
Abstract
Nearly 90% of terminally ill patients who have used Oregon’s distinctive death with dignity law to receive a medication to end their lives are enrolled in hospice care programs. In 2009-2010, we conducted a study of the policies developed by Oregon hospices to address patient inquiries and requests for death with dignity. The study examined the stated hospice values and positions and identified the boundaries to participation drawn by the hospice programs to protect personal and programmatic integrity. The boundaries were drawn around 6 key caregiving considerations: (1) language regarding physician-assisted death (PAD); (2) informed decision making by patients; (3) collaboration with physicians; (4) provision of lethal medication; (5) assistance in the patient’s act of taking the medication; and (6) staff presence at the time of medication ingestion.
Case 1
A hospice nurse develops a professionally meaningful caring relationship with a cancer patient and her family over 3 months. The nurse is aware that her patient has requested a prescription from his attending physician to end his life under the Oregon Death with Dignity Statute. As this prospect approaches, the patient asks the nurse whether she will be present when the patient takes the medication (the law requires the patient to self-administer the medication). The nurse has a professional but deep commitment to this patient and has expressed how meaningful it has been to be a “companion on the journey” of her patient.
In contemplating the patient’s request for her presence, however, the nurse is cognizant of the written policy statement of her hospice regarding staff participation in requests for “death with dignity.” One feature of this policy prohibits any hospice staff or volunteer from attending the dying of a patient using the law. This prohibition encompasses not only attending the dying of the patient at the time of patient self-administration of the medication but also the duration between self-administration and the time of death.
The nurse is conscientiously committed to the purposes of hospice care, but experiences conflict over how she can balance devoted caring to her patient, fidelity to core hospice values of nonabandonment, and loyal support of her hospice program.
Overview
According to the data collected by the Oregon Department of Human Services (ODHS), 88.7% of terminally ill patients who have used the state’s Death with Dignity law 1 to end their life from 1998 through 2010 have been enrolled in hospice care. This figure climbs to over 93% in the 3 most recent years (2008-2010) of available data. 2
At first glance, these figures seem perplexing. Hospices are committed to offer the highest quality of care at the end of life to ensure responsible and appropriate symptom management and to provide caring companionship on a person’s final life “journey.” Given these commitments, it might then be thought that hospice care would address the physical, emotional, relational, and even existential concerns that terminally ill patients face and diminish the frequency or nature of requests for a hastened death. Indeed, some hospices in Oregon contend that hospice care will make patient recourse to a death with dignity procedure through physician-prescribed medication “unnecessary.”
In point of fact, of any end-of-life caregiving venue, patients in hospice care in the state of Oregon are the recipients of high-quality hospice and palliative care. Patients enrolled in hospice do not exercise the legal right granted by Oregon to choose death with dignity due to an inability to obtain good hospice care and symptom management. Instead, what appears to account for the high levels of death with dignity patients enrolled in hospice is that hospice programs are rightfully perceived as an important societal mechanism to assure responsible practice of a hastened death through physician prescriptions. 3 Indeed, the most prominent patient right’s advocacy organization, Compassion & Choices of Oregon has since its inception made referrals to hospice a primary feature of its patient care counseling. 4
Previous studies have indicated general support, with some opposition, for patient’s rights under the law among hospice social workers and hospice nurses. 5 To assess the extent of participation of Oregon hospice programs in the state’s Death with Dignity Act, during 2009-2010 we contacted 65 hospice programs affiliated with the Oregon Hospice Association (OHA) and requested policy statements, program guidelines, and staff education materials developed by these programs to address patient inquiries about the Death with Dignity Act. We received documents representing the policies or educational materials from 56 of the 65 programs.
Our analysis of these documents, supplemented by site visits to 2 hospices and conversations with hospice staff at these hospices about problematic cases they have experienced, suggests individual hospice programs generally understand themselves to assume a minor role in the decision-making process of patients who exercise their legal rights under Oregon law. Moreover, Oregon hospice programs commonly draw boundaries and set limits to their participation and the participation of staff members, especially with respect to (a) providing information to the patient, (b) notifying the primary physician of the patient, (c) providing or assisting with the medications necessary to hasten a patient’s death, and (d), as illustrated by case 1, permitting the presence of staff members at ingestion or death. The ambivalence presented by hospice programs in their documents may be attributable to concerns about protecting the integrity and conscience of the organization or staff members, to issues of legal compliance and liability, and to complicity with a medical process that remains morally and professionally controversial in end-of-life care. 6 In general, hospice programs want to avoid any level of participation that transforms physician-assisted death (PAD) into hospice-assisted death. This article explores these questions of boundary drawing in the context of the information we gleaned through the documents we collected and case study conversations in our site visits.
