
Abstract
Despite improving organization of hospice for children with life-limiting illnesses, services may be underutilized. We asked representatives of all 76 existing North Carolina hospice organizations about barriers to serving children. Representatives of 61 agencies responded (80%). Hospices serving children differed from hospices not serving children on perception of barriers: 1) Lack of pediatric trained staff (8% vs 42%, p = 0.01); 2) lack of pediatrician consultation (23% vs 50%, p = 0.03); 3) lack of pediatric pharmacy (4% vs 32%, p = 0.006), and inconsistent plan of care between pediatrician and hospice (12% vs 47%, p = 0.01). Lack of pediatric referrals (78%) and families wanting to continue curative therapies while receiving hospice care (77%) were felt to be the most important barriers overall. Enhanced training of pediatric providers and a model of care which blends disease-specific treatment with hospice may improve access to hospice services for children.
Introduction
Each year in the United States, approximately 50 000 children die and 500 000 children cope with life-limiting conditions. 1 Hospice plays an important role for children with life-limiting illnesses by providing services that meet the medical, social, spiritual, and psychological needs of these children and their families, but it only reaches 10% to 20% of the children dying in the United States. 2 Hospice services have been shown to reduce symptoms, improve quality of life, and impact the perception of quality end-of-life care in adults. 3 A survey of pediatric medical care providers concluded that the majority observed an advantage to utilizing hospice care for dying children as compared to providing end-of-life care without hospice involvement. In this study, the most frequently cited reason for preferring hospice involvement was better provision of nonmedical services such as psychosocial services, anticipatory grief support, and superior care coordination. 4
Despite relatively limited data on hospice care for children, the Institute of Medicine and the American Academy of Pediatrics strongly advocate for the integration of palliative care and hospice care for children with life-limiting illnesses. As hospice is utilized by a minority of children with life-limiting illnesses dying in the United States, further understanding of barriers to use can suggest opportunities for improvement. The aim of this study was to describe the current status of hospice care for children in the state of North Carolina, which has average to low overall hospice use in the United States 5 and to describe the available services and barriers to hospice care as perceived by representatives of hospice organizations.
Methods
Hospice organizations were identified in North Carolina via membership in the Carolinas Center for Hospice and End-of-Life Care as well as those facilities licensed by the State of North Carolina by the Department of Health and Human Services. 6,7 Hospice directors or appointees were invited by e-mail to complete a 23-question Web-based survey. Potential participants were given 1 month to respond, and then 2 reminders were sent by e-mail at 1 month intervals to those not responding. Those who did not complete Web-based surveys after 2 reminders received a request by mail, and a final request was made by telephone.
Survey questions were developed by our research team based on the review of prior research on barriers to hospice services. 8 Items were drafted and then refined with input from health care professionals who participate in the Pediatric Palliative Care Coalition of North Carolina. This coalition includes local hospice directors, community advocates, and palliative care team members from around the state. Question topics included hospice agency characteristics, current service to children and willingness to serve children, services provided over the past year, and perceived barriers for hospice care for children. The 16 multiple choice questions about barriers to hospice care for children used a 4-point scale for responses, ranging from very important to not at all important. The study protocol was reviewed and approved by the University of North Carolina Institutional Review Board prior to data collection.
Statistical analysis included descriptive statistics and frequency tables for all responses. Responses were compared for differences among agencies that did and did not provide services to children using Fisher Exact tests. All analysis was performed using SAS statistical software, version 9.2 (SAS Institute Inc, Cary, North Carolilna).
Results
Representatives of 61 of 76 eligible hospice organizations agreed to participate (80% response rate). Responding hospice organizations were typically free standing (60%) and organized as nonprofits (82%). The distribution of agency types was similar to all Medicare-certified hospices, 9 but the tax status was more often nonprofit (Table 1). Most surveys were completed by the directors or administrative personnel (81%), and 19% of the surveys were completed by clinical personnel.
