
Abstract
For the past years, Ecuador has been transitioning away from a hospital-based model of mental healthcare to one that is community-centred. However, challenges associated with hospital-based models endure, notably financial burden faced by those with severe mental health problems (SMHPs) due to labour market discrimination. Employment access for this group is often disregarded in policy planning, despite evidence of its benefits on mental health. Huertomanías, an urban garden initiative in Ecuador founded in 2015, works with individuals with SMHPs, providing work, income, and social inclusion. A case study using a participatory approach was carried out to explore factors that impact the recovery of people with SMHPs. Twelve participants engaged in diverse stages of the research, where several participatory activities were conducted including cognitive mapping, a photovoice project, and interviews. The analysis employed a thematic approach leading to four categories of impact within the urban garden: autonomy (financial and personal), interpersonal relations and relation with the environment, mental health, and family dynamics. A final category of impact was established encompassing external factors (family support and public policy and healthcare services) that influence recovery. Findings suggest that the urban garden promotes autonomy and active participation within society, improves mental health, and transforms family dynamics. Further, this study highlights the importance of community-based mental healthcare (CBMHC), emphasising the need of public policies and healthcare in promoting autonomy through employment and community-centred services. Lastly, the study contributes insights into recovery experiences and CBMHC benefits, informing programme development and similar initiatives in Latin America.
Keywords
Introduction
Mental Health in Context: Ecuador
In 2014, the Ecuadorian government launched a National Mental Health Strategic Plan (Ministerio de Salud Pública del Ecuador, 2014), which aimed to promote a community-based model for mental healthcare, and initiated the country’s transition away from a hospital-based model (PAHO, 2013; Pūras, 2020). The community-based model seeks to promote mental healthcare that is accessible, participatory, uninterrupted, preventive, and comprehensive (Minoletti et al., 2012; PAHO, 2013). However, the extent to which the aforementioned plan has been implemented is unknown (Asamblea General Naciones Unidas, 2020).
Despite these efforts, challenges still remain for people living with mental health problems in the Ecuadorian context. For example, the financial burden for people living with severe mental health problems (SMHPs) is often particularly high. People living with SMHPs are largely excluded from the labour market, either due to discrimination or a lack of flexibility of work conditions, for example, lack of understanding when there is work absenteeism due to hospitalisation (Román, 2019).
In high-income countries, only around 10–15% of people living with SMHPs have access to a job (Drake et al., 2020; Drake & Wallach, 2020); this number is expected to be lower in low- and middle-income countries, such as Ecuador. This leaves thousands of people living with SMHPs confined to their homes – depending economically entirely on their families – psychiatric hospitals, or living in the streets (Drake & Wallach, 2020). Access to employment for this group remains inappropriately addressed in policy planning, despite evidence that participation in the workforce leads to increased mental health and well-being of people living with SMHPs due to the promotion of positive self-esteem, better symptom control, increased quality of life, social relationships, and community integration (Drake & Wallach, 2020).
Furthermore, a qualitative metasynthesis has highlighted that individuals facing mental health challenges recognise several advantages of employment, including greater autonomy, societal acceptance, and opportunities for personal development (Modini et al., 2016). Lastly, a study focusing on participants with psychotic illnesses revealed that employment correlated with an enhanced level of functioning and a decrease in negative symptoms (Wallstroem et al., 2021).
The Case of Huertomanías, a Social Entrepreneurship for People with SMHPs
Huertomanías was founded in 2015, during a mental health community assembly with people living with SMHPs, family members, and healthcare professionals in Quito, Ecuador. The project is a person-centred, community-based mental health (CBMH) device, which aims to support the well-being of people living with SMHPs in Ecuador, through financial autonomy, care for the environment, and social inclusion (Montenegro et al., 2021). A person-centred approach seeks to promote living a life that does not revolve around illness and prioritises people’s own needs and decision-making processes (Davidson & González-Ibáñez, 2017; Macías Saavedra, 2011).
Working at the intersection of human rights and healthcare, Huertomanías was created as a safe space for people living with SMHPs to exercise their human rights by promoting their autonomy through work, income generation, access to information, and participation in organisational decision-making and by strengthening their social network and peer support (Montenegro et al., 2021). Huertomanías members are called ‘partners’, since this word emphasises their equal and active role within the programme; they are not ‘patients’ nor ‘workers’ but rather active members that have a central part in the decisions and direction of the project. Partners are adults who have been excluded from the labour market due to stigmas related to their mental health problems (schizophrenia, severe depression, and bipolar disorder) and who are economically dependent on others, often their families.
Huertomanías has been operating on 1600 m2 of cultivated land in Nayón-Quito. Their crops are cultivated under permaculture principles, and the produce is processed to obtain jams, sauces, infusions, flavoured salts, etc. (see Images 1 and 2). They hold events such as workshops on garden management based on permaculture techniques, harvest days with the community, workshops on human rights and deinstitutionalisation, film forums on SMHPs, exhibitions, and festivities (Image 3). All these activities are strongly rooted in the person-centred and human rights–based approaches described in the WHO guidelines on community mental health services (WHO, 2021). In addition, Huertomanías is also a learning space for students from different academic backgrounds, through a student internship programme. Huertomanías’ products. ©Elizabeth Dalziel in collaboration with Ember Mental Health. Huertomanías’ partners working. ©Elizabeth Dalziel in collaboration with Ember Mental Health. ‘Freedom is therapeutic’ sign. ©Elizabeth Dalziel in collaboration with Ember Mental Health.


