
Abstract
Therapeutic communities (TCs) have been a longstanding intervention for individuals with complex mental health needs; however, there remains a lack of research into how UK-based TCs work to support their members. Modifications to TCs include the merging of “concept” and “democratic” TC practices, producing a “fusion” model. The aim of this study was to explore processes of change that occur within a community-based, non-residential “fusion” TC across two community sites. This was done through exploring lived experiences of active members and graduates of an established and a newer TC site. Eleven participants took part in online or face-to-face interviews. Interviews were analyzed using interpretative phenomenological analysis. Three themes emerged from the analysis: (1) Exploring the Authentic Self: Encouraged and Supported in Showing Emotional Vulnerability Within the TC (subthemes: “Nowhere to Hide”: Sharing With Others and Looking Back to Move Forward: Reflecting On Change and Self-Discovery); (2) Developing a Sense of Community: Learning to Navigate Relationships Within the TC (subthemes: “They seem to fit”: Building Connection With Others and Unravelling the Clashes: Holding Space to Manage and Tolerate Conflict); and (3) “Me to We”: The Lasting Benefits of the TC Co-Production Experience. Staff were integral in supporting change identified across all three themes. The findings highlight processes that could be implemented into existing TCs to support change for members and evolve the community structure. The study provides insights into how TC practice could be informed to accommodate the growing diversity of TC members and support staff development.
Introduction
Therapeutic Communities
Therapeutic communities (TCs) are psychiatric interventions, designed to treat people through a structured, peer-supported culture and environment (Kennard, 2004). There are two main types of TCs described within the literature, which are modified accordingly to suit different needs of populations (de Leon & Unterrainer, 2020; Magor-Blatch et al., 2014; Malivert et al., 2012). British Democratic TCs (DTCs) traditionally accommodate those with complex mental health difficulties. They uniquely emphasize equality and adopt a “flattened hierarchy” within community meetings (Akerman & Mandikate, 2018; Campling, 2001). American concept TCs support individuals with addiction and substance misuse. They differ from DTCs, using a phased model for members to progress through treatment. They encompass a hierarchical system of members and enforce more stringent conditions, like “pull-ups,” to challenge members who break TC rules (Campling, 2001; Perfas, 2014).
TCs are traditionally residential; however, the late 50s signified a step toward community-based care, through the introduction of non-residential TCs (Siroka, 1974). UK TCs have gradually adapted to fit with the current economic and social climate, resulting in the closure of all traditional, residential DTCs commissioned by the National Health Service (Gallagher, 2017; Haigh, 2019). Non-residential TCs like day TCs operate over 3–5 days, mini-TCs provide less than 2 days of support, and micro-TCs provide half a day (Haigh, 2007; Lees et al., 2017; Pearce and Haigh, 2008). Day TCs were shown to be as effective as residential setups in reducing harm and improving social functioning in individuals diagnosed with personality presentations (Barr et al., 2010; Dye et al., 2009; Malivert et al., 2012). While this can be resource-efficient and promising, there remains concern that non-residential TCs are not intensive enough to support severely unwell individuals who cannot be contained safely within the community (Haigh, 2007). This highlights a need for research to determine how therapeutic interventions work and whether they can be adapted (Adair-Stantiall & Needs, 2018).
“Fusion” TCs
While DTCs and concept TCs have longstanding theoretical differentiations, the two types of TCs share commonalities. At the heart of TC practice, both DTCs and concept TCs encompass “Community as Method,” highlighting the power of the community as key to promoting recovery. The community becomes a trusted, respected place to all members, and everyone is responsible for its maintenance (de Leon, 2000; de Leon & Unterrainer, 2020). Some communities have encapsulated both democratic and concept elements, creating a “fusion” TC model (Haigh & Lees, 2008; Young, 2010). According to Haigh and Lees (2008), the shared concepts of “fusion” TC captures are embedded within the setup of the TC (e.g., the culture, structure, and activities), agreed expectations within the group (e.g., decisions, behaviors, and responsibilities), and members’ responses/reactions to their peers (e.g., feedback and pull-ups). European and American TCs have exemplified a “fusion” TC model in treating addictions and comorbid difficulties and a move from traditional diagnostic criteria of TCs. Coined as a “third generation TC,” the model appeared more culturally fitting for members, through the adoption of the DTC’s closely connected community supported by professionals. Fostering relational engagement with peers and family, alongside a structured, phased model of the concept-based TC, was effective in promoting recovery for this population (Broekaert et al., 2005; Goethals et al., 2011).
Mechanisms of Change in TCs
While there are regulatory standards for accredited TCs (Paget, 2008), TCs can create what fits for the community needs. TCs are theoretically grounded in various branches of social psychology, systems theory, and psychodynamic theory (Campling, 2001; de Leon & Unterrainer, 2020; Harrison, 2023; Magor-Blatch et al., 2014; Malivert et al., 2012). While theoretically robust, Shuker (2010) argues the concepts remain largely “ideological,” lacking evidence-based research in TCs to support them. However, there is a growing evidence base on the effectiveness of TCs; these include empirical studies (Barr et al., 2010; Debaere et al., 2016; Dye et al., 2009; Morris, 2014; Sacks et al., 2008), case studies (Howe et al., 2022; Spandler, 2009), and systematic reviews (Capone et al., 2016; Magor-Blatch et al., 2014; Lees et al., 2004). Taken together, these broadly suggest that relationships between members and the unique environments and practices within a TC are pivotal toward achieving sustainable, cost-effective treatment.
Pearce and Pickard (2013) theorized two modifiable change processes in TCs that are thought to manifest successful integration and recovery of individuals: belongingness and responsible agency. Belongingness is fostered through the development of relationships within a safe community environment (Janeiro et al., 2018). For many individuals who enter TC treatment, this can often be a lifeline to the creation of healthy future relationships with others, given they may have grown up in insecure environments where relational connections were inconsistent or hostile (Haigh, 2013). The opportunity to connect with other members has been shown to promote confidence and increase feelings of being seen and heard within communities (Clarke et al., 2016).