Characteristics of Hospices Agencies Participating in the Survey as Compared With the Center for Medicare and Medicaid Services (CMS) Data on Certified Hospice Agencies
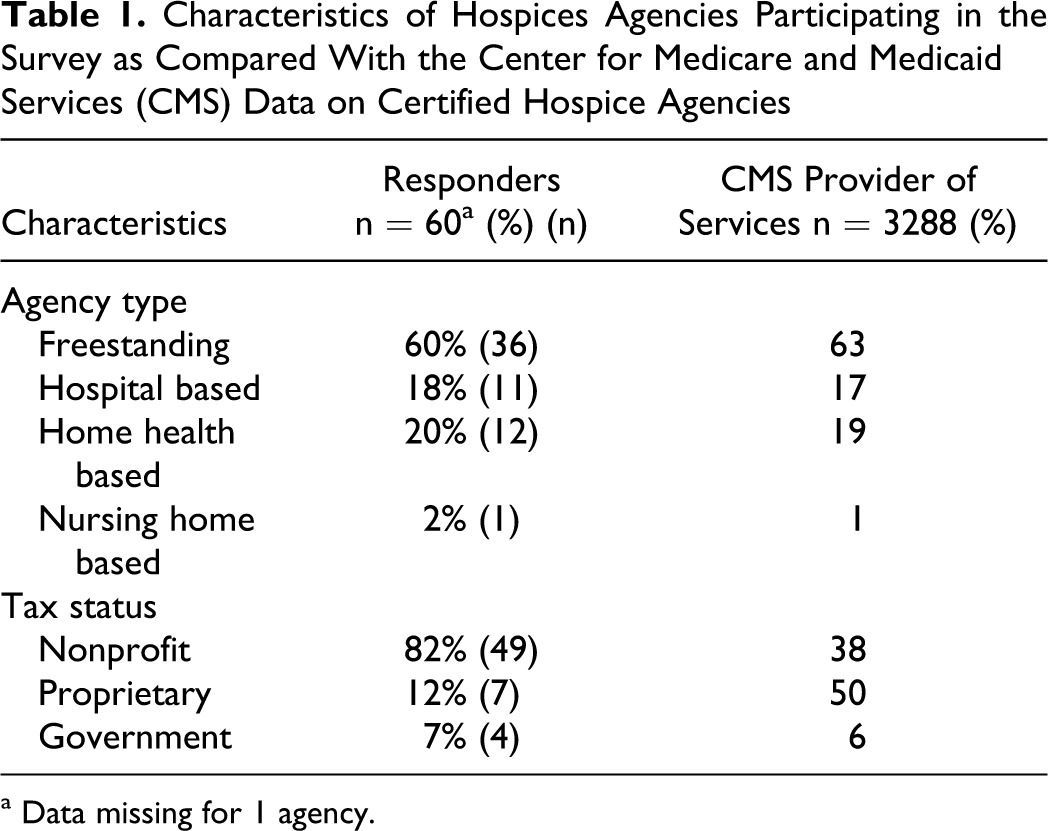
a Data missing for 1 agency.
Services Provided by Hospice Agencies
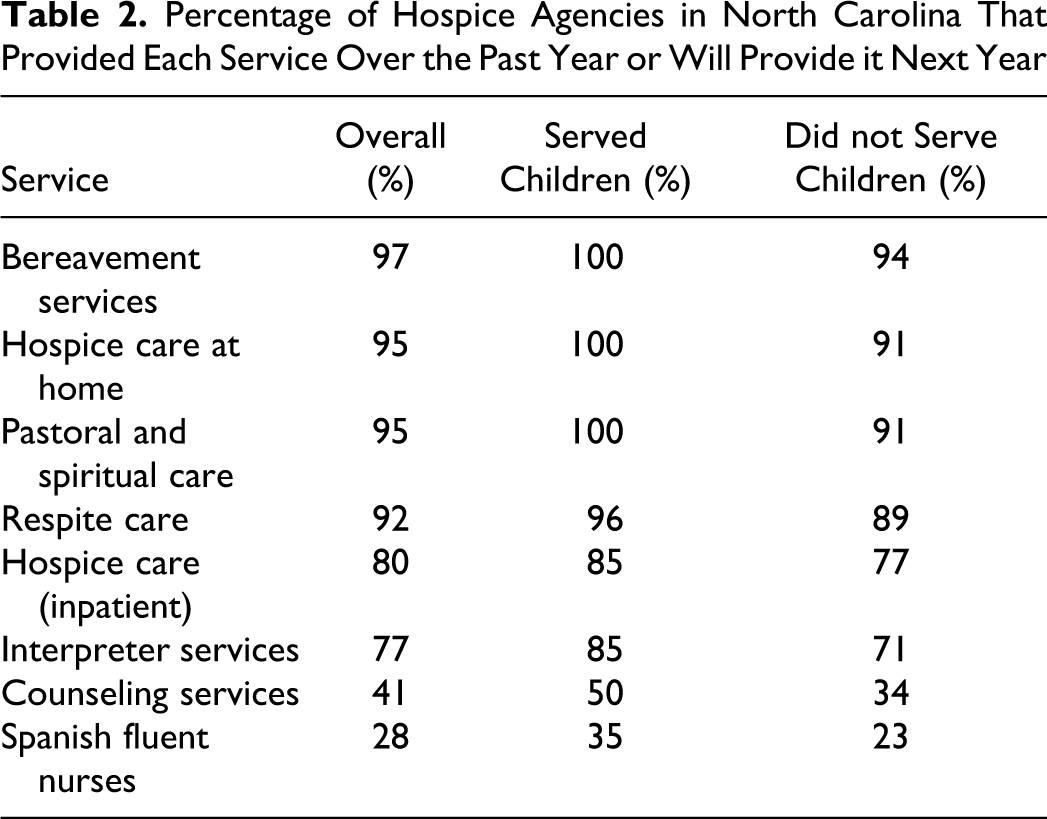
When asked about services they provided in the past year or will be able to provide in the next year, 58 (95%) agencies indicated that they provide hospice care at home and 49 (80%) offer inpatient hospice care. Other services offered include pastoral and spiritual care (95%), respite care (92%), and bereavement services for family members (97%). While 77% of agencies offer interpreter services for non–English-speaking patients, only 28% employ Spanish-fluent nurses. For all services, a higher percentage of agencies that serve children provide those services, but no differences were statistically significant (all P values ≥ 3 .25; Table 2). Figure 1 shows the geographical distribution of hospice agencies that serve children in the state of North Carolina.
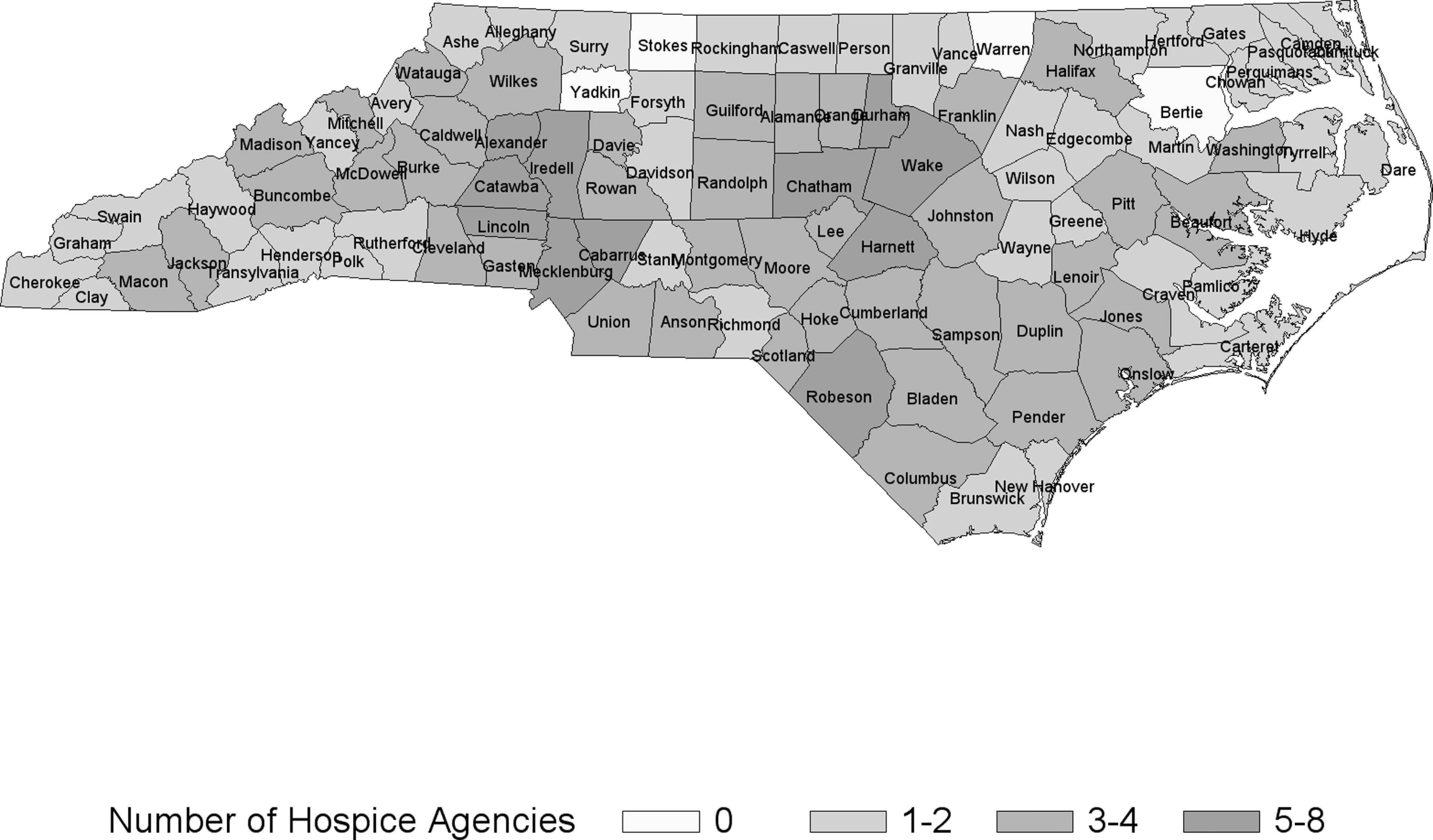
