternal nutrition on milk supply, and the importance of milk expression.
First Feeding
The participants frequently described the importance of feeding the infant at the breast within the first hour of life and how this first feeding is facilitated by the LHW or nurse before the dyad is discharged from the Basic Health Unit. Most rural mothers deliver in a Basic Health Unit, and in that setting the LHW is able to provide breastfeeding assistance for the first feed before discharge. So when they deliver here and we shift them to the other room, they ask us when they will be discharged. We tell them that we need to see the child being breastfed to ensure that the milk is okay and you are able to feed properly, that there is no issue or anything for the child or you. (P8)
Not being able to sit up to feed was seen as a barrier to early breastfeeding, but in some cases participants recognized that the first feeding can happen while the mother is lying down. With a cesarean birth, the first feeding is often not done within the first hour because in many cases the mother is recovering from general anesthesia and unable to feed. We tell them that it [breastfeeding] has to be given in the first hour, some say they cannot move at all so how should they even feed. We tell them that they can just do it in a lying down position and they need to try and figure out how to give it in the first hour. Those who have c-sections do not feed in the first hour as they are unconscious, those who have normal deliveries they mostly can. (P3)
LHWs are often present at the delivery to help with the first feeding, but they described difficulty helping with initiation when the baby is born at night when they cannot be present. In these cases, the mothers have less support for breastfeeding and may give prelacteal feeds or introduce formula. There are certain mothers who we cannot accompany, for instance, those who deliver at night, so sometimes they are the ones who just initiate feed by giving the ghutti (honey or if nothing else then sugar). (P5)
Colostrum (Boli)
The participants perceive that many people in their community understand the benefits of colostrum and give it as the first feeding; this is a change from the past when most people believed that colostrum was dirty and should be discarded. LHWs emphasize the health and nutritional importance of colostrum and exclusive breastfeeding when providing perinatal education in the community. Ten years ago, they would say that this is the ninth month’s milk of the mother and it is not clean for the child, so we should wait and only feed the clean milk to the child. (P6)
Prelacteal Feeding
The participants emphasized the importance of the first feed happening at the breast within the first hour of birth and the health benefits of colostrum. While they have seen improvements in exclusivity, some LHWs acknowledged that families continue to give religious/cultural feedings once the family has returned home; these are mostly herbal/homemade remedies that are carried across generations. Per the LHWs, these traditional feedings include jamun ghutti (a herbal mixture), honey, sugar water, and rose water. Mostly it was jamun ghutti, but now it is less common, and both drugstore gripe water and herbal gripe water—help to keep the child clean, etc. Then we guided them not to give jamun ghutti as it could cause a lot of diseases. We told them that the mother’s first milk is like jamun ghutti, it has everything that the child needs. (P2) We tell them that the child cannot take in anything, but well, they do still give something else (like tasting honey) when they go home, like the mother-in-law or the sister-in-law or someone else at home just gave something. (P6)
Maternal Nutrition
Several LHWs mistakenly believe there is a strong connection between maternal diet and milk supply and/or quality. They encourage mothers to consume foods with high nutrient density such as milk, legumes, and vegetables as well as adequate water to increase milk supply. They presented that an alternative to giving animal milk or formula to the baby is for the mother to consume it as part of her dietary intake to help produce milk. None of the participants mentioned the importance of frequent breastfeeding on milk supply (supply and demand). Yeah, so the mother-in-law thinks that if the child is crying then that is because he/she is hungry, so then we guide the mother that she needs to improve her own diet. If her diet is appropriate and she is able to feed, then the child would never have to starve as she can feed whenever the child wants it. (P2) We tell them that if you are giving the child the feeder [formula or animal milk], don’t do that and instead drink that milk yourself and then feed the child. It’s not as if you keep giving the child the milk so he/she stays full, no, just improve your diet and that is most beneficial for the child. (P3)
Milk Expression
Most participants were not familiar with milk expression with breast pumps, and they only discussed hand expression in the context of discarding colostrum. Breast pumps are not common in this setting; however, one participant talked about using a pump if the mother is having a difficult time getting the baby to latch. No not the hand, they do it directly. People also don’t use a pump in my community. (P2) If the mother is finding it hard to feed the baby, then she uses a pump, but generally we do advise mothers that if they can get the baby to latch it is better because it is not natural if you are using a machine to do this. There is also a risk of getting germs and bacteria, etc., so it should be avoided. (P10)