The second mechanism of responsible agency requires the motivation of members to develop self-awareness and modify behaviors (Davidson & Young, 2019). Members within a European residential “fusion” addiction TC developed self-awareness and initiative by partaking in a structured program, providing routine through task-focused work, opportunities to encounter healing relationships, and engagement in future planning (Janeiro et al., 2018). Developing agency enhanced questioning utilization of maladaptive behaviors like self-harm and freedom to choose how to respond to situations or triggers (Hodge et al., 2010; Miller et al., 2006). Pearce and Pickard (2013) identified the need for more empirical research with TC users to evaluate how the theoretically driven processes of change translate practically into TC models.
Context of Intervention
This study is set in a two-year NHS-based non-residential, community “fusion” TC located in the United Kingdom. This TC recently established a second TC branch within the locality. Both sites are supported by staff and peer mentors and accept members diagnosed with non-psychotic presentations, including difficulties with emotional intensity. The program comprises two and a half hour weekly community meetings. Outside of the meetings, members can call the dedicated phone line between working hours, should they need support and signposting to other services.
The treatment is structured across four phases, much like concept TCs, combined with the democratic TC’s “flattened hierarchy” ethos, illustrative of the “fusion” TC model (Haigh & Lees, 2008). Phase 1 enables members to settle into the TC. Phase 2 encourages members to participate in activities (e.g., attend workshops and contribute to group discussions). Phase 3 enables members to explore responsibility within the TC (e.g., group-chair and secretary) and local community activities. Phase 4 expects members to share skills (e.g., facilitating workshops) and prepare for treatment completion. Each phase lasts six months, and a reflective space marks the ending of each phase. The communities adhere to an agreed agenda, share lunch, and discuss both internal and external community events, alongside therapeutic check-ins, feedback, and check-outs. The communities have an agreed set of safety boundaries which all are expected to abide by. Should these be broken, the incident would be brought up in community meetings and if needed, a supportive space with staff and peer mentors would be facilitated outside of community time. Supportive spaces are also held if individuals are struggling with engagement.
Research Aims
Our study explored the experiences of members and graduates of a community-based fusion TC, split across two sites. To our knowledge, this is the first study to explore the processes of change in this setting. Our study aimed to (i) understand people’s experiences and perceived impact of the TC and (ii) explore potential processes of change experienced by participants through these experiences. We used interpretative phenomenological analysis (IPA) to gain a detailed, richer view of the lived experience of participating in the TC (Denis et al., 2022; Thirsk & Clark, 2017).
Method
Ethical Approval
The study was approved by the University of Southampton Ethics Committee (ERGO II 79605) and the London Camberwell St Giles NHS Research Ethics Committee (REC Reference Number: 23/LO/0603). The study was pre-registered on the Open Science Framework (Li, 2021). While the study was registered, the authors allowed for the occurrence of development in study materials, including interview schedules.
Participants
Twelve participants initially volunteered to take part in the study, one of whom dropped out due to personal circumstances. Participants were aged between 24 and 66 years (M = 41). Eight participants identified as female, two as males, and one as non-binary. Nine participants were White British, one participant was Asian, and one participant was White-Other.
Of the 11 participants, six were current active TC members and five were graduates. Five active members were part of the newer TC site. One active member and the graduates were part of the established TC site. Four of the graduates were peer mentors of the TC or paid members within the NHS.
Although Smith et al. (2021) reported that there was “no right number” of participants for an IPA study, the researcher and supervisory team together reflected that a maximum of 12 participants would be enough, relative to the participant population’s estimated level of insight and awareness (Levitt et al., 2017).
Procedure
The primary researcher (CF) sent an “Information Sheet for Clinicians” to the “fusion” TC for staff, detailing a summary of the study and the eligibility criteria, a recruitment advert, participant information sheets, and opt-in research forms. The advert was circulated through key clinicians to eligible members and graduates. Eligible participants were active members who attended for a minimum of a year and completed a minimum of two “phases” of the TC program or graduates who completed the program.
Participant information sheets and an opt-in research form were provided to eligible members by clinicians. Interested participants signed the opt-in form, giving permission to be contacted by the researcher (CF). Following receipt of opt-in forms, participants were contacted by the researcher (CF) to answer any questions and arrange a face-to-face, telephone, or online interview. Six participants opted to take part via an online interview and five opted for a face-to-face interview.
On the day of their interview, participants were asked to read and sign a consent form. They were reminded of their right to withdraw following opt-in, during the interview, and within two weeks from their interview date. For participants who opted for face-to-face interviews, a written consent form was provided to read and sign. For participants who chose online interviews, a Microsoft Teams consent form link was sent to them while on the call; participants filled this out and submitted it. The researcher (CF) checked all consent forms were filled out and signed correctly before continuing. All participants completed a demographics form and expressed verbal consent to take part and record their interviews. Interviews were undertaken by the researcher (CF) in a private, confidential room. Interviews lasted for approximately 30–75 minutes and were recorded via MS Teams. Participants were reminded to answer questions in as much or as little detail as they wished and offered breaks. Semi-structured interview schedules (one for members and one for graduates) were used to guide interviews. The active members’ schedule was written in the present tense and the graduate members’ schedule was written in the past tense. This reflected their relationship to the process, either current or past. These were created by the primary researcher (CF) and discussed with the research team to ensure questions were neutral. A voluntary former TC member provided feedback on this and all other study documents, which was considered and incorporated. This volunteer was reimbursed for their time with shopping vouchers. The schedules consisted of seven main open-ended questions, including exploration into • Structural elements of the TC and a “typical day” • Experiences of being with others • Helpful and challenging TC experiences • Any changes seen in areas of participants’ lives
Participants were verbally debriefed after interviews, offered a chance to ask questions, and given a written debrief. They were given a £25 shopping voucher upon completion. All participants were given a Participant ID Number and pseudonym. Data were stored securely in the University of Southampton file store, which was encrypted and only accessible to the research team. Video recordings were deleted once interviews were transcribed by the primary author.
