
Abstract
In order to graduate physicians prepared to effectively address clinical issues in palliative medicine and to comply with LCME requirements, the Northeastern Ohio Universities Colleges of Medicine and Pharmacy (NEOUCOM) integrated a coordinated four-year palliative care (PC) curriculum. This report describes the development of the longitudinal curriculum and provides helpful resources and strategies to guide clinicians and administrators undertaking similar efforts. This is a retrospective, descriptive report based on data collected throughout development of the new curriculum. A Palliative Care Advisory Committee initiated development of curricula in PC. An Office of Palliative Care was established to assess and coordinate offerings. Curriculum transformation was based on best practices. Two cornerstone pieces are highlighted: a mandatory hospice experience and a case based small group discussion prior to graduation.
Introduction
Palliative medicine is an interdisciplinary approach to care that aims to improve the quality of life and function and relieve suffering for patients with serious and life-threatening illnesses and their loved ones. Given the demographics of our rapidly aging population and the shift toward chronic conditions that practitioners are now expected to manage, it is clear that palliative and end-of-life care and the issues surrounding them will be confronted with increasing frequency. As such, it is imperative that all physicians-in-training be exposed to this rapidly growing field. 1 This has been widely recognized such that in 2000, the Liaison Committee on Medical Education instituted requirements for education on end-of-life care. 2 Despite the requirement, the training that most medical students receive in this realm varies widely, is often disjointed and sporadic, and can leave students feeling unprepared.1,3–6
In response to the lack of a cohesive curriculum in palliative medicine, Northeastern Ohio Universities Colleges of Medicine and Pharmacy (NEOUCOM) chose to implement a comprehensive program of study spanning all 4 years of its medical education program. Using limited resources, this was accomplished within a 3-year timeframe. Key elements of the process included: securing the commitment and resolve of core clinical faculty leaders and students; building on the best of the existing curricular pieces; filling the gaps in content areas while eliminating overlap of other material; and establishing an administrative Office of Palliative Care at NEOUCOM to coordinate and evaluate offerings. This article will describe the above processes and focus on 2 cornerstone pieces of the mandatory curriculum during the third and fourth years of medical school.
Methods
Needs Assessment
In 2006, a Palliative Care/End-of-Life Task Force convened to assess the quantity and quality of palliative medicine education at NEOUCOM. Task Force representatives included faculty in basic, behavioral, and community health sciences, geriatrics, palliative medicine (adult and pediatric), local palliative care practitioners, members of the student body, and recent medical school graduates. The Task Force conducted an assessment of what was already available to students in the realm of palliative care. Through use of careful curricular mapping, a survey of M4 students, and student focus groups, it was found that there were didactics, small group discussions, and experiential learning opportunities occurring, however, they were not presented in a cohesive nor coordinated manner. While there was some overlap in topics covered, there were other clear gaps in core content areas. Additionally, clinical experiences were erratic and depended largely on the institution where the student happened to be assigned to their clinical rotations. The initial conclusion of the Task Force was that existing learning opportunities in palliative medicine were disconnected and serendipitous.
Challenges
Securing “champions” for palliative care both within the medical college and on each of the clinical campuses was the crucial next step. NEOUCOM has 8 major community-based teaching hospitals located in 3 geographically distinct areas, each with widely varying resources in hospice and palliative care. Students are placed across all sites for their required clinical rotations and electives, making it necessary to gain buy-in from administrative and clinical leaders on each of the campuses. The clinical faculty from these sites who joined the Task Force played a key role in garnering the support of their palliative medicine colleagues within the hospitals and community hospice agencies. It was critical to the success of this endeavor to find a group of dedicated and passionate clinicians willing to donate their time and effort.
The College itself was in the midst of a major curricular reform effort, and the Task Force used this momentum for change as a catalyst to integrate palliative medicine into the general curriculum. More challenging was eliciting full administrative support from the College of Medicine. Based on the efforts and recommendations of the Task Force, the College was supportive in principle, however, financing change was more complex. Fortunately, NEOUCOM was selected at this time to participate in the Medical School Palliative Care Education project sponsored by the Medical College of Wisconsin through the Robert Wood Johnson Foundation. This highly competitive grant provided minimal funding but was a key factor in solidifying administrative support and providing the impetus for embedding offerings into the clinical years. It also convinced administration that the curriculum and an Office of Palliative Medicine could be sustainable.