Context and Background
The Oregon Death with Dignity Act was approved by Oregon voters in November 1994, and following several legal appeals, was finally approved for implementation in October 1997. The law’s most essential feature permits physicians to “writ[e] a prescription for medication to enable a qualified patient to end his or her life in a humane and dignified manner.” 1 The law also stipulates compilation of information about frequency, patient rationale, and safety of the law by the ODHS, which has published annual reports about the usage of the law each year from 1998 to 2010.
According to the most recent annual report, during the 13 years of the law’s authorization, 821 terminally ill persons have received a life-ending prescription from physicians, and 525 persons have used the prescription to end their life. As previously noted, 454 of the persons who have taken the medication have been enrolled in hospice care programs, with 58 patients not enrolled in hospice; the ODHS report considers this ratio to constitute 88.7% hospice enrollment, as the venue of end-of-life care is “unknown” for 13 patients. 2
After some initial reluctance during the early 1990s on the part of the OHA to embrace the death with dignity framework as a legitimate option for terminally ill patients 7 —attributable in part to concerns about organizational fragmentation as well as avoiding reinforcing negative public perceptions about hospice as “the place to die”—the OHA has subsequently become an advocate of patient rights in the method of dying. The OHA educates its professional and patient constituencies that hospice and palliative care programs are “uniquely qualified to address the needs of the dying,” and that terminally ill patients need not feel compelled “to choose between hospice and physician aid-in-dying.” Moreover, the OHA contends that it is supportive of patient choice, and that “a hospice should never deny a person its services because he or she has asked a doctor for a prescription, even when the hospice intends to exercise its right to not be involved.” 8 A similar perspective of ensuring customary care was presented in 2007 in a policy statement on Physician-Assisted Death by the Board of Directors, American Academy of Hospice and Palliative Medicine (AAHPM), “… neither a person requesting PAD nor his family should be deprived of any other measure of ongoing palliative care during the dying process and period of bereavement.” 6 Yet, as illustrated by our beginning case and by our subsequent analysis of the policy documents of individual hospice programs, what hospices are permitted to do and required to avoid are very complex questions of organizational integrity, mission, and values.
Indeed, the very phrasing of the OHA aspiration that a hospice program should not deny services places individual hospices in an organizational and ethical bind. One provision of the statute (ORS 127.885.s4 01) states there is “no legal requirement to participate” in the law on the part of any health care provider or facility. Individual hospice programs that have opted out of participation confront a caregiving issue of whether it will still be able to provide the full array of its services to a patient who makes a request for death with dignity. Our analysis reveals that the vast majority of Oregon hospice programs set programmatic, professional, and moral boundaries to their involvement in deaths attributable to patient requests for death with dignity. This raises an underlying question of whether Oregon hospice programs treat deaths attributable to physician-prescribed medications differently than other deaths that they attend. In this essay, we will use the language of PAD to refer to this practice, following our personal preferences as well as the nomenclature adopted by the AAHPM.
Hospice Values and Positions
The documents we received from Oregon hospice programs generally (with some variation) were comprised of 3 sections: (1) A prefatory statement about the philosophy and mission of hospice care and the formative values of caregiving; (2) A policy statement about the position of the individual hospice on its role in participation or nonparticipation in the Oregon statute, including permissions or prohibitions for hospice staff (as in case 1); (3) A detailed outline of the caregiving process the hospice and staff would undertake upon receiving an inquiry or request from a patient regarding PAD. Using these statements of hospice philosophy and mission, hospice policy, and hospice caregiving processes as our basis, we then analyzed individual documents as well as the entire body of 56 documents for comprehensiveness, consistency, coherence, and clarity.