Analysis
Interpretative phenomenological analysis was used to analyze interviews following guidelines by Smith et al. (2021). Each transcript was re-read and the recording was re-listened to several times prior to undertaking exploratory noting to ensure immersion. Noting was completed manually by the primary author using three levels: first, descriptively to summarize participants’ experiences; then linguistically, paying attention to the language and verbal/non-verbal cues; and finally conceptually, where a more interpretative stance was taken to reflect their experience. The primary researcher’s (CF) critical realist stance aligned with IPA, as thoughts, emotions, and behaviors were acknowledged to be shaped within the participants’ environment, interactions, and life experiences. Furthermore, IPA allows for the “double hermeneutic,” whereby the researcher is invited to interpret the participant’s subjective understanding of their experience (Tuffour, 2017). This creates another layer of knowledge which is contextualized by the researcher’s experiences.
Experiential statements were created from the exploratory noting, which were subsequently grouped to form personal experiential themes. This process was repeated for each transcript; each transcript was fully analyzed prior to moving on to the next to preserve the unique narrative of participants accordingly. The primary researcher (CF) reviewed versions of personal experiential themes and exploratory notes with the research team (NB, TM, and KS). This helped to engage with the data on a deeper, theoretical level and get feedback to ensure interpretations aligned with the data and meaningfully answered the research questions (Yardley, 2000). Notes of supervision meetings were taken by the researcher and considered in the reorganization and renaming of themes (Johnson & Haigh, 2011; Smith & Nizza, 2022).
A cross-case analysis was then undertaken to determine group experiential themes. The researcher looked for convergence and divergence across personal experiential themes and organized these electronically using tables in Microsoft Word, remaining iterative and open to the formation of new interpretations. These tables were shared across the research team, whose discussions shaped and updated the analysis, to ensure the themes fit with the aim of exploring TC change processes.
Reflexivity
The primary researcher (CF) and one research supervisor (NB) had experience of working in the studied fusion TC. To reflect on this influence, the researcher (CF) kept a reflexive journal, logging their reflections through the process of designing the study, interviewing, and analysis. Reflections were brought to research supervisions accordingly to discuss and support the primary researcher (CF) in the data collection process (Rager, 2005).
Findings
The analysis identified three group experiential themes: (1) Exploring the Authentic Self: Encouraged and Supported in Showing Emotional Vulnerability Within the TC, allowing members to explore exercising their vulnerability and practicing self-reflection in the community; (2) Developing a Sense of Community: Learning to Navigate Relationships Within the TC, which focused on exploring interpersonal connections; and (3) “Me to We”: The Lasting Benefits of the TC Co-Production Experience, allowing for collective participation and furthering opportunities for development. Figure 1 illustrates the themes and connections. Thematic Map of Processes of Change in Fusion TCs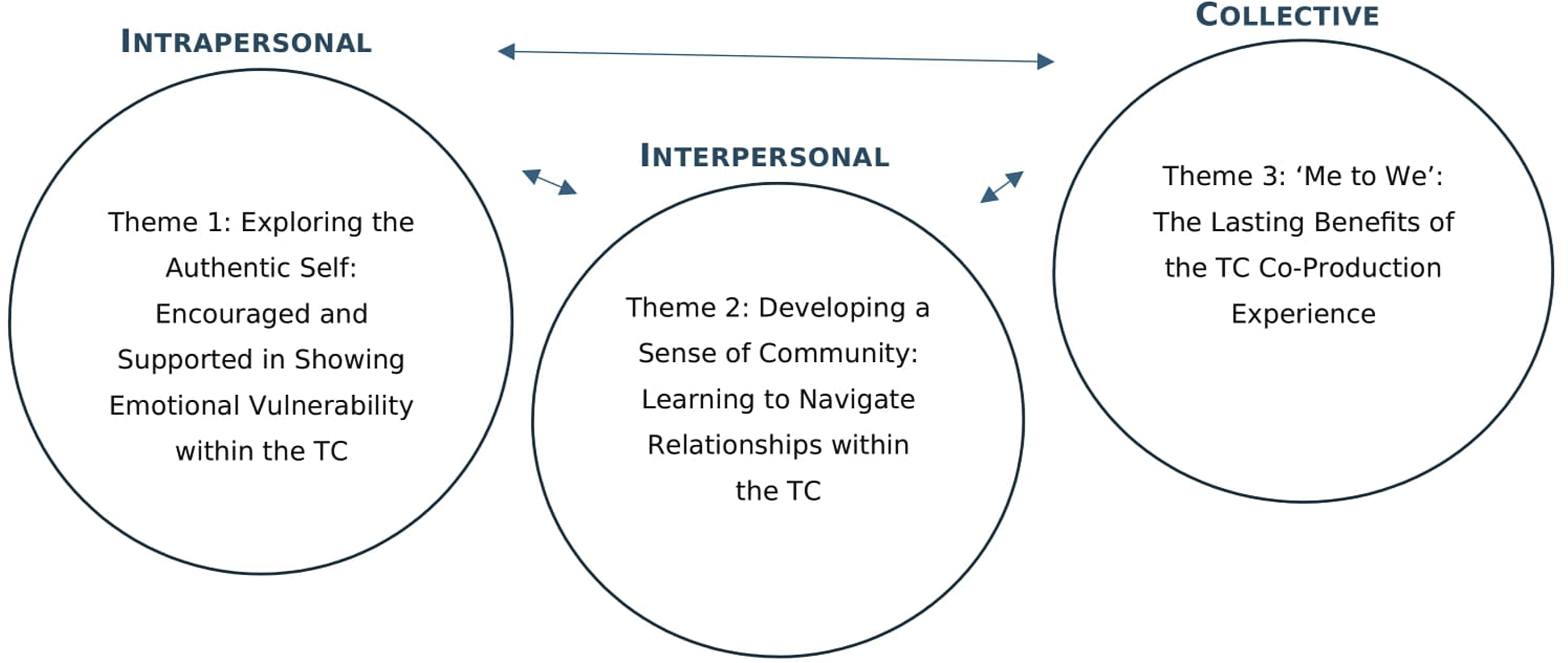
Theme 1: Exploring the Authentic Self: Encouraged and Supported in Showing Emotional Vulnerability Within the TC
The first group experiential theme relates to participants’ experiences of exposing stories, thoughts, and feelings. For most participants, the TC was a safe space to openly explore life events. The two subthemes portray how most members became confident in expressing complex thoughts and emotions. This created opportunities to reflect on and learn from their experiences.