Geographical distribution of hospice agencies that serve children in the state of North Carolina
Percentage of Hospice Agencies in North Carolina That Provided Each Service Over the Past Year or Will Provide it Next Year
Perceived Barriers to Serving Children
In all, 26 (43%) agencies currently provide services to children. All agency representatives were asked about barriers to hospice care for children. The most important perceived barriers (rated as very important or important), regardless of current service to children, include lack of pediatric referrals (78%) and families wanting to continue curative therapies while receiving hospice care services (77%; Figure 2). These were described as very important by 58% and 51%, respectively. Other perceived barriers (rated as very important, important, or somewhat important) include complexity of children’s care needs (79%), lack of pediatric-trained personnel (71%), lack of pediatric consultation (67%), lack of certainty about meeting determination that the patient has no longer than 6 months to live (66%), and language barriers (64%).
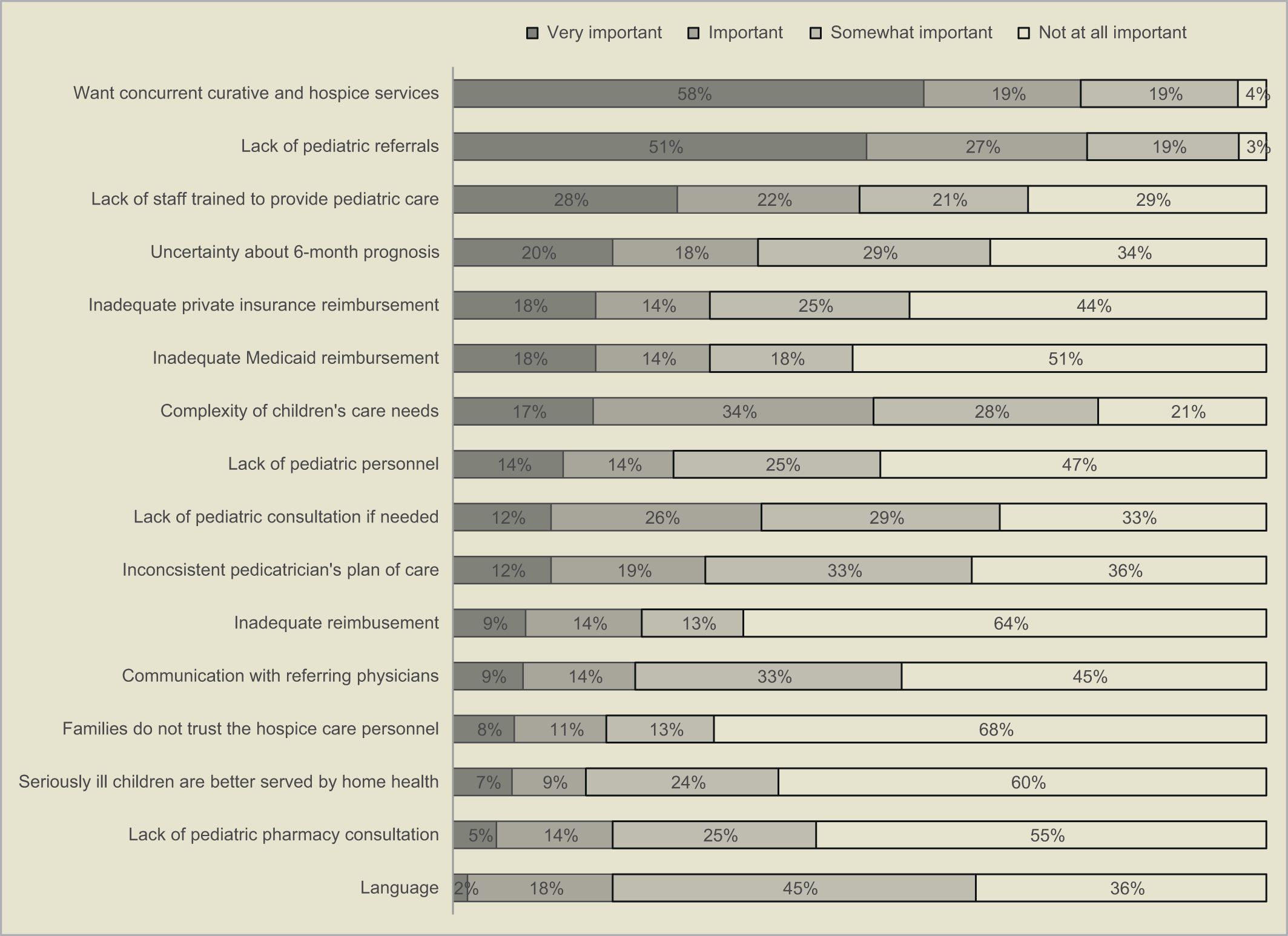
Barriers as perceived by all hospice agencies combined
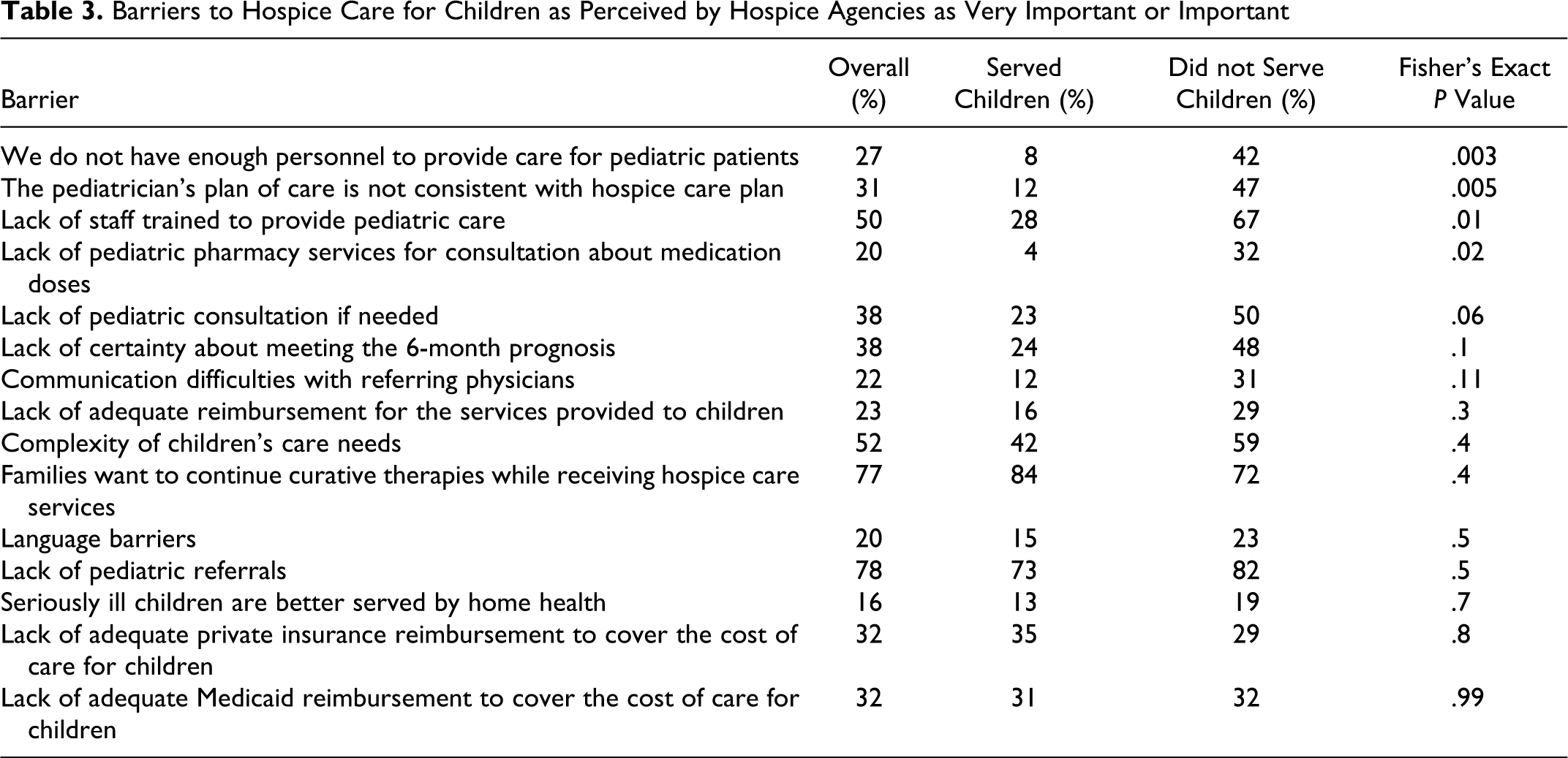
Differences in perceived barriers for agencies that did and did not serve children are summarized in Table 3. A significantly higher proportion of agencies that did not provide services to children indicated that lack of trained staff to provide pediatric care was a very important issue (42% vs 8%; P = .02). Other barriers reported as very important or important more often by agencies that did not serve children were inconsistent pediatrician and hospice plan of care (47% vs 12%; P = .01), lack of staff trained to provide pediatric care (67% vs 28%; P = .01), lack of pediatric pharmacy services for consultation about medication doses (32% vs 4%; P = .02), and lack of pediatric consultation if needed (50% vs 23%; P = .06).
Barriers to Hospice Care for Children as Perceived by Hospice Agencies as Very Important or Important
Discussion