The Current Study
This study aimed to evaluate the impact of the Huertomanías programme on the recovery of its partners. Evaluations of community interventions’ impact on people are essential to provide evidence on effectiveness, as well as to identify possibilities for improvements and increase their opportunities for impact-based funding. This study is unique in that it offers insights into a community-based organisation promoting autonomy through financial independence in Ecuador. Thus, the results of this study will not only contribute to the internal strengthening of the Huertomanías programme but also contribute learnings for others intending to develop similar projects in Ecuador or Latin America more broadly.
This work was conducted as part of a larger study with three objectives: (a) to understand the meaning of recovery for partners with SMHPs, (b) to explore the impact of Huertomanías on the recovery of its partners with SMHPs, and (c) to explain the processes and mechanisms by which this impact occurs. The current paper reports the findings of the second and third objectives.
Method
Design
We used a case study design to explore the impact of Huertomanías on the recovery of its partners living with SMHPs. Yin (2009) indicates that case studies are suitable for capturing complex social phenomena in a holistic and meaningful way, while at the same time allowing the exploration of contemporary phenomena in depth within the context in which they occur. Huertomanías was the main unit of analysis, which was composed of different subunits: the partners with SMHPs, their family members, and their mental healthcare professionals (Urra Medina et al., 2014).
To explore the perspectives of each group, we used qualitative methods (Yin, 2009) under a participatory approach (Vaughn & Jacquez, 2020). To this end, we used participatory methodologies, including cognitive mapping workshops (Cole & Persichitte, 2000), a photovoice project (Carlson et al., 2006; Fleming et al., 2008; Mizock et al., 2014), and individual interviews guided by the Most Significant Change (MSC) method (Davies & Dart, 2005; Serrat, 2017) and involved participants in the interpretation of data during the analysis through feedback sessions.
Sample and Recruitment
All partners of Huertomanías with an SMHP were eligible to take part in the study. Five partners were working in Huertomanías at the time when the study was being conducted. We aimed to recruit all partners, and at least one family member and mental health professional of each partner; so, the initial sample was all five partners, six family members, and two mental healthcare professionals. One partner dropped out of the study after the first stage of data collection; therefore, a total of 12 participants took part in the current study.
Partners with an SMHP were invited to attend an online meeting about the study by the research team. During this meeting, attendees were explained the objectives, procedures, and ethical considerations of the study. Those interested were asked to sign an informed consent. Then, partners were asked for consent to invite their family members and mental healthcare professionals (if available) to take part in the study. Those who provided consent were asked to share an invitation of the study, which had been prepared by the research team. Those family members and mental healthcare professionals who were interested in taking part were invited to an online call where the aims, procedures, and ethical considerations of the study were explained before being asked to sign an informed consent. For all participants, the informed consent emphasised that all data collected would be anonymised and remain confidential. Participants were also informed that their decision to take part or not in the research study would not have an impact on their participation and involvement in Huertomanías.
Data Collection
Data collection was carried out between March 2021 and July 2021 by a group of four Spanish-speaking researchers with backgrounds in Psychology and/or Global Mental Health and with experience in conducting qualitative research. As shown in Figure 1, the data collection process was divided into three phases: (1) Cognitive Mapping (Cole & Persichitte, 2000), (2) Photovoice Project (Carlson et al., 2006; Fleming et al., 2008; Mizock et al., 2014) and Interviews Guided by the MSC Method (Davies & Dart, 2005; Serrat, 2017), and (3) Feedback Sessions. This selection of data collection techniques was deliberate and aligned with the participatory approach of this research. The primary focus was to recognise that partners held invaluable insights into their own recovery processes, and these techniques allowed us not only to capture the perspectives of the participants but also to emphasise and facilitate their direct engagement in the research process. Data collection process.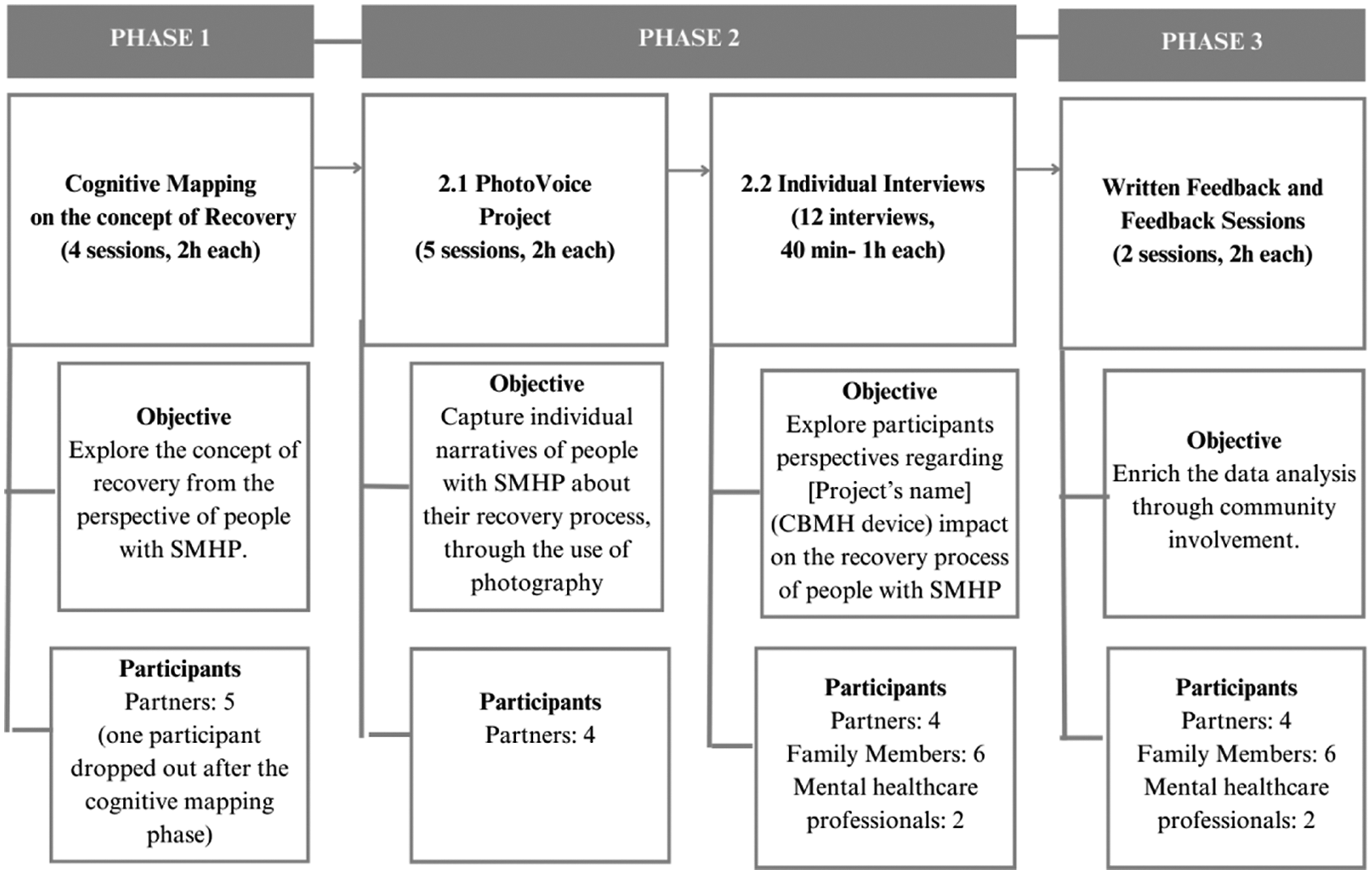
Phase 1: Cognitive Mapping on the Concept of Recovery