Subtheme 1: “Nowhere to Hide”: Sharing With Others
All participants described having to be vulnerable in sharing experiences during community meetings, which evoked honest emotions, creating authenticity. For some participants, sharing did not come naturally. Daisy described “wearing multiple hats and saying they’re fine when they’re not.” Daisy appeared to be externalizing her experience having changed to third person, potentially distancing herself away from the uncomfortableness of bringing her authentic self. Tom wore “a mask” to try and present themselves in a way that aligned with how they felt they should, which appeared symbolic of their insecurity. However, when considered from the lens of the author who has worked previously in TCs, masking was quickly recognized to not be conducive to therapy and was inescapable, leaving them to confront their true self within the group setting: There’s really nowhere to hide … you have to be um, comfortable with that level of showing up. (Tom)
Similarly, Jess grew aware of her fears of being in group spaces, but the group gave her the freedom to explain: I made that clear … I think it helped … It’s not that I’m being rude. It’s not that I’m not paying attention. It’s just that I struggle with [eye contact].
Some participants struggled to articulate their words and adjusted their approach by writing things down or initially used smoke breaks outside of therapy to open up. When considered from the lens of a clinical psychologist with experiences of working in group therapy settings, these may have also served as a focus to detract from the anxiety of the spotlight when they were due to speak. Jordan found writing in the “green book” helpful; this was a TC mechanism used to capture and highlight thoughts of members: Whenever I’m extremely stressed, I write it in the green book and then people read it out … I feel like I can write better then I can speak. (Jordan)
Participants appeared to value time to think deeper into their thoughts and emotions of their experience and conscientiously convey them and feel heard.
Contrastingly, although initially feeling nervous upon starting at the TC, Flo reflected positively on the process of sharing her check-ins with the group. The researchers discussed how the use of imagery in describing the experience may demonstrate that she found it an emotionally relieving experience and an achievement: I find it very cathartic … Being able to share those things. Umm. And I thought of it just being like a burden lifted off your shoulders … you’ve managed to share them.
As participants became used to the structure, most appreciated the opportunity to share, feel listened to, and validated in their experiences. The TC appeared to allow members to shape their personal life narrative in ways that made sense to themselves and others. The recognition that others had gone through similar things facilitated a platform for members to “step into another person’s shoes” (Linus) and learn valuable things from each other.
Receiving feedback from others in the group was an integral part of being vulnerable with others as it indicated people understood one another’s difficulties. Two participants had received serious health diagnoses and chose to share these with the group. Both commented on how much “love” (Julie) and feedback (“they were just there for me” (Lauren)) they helpfully received.
Being vulnerable with others enabled some participants to feel more comfortable in showing their emotions and process difficult situations, without fearing how they would look to others. This demonstration of raw emotion is a core and rare aspect of vulnerability for Daisy. Feeling held by the group when expressing her true feelings was a key toward learning healthy emotional regulation: I’ve always had an issue with [crying] in front of people … at the time I felt awful … I thought, Oh my God, I’m a baby … but it made me feel so much better. (Daisy)
Several participants commented on how their families struggled to understand them which was why TC peer support was invaluable. However, Abigail commented on how the “Family and Friends” group held by the TC was useful in helping her close friends understand her: My friends who are my my strongest support. They come to something like this. To see the other side of my life … It’s been really important for me, even going forward. (Abigail)
Abigail’s comment about the future suggests this meeting served to repair any ruptures that previously existed with friends through their acquired knowledge of how she experiences life and how best to support her.
Sharing with others was practically challenging for some participants. One described how others took up a lot of space in the group. Through the lens of a clinical psychologist, this could additionally translate into members oversharing and triggering others: I’m hoping things will get better, but it is (pause) making it seem as though the whole group is really there about her, which is not great. (Zoe)
Participants in the newer TC struggled with obtaining feedback from others and named possible barriers members have in giving feedback. Jess shared members “either … didn’t have the knowledge or they were just too anxious to speak.” Compared with experiences of feedback from Julie and Lauren who were in the established TC, this suggests the skill of feedback may gradually develop in members as the TC matures over time.
The differences in TC maturity could further explain how members perceived sharing experiences with older members. Jordan, who attends the established TC, recalled how age made no difference in his ability to share and receive support with difficulties: … Even though everyone else was, well, quite a bit older than me, uhhh, we still had similar problems … we could still support ourselves in similar manners. There’s no ageism there. (Jordan)
In contrast, Jess, who attends the newer TC, experienced an opposing experience, with age seen as a barrier in embracing her vulnerability with others: I probably feel a bit like a baby in terms of things that I might struggle with now … they might have done when they were my age, but they might be years past that by now … sometimes I feel that the age difference does make it hard to talk.
Jess’s expression that she felt like a “baby” suggests that she felt her struggles would not be taken seriously and construed as less important than others. Her early experiences discussed in her interview indicated that she grew up in an environment where she had to independently navigate struggles. Thus, this may have been an unfamiliar situation to share things, particularly if she felt they were trivial.
Abigail noted other barriers to expressing her emotions and true self. When considered from the lens of the primary author who is from an ethnic minority background, it appeared her ingrained cultural and social norms were strongly portrayed through metaphor: From my background I’m always told you know, don’t air your dirty laundry in public. So, I have that sort of in my head constantly … it’s really always a.. [pause] struggle.
Abigail appeared to have felt torn between knowing what will help her mental health and what would potentially trigger a sense of shame, thereby illustrating incongruency between western therapy norms and her cultural values.