The Office of Palliative Medicine
Through the strong advocacy efforts of the Task Force members, an Office of Palliative Care (Office) was established in 2007 within the Department of Behavioral and Community Health Sciences on the College of Medicine campus. This was a major step toward entrenching palliative care into the framework of the College of Medicine. The Office is necessary in order to provide centralized administrative support to the faculty teaching palliative medicine at all the clinical sites as well as coordination and assessment of curricular offerings and evaluations. Due to fiscal constraints, resources for the Office were primarily drawn from the existing Office of Geriatrics in the Department of Behavioral and Community Health Sciences. However, the 2 offices remain distinct, with the Office of Palliative Care focusing on palliative issues throughout the life span.
A Palliative Care Advisory Committee for the Office was officially formed from the original Task Force; it expanded to include representatives from many of the disciplines involved with end-of-life care—chaplains, social workers, nurse practitioners, physicians (both adult and pediatric), faculty members from various departments of the medical school, and students. This Advisory Committee continues to be the driving force behind the project, providing valuable oversight to the curriculum, helping to recruit faculty, and guiding Office activities.
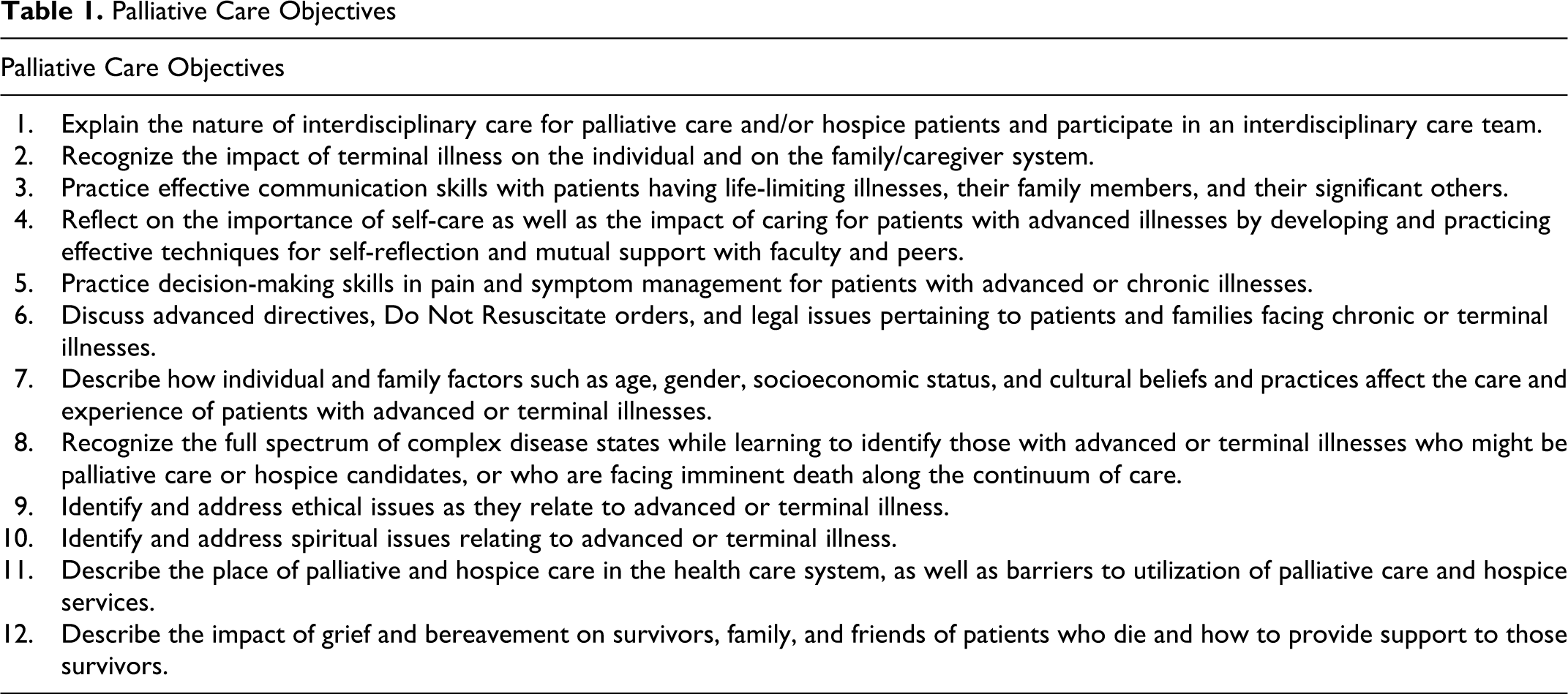
Curricular Design and Implementation
Consensus of the Task Force was that the most effective method of implementing the new palliative medicine curriculum across all 4 years was to embed it into existing courses and clerkships rather than vying for large blocks of curricular time. Goals and learning objectives for the curriculum had been developed by the original task force based on expert consensus, student need, literature review7,8 and LCME requirements (see Table 1 ). To comply with the Medical School Palliative Care Education Project, new curriculum development began in the third and fourth years, which are often the most difficult to permeate. The 2 best experiences on any of the individual campuses were selected to be replicated at all other sites based on student input via evaluations and focus groups as well as faculty consensus. Implementing this “best practice” approach was most efficient as the curriculum was already developed and there were experienced faculty who could teach others how to implement it. Moreover, starting with experiences that would likely generate positive feedback among students and faculty would open the door for recruitment of more faculty and support for additional curricular development and implementation.
Palliative Care Objectives
Curriculum