Four cognitive mapping sessions of 2 h each were held to define ‘recovery’ from the perspectives of partners with an SMHP and identify the main factors that influence their recovery process. Workshops were guided by two questions: (a) What comes to your mind when you think of recovery from a mental health problem? and (b) What factors do you think are associated with this recovery and your well-being? The sessions were conducted either face to face or online via Zoom. Sessions were audio-recorded and transcribed verbatim for analysis. Through these cognitive mapping sessions, recovery was defined as ‘the non-static and non-linear process, with ups and downs, in which one copes with the illness and walks towards well-being’. This definition was used to guide the subsequent phases of this study.
Phase 2.1: Photovoice Project
The Photovoice methodology was used to understand the elements that the partners consider important for their personal recovery process (Wang & Burris, 1997). They were asked to create photography projects around two themes: (a) ‘my recovery’ and (b) ‘the impact of Huertomanías on my recovery’. Five sessions of 2 hours each were held by a professional photographer and the research team to introduce photography techniques and photovoice methodology and its ethical considerations. Several meetings were established to comment on the progress of each photography project. The final stage of the project consisted of individual meetings with the partners, in which each of them selected around 10 photographs and created a short narrative (100–150 words) that best represented its reality and the selected theme. A final group session was convened in which each participant presented their final project. Finally, individual interviews with each partner were conducted to delve deeper into the participants’ photovoice projects. These interviews were audio-recorded for later transcription. A total of 6 hours of transcription were used for later thematic analysis (see Appendix 1 for full interview guide in supplementary material).
Phase 2.2: Individual Interviews
Twelve individual interviews were held with family members and their mental healthcare professionals. The interviews lasted between 40 minutes and 1 hour and were carried out via Zoom. The interview guide (see Appendix 2 in supplementary material) was based on the Most Significant Change (MSC) methodology (Davies & Dart, 2005; Serrat, 2017) and inquired into the participants’ perspectives on the health and well-being of Huertomanías’ partners prior to their participation within the programme and its impact on their recovery process.
Phase 3: Written Feedback and Feedback Sessions
Due to the participatory nature of this study, two feedback sessions of 2 hours each were held with the participants during analysis and interpretation of data at each stage (see Figure 1). When more convenient for participants, feedback was received in written format. Community involvement in the analysis and interpretation phases of participatory studies occurs less frequently than in other research phases (Cashman et al., 2008). However, this was considered essential to this study – the joint interpretation of data in which different perspectives are articulated and integrated enriches study results. Importantly, this process ensures that the study’s findings are faithful to the experiences and stories of the participants.
Data Analysis
Transcripts from interviews conducted in Phases 2 and 3 were analysed in their original language, Spanish, using Dedoose software to help organise data and following the approach described in Gale et al. (2013).
All four researchers familiarised themselves with the data by reading all transcripts, writing memos on key emerging themes, and conducting a group discussion to reach an agreement on an initial analytical framework, which parsed the data into three broad categories: (a) Huertomanías’ impact on the recovery process of its partners; (b) external factors that impact the recovery process of Huertomanías’ partners; and (c) Huertomanías’ opportunities for improvement.
This analytical framework was then applied to the data by EZ and BH. Subsequently, the resulting codes were reviewed by all four researchers to develop a more detailed coding framework, which was then also applied to the data by EZ and BH in line with the thematic analysis process (Gale et al., 2013) (see Appendix 3 for detailed themes in supplementary material). All transcripts were coded by two researchers independently. The final resulting themes were reviewed and discussed by all researchers.
After the feedback sessions, any new emerging themes were incorporated into the results. Content selected for inclusion in the report was translated to English, and specific quotes were discussed with two independent native Spanish-speaking researchers to verify the accuracy of the interpretation. For full details of the analysis along with a full coding framework, see the supplemental data.