Even when asked, the participants did not describe using hands to express milk when the mother and baby are separate for work outside of the home. In these cases, the LHWs explained that the baby is given a bottle with animal milk or formula. And they say that because we have to go out sometimes we just give the bottle once or twice a day. So the mothers who go out, they introduce the other feed [formula or animal milk] too … but this is rare—those who stay at home don’t do that. (P7)
One participant described that breast massage and hand expression was historically done to remove colostrum and to allow the milk to come out by opening the nipples. Boli [colostrum]? They just waste it. Back in the days it used to be that they would take it out, they would do it with their hands, the community midwives when there used to be home deliveries. (P5)
Human Milk Substitutes
The LHWs do not see commercial infant formula used commonly because it is less accessible and affordable in rural areas. It is more common for families to use cow or buffalo milk for supplementing, which is readily available. Sometimes, the animal milk is diluted with water or has spices added to help with digestion, but the LHWs do not have specific guidelines for preparing animal milk other than not recommending its use. And because formula is expensive, they simply prefer cow or buffalo milk and they dilute it more by adding water and also even add cardamom and other things … They say that it changes the taste and flavor of milk, improves digestion. (P5)
Even when infant formula is recommended by a doctor, families do not always follow preparation guidelines due to limited knowledge or resources. The LHWs recognize that improperly prepared formula can lead to illness for the child, but they are not trained to provide guidelines themselves. Yes, there are some who come and say that the baby’s stomach is not doing okay, and that is because they don’t understand how to even give the formula, in what proportion to add water, etc. They just do what they are able to understand, and so of course the baby gets sick and then they have to come here, but this is very rare like maybe one case. (P1)
Families are reluctant to continue using infant formula as it is expensive and not easily accessible in their communities. LHWs reported that families would only purchase it once after it was initially suggested by the doctor but not again because it is not an affordable substitute for human milk.
Management of Breast Conditions
The LHWs described that it was difficult to identify and manage breast conditions, which resulted in them giving advice that was not based on clinical guidelines. The participants were unclear about the best course of action in the case of a plugged duct or mastitis, and in some cases they advised discontinuing breastfeeding. The terminology for breast infection and wounds overlapped with the milk itself being bad. In the case of wounds or lumps in the breast, the LHWs typically correctly refer mothers to the hospital. The LHWs used “zehar baad” as an umbrella term in their local language to describe any type of breast infection in which the milk cannot be fed to the child. First thing is that there can be a lump in the mothers breast (because of accumulated milk) which can be cancerous and sometimes people overlook it, but we refer them to the hospital immediately because that is what a lot of mothers complain about that they feel a lump and pain in the breast. (P9) [Zehar-baad] happens to the milk. It’s a condition, due to which you get wounds and then it slowly gets worse, so if that happens, they are not able to feed. (P1)
Lack of clarity on how to diagnose and treat breast issues and conditions often results in unnecessary discontinuation of breastfeeding because LHWs believe that mothers are physically unable to provide their own milk. Moreover, the LHWs see that when such cases are referred to the doctors, the general guideline is to recommend formula milk. Doctors definitely advise mothers’ milk, but when mothers say they are unable to feed because the milk is not coming out—because of pain or cuts on nipples—that is when they switch to formula instead. (P4)
Nipple/Breast Preparation
Two LHWs recommended that women with flat or inverted nipples prepare their breasts/nipples during pregnancy by wearing loose fitting clothing and massaging their nipples. A lot of mothers have their nipples inverted (they are inwards), so we tell them that they need to stop wearing bras and can wear tank tops or just something loose so that every time they take a shower or change, they can sort of rub their nipples and massage to bring the nipples out so the milk is going to start coming out. (P8)
Three participants mentioned that they instruct mothers to wash their breasts with lukewarm water before breastfeeding or wipe off with tissues in the cases where there is a lack of clean water even though washing breasts before feeding is not necessary and can be detrimental to breastfeeding. They also described that washing before breastfeeding was recommended by mother-in-laws. Washing it [the breast] first with lukewarm water means that if there is anything formed on the nipple which is a little hard, it comes off and then the milk can come out smoothly and they can continue when they return home. (P11)
LHW Counseling Strategies
Strategies LHWs use to promote breastfeeding include leveraging their role as established members of the community, conducting frequent visits, building trust, sharing personal experiences, and providing counseling with multiple family members present. They use this position to educate the community, focusing on the health benefits of human milk and the religious recommendation for breastfeeding.