Philosophically, the policies and guidelines of Oregon hospices on PAD attempt to be faithful to the historically formative values of hospice care, including the philosophy that death is a natural continuation of the human life span, affirming the dignity of each dying patient, promoting the quality of a patient’s remaining life through the highest level of caring commitment, and a distinctive devotion to symptom and pain management. 9 –11
These constitutive values tend to apply broadly to both nonreligious hospice programs (n = 47) and hospices with religious affiliations (n = 9). Figure 1 presents the most commonly articulated values as self-reported by individual hospices in their PAD policies.
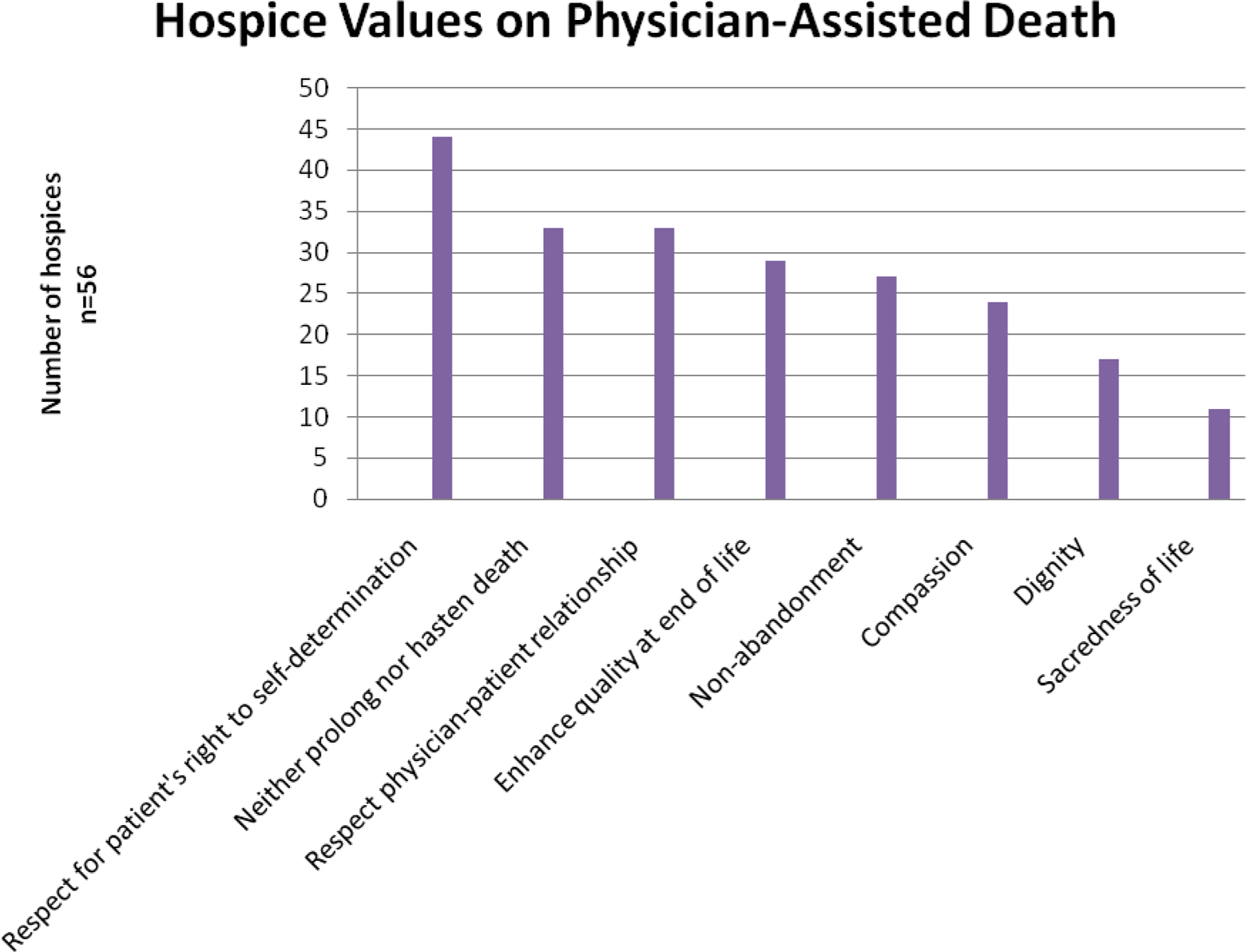
Hospice values on physician-assisted death.