Ethics Statement
The current study received ethics approval from the Comité de Ética de Investigación en Seres Humanos (CEISH) at Universidad de las Américas – Ecuador (reference number: 2020-1020). All participants gave their informed consent for all the phases of the study.
Results
Three main themes were identified through the analysis: (a) the impact of Huertomanías on the recovery process of its partners; (b) external factors that impact the recovery process of partners; and (c) Huertomanías opportunities for improvement.
Huertomanías’ Impact on the Recovery Process of Its Partners
Participants described Huertomanías as (a) a workspace, as (b) a space for social interaction, and as (c) a space for emotional support. Across these three areas (see Figure 2), four factors were found to have an impact on the recovery process of partners with SMHPs: autonomy (financial and personal), interpersonal relations and relation with the environment, mental health, and family dynamics. These areas are not mutually exclusive but rather intertwined in complex ways (see Figure 2). Huertomanías’ (CBMH device) impact on the recovery process of its partners.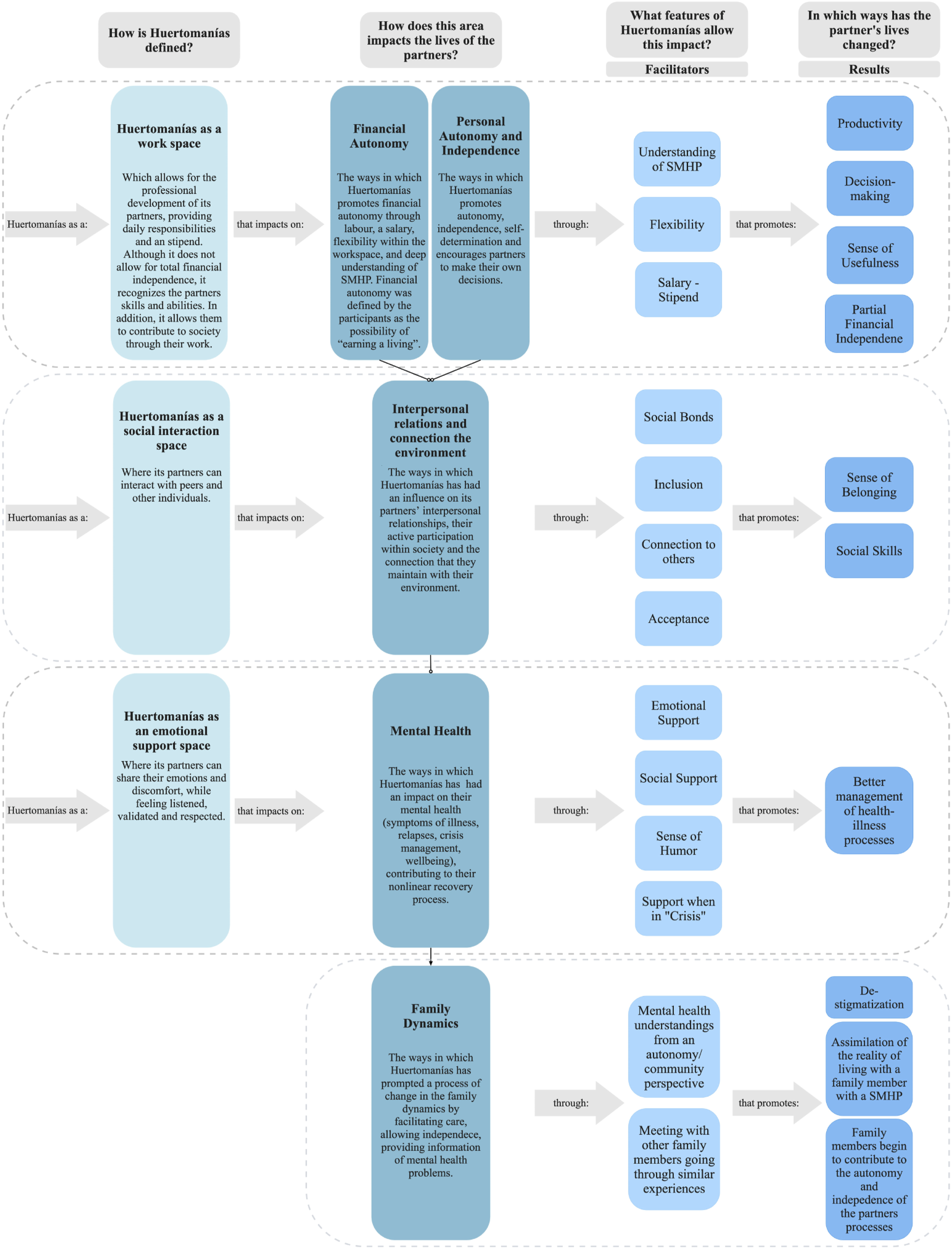
Autonomy
Financial Autonomy
Financial autonomy was defined by participants as the possibility of ‘earning a living’, in this case facilitated by Huertomanías through the stipend received for working in the garden and delivering workshops, guided visits, and selling products. This opportunity for financial autonomy was reported to foster a sense of usefulness and productivity. For example, one family member described how feeling remunerated for work at Huertomanías brought their relative a sense of value and happiness: I think it’s about feeling useful [...] And I see that it makes them happy when they make a contribution to the house and bring some money home. (F41 y F42)
Partners attributed these feelings to being able to generate an income of their own: The money I earn every month is important. One always needs money and when I work, I feel good because I see how my finances progress. (S3)
However, various family members and mental healthcare professionals raised a concern that the partners’ stipend at the time did not offer total financial autonomy: [...] in order to obtain total autonomy, an amount of income is obviously needed [...] and I think that is the struggle that has not been met, not yet. There are still many difficulties so that the amount of income is sufficient for you to have this autonomy. So that would be like the missing aspect yet in this element of autonomy. (PS1)
Personal Autonomy and Independence
Participants described Huertomanías as a project able to promote independence and self-determination and which encourages partners to make their own decisions. This is driven by participatory work, assembly decision-making processes, and also the stipend received. A mental health professional shared their opinion on the importance of the stipend for fostering independence and autonomy. This allows us to exemplify how financial autonomy and personal autonomy and independence are intertwined. I think it’s a very important element [the stipend they receive at Huertomanías] because it provides a greater sense of autonomy and independence, because [the partner] won’t just depend on someone else to take care of them when they are not feeling ok, but they can sustain and support themselves even to a lesser extent. (PS1)
Family members also described the change in their relatives and how this led to a shift in the relationship and division of tasks within the home: Yes, for us, as a family, it has been a benefit too [...] The peace of mind of knowing that they know [how to do things], because I thought they couldn’t. It was difficult for them to communicate, even more so to move around. [...] And, now, even at home, with house chores, in things like buying food, things that they have to take care of, they can do it. (F4.1)
Interpersonal Relations and Participation
This theme emerged from participants’ accounts of Huertomanías influencing partners’ interpersonal relationships and the relationship that they maintain with their environment. According to participants, Huertomanías was able to generate a deep sense of belonging: [Huertomanías has helped the partner] in feeling accepted, in feeling that there is a place where they could go, where they would be understood to a certain extent [...] that helped them feel a sense of belonging. I mean, they would say “I’m a part of Huertomanías.” That helped. (F5.1)
Additionally, participants described that Huertomanías promotes their active participation within society. As a family member explained: Being able to go to different places, when they participated in the sale fairs every Sunday. They went to museums, to all the activities that were scheduled, like participating in mental health forums. They have given an interview on the radio, and all these things [...]. (F4.1)
Some family members shared how their relatives had previously isolated and how they had lost their connections with the world due to stigma and discrimination regarding their mental health; however, they also described how Huertomanías benefits their relatives in providing access to spaces where they can navigate on social worlds: ... [Huertomanías’ director] has not isolated them from the world, she has welcomed them to the world; and in this world where they live, in the one we live in, she has introduced them to a lot of people. (F3)
Participants reported Huertomanías has been an accepting, inclusive, and flexible work space, which allows them to develop social bonds, to connect and experience fraternity. As mentioned by one partner: Huertomanías is being a part of a project which seeks to embrace differences, which seeks to build a community, which seeks to be democratic by giving everyone an equal value, and where there’s a lot of good humour and friendships. (S1)
In addition, the garden space emerged as an important component to help form a deeper connection with the environment. In fact, to be able to be in contact with nature was described as “therapeutic even though it’s not therapy” (F3): We work in a garden where there are flowers, plants and animals. This helps me to identify myself with what I’m doing, with the contact with nature and ecology. (S3)
In relation to the above, a family member also mentioned: Huertomanías is a space where you can remember, that plants continue to grow, that the products continue to come out. And there’s this important symbolism of the soil: the cycle of life, the cycle of death, the cycle of production, of harvest, the sowing, the sun, the moon, all that. So, I believe that this is good for [their partner] and to embrace her condition. (F1)