Member of the Community
LHWs gain trust by living in the community and being within reach when needed. They see themselves as a trusted source of information in the community, and they believe families value their advice and generally follow it regarding infant feeding/breastfeeding. I would say when we carefully explain to them, they listen and follow our advice. There has been a substantial change in the way people think now—we have really been able to bring about this change. We live in the same community; they know we are not going to leave this place, they listen to us because we are going to be here, whatever we say they will follow. (P3)
Frequent Visits
Participants start visiting mothers at home prenatally with monthly frequency through the eighth month, then weekly until delivery, with continued visits and support after the baby is born. They may also stay in contact by telephone. The exception is when a mother returns to her mother’s home for delivery and the following 40 days. They stay in touch with us … No one really goes for a very long time, it is usually a month and that too if it is the first baby. This is also because they follow the tradition. The ones who are sensible still do feed, vaccinate if they are away and if they do not then when they return, we get the vaccinator to come, tell them about the benefits of the mother’s milk. (P3)
Through this contact, the LHW plays a central role in providing education related to infant feeding. Frequent home visits mean that they are able to engage with families, hear their concerns, and advise them on a regular basis. The most effective way is that you need to make up the mother’s mind since the very beginning, we have posters, etc. so since the start of their pregnancy we start convincing them, and I think that is the best way. (P6)
Trust-Building
LHWs build trust with mothers by sharing their own experiences, both challenges and successes. They indicated that developing rapport with mothers is a key factor in convincing them to breastfeed and become comfortable reaching out when they need support. In addition, what they are teaching is in line with their stated beliefs about breastfeeding. My personal belief is that I will tell her about my own experience with breastfeeding: I have exclusively breastfed my child for the first six months and did not give any water or any other drink and never spent even a penny on any medication. And they say oh sister, your kids are so healthy and strong. (P9)
Over time with frequent home visits and positive outcomes, they believe that their influence in the community has increased and their advice is taken. A few participants also reported that mothers considered them to be their trusted confidantes and would reach out to them for advice on their personal matters as well. Then we worked really hard on guiding them and now thankfully people really listen to us and actively follow our advice. (P2)
Role of the Family
Several LHWs described the role of the mother-in-law, and in some cases the sister-in-law or the father, in feeding decisions. The dynamic within the family unit plays a role in the influence of the other family members. In cases where the mother-in-law has a strong influence, educating mothers might not be sufficient, particularly if they have more traditional beliefs that promote discarding colostrum and giving prelacteal feeds. So if in the family, the mother is strong-headed, then she takes these decisions. But if she is under pressure from the mother-in-law, sister-in-law or husband, then she also has to listen to them because when the child is born, the mother is weak. She does not want to take all the decisions herself. The mother-in-law starts saying give her rose water, etc. She is weak and so she can’t pay much heed to what is going on; she just goes with the flow. (P5)
The views expressed by dominant family members can also have a strong influence on the way the LHW communicates. Some participants adapt their counseling based on the family’s views and education. In some cases, the mother-in-law could hinder the interaction between the mothers and the LHWs by restricting her access to the household if she feels that the advice being given is not aligned with her own beliefs. Therefore, LHWs have to dedicate additional time and effort to convince skeptical families about the positive health outcomes related to breastfeeding. And also guiding the mother-in-laws in an effective way—tell them that this child is also related to you, your future depends on him/her! (P3)
Benefits of Breastfeeding