An outline of the coordinated 4-year curriculum is provided in Table 2 . A curricular map such as this is a useful way to visualize and evaluate the curriculum’s ability to meet its stated objectives and address the corresponding competencies. It also provides a shorthand means of illustrating and communicating curricular impact across the educational continuum to key stakeholders.
Curricular Map a
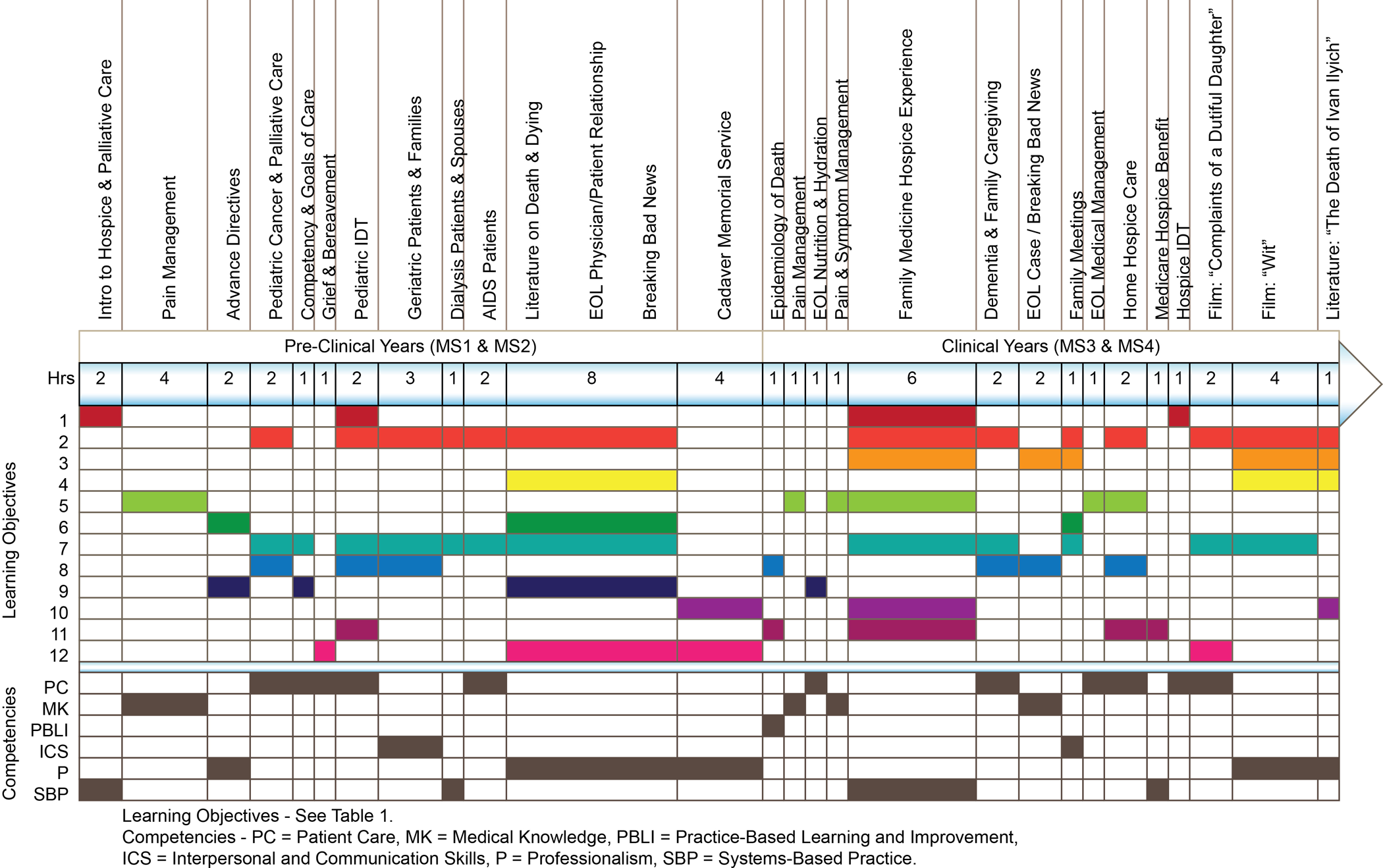
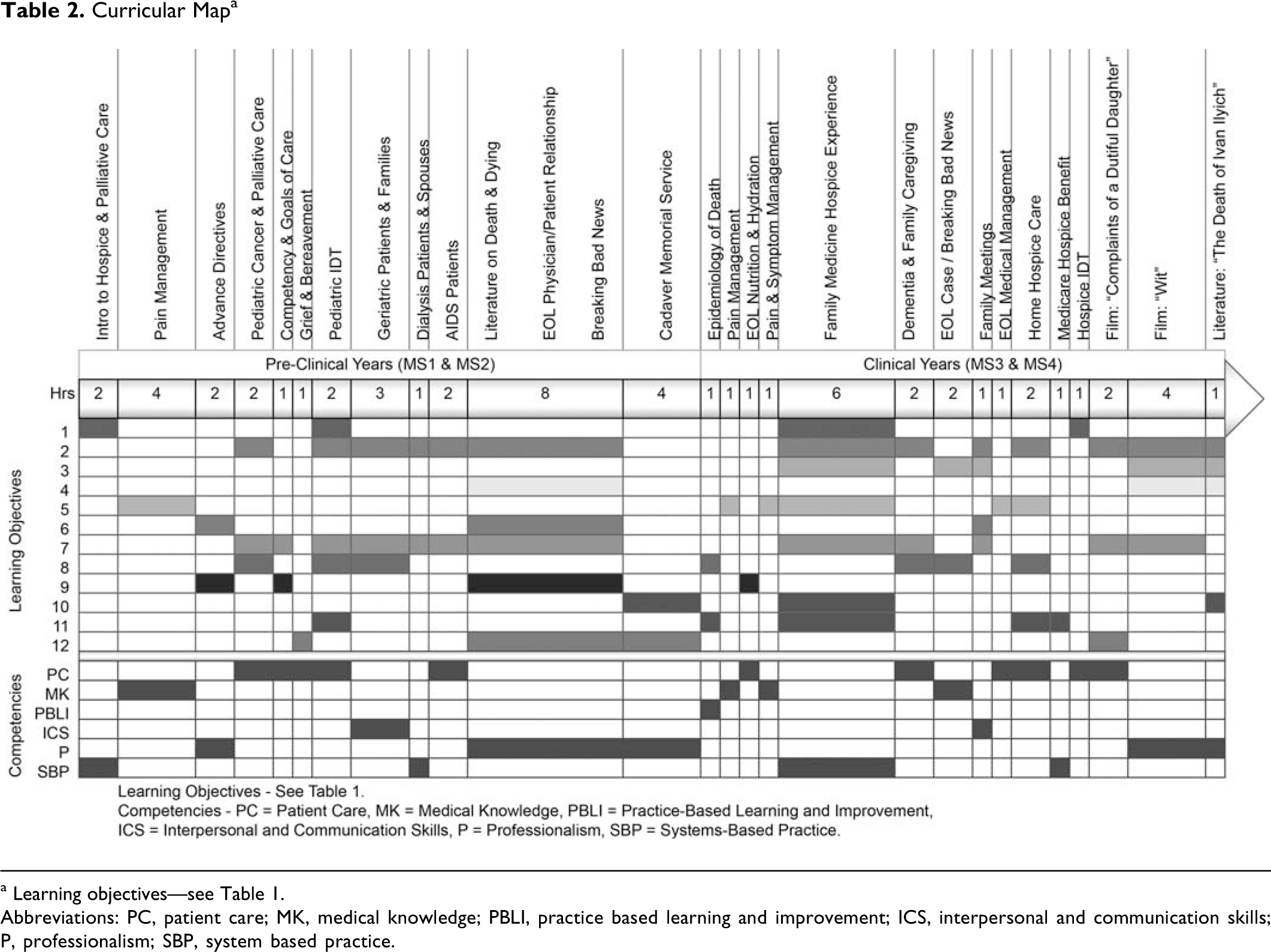
a Learning objectives—see Table 1.
Abbreviations: PC, patient care; MK, medical knowledge; PBLI, practice based learning and improvement; ICS, interpersonal and communication skills; P, professionalism; SBP, system based practice.
Preclinical Years
First- and second-year students receive introductory lectures on key palliative medicine topics—legal and ethical issues, pain and symptom management, end-of-life discussion skills, grief, etc. They also observe an interdisciplinary team meeting, engage in standardized patient discussions, and write reflective essays on assigned readings with supplemental discussions. Efforts have been made to minimize repetitious lectures and ensure core material is introduced prior to embarking on the described clinical experiences below. Furthermore, an active student interest group has helped garner interest among students in their preclinical years. The Office works closely with this group to sponsor enrichment activities, service projects, and mentoring experiences.
Clinical Years—M3
There are 6 required rotations for students in the third year of medical school—internal medicine (IM), family medicine (FM), surgery, OB/GYN, psychiatry, and pediatrics. Curriculum integration began with the internal medicine and FM rotations, with the eventual goal of including mandatory material in all of the above core disciplines. Internal medicine and FM were selected first due to the “best practices” model discussed above. A case-based learning experience during IM regarding pain and symptom management and end-of-life discussions was expanded from one clinical site to all of them. During this clerkship, a requirement to complete a workbook on core hospice and palliative medicine topics was added. The American Academy of Hospice and Palliative Medicine Primer of Palliative Care 9 is provided to students as a reference at each clinical site and for completion of the workbook.
From a single FM clerkship site, a hospice experience was expanded to all clinical sites. During the hospice experience, students participate in an interdisciplinary team meeting at a community hospice, are paired with a patient from the hospice agency, and make 3 home visits. The visits are supplemented by didactics and small group discussions and debriefing. The didactic materials are videotaped and made available online for the convenience of students and faculty. Finally, each student is required to write an essay reflecting upon their encounters with the hospice patient (see Appendix A for details regarding this experience).