Mental Health
Beyond the accounts of Huertomanías supporting its partners by fostering their autonomy and providing a space for relationships to be nurtured, participants directly referred to the impact of Huertomanías on their well-being and mental health management. They described the validation received from coworkers with mental health knowledge, the job’s flexibility, the social support offered by peers, and the sense of humour infused throughout the programme as factors that promoted acceptance of the diagnosis, adherence to treatment, and crisis management, thus contributing to their non-linear recovery process.
A family member shared an experience that portrays their view on how Huertomanías’ members have supported its partners’ mental health by being knowledgeable about mental health problems and through their willingness to be in contact with their mental healthcare professionals.
The bigger context of this quote narrates the experience of a partner wanting to quit their psychiatric treatment because their doses were augmented excessively, to which Huertomanías’ director accompanied them to negotiate on those doses: S3 had stopped going to his psychiatrist for some time and did not want to go back because their medication doses were augmented excessively, [..] But [Huertomanías director] probably suggested that they go back to the psychiatrist and continue with the treatment and see how it goes. I have seen her take care of those things, and not only with S3, because she knows all the psychiatrists who treat them. [Huertomanías director] accompanied S3 to go to the doctor again, obviously, we both were there with them. (F3)
In line with the above, F3 also shared that within Huertomanías, the team not only demonstrates a commitment to supporting partners during the process of engaging and negotiation with their psychiatrists but also establishes Huertomanías as a designated space where partners are given the opportunity to openly question and address their doubts around medication, encompassing aspects such usage, dosage, and side effects: But he [Huertomanías’ Partner] told her [Huertomanías’ Director], “I want you to tell me what these pills are for and what side effects they have.” So, she resolves their doubts, she resolves their anxieties, even if it’s about their treatment, because that gives them security and then they [Huertomanías’ Partners] continue with the project, they continue working. (F3)
Moreover, an interviewee also suggested that having a structured job, and specifically one that has to do with nature, helped a partner face a depressive episode: When they have had very strong episodes of depression and they don’t want to get out of bed, Tuesday arrives, which is when they go to remove the soil and do more field work, [...] they decide to get up early to go and fight depression. In other words, in those small things, for me that is really significant; that even though they are ill, they have a place to go, where they want to go and that for me is more than enough. (F1)
A family member also reflected on how all members of Huertomanías have contributed to the mental health crisis management of its partners: One day one of the partners had a crisis in the garden, and no one, none of them wanted to leave this boy all alone, no, no, no, no and no. [...] they were there to support the boy [...] So you can see that they respect each other and help each other, they support each other. (F3)
Family Dynamics
Huertomanías was also described as prompting a process of change in family dynamics, facilitating care, understanding of mental health problems, and emotional support (for both, the partners and the families). One family member explained that meeting other people going through similar experiences contributed significantly to understanding things from a different perspective: That was a contribution [of Huertomanías]. Meeting other people who were suffering from the same illness. Seeing other mothers who are also in situations of having children with schizophrenia does give you another perspective. That is a contribution. I mean, there should exist more support networks and in the garden I found four families, which, within the community is minimal; but at least we are four families who know that we are in a similar situation. And, it helps. [...]. (F5.1)
Family members mentioned acquiring new caring roles, which requires them to de-stigmatise and learn about mental health, incorporating ways in which they can be more supportive. These changes, which are on-going, have been promoted by the opportunities of participating in gathering spaces with other family members, as described above, and by having access to new understandings of mental health that focus on autonomy and community care, as F4.1 and F3 mentioned: We realise that with this type of project the family can assimilate better, erasing the stigmas that there are with this type of illness. (F4.1) Now I tell S3 [partner] “well, you have to start doing things here at home too [...] it’s inside the house where you also have to look after yourself,” I tell them “you have to learn to cook, you have to learn to take your clothes and put them in the washing machine, you have to take care of all that because that is being autonomous, it is not just working, you have to know how to pay for electricity, water, the telephone, go to the ATM, get your money, go to the bank” [...]. (F3)
External Factors That Impact the Recovery Process of Huertomanías Partners
In addition to the impact of Huertomanías, this study found that two other factors have promoted or influenced the recovery process of its partners: family support and public policy and healthcare services.
Family support was described as a fundamental contributor to recovery, particularly to generating and maintaining well-being in the partners’ lives. Similarly, the lack of public policies that prioritise promoting autonomy and deficiencies in healthcare services were identified as barriers to recovery.
Family Support
Participants suggested that family has been an important contributor to the recovery process of Huertomanías’ partners given the care and support, both financial and emotional, that they have provided. For example, F4.1 and F4.2 recalled how they have supported financially their family member [partner], since before he moved in with them, back in 2015. Yes, we have always taken care of [the partner] financially … We even helped them from afar [when the partner lived in another country]. And now, we help them here.