The LHWs were well versed in the health benefits of breastfeeding for mothers and children and use this information to encourage breastfeeding when talking with families. Participants described how breastfeeding is like a first immunization and continues to offer health benefits throughout life for the child and exclusive breastfeeding during the first 6 months of life can increase birth spacing for mothers. They share this information with families when they educate them on the importance of breastfeeding. We start in the seventh month, we tell them that the child will be healthy, will not get sick and that you will not become pregnant again. (P8)
Addressing Misconceptions
Participants address common misconceptions when they counsel mothers on breastfeeding. Myths include that an insect should be thrown in the milk to check its quality and that pregnant mothers should discontinue breastfeeding. They listen to each and every thing the LHWs say to them, but the ones who have mother-in-laws who are old school, they say that they are pregnant so the milk is not okay anymore, it will affect the child, etc., so myths like that. So we tell them (mother-in-laws) that there is nothing like that, this will not harm the child. (P3)
Faith
Participants use faith as a strategy for promoting breastfeeding, particularly for the first feedings instead of honey or water. The simple way we do that is we tell them that Allah has made the mother’s milk full of nutrition, they don’t need water or honey or anything else at all to fill up their stomachs. (P3)
Religious support for breastfeeding follows that God sent the child and provided a way for the mother to nourish the child. The belief that milk can be poisonous is not logical because Allah would not have provided milk that was not good for the child. So mothers would say our milk is not okay and we ask them “how would you know your milk is not okay?” Then they say they would put an insect in the milk and if it dies then that confirms the milk is not okay. We tell them this is not right because putting anything in the milk means it will drown and die. Allah provides this diet for the child and it is absolutely okay, this is just in your mind. (P7)
Discussion
Participants’ knowledge and retention of information varied based on their training, personal experiences, and the clinical issues they encountered with the mothers in their respective catchment areas. Our research indicates LHWs are well versed regarding the benefits of breastfeeding and the importance of the first feeding and colostrum; however, they had misconceptions and lack of knowledge regarding positioning to facilitate the first feeding after delivery, the physiology of milk production, milk expression, preparation of human milk substitutes, and management of breast conditions. LHWs incorporated several strategies to promote effective breastfeeding practices. Our study found that LHWs leverage their role as trusted members of the community to serve as teachers, confidants, and mentors for the women in their community and are also able to use this position to educate older women in the community as needed. They are able to counter misconceptions and resolve conflicts within the family related to feeding decisions for the child by counseling mothers in the presence of other family members, disseminating knowledge about the health benefits of breastfeeding for the child, and emphasizing the importance of breastfeeding as encouraged in the Islamic faith.
As previously mentioned, national rates of skin-to-skin and breastfeeding initiation within an hour of delivery are low (Agha et al., 2019; Akhtar & Shaikh, 2019). However, our study highlights that LHWs demonstrate strong knowledge about the benefits of breastfeeding for mothers and infants and use frequent educational visits to improve breastfeeding knowledge in the community. They emphasize that breastfeeding is more convenient compared to formula, is cost-effective, and can significantly reduce the return of the postpartum menstruation/increase birth spacing. As noted by the LHWs in the study, the lactational amenorrhea method (LAM) can be an effective method of birth control and has been shown to provide >98% protection from pregnancy for women who are amenorrheic and exclusively or nearly exclusively breastfeeding their infant for the first 6 months of life (Kennedy et al., 1989). LHWs also strongly advocate against prelacteal feeds, but traditional beliefs that water, honey, and tea are safe for the baby to consume along with the mother’s milk are still widespread in the community (Ahmed et al., 2018; Akhtar & Shaikh, 2019; Asim et al., 2015; 2020; BSP, 2018; Fikree et al., 2005). While traditional prelacteal feeds are common in low- and middle-income countries, they delay breastfeeding initiation and can have a negative impact on breastfeeding exclusivity (Neves et al., 2022).