Taking these values as they stand, participating in patient requests for PAD can be an organizationally vexing challenge for hospice programs simply because of some inherent tensions in these core values. These challenges include:
reconciling the historical hospice commitment to not hasten death with patient requests for physician assistance for medication to hasten death;
reconciling the hospice commitment to nonabandonment of patients and their families with the general posture of hospice noninvolvement with medication or assistance regarding the act of medication ingestion; and
reconciling the commitment to respect the integrity of the physician–patient relationship for patients who request death with dignity with the interdisciplinary and holistic mode of hospice care that involves nurses, social workers, spiritual care counselors, and others.
While the foundational values of hospice provide directions for caregiving, they do not readily generate resolutions to these 3 challenges. Hospice programs must necessarily live with some level of perplexity and conflict, given that it does not seem possible for a program to fulfill all these core values in circumstances when a hospice patient makes a request for PAD.
This perplexity underlies the diversity of Oregon hospices in their statements of policy or programmatic positions on participation. In their policy statements, hospice programs seek to balance the values core to their programmatic mission with issues of legal responsibility while also refraining from transforming physician assistance in a patient’s death into a hospice-assisted death.
Figure 2 displays 8 different ways that Oregon hospices self-reported their programmatic positions on participation with the Oregon law on death with dignity.
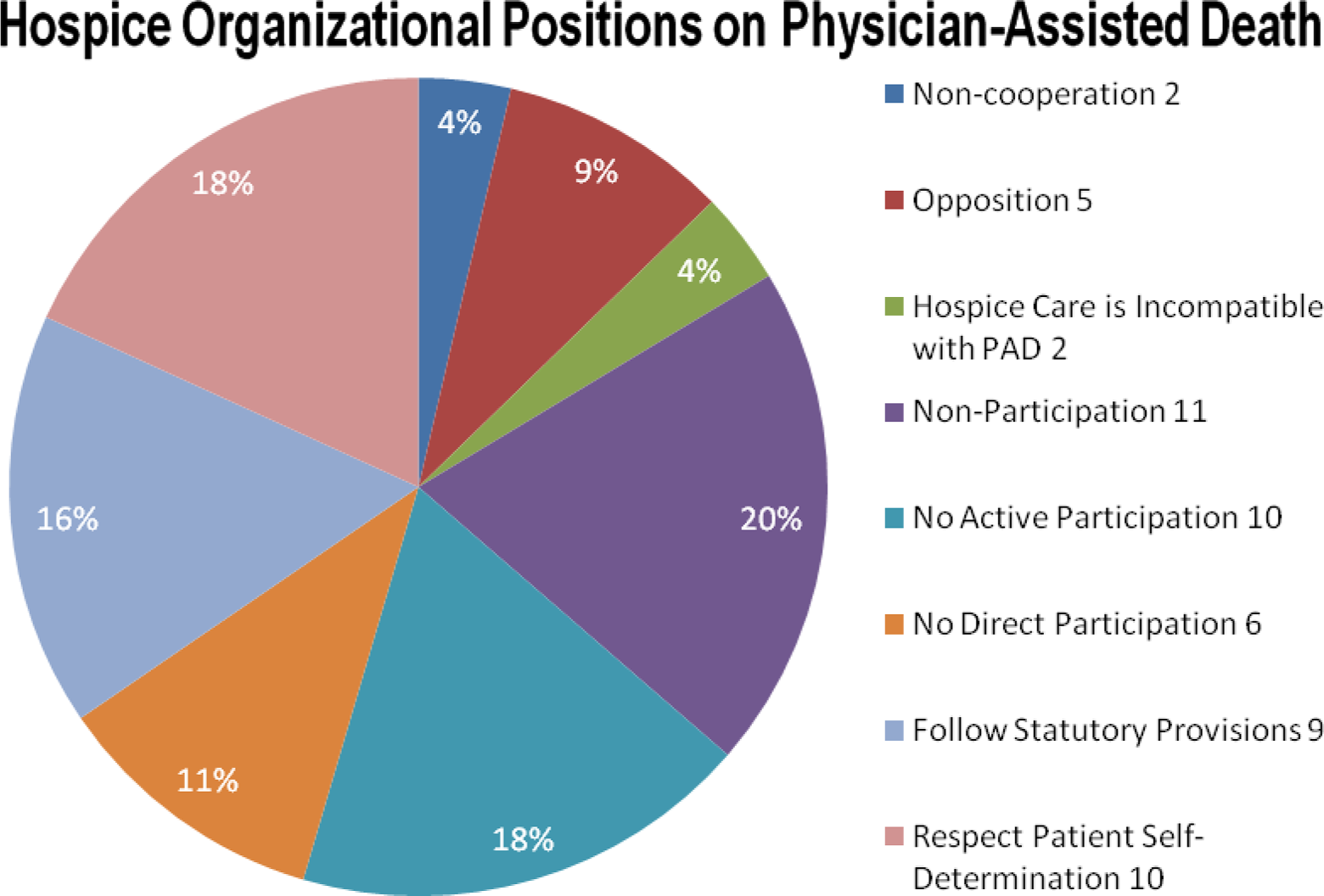
Hospice organizational positions on physician-assisted death. The number 55 in Figures 2-5 reflect that 1 hospice is currently writing their policy and no information is available for those aspects of analysis
For the most part, those hospices who affirm positions of opposition, noncooperation or that PAD, whatever be its legal status in society, is not compatible with values of hospice care have an affiliation with a religious tradition of caregiving. For a second cluster of programs, it is not clear whether there is any meaningful moral and practical difference between hospice positions that indicate “no participation” from those that proscribe “direct” or “active” participation, although the latter phrasing leaves open the possibility for some form of indirect or passive participation. A third cluster of programs indicate compatibility with participation to the extent permitted by law, including (for some) giving stated policy priority to respecting informed decisions of the patient. Prioritizing one value is one method of reconciling the tensions identified above. Interestingly, no Oregon hospice used the language adopted by the AAHPM - that of “studied neutrality.”