For the 50 000 children dying in the United States each year, hospice is the exception rather than the standard of care at the end of life. The results of this survey of hospice providers across 1 state, North Carolina, provide a more detailed description of current services and suggest barriers that need to be overcome to expand hospice services for children.
The most important barrier recognized by hospice organizations was lack of pediatric referrals. As described by Fowler et al, 10 pediatric oncology patients may be referred to hospice late in the disease course. Pediatric oncologists most commonly cited continued therapy as the reason for not referring patients to hospice. In the same study, oncologists who had more patients die at home had more access to hospice services that allowed continuing chemotherapy and blood product transfusions. Thus, having a more flexible hospice service may lead to increased referrals. 10 Davies et al 11 also explored pediatric providers’ perceptions of barriers to hospice enrollment. The most common responses included uncertain prognosis, family preferences, language barriers, and time constraints of the medical provider.
Since life-limiting conditions are rare in children, general pediatricians and subspecialists may have limited experience caring for dying children. They may also perceive hospice referral as a failure or as giving up hope. 12 Friedman et al 13 reported lack of awareness and misunderstanding of hospice care by patients and families. They also reported that physician difficulties in prognostication and denial of severity of patient’s illness may delay referrals to hospice. More exposure to outpatient care of children with life-limiting illnesses during medical school and residency training would address this barrier. In the 1970s, 6% of medical schools addressed palliative care in their curriculum. By the 1990s, that figure had risen to 30%, but most courses were preclinical or elective. 14 Even within a pediatric subspecialty exposed to relatively high patient mortality rates, such as oncology, physicians have reported inconsistent preparation for, and comfort with, providing comprehensive end-of-life care. 15 Physicians who are unprepared to discuss hospice as an option may find it natural to support hospital care for dying children.