A partner also described how their family has been essential to their recovery: My stepfather, my mother and my father, yes, those are three fundamental pillars, but above all my stepfather and my mother who have been much more involved in my process. (S5)
Despite that the family was consistently reported as a fundamental support system, a level of complexity was identified in this theme; some family members have stories that portray the ways in which they have caused pain, due to the lack of knowledge on mental health or as a consequence of stigma: The family always tends to overprotect and even I started being overprotective until I realised that it wasn’t good for them [...] Huertomanías, gave us the light of that: To be able to let go, to loosen up a bit, because overprotection is bad, very bad. (F4)
An interviewee also expressed how sometimes the family is not able to fulfil all of the partners’ needs: [...] The family system is not able to have all the resources, the solidity, the energy and the conditions to be able to give S5 the containment and the collective support [...] that they need. (PS5)
The aforementioned quote demonstrates the burden that is put on caregivers due to the lack of comprehensive policies and appropriate healthcare services that address the needs of people living with SMHPs.
Public Policy and Healthcare Services
According to participants, public policy and the access or lack of access to integral healthcare services has directly affected the recovery process of partners. The absence of public policies related to community mental health was discussed, as well as the deficiencies in mental health services. A healthcare worker explained how multiple services and systems are necessary to address the different needs of people living with SMHPs: What would be ideal, obviously, is to have a network. A network where, on one hand, there is a health care system, and on the other, there are work options, for example, spaces such as Huertomanías [...]. So, the idea is that, ideally, there would exist such networks. Yet somehow, it doesn’t exist in the country. We have a health care system that isn’t working as a network and that doesn’t have the capacity to provide all these elements. [...]. (PS1)
The interviewees also suggested that the State should be taking a more active and responsible role to improve the recovery process and quality of life of people living with SMHPs. Improvements suggested included having access to an integral medical treatment or having available medication all year long. Some family members reported that people living with SMHPs seem to be forgotten by the State, since there is a lack of initiative to help them or organisations that work with them. F3 suggested that: [...] the State, as such, should take responsibility. In the same way as with the disabled, that are missing a foot, that are deaf, this and that, the same with mental health. Because sometimes it’s not very noticeable [referring to the disability], and people think that they can do it; but the mind is everything. They need help. They need help so they can work according to their abilities. To include them in any way. Even medical care, any sort of help. The State needs to own that responsibility. Or help the institutions, because private institutions do a lot of things, so the State can help them [...]. (F4)
On the other hand, while some members mentioned that the health system was deficient and precarious, one participant stated that the Ecuadorian health system made it easier for their family to cope with the recovery process. [...] The social system is very important, the facilities that there can be in a country, the attention that there can be from a government. For example, for the disabled, it's important. And for all of us. We were in a bad situation there [country of origin] and here [Ecuador] it changed everything in our life. We started from scratch here. (F4.1)
Huertomanías’ Opportunities for Improvement
Participants described areas where Huertomanías could improve or grow further. Primarily, partners’ relatives agreed that promoting the financial independence of the partners through greater remuneration that allowed for complete financial autonomy was a remaining need: Huertomanías falls short in providing stability and financial independence to its partners. (PS5) Huertomanías has not made it possible for partners to earn a decent salary, it has not gotten to a point where it can become a truly self-sustaining company [...]. (F1)
Some participants also suggested that Huertomanías could be more open to new initiatives proposed by the family, to diversify the activities in the garden and promote greater family involvement. It does not involve the family and other support points as much as it could. (PS5) Finally, the people in charge are not very open to listening to possibilities of expanding the impact beyond a garden. (F5)
Lastly, a family member and a mental healthcare worker suggested incorporating in Huertomanías spaces for cohabiting (housing) for the partners. However, this recommendation surpasses the project’s objectives, although it highlights a wider need within this population: The first thing would be to offer basic infrastructure to live in [...] Similarly to the situation of university students who have access to housing and other services, provided by the university itself. Imagine a daily support network, of course, adapted to the specific needs of that group, whilst being accompanied and supervised. Though, I know this is a very utopian and challenging idea. (PS5)
Discussion
This study offers important insights into the impact of a CBMH device for people living with SMHPs and adds to the general understanding of recovery of mental health problems. First, it highlights that this urban garden project (person-centred, community-based mental health device) positively impacts the recovery of its partners in the following areas: autonomy (financial and personal), interpersonal relations and connection with the environment, mental health, and family dynamics. Second, this research also demonstrates that there are other factors beyond the CBMH device that are key to the recovery process of people living with SMHPs, such as family support (economic and emotional), and public policies and healthcare services. Finally, despite its strengths, the current evaluation allowed us to identify some opportunities for improvement within the CBMH device, such as higher stipends for its members.