Subtheme 2: Looking Back to Move Forward: Reflecting on Change and Self-Discovery
Alongside sharing experiences with the group, the TC enabled participants to partake in self-reflection. This was perceived as a vulnerable and sometimes painful process, or a breakthrough in their personal development within therapy. Some participants did not anticipate needing to do as part of their recovery. Julie initially experienced fear in exposing herself to memories, with the “main goal” being fixing her present: I could not see that, but somehow it’s like looking back … before I used to refuse, I don’t wanna look back. I want to focus on main goal. Never touch on the past again … but now I start looking back a little bit. (Julie)
Linus explored how the TC gave him a chance to exercise self-kindness and acceptance. He alluded to actively slowing down and reframing the automatic self-critical thought process he used when something difficult happened, prior to joining the TC. This appeared to facilitate the development of compassion for others. I think it’s given me time to err ... gives me the opportunities to self-reflect as well. And just to to be kind of. More self compassionate … hopefully that comes out when when you’re with people. (Linus)
The phased structure of the TC enabled participants to compartmentalize their journey through treatment, making it feel more manageable. We considered how Tom’s reflection of how the phases break up the journey demonstrated the meaningfulness of engaging in therapy rather than going through the motions of attending each week blindly. The reflection highlights pausing as crucial to the program, a mandatory process requiring dedication and focus: That ability to pause and reflect is really crucial to to the [TC programme] and and to why the phases work … you’re not just constantly on the go, you do have built in time to stop and breathe and and look back … I found that very helpful. (Tom)
The TC offered participants reflective spaces between phases of the group. These were facilitated by staff and peer mentors. Most participants recalled how these spaces were helpful to reflect on their progress and identify strengths and areas for development. They also valued staff and peer mentors in assisting them with this process, which helped develop their self-belief and confidence: I was assaulted about a year ago … about a month or six weeks later, I went in for my end of phase one reflective space. [They]noticed that I’d become stronger in myself … all of them agreed that if what had happened had been at the beginning, I probably would not have coped as well. (Zoe)
Tom recalled how they were able to use reflection to think about their own understanding about aspects of their identity, leading toward self-acceptance and freedom to express themselves. Group membership may have coincided with a pivotal period of transition for Tom which appeared helpful to question and work through their feelings with the group: One of the things that the group kind of really helped me start along the the path of was coming out as queer really … the ability to kind of um question the way that society does things is something I felt more confident from being part of the group.
Jordan found reflective spaces challenging as they required reflection on progress and future goals, which he appeared to find confronting. Participants’ life transitions may again have played a role in making it harder for some to envision plans than others, as Jordan was contemplating going back to university at the time: They ask me questions like what I see myself doing in six months time … reflective spaces for me is quite anx..stressful … It’s important—It’s like eating your vegetables. You might not like to do it … but you know you have to. (Jordan)
Theme 2: Developing a Sense of Community: Learning to Navigate Relationships Within the TC
The second group experiential theme relates to participants’ experiences of developing and managing relationships. The TC offered a platform to interact with others and build upon their socialization skills. Managing relationships involved both fun and difficult situations. While difficult situations were uncomfortable, they provided vital lessons in how to repair, with the support of their peers and staff. The TC encouraged belongingness within formal therapy and informal events held within the TC.
Subtheme 1: “They Seem to Fit”: Building Connection With Others
Feeling connected was reliant on participants committing to attending the group or letting the group know when they were not going to be there. Participants who attended consistently developed connections with others, which increased their ability to engage. This provided some familiarity and comfort knowing that they would be met by people they knew each week: The peer mentors will always be there um which is really nice … to walk in and see them setting up and sort of smile and wave … that was very um calming. (Tom)
Tom appreciated the positive friendly non-verbal gestures, which helped build connection without pressure to say anything. This was important to acknowledge, as the gestures of waving and smiling are indicators of a friendly and welcoming environment within the United Kingdom. Understanding other forms of non-verbal communication specific to individuals’ culture may help them feel welcomed too.
Participants described the benefits of attending the TC to experience a sense of belongingness, thereby reducing isolation and loneliness and develop “healthy relationships” (Flo). Both these opportunities may have been limited to members prior to joining; thus, the opportunity to join may have been precious: … you’re one of many … maybe some people felt they’ve been on their own for years and years dealing with this, and then they come into a group like this where they just seem to fit. (Daisy)
Participants enjoyed opportunities to connect with others over “normalized” parts of the TC, for example, informal conversations, that did not encompass talking about difficulties, group lunches, and other celebrations: I’ve loved our annual Christmas party where we got to meet a lot of uh, old faces … it was like a party that I actually wanted to be in. Most times, when I go to a party, it’s just me in a corner. (Jordan)
Jess alluded to the idea of needing time to “ground” or adjust into coming to the TC each week. By reconnecting with members each week after a break, this may highlight the need to prepare herself for what might be brought into therapy, through “random conversations,” revealing participants’ emotional states and thoughts. This would not be the case in residential TC settings, where members are with each other 24/7 and would ordinarily know about each other’s activities.
Participants spoke about the group sending them cards when they were unwell, which signified others cared and thought about them, when they were not physically present. These all contributed to the increased sense of inclusivity, as four participants’ likened membership to being in a “family” (Lauren, Jordan, Lucy, Julie), “finding a space within the group dynamic” (Tom), and “[feeling] loved and warm” (Julie).
Group connection gave participants a chance to look beyond mental health difficulties and see others in a different way, which was an important change for Linus in particular, who had spent prolonged periods in a psychiatric hospital prior to joining. He was able to reflect on how being treated as the person he is rather than a diagnosis was a crucial component of his recovery. This formed into part of his own approach when meeting other members and allowed for a more personalized sense of connection: It was something that kind of er I looked forward to … seeing the person’s value rather than seeing their their illness. (Linus)
While consistency was highlighted to help participants feel safe in developing relationships, Jess and Zoe, both members of the newer TC, described how their felt sense of safety often fluctuated due to the chaotic nature of people entering and leaving without warning.
Abigail experienced the planned leaving of staff which was very difficult; however, the importance of a healthy ending was emphasized and taught within the group environment: I was quite upset when [staff member] left … she enforced the importance of saying goodbye.
The staff member reminded her of a friend who had recently died. Abigail’s use of the word “enforced” was very formal and emphasized how difficult and unpleasant Abigail found endings.