The second most important barrier identified by hospice providers was families wanting to continue curative therapies for their children while in hospice care. This has been described previously; parents of children with life-limiting conditions usually have dual goals of treatment—hoping for cure, while keeping pain and other distressing symptoms under control. 16 Families and even health care providers may perceive a referral to hospice as giving up or losing hope. 12
The Medicare Hospice Benefit, created by Congress in 1982, provides a per diem reimbursement for hospice care of patients determined to have a life expectancy of 6 months if the disease follows its expected course, and for whom the goal of care is palliative rather than curative. Some hospices may require patients and families to forgo therapies such as noncurative or experimental chemotherapy and blood transfusions. 10 Most hospice care is provided in the home, yet the majority of infants and children die in hospitals. 17 Thus, dying children may not easily fit into the current structure of hospice care. Furthermore, children with complex medical conditions may have health care needs, such as a requirement for parenteral nutrition, transfusion, assisted ventilation, or in-home nursing, that are not reimbursable under most health insurance plans. 18
The Concurrent Care for Children Requirement (CCRC) provision (Section 2302 of the Patient Protection and Affordable Care Act), recently enacted into law by President Obama, states that children under the age of 21 who have been diagnosed with a life-limiting illness—and are eligible for Medicaid or the Children’s Health Insurance Program—may receive all services that are related to the treatment of a child’s life-limiting illness. 19 This would allow these children access to hospice care services while they are receiving other disease-modifying treatments. As implementation of this legislation will vary from state to state, its exact implications will also vary. This policy change has the potential to overcome one of the leading barriers reported in this survey study—the desire of families to continue curative or disease-modifying therapy while entering hospice care.
As North Carolina has one of the fastest growing Hispanic populations in the United States, with 8 times the growth of the non-Hispanic population and more than doubling in the last 10 years, 20 we inquired about access to Spanish-speaking nurses and interpreter services. In all, 77% of organizations responding to this survey offer interpreter services for non–English-speaking patients, but only 28% employ Spanish-fluent nurses. Language barriers were recognized by 64% of the agencies as a particular concern for pediatric care. These may lead to ethnic disparities in access to hospice services. In the state of Florida, hospice expenditures were reported to be lower for children of other races as compared with white non-Hispanic children. Lower expenditures could be explained by delays in admission to hospice for this population of children or reluctance by ethnic and racial minorities to use hospice care. 21
Other perceived barriers (rated as very important, important, or somewhat important) include complexity of children’s care needs (79%), lack of pediatric-trained personnel (71%), and lack of pediatric consultation (67%). Children under 17 years of age make up only 0.4% of all hospice admissions in the United States, 22 and few hospice providers admit a sufficient number of children to achieve expertise in pediatric care. In order for hospice agencies to provide the same services for children that they provide for adults, they should employ staff with pediatric training that are competent and comfortable in providing care to children and families. Many hospice organizations have expanded their services to children and young adults in recent years, with 64% of 4700 hospice organizations surveyed in 2007 reporting willingness to accept children vs only 18% in 2005. 23 However, access to hospice care for children remains limited in many parts of the country.
There are several limitations to this study. The survey instrument was designed de novo and did not use a validated index or scale measuring barriers. A search for the previously validated instruments to measure barriers specific to pediatric hospice care was unsuccessful. Recall and reporter biases inherent to the retrospective design and survey format could also potentially misrepresent clinical realities. While the response rate was good, it may not fully represent all the resources available in the state of North Carolina. This study is also limited by describing only a single state, and hence may not be generalizable to the rest of the country. However, overall hospice utilization in North Carolina is similar to the United States. The survey did not address hospital-based or hospice-based palliative care services structured outside the hospice model of care, which is another innovation that may provide access to pain and symptom management and supportive care concurrent with disease-specific treatments. Additionally, this survey did not include specific questions about therapies (play, art, and music), child life specialists, and sibling care which are relevant to the pediatric hospice population.
There are several important implications of this study. For pediatric residency and subspecialty training, the results highlight the importance of including clinical rotations where physicians are exposed to hospice services. For hospice agencies, employing nurses with experience caring for children and providing services for non–English-speaking families appear to be important steps toward decreasing barriers to serving children. Further research on the perspectives of parents, general pediatricians, and pediatric subspecialists on hospice care for children would be helpful in further delineating barriers and developing interventions and policies to improve access to hospice care for children.
Footnotes
Acknowledgments
The authors are grateful to the members of the North Carolina Pediatric Palliative Care Coalition for their contributions to the development of the survey instrument and to the representatives of hospice agencies for participating in the study.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the North Carolina Children's Promise.