In Pakistan, women may have a preference for general over regional anesthesia despite its impact on recovery and initiating breastfeeding (Ahmad & Afshan, 2011). LHWs described the difficulty of initiating breastfeeding with mothers who have a cesarean birth or who are too tired to sit up to breastfeed. However, research on laid-back breastfeeding (also called biological nurturing, where the parent lies back in a semi-reclined position) and self-attachment during first feed indicates that both side lying and laid-back positioning facilitate breastfeeding for mothers who are not able to sit upright (Puapornpong et al., 2017). Furthermore, most LHWs did not understand the physiology of milk supply (Ahmed et al., 2018), incorrectly indicating that supply was primarily dependent on maternal nutrition. This is particularly relevant because concerns about low milk supply are commonly cited by mothers as a reason for discontinuation of breastfeeding (Moyo et al., 2020; Zakar et al., 2018). While maternal malnutrition in low-resource settings can affect the micronutrient content of milk, particularly with B vitamins (Allen, 2012), milk removal rather than the quantity or quality of maternal diet is the primary driver of milk supply (Kent et al., 2016). Providing more training for LHWs about the options for breastfeeding positions that facilitate the first feedings could increase early initiation rates, while content on supporting an adequate milk supply would increase breastfeeding duration.
Our research showed a lack of support for working mothers, especially related to hand or pump expression of milk when the mother is separated from the baby. Hand expression is an evidence-based skill for supporting breastfeeding and expressing milk when pumps are not available or affordable (Becker, et al., 2016; Flaherman et al., 2012), but LHWs need more training to incorporate hand expression and pump practices to support mothers per WHO guidelines (World Health Organization, 2017). Furthermore, recommendations for the safe preparation of formula and animal milk among study participants were unclear; instead, they emphasized the importance of exclusive breastfeeding. While human milk is optimal for infants, safe preparation of formula and guidance to reduce the risk of the common practice of feeding animal milk could improve infant morbidity and mortality (Saeed et al., 2020). Ultimately, teaching mothers how to express and store their milk when separated from their baby would provide the best infant health outcomes due to the demonstrated benefits of human milk over formula or animal milk feeding (Victora et al., 2016), particularly in this setting where formula feeding is not affordable, sustainable, or safe due to poor water quality and sanitation (BSP, 2018).
Participants demonstrated a lack of understanding about the management of breast conditions including engorgement, plugged ducts, mastitis, and abscess. During interviews, variations in their responses and difficulty elaborating about breast issues faced by mothers indicated that this was not a core area of focus of their training. Although these topics are covered in the LHW training manual (IRMNCH and Nutrition Program, 2019), participants were unable to differentiate between breast conditions or provide clinical guidance on their management. They also had misconceptions about the need for treatment of flat or inverted nipples and the need to clean the breast before feeding. While drawing out nipples was commonly described and is supported for inverted nipples (Youssef Ahmed Abd-Ella & Fouad Mohammed, 2021), there is a lack of clinical evidence to support the preparation of flat or inverted nipples prenatally (Mitchell & Johnson, 2022; Walker, 2013). Washing breasts before feeding is not an evidence-based practice; in fact, it can remove the natural odors that babies use to locate and latch on the nipple (Doucet et al., 2007). However, it is a common practice in several parts of the world including Pakistan (Chachar et al., 2019; Shobo et al., 2020). This practice can delay breastfeeding and, in areas where access to clean water is limited, introduce pathogens. In Pakistan, only an estimated 20% of the population has access to clean water with both fecal and toxic chemical contamination common in the household water supply (Daud et al., 2017).
Previous research highlights the effective use of home and community-based counseling and education to promote optimal breastfeeding practices (Haroon et al., 2013; Sinha et al., 2015). Additionally, increased duration and frequency of prenatal breastfeeding counseling improves breastfeeding practices (Benedict et al., 2018). The LHWs in this study report that they build trust with families through frequent visits, and mothers are more willing and able to initiate breastfeeding in their presence. LHWs also provide moral support that serves as a barrier against contrary feeding advice by family members, particularly the mother-in-law as she is often considered an authority on the matter (Negin et al., 2016), given her experiences with childbearing.