Two participants felt worried about losing the group relationships, following the end of their TC journey, further suggesting how important connection was to them: I’m scared of what the future’s going to be like once I finish … and missing the connections … (Lucy)
Subtheme 2: Unravelling the Clashes: Holding Space to Manage and Tolerate Conflict
Learning to hold and manage conflict together appeared integral for participants to develop healthier relational skills within the group environment. Some participants talked about their experiences of conflict, which initially appeared to compromise group connection. Experiences ranged from being directly part of the conflict to observing the conflict taking place. Jordan used a powerful metaphor to describe the anguish caused: She would pick arguments … at one point I thought I might actually have to defend myself against her like physically … feels like I’m a lion tamer with an angry lioness. (Jordan)
Jordan’s use of metaphor appeared to symbolize a role in mitigating the situation himself, given how targeted he felt. However, participants reflected on how conflict was also spoken about. All members were able to contribute their views and opinions, with view to resolve the issue. This is demonstrative of the power peers hold in holding and managing situations.
Participants reflected on the usefulness of experiencing inevitable conflict in the TC setting in giving them a template in how to manage it: Being in a room of people whose personalities are constantly clashing has also actually helped … because that happens on the outside … it’s happening in a slightly safer, more comfortable space. (Jess)
However, six participants expressed that staff were relied upon to ensure the overarching safety within the group: [staff] don’t take over. I mean initially the group was trying to be sort of run by clients I suppose, but you still got to have somebody there as I said, just to make sure things don’t take off in a—in the wrong direction. (Daisy).
There was a contradiction in Daisy’s statement in the fact that staff did not resolve situations but were still expected to step in and help. This serves to dilute the responsibility between staff, peer mentors, and members. This would not be the case in a traditional residential TC as staff would not be expected to get involved at all.
Julie mentioned how a staff member helpfully acknowledged and managed her emotional intensity when they saw her getting irate: She insulted [staff member]. And really I was sitting with [staff member] next to me. I’m gonna go to start on this … I started heating up myself and [staff member] saw it coming and told me to slow down “cause he knew.”
This illustrates the strong familial therapeutic relationship and how members can develop empathy and compassion toward others who theoretically and perceivably “hold power,” which perhaps was confusing.
Staff helped participants to deal with conflict by facilitating a special learning space, which helped with healthy reconciliation and reconnection with peers: I explained to [the other member] how she’d made me feel and everything she said, “oh I didn’t realize how I made you feel … now I understand that you didn’t do it.” Then I got an apology. (Lauren)
Theme 3: “Me to We”: The Lasting Benefits of the TC Co-Production Experience
Co-production gave participants chances to work together with both staff and peers, allowing them to gain a sense of purpose and agency. Participants described their understanding of what co-production was, including stepping into more empowered positions requiring effective planning and decision-making for opportunities to connect with others, linking to our second theme: … you brainstorm ideas … with the help of everyone … [for our] Halloween party … people are going to bring various food items and we are going to decorate the place. (Jordan)
The participants who were TCs’ founding members elaborated on their positive experiences of “first-hand” co-production. Together, they evolved and structured the TC from the ground up, thoughtfully integrating TC principles. They appeared to embrace the sense of ownership, dedication, and responsibility in such roles. … I was very proud of at the time … [we] decided between us which was the right right way to go. It was … sort of like you had to. Try things out to see if they work. (Lauren)
As seen in traditional democratic TCs, the equality of decision-making was further acknowledged through co-creating and adapting boundaries for the group. This appeared especially important to Daisy in ensuring nobody felt left out or blind-sided: … it’s not just changed by the staff and they think, “Oh yeah, we need to put that in, so we’re going to,” no … the group discuss it as a whole. (Daisy)
Co-production also gave opportunities to create workshops and groups which were external to the TC meetings. These were described as voluntary “spokes of the TC experience” (Tom) bringing a sense of achievement for those who created them. The innovative designing of such workshops allowed others to express themselves in different ways, connecting back to the first theme of exploring the authentic self: I actually did a workshop called “All About Me” … So we could find out different things about each other. That wasn’t necessarily mental health related or difficulty related … (Jess)
Tom co-producing a young person’s group with staff was integral toward developing a sense of purpose, self-belief, and important professional teamworking skills. … we cocreated this this space … I felt almost a sense of of ownership, maybe or a sense of “hey I am capable of doing a nice thing”—that was very meaningful to me.
Other pieces of work Tom led included the development of a co-produced TC newsletter, which captured the interest of healthcare professionals and resulted in securing paid employment.
Co-production assisted participants to freely showcase their individual talents, express their creativity, and connect with their passions. Zoe expressed how the group valued her contributions toward a new logo for the TC: I am a photography student, so I kept looking at the (TC logo) and there was one bit on there that just really annoyed me … I just said look, can I redo the picture … (Zoe)
Three participants reflected on the external opportunities co-production brought, including attending and presenting together at public events and conferences, which provided new possibilities and experiences. These opportunities appeared unintimidating for Linus, who took comfort in having his peers alongside to help him focus and disseminate information about his TC confidently: … we had a meeting from all the different communities from across the UK … I didn’t actually present by myself … [everyone] had their own parts. (Linus)
Abigail reflected on a challenging experience of co-production running a creative writing workshop which her peers had not prepared for. This left her feeling disappointed, disempowered, and self-critical, taken back to a place of insecurity, through recollection of her past. She required acknowledgement from staff to move forward from the difficult situation: It was … horrible … [it] reminded me of the stress of being a teacher … I went home … sent a message a little bit later, saying how I felt … [staff] replied and apologized for not seeing it and seeing that anxiety. (Abigail)
Discussion
Our study used IPA to qualitatively understand experiences, perceived impacts, and change processes within a community-based “fusion” TC through interviewing 11 active members, graduates, and peer mentors across the two sites. Experiences were thus seen through the multiple lenses of participants at different stages of their journey. IPA enabled insight into convergent and divergent experiences of members, giving a richer understanding into people’s individual experiences (Smith et al., 2021).