Since the integration of these first 2 experiences, lectures regarding pediatric palliative care have been introduced into the pediatric clerkship, and another case-based learning experience added to the surgery rotation curriculum. Work is still being done to include palliative medicine in the OB/GYN and Psychiatry rotation experiences.
Clinical Years—M4
Additional elective opportunities are available to fourth-year students in an inpatient acute palliative care unit, community hospices, and pediatric palliative medicine. These clinical experiences conclude at the end of the fourth year with the Clinical Epilogue. The Epilogue involves small group discussions, led by a physician and other hospice and palliative care team members, of cases illustrating key issues students are likely to face in their transition to residency. The cases are specifically designed for and organized by the specialty the student will be entering. These discussion groups are staffed by faculty from those specialties and are paired with palliative care faculty who act as facilitators. Students appreciate the practical focus of this module in providing guidance in delivering bad news, death pronouncement, and prescribing pain medication. By gathering the entire class weeks before graduation, the Epilogue has served to consolidate and reinforce elements of the PC curriculum previously encountered (see Appendix B for details regarding this experience).
Evaluation and Outcomes
A multifaceted approach is being used to track outcomes of the new curriculum (see Tables 3 and 4 ). To acquire baseline data to assess changes in student knowledge and attitudes, surveys based on the work of David Weissman, MD, Medical College of Wisconsin, focus groups, and objective examinations were conducted with 2 classes of senior medical students who did not receive any of the new curricula. These measures are conducted annually with senior students for comparative data. In addition, relevant results of the Association of American Medical Colleges Medical School Graduation Questionnaire are being tracked for several years precurricular and postcurricular implementation to assess longitudinal changes in the learning environment for palliative care.
Assessing the Learner
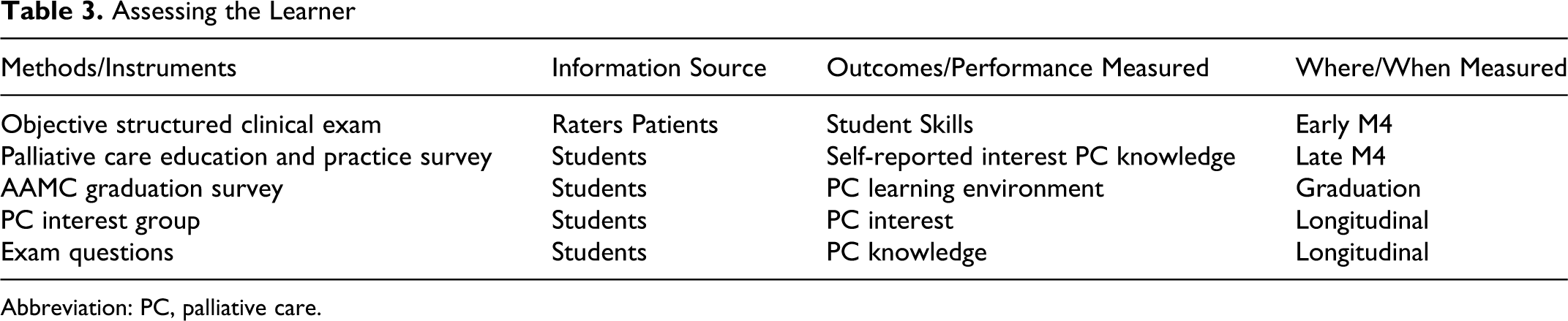
Abbreviation: PC, palliative care.