As previously studied, LHWs display a strong sense of self-confidence and over time have been able to influence overall decision-making within the households they serve, which has led to positive perceptions of community health workers (Oxford Policy Management, 2009b). Our results indicated that LHWs use a reflexive approach when engaging with family members regarding commonly practiced myths such as the colostrum being poisonous. For example, they may improvise their counseling for elder family members to challenge misinformation. As a result, they are able to gain the trust of the other members of the household, such as the infant’s father and grandmother, who have a strong influence on the child’s feeding decisions (Mithani et al., 2015; Negin et al., 2016; Zakar et al., 2018). Therefore, LHW counseling strategies targeted toward mother-in-laws should continue to disseminate accurate and up-to-date knowledge of breastfeeding guidelines and practices that can add to their traditional knowledge base and enable them to increase support for breastfeeding (Moyo et al., 2020; Negin et al., 2016).
The Islamic faith guides that women should breastfeed for 2 years, and existing research demonstrates that many mothers are aware of the teaching from the Holy Quran (Chachar et al., 2019). In our study, LHWs report that mothers are aware of the importance of breastfeeding for 2 years and its nutritional value for the child. LHWs also include the teaching that the dietary needs of the child are fulfilled by God through means of breastmilk (Bayyenat et al., 2014) and therefore no supplementation is required, in their counseling sessions with families. Hence, LHWs can discourage the practice of discarding colostrum and exclusive breastfeeding by emphasizing the teaching from the Quran.
Conclusion
Our study demonstrates that LHWs engage a variety of strategies to promote positive infant feeding practices in their communities. They are aware of the impact of their work and their position within the community that allows them to influence feeding decisions within families. They are also well versed in the benefits of breastfeeding and providing support during the perinatal time.
The findings of this study may not be generalizable to other contexts as the performance and experiences of LHWs could vary based on their individual qualifications, geographical location, and health infrastructure in their respective catchment areas. Moreover, the study is also at risk of social desirability and recall bias as participants who were interviewed could have overestimated their role in the community and the impact of their work. The analysis and interpretation of the data are subject to the researchers own experiences, background, and prior assumptions. Hence, the researchers used active listening and probing during interviews to overcome any insider bias, and the two authors worked independently to prepare the codes, write vertical memos, and identify themes that were then compared and incorporated in the final codebook.
Despite these limitations, this study highlights the role of community health workers in promoting breastfeeding in rural communities and identifies gaps in clinical lactation training for future targeted interventions. In order to maintain and expand LHW skills, there should be a robust system of updating the training curriculum, providing regular refresher training, and evaluating the impact of delivered training on LHW knowledge and efficacy. Curriculum updates should address the physiology of milk supply, milk expression, and the management of breast and nipple conditions to fulfill the lactation needs of mothers in rural communities. Overall, maternal and child health would benefit from more formalized and coordinated efforts to ensure that training is provided to all levels of healthcare staff, including the community workers as well as those based at the health facilities such as nurses and doctors.
Supplemental Material
Supplemental Material - Beliefs, Experiences, and Practices of Lady Health Workers in Facilitating Breastfeeding in Rural Communities in Pakistan
Supplemental Material for Beliefs, Experiences, and Practices of Lady Health Workers in Facilitating Breastfeeding in Rural Communities in Pakistan by Nicola Singletary and Zoha Waqar Farooqi in Qualitative Health Research
Footnotes
Acknowledgments
Fieldwork research budget was provided by Professor Erica Field, Duke University. We would like to thank the lady health workers who participated in this study. The findings from this qualitative study were used to design an intervention to meet the lactation training needs of LHWs in rural communities, in a scalable and cost effective manner.
Author Contributions
Both authors contributed to the study conception and design, data analysis, and manuscript preparation. Data collection and translation were performed by Zoha Waqar Farooqi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by USAID DIV, Award No. 7200AA22FA00002, and Weiss Fund, Award No. DUK-001.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.