Results highlight that having access to a paid job promotes a sense of usefulness, independence, and improved life satisfaction for people living with SMHPs. This is in line with previous literature that has described how access to work allows people living with SMHPs to regain independence in their daily life and its fundamental role in pride and self-esteem (Drake & Whitley, 2014; Modini et al., 2016; Wallstroem et al., 2021). Even though partners at Huertomanías receive a monthly stipend – below the basic salary in Ecuador – participants suggested that the current stipend does not allow for full independence.
However, it is important to note that this limitation was only mentioned by family members and mental healthcare professionals. For partners, the stipend did not emerge as something central – instead, more value was placed on the social recognition and the opportunity to access a paid job. It can be argued that this perception might be influenced by the consistent discrimination in the labour market that people living with SMHPs experience. From that viewpoint, having access to a paid job is already an important achievement, despite insufficient remuneration.
Additionally, the difficulty of the CBMH device to offer its members a salary that allows them for full financial independence does not respond only to its individual operation but rather to the scarce resources available (governmental and non-governmental) to finance and support the growth of community mental health initiatives, as well as the unequal allocation of those funds. This limitation has been previously reported in the literature as an urgent need to be addressed globally, since it significantly hinders the CBMH device’s impact and threatens its sustainability (Larrieta et al., 2023).
This study also examined personal autonomy in relation to the partners’ decision-making, independence, and self-determination. Huertomanías’ participatory approach in the workplace, which includes assemblies for decision-making and opinions/knowledge exchange, likely contributed to this. This approach to work aims to transform internalised beliefs that people living with SMHPs cannot make decisions of their own and that they need to be taken care of by someone else. Participants shared many experiences, in which partners took more responsibilities in their private lives; they improved their ability to perform daily self-care activities and chores and started to take care of others within their homes.
The experiences described above promoted change in family dynamics; families learned to let go of control in care, support, and encourage those processes of independence, while offering emotional and economic support when needed. This transformation was described as complex by family members, since it differed from the forms of care and overprotective practices performed by them before participating in the CBMH device. The overprotective behaviour has been described in the literature as a common practice by family members of people with disabilities, increasing dependence and hindering autonomy (Román, 2019; Siddiqui & Khalid, 2019). In that sense, the work of this CBMH device in supporting families to gain knowledge on the importance of autonomy is transformative and should be taken as an important learning for community mental health. The CBMH device generates a safe space to meet and connect with other families facing similar situations and allows them to feel supported and inspired by similar life stories. These findings resonate with Magliano et al. (2002) who proposed that professional and social network support represents crucial resources to reduce family burden of people with schizophrenia, and it has also been described by PAHO as a facilitator in the process of deinstitutionalisation (PAHO, 2020).
Having a workspace which encourages independence through active participation allows partners to be strongly involved, not only with the permacultural work and the fruits of their labour but also to actively engage and contribute to society through social and political events promoted by the CBMH device. Some events described by participants include interviews on the radio and TV and participating in mental health debates and forums. In reviewing the literature, several authors confirm that social and political participation of people living with SMHPs can lead to a positive impact on their well-being and their quality of life (Abraham et al., 2010; Anderson et al., 2015; Clatworthy et al., 2013; McCorkle et al., 2008).
Furthermore, results highlight how for people living with SMHPs, it is crucial to have a workspace that is flexible and knowledgeable of mental health problems. These findings align with others which suggest that access to a job is not solely sufficient, but that people living with SMHPs adapt and engage better with jobs that offer support and actively work towards de-stigmatising mental health problems (Drake et al., 2009; Román, 2019). The CBMH device’s model provides opportunities to break the stigma surrounding mental health problems as part of their daily work, for example, when offering guided tours of the project for the community (Montenegro et al., 2021). The aforementioned findings offer relevant insights for the design of programmes and policies aimed at the inclusion of people living with SMHPs in the labour market. It emphasises the importance of flexibility and active work in the de-stigmatisation of mental health, as key aspects to promote recovery from the workplace.