Evaluating the Curriculum
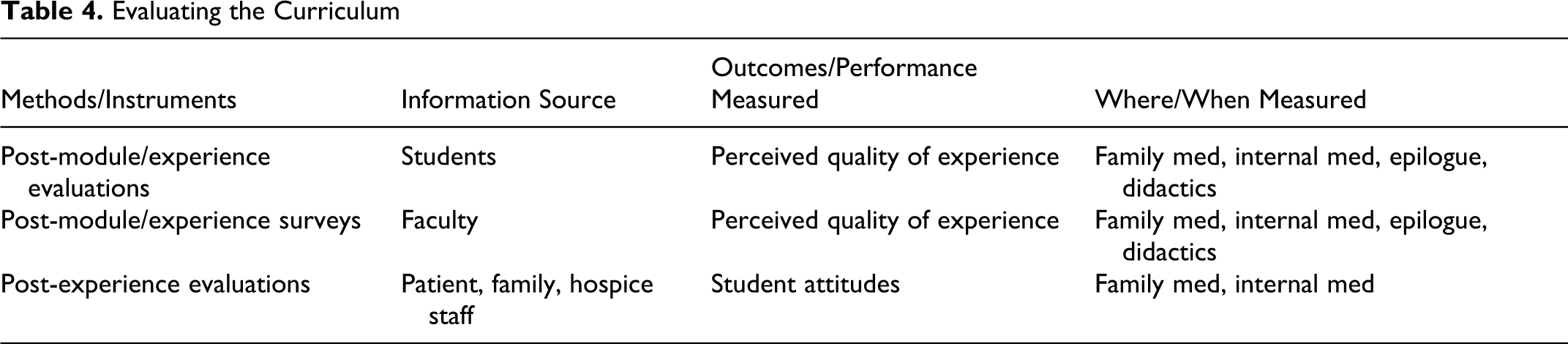
Students participate in Clinical Skills Assessments throughout their medical school training and may be exposed to cases with palliative care themes as a part of these examinations. Work is being done to better standardize the assessment of the palliative cases and to ensure that all students have the opportunity to practice their skills with a standardized patient. Objective exam questions are also used in the first and second years to assess students’ knowledge of core material and effectiveness of the teaching modalities. Student and patient evaluations are routinely completed for third- and fourth-year palliative care activities; feedback has been overwhelmingly positive. See Table 5 and 6 .
Family Medicine Hospice Experience Student Evaluations a
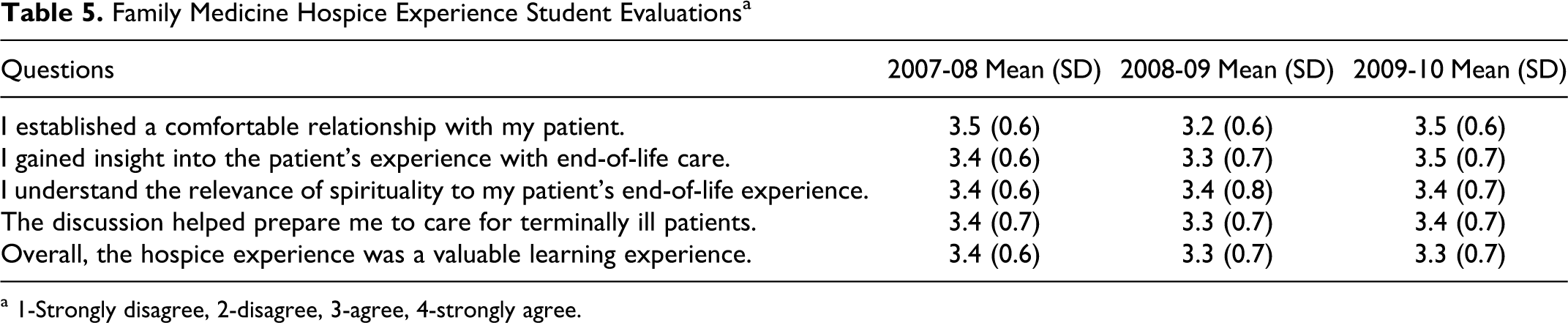
a 1-Strongly disagree, 2-disagree, 3-agree, 4-strongly agree.
Clinical Epilogue Student Evaluation a

a 1 = Strongly disagree, 2 = disagree, 3 = undecided, 4 = agree, 5 = strongly agree.
Perhaps, most revealing have been reflective essays written by students upon completion of their family medicine hospice experience. These essays have repeatedly shown that this experience is very powerful for students. As one student put it: “I can confess that each visit has left an unforgettable memory on my heart …. I have been exposed to a tremendously different view of medicine.” Others have discussed the important lessons their patients imparted: “Going into this situation, I thought that I was supposed to offer or do something for this patient. I now realize that he did far more for me than I could ever do for him.” Software is currently being utilized as part of a qualitative analysis of these essays to identify recurring themes.