The results of the study revealed three main themes depicting the processes of change through experiences of TC participants. The order of the themes highlights the TC’s ability to guide members through the intrapersonal, interpersonal, and collective community-level processes, making for a rounded recovery journey. Exercising vulnerability within community meetings and self-reflection via individual reflective spaces helped members notice and learn from past experiences and motivate them toward making personal changes in their lives. However, some members struggled to open up and communicate with the group, hindering their progress. Learning to navigate relationships helped build integral connections with peers and staff, both through positive, inclusive experiences and challenging “conflict” experiences. Participation in co-production opportunities both within the TC, that benefited the group (e.g., adapting the TC structure, activities, decision-making processes, and TC safety boundaries), and external to the TC (e.g., public events) served to promote empowerment, purpose, and confidence. This active power-sharing partnership across the community mirrors how co-production is utilized in healthcare, with service users and staff working to co-create high-quality and robust services moving forward (Ostrom, 1999).
On an intrapersonal level, the gradual process of exposing oneself to vulnerability through sharing stories and relating to others’ situations in community meetings appeared useful to members. This provided opportunities to openly explore emotions, learn coping strategies, and communicate via group feedback. This may have furthered the building of connections and inclusivity within the groups. This aligns with findings by Hodge et al. (2010), who showed that sharing difficulties enabled relationships to develop through acknowledgement of other’s suffering. Further, relating to one another’s difficulties and learning that things could get better provided them with optimism; this has been shown to be crucial in improving individuals’ mental and physical well-being (Conversano et al., 2010; Loat, 2004). However, some members experienced difficulties in sharing, with cultural barriers (e.g., hesitancy in sharing personal stories outside of family) and age differences reducing the central TC principle of permissiveness of freely expressing themselves without negative consequences (Lauzière et al., 2022; Rapoport, 1960). Scott (2011) exemplifies how “unconscious shame” creates disconnection and difficulties in group communication, which may explain these findings. However, other studies have found that similar cultural barriers, pertaining to a member’s race, religion, family values, etc., were experienced in prison-based TCs, which left members shut down, as they were perceived to be unaccepted by others (Brookes et al., 2012; Jones et al., 2013). This suggests a need for TCs to consider ways of employing culturally informed support to help such members.
Vulnerability through self-reflection within the group via feedback and reflective spaces invited members to pause and look inward to understand their journey, and this appeared captured between phases of the “fusion” TC model. Thus, the concept of reality testing whereby members were regularly confronted with aspects of themselves was achieved within the TC (Rapoport, 1960). Reflection requires agency; thus, individuals have to consciously choose to undergo this process and remain accountable to what they find (Pearce & Pickard, 2013; Shuker, 2018). However, self-reflection appeared to extend to encompass vulnerability, as members expressed avoidance of their past and a disconnection with themselves that needed to be explored to move forward. The findings connected to prison-based DTC research, whereby residents used small groups to reflect on difficult experiences of criminal activity which helped them see the perspectives of victims and their families affected by their crimes (Dolan, 2017). While group reflection is beneficial, our findings show members appreciated and thrived with privacy in planning and reflecting separately from community meetings, suggesting the importance of these spaces in contemplating future change and personal development. Incorporation of such spaces in new and existing TCs could therefore be helpful.
Moving interpersonally, connection among peers appeared to be an important change mechanism, in both positive interactions and navigating challenges (e.g., conflict). Members appeared able to build up a secure network of peers, to develop skills in socialization and conflict resolution. This served to create healthier ways to navigate interpersonal situations, through freely communicating with others verbally and non-verbally, encompassing the principle of communalism (Phutela, 2015; Rapoport, 1960). This theme appears to align with Haigh’s (2013) quintessence TC theory in highlighting the importance of “secondary emotional development” in creating opportunities for members to experience developing secure attachment (via peers and staff) and experience healthy disputes safely. Haigh (2013) recognizes these opportunities may not have been available to TC members in early childhood, growing up in dysfunctional circumstances. Members obtained an identity that goes beyond their mental health difficulties through normalizing activities, which was a key change process (Paget, 2008). The “healing milieu” or environment is indicative and may have aided the recovery process of members through its structured activity and safety boundaries, shown to positively influence health outcomes for patients (Mahoney et al., 2009; Pearce & Haigh, 2017a). This further promotes a natural and genuine caring connection, which provides an ideal foundation for trust (Bell, 1994). However, a future pitfall to this exists in sustaining the recovery identity following discharge, given how members demonstrated they can become too attached to the relationships of the TC and struggle to engage in outsider groups (Best et al., 2014). This highlights how connections with the external community through co-production can be useful in socializing and preparing members to maintain progress following graduation. Our study provides novel evidence of effective, dynamic co-production, highlighting the TC’s collective therapeutic process. The TC appeared to emphasize the user-led aspect, which was conducive in promoting growth for those involved and provided authenticity for those receiving the service (Lees et al., 2019). Co-production further extended empowerment through linking members’ strengths with local community and employment opportunities after graduation. Marcus (1998) demonstrated how inherent strengths of members are often highlighted and valued within TC settings, which can influence successful recovery. Conventional empowerment processes within TCs typically include gaining consensus on group decisions, taking on roles within community meetings and domestic chores in residential TCs that benefit the group (Kennard, 2004). Co-production appeared to benefit the “fusion” TCs, enabling groups to work together to adapt conventional aspects of DTCs to processes more accommodating to members. These adaptations were shown to support the other identified change processes and could reduce the likelihood of drop-out, which is a prevalent issue across TCs, particularly at the start of therapy (de Leon & Schwartz, 1984; Morris, 2014). The constant changes that occur within the TC due to co-production demonstrate the adaptability of the group. This was opposed to Clarke’s (2015) finding that members needed consistency to achieve synchronicity and familiarity with the TC group and its processes. As the present research findings show changes were discussed and agreed upon by all members, the TC’s key principle of democratization appeared to lead to greater compliance (Rapoport, 1960).