The study also suggests that this CBMH device allows for opportunities for social interactions and peer support. Participants described that these experiences increase their sense of belonging and connectedness by encouraging them to share their life stories and to support others in their mental health treatment and recovery process. Previous research has suggested that social interactions enhance connections and decrease loneliness in people living with SMHPs, therefore promoting their recovery (Abraham et al., 2010; Clatworthy et al., 2013; Drake & Whitley, 2014; Haslam et al., 2022; Warner, 2009). This evidence is particularly important as many people living with SMHPs are excluded and alienated from social atmospheres, hindering their recovery process. Therefore, it appears to be crucial to continue expanding and strengthening community mental health services, which allows individuals to maintain their connections to their community and emotional bonds while also fostering a strong sense of community.
Our results highlight an important yet complex theme that requires further discussion in the literature – specifically, the support required by people living with SMHPs to make informed decisions regarding their medication. Our study demonstrated the critical role of the CBMH initiative in supporting partners throughout their psychiatric treatment, serving as a space where partners actively participate in learning about their medication, including usage, side effects, and dosages. The CBMH programme promotes and supports people living with SMHPs in the process of discussing these matters with psychiatrists and mental healthcare professionals, encouraging active involvement in their treatment. This aligns with the principles of the community-based mental health model, promoting and respecting autonomy and individual capacities to take control over decisions (Minoletti et al., 2012; Montenegro et al., 2021; PAHO, 2013). This model further recommends increased involvement of psychiatry within the community, and while it advocates to move away from overmedicalisation, simultaneously, it recognises the significance of ensuring proper access to medication and psychiatric services (PAHO, 2013).
Finally, participants expressed a consensus on the fundamental role of mental health services and public policy in promoting recovery from mental health problems. For example, they referred to the lack of spaces such as this CBMH device, which is specifically oriented towards labour inclusion, as well as the lack of uninterrupted comprehensive healthcare services. These gaps are generally associated with the care burden placed on families, which was also found in this study. This resonates with the most recent literature and emphasises the importance of increasing community mental healthcare services as they promote autonomy, employment, independent living, interpersonal relationships, personal agency, and symptom management (Drake & Whitley, 2014; WHO, 2021).
Policy Implications and Practical Applications
The findings of this study have practical and policy implications. First, the study highlights the imperative role of community-based mental health services in the recovery of individuals with mental health problems, which calls for the development of public policy to strengthen and expand such services. Further, the study emphasises the importance of work as a key element for recovery and effective inclusion in society extending beyond sole treatment. Creating educational and professional opportunities for people living with SMHPs should be prioritised, as there is a clear link between access to employment, recovery, and well-being. Finally, it is crucial to gain a comprehensive understanding of how individuals with mental health problems interpret and experience recovery. This knowledge can help shape policies that promote their mental health and well-being based on their lived experiences.
Strengths and Limitations
The study’s participatory approach engages individuals with SMHPs as active collaborators, enhancing insights into the urban garden projects’ impact on recovery. This framework amplifies marginalised voices, ensuring their perspectives are integrated. The study involved those with mental health experiences, families, and practitioners for a nuanced examination of the urban garden projects’ impact. In addition, this research uniquely illuminates Ecuador’s sole community-based initiative fostering autonomy through financial independence.
On the other hand, the study’s sample size, limited to 12 participants, may restrict its generalisability to a broader population. Further, the generalisability of findings may also be limited, as the study’s focus is on an urban garden project, constraining its relevance in other contexts, such as rural or suburban areas, or different types of work-based interventions. Lastly, the absence of comparable models similar to Huertomanías might be a constraint for determining its impact.
Conclusions
Huertomanías, the only person-centred, community-based mental health device in Ecuador, aims to provide a workspace for people with SMHPs that had been discriminated against in the labour market. This study aimed to evaluate the impact of Huertomanías on the recovery process of its partners living with SMHPs. The results show that the programme has had a positive impact on their recovery, providing a safe space for people living with SMHPs to exercise their rights by promoting their autonomy through work, income generation, access to information, and participation in decision-making, and strengthening their social network and peer support. While the CBMH device has limitations in terms of providing full financial independence, it offers valuable social recognition and access to paid work, which was consistently reported by most participants. The findings of this study not only contribute to the internal strengthening of the Huertomanías programme but also provide learnings for others intending to develop similar projects in Ecuador or Latin America more broadly.
Supplemental Material
Supplemental Material - A Participatory Evaluation of an Urban Garden Project in Ecuador: Exploring Factors That Impact the Recovery of People With Severe Mental Health Problems
Supplemental Material for A Participatory Evaluation of an Urban Garden Project in Ecuador: Exploring Factors That Impact the Recovery of People With Severe Mental Health Problems by Emilia C. Zamora-Moncayo, Bernarda Herrera, June Larrieta, Aimée DuBois, and Georgina Miguel Esponda in Qualitative Health Research
Footnotes
Acknowledgments
First, we would like to extend our appreciation to Ember Mental Health and its members for their guidance and unwavering support throughout the study. Second, we wish to express our infinite gratitude to Huertomanías’ partners, family members, mental health professionals, volunteers, and director for sharing their stories, knowledge, and time with us and working hand in hand with the research team on this project. Your invaluable insights were the foundation of our findings. A special commendation to our research assistants: our gratitude to Anita Mejia, for her meticulous work on transcripts and quote translation/verification. We would also like to thank Ana Paula Maldonado, Evelyn Cobos, and Maria Emilia Cofré for their dedicated efforts while transcribing our audio data. This paper is a result of a collective effort. Your contributions will undoubtedly leave a lasting impact on the quality and depth of our research.
Author Contribution
GM-E, JL, and EZ-M were responsible for conceptualisation, methodology, and the ethics committee application. EZ-M and BH were responsible for data curation, formal analysis, writing of the original draft, review, and editing. GM-E and JL were also involved in supervision, validation, writing review, and editing. AD was responsible for validation, writing review, and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (August 2024):
Credits for Images 1-3 have been added to the article since its original publication.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.