Informally, the degree of participation in the Palliative Care Student Interest Group (increasing annually, from 17 students in the 2007-2008 academic year to 41 students in the 2009-2010 academic year), attendance at Palliative Care-themed or sponsored events, the number of palliative care electives taken by students, and student career choices (at least four recent graduates have sought palliative medicine fellowship training) suggest that the curricular changes have had a positive impact on student attraction to palliative medicine.
Faculty involvement and feedback have also been tracked. Retention of volunteer physicians and representatives from other palliative care and hospice disciplines has been consistently stable (91%-100%) as has their expressed satisfaction with participation in educational activities. We attribute faculty retention and satisfaction in part to the Office’s responsiveness to faculty course evaluations; for example, revisions made to the Epilogue were based on faculty feedback. Additionally the Office maintains timely communications, efficient quarterly meetings, and reports positive feedback from students, which reinforces the impact of their efforts and commitment.
Plans are in place to continue obtaining student feedback as well as to obtain feedback from graduates in residency training and clinical practice to guide further curriculum reform with the goal of documenting a lasting impact on their clinical practices attributable to the comprehensive curriculum.
Limitations
While the integration of palliative medicine material throughout the 4-year medical school curriculum has been successful and feedback thus far from all involved has been overwhelmingly positive, the process itself has certainly been imperfect. For example, due to financial constraints and time pressures, curricular pieces were sometimes designed and implemented, without allowing for clearly measurable learning objectives to be created and tracked over time. Additionally, gaining access to evaluation data embedded in multiple courses across all 4 years has been challenging. Evaluation data have therefore been largely limited to subjective feedback from faculty, students, and patients. Education specialists at the medical school, along with course directors and others involved in the evaluation process, are included in creating newer more comprehensive evaluation tools to assess the impact of the curriculum and how best to revise it to meet both students’ and practitioners’ needs. Another area of concern remains that teaching faculty experience and institutional cultures with regard to end-of-life care differ significantly across the consortium. So, while student exposures are more standardized now than in the past, there is still a degree of variability in the quality of their experiences.
Future Directions
As with any new educational endeavor, the palliative care curriculum requires continual oversight, rigorous assessment, and revision. New content has been recently introduced into the Pediatric and Surgery clerkships and there are plans underway to integrate into the remaining core clerkships of OB/GYN and Psychiatry. Collaboration with faculty in the Human Values in Medicine and the Biomedical Ethics programs at the College of Medicine shows great promise for further enrichment of curricular content. A subgroup of faculty has formed to consider enhancing the curriculum with more content related to spirituality and cultural diversity. Student interest has grown as reflected in the activities of the Palliative Care Student Interest Group. Pharmacy students, new to the campus, also have mandatory palliative curricula and available electives in pain and palliative pharmacology, which are well subscribed. They too are joining the palliative care student interest group, creating opportunities for informal interdisciplinary collaboration.
The Office of Palliative Care faces ongoing challenges in securing sustainable funding, monitoring this multifaceted and complex curriculum at diverse sites and in recruiting additional faculty all while maintaining student interest and enthusiasm.
Conclusion
Palliative medicine is rapidly expanding due to the changing nature of the patient population. Nearly all medical school graduates will be faced with these issues as they continue in their training. In order to ensure that high-quality care is provided to terminally ill patients, it is crucial to educate students in a coordinated, comprehensive manner. By gathering a team of dedicated clinicians and faculty, securing administrative and student support, and creating a centralized office for coordination, it is possible to increase both the quantity and quality of palliative care education for future physicians.
Footnotes
Acknowledgments
The authors would like to thank the members of the original Palliative Care/End-of-Life Task Force and the current Palliative Care Advisory Committee for their commitment to bringing this vision to fruition. The authors would also like to thank David Weissman and Timothy Quill for their early advice and encouragement as well as the Robert Wood Johnson Foundation its seed funding of this project.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.