Across all themes, staff and peer mentors appeared to play a guiding role in providing tailored support to members to sustain progress, with members seemingly relying on them to contain the group at times. This appeared through facilitating reflective spaces, managing some conflicts within the group, providing phone support for members outside community meeting hours, and supporting co-production projects. Harrison (2023) discusses how leadership is necessary in establishing and upholding group boundaries, thus advocating the need for staff leadership. The employment of experts by experience is described by Lees et al. (2019) as the “third position” in mental health services, providing valuable support to patients and staff in delivering care (Davidson et al., 2012). While staff involvement could be seen as a divergence from the TC theory “community as method” and the emphasis of peer support (Pearce & Pickard, 2013), it may be a necessary provision for protecting modern day TCs within the NHS (Haigh, 2017). Thus, the importance of equipping and preparing staff and peer mentors in supporting TCs effectively is highlighted.
Strengths and Limitations
The study was unique in exploring perspectives of members from an established TC site and a newer TC site with the same therapeutic and structural principles. Although this was less considered in the research, the findings gave some insights into similarities and differences in experiences. The study utilized participants who were currently engaged as a group member, enabling a more accurate insight into “present” experiences of a phase. The study also included members who were “founding members” of both TC sites, generating longitudinal perspectives of the communities. This was helpful in providing insights into how the communities evolved from inception.
There were several limitations in the research. First, peer mentors were asked to look back on their own experiences of the TC while they were active members which created a retrospective account. As such, their experiences as a group member may have been influenced by their peer mentor experiences. The criteria for members to have completed two phases (one year of their treatment) may have resulted in missed processes of change that could have occurred in the first phase, which members may have forgotten to mention retrospectively. Including members currently completing their first and second phases could help capture these experiences in vivo. An extended analysis of members’ patient documentation, written feedback as demonstrated by Janeiro et al. (2018), may enable more accuracy in members’ reflections.
The researcher was aware that entering a tight-knit community may have influenced some members’ responses, particularly when discussing challenges with someone they did not know (Waldram, 2007). A longitudinal qualitative approach, whereby the researcher interviews members at each phase completion timepoint, would be beneficial in tracking each individual member’s journey. This approach could form a more trusting relationship between the researcher and participant and increase the chance of participants’ sharing more sensitive issues. Sharing the group experiential themes with participants could have provided an opening for further conversations about generated ideas, which may have been helpful in eliciting more information and increase rigor. Using TC specific measures such as the Survey of Essential Elements Questionnaire (Melnick & De Leon, 1999; Melnick et al., 2000) may also help track participants’ experiences of change as they move through the phases of being in and graduating from the TC.
On a wider scale, TCs are unique to their service member needs and ways of working, making them heterogeneous services by nature (Campling, 2001; Sacks et al., 2008). Thus, findings may not necessarily be applicable for many reasons, for example, time and space practicalities, funding, and diagnostic populations, but could be adaptable.
Implications and Future Research
The empirical findings have important implications in inspiring and enhancing existing TCs. As demonstrated, TCs are a treatment setting for a diverse range of individuals from different backgrounds. Needs (2018) acknowledges the unequivocal importance of creating a therapeutic environment that is conducive in establishing trust and social support. Through co-production, theme 3 mostly emphasized how the TC environment was thoughtfully constructed by members to enhance these aspects through projects. This emphasizes the need for NHS-based TCs to encourage suggestions from those utilizing services, to improve patient experience and engagement within appropriate therapeutic environments (Marshall et al., 2019; Pilgrim, 2018).
Cultural differences can impact members’ engagement in sharing and connecting with others. Cultural aspects appear less outrightly addressed within the Core Standards and Values for TCs (Paget, 2008). This may be helpful in acknowledging directly, to promote the need for supporting diversity and adapting therapeutic elements in TCs (Bunt et al., 2008). Such adaptations may include providing open spaces for TC members to discuss and celebrate cultural differences as part of therapy, which could allow for a more inclusive environment (Jones, 2018). Additionally, when members first enter the TC, they could be asked about their style of communication and whether any adaptations need to be considered to help them adjust to TC. Pearce and Dale (2018) assert the importance of training for TC clinicians, involving learning about the theoretical underpinnings of TCs, alongside relational practice and experiential training through visiting established TCs. Supplementing this with cultural training for TC staff may help to promote understanding into how client, staff, and organizational backgrounds can serve to create diversity among group processes encountered within the TC (Jones, 2018). Furthermore, the training could highlight how the influence of the socio-political environment TCs are embedded in can impact individual change (Mallow & Cameronkelly, 2006).
Across all themes, the role of staff is highlighted through complex situations, risk, and assisting with co-produced projects. Alongside, peer mentors are experts-by-experience who provide a vital layer of lived experience–informed knowledge to guide active members. Lees et al. (2019) advocate for the continued supervision of mentors as their roles evolve, to ensure they are well informed to provide help to others. Care needs to be taken to ensure they are feeling mentally and physically well enough to function within their role. This extends to active members exploring experts-by-experience opportunities while undertaking their own TC therapy. Future research could explore how fusion TCs are experienced by staff to complement this study and expand insights into supporting staff. The results indicated that reflective spaces in between phases helped members reflect on progress. Reviews are integral parts of TC treatment; however, in DTCs these are done in front of the whole community rather than individually (Pearce & Haigh, 2017b). Further research into how reflective spaces or “reviews” with members work within TCs may provide further insights into aspects of change, beyond the TC’s weekly community meetings.
Conclusion
The study explored processes of change through residents engaging in a fusion TC setting. The study revealed themes pertaining to embracing vulnerability through sharing with the group and personal reflection, navigating relationships through building connections with others, and managing conflict together and engagement in co-production. The discovered themes provide evidence of change processes which align with existing research, thus reducing the ideological status of current theory (Shuker, 2010). The findings also highlight processes that could be implemented into existing TCs and provide insights into how TC practice could be more informed to accommodate the growing diversity of TC members and support staff development.
Footnotes
Acknowledgements
Many thanks to the members of the therapeutic community for their interest and participation in my research. I extended thanks to the staff members of the therapeutic community for their help in recruiting participants and organizing clinical and community space to interview participants.
Ethical Considerations
Our study was approved by the University of Southampton Ethics Committee (ERGO Number: 79605) and the NHS London- Camberwell St Giles Research Ethics Committee (IRAS Project ID: 323693).
Consent to Participate
All participants provided verbal and written informed consent prior to enrolment in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two of the authors (CF and NB) have worked in the researched therapeutic communities.