What can explain this rather remarkable diversity of positions among Oregon hospices relative to participation? From our analysis, we do not believe this diversity is explicable only through explicit statements of values or fidelity to common hospice philosophy but also manifests divergence regarding the third level of hospice discourse on PAD, the process of embedded caregiving practices.
Boundaries of Hospice Care
The policies of all Oregon hospice programs promise “standard hospice services” to all patients, regardless of a patient’s intent or request regarding PAD. In that manner, individual hospice programs seem to comply with the OHA stipulation that services should not be denied to hospice patients because they have requested a prescription to hasten their death. However, our analysis of why Oregon hospices present 8 general programmatic positions on their participation reveals differences concerning the concept of a “hospice service,” and in particular, over 6 principal caregiving considerations. Rephrased in question form, the policies and caregiving processes of hospice programs manifest differences regarding the following matters:
Does the hospice program understand the process to concern death with dignity, or PAD, or “physician-assisted suicide”?
What is the policy of the hospice concerning responses to patient inquiries? What information is disclosed, how, and by whom?
What is the nature of the hospice’s interaction with the patient’s attending physician?
What role will the hospice program play in securing or administering the medication or prescription for the patient?
Will the hospice program permit hospice staff to be present when the patient ingests the medication?
What responsibilities do hospice staff have in the event of complications when a patient takes the medication?
In examining the different approaches to these caregiving considerations in the 55 Oregon hospice programs, we suggest the issue of PAD confronts hospice programs not only with the challenge of reconciling conflicts on constitutive values but perhaps more fundamentally to define the meaning, boundaries, and integrity of “hospice” and “hospice care.” We discuss each of these caregiving considerations in turn.
Language: dignity, suicide, or death
The terminology used to describe what occurs when a physician prescribes a lethal dose of medication for a terminally ill patient who subsequently self-administers the medication to hasten death has been a perennially divisive issue in Oregon. The law is entitled Death with Dignity as that language was found to be more palatable to voters. 12 However, others contend this misrepresents both the nature of the action and the role of professional caregivers. Hospice programs have not been immune from either this linguistic controversy or the normative value assessment embedded in the choice of terms. As illustrated by Figure 3, Oregon hospices have no uniform concept in their program policies; the majority retains the language of “assisted suicide,” while somewhat strikingly, none uses the language of the state association, “physician aid-in-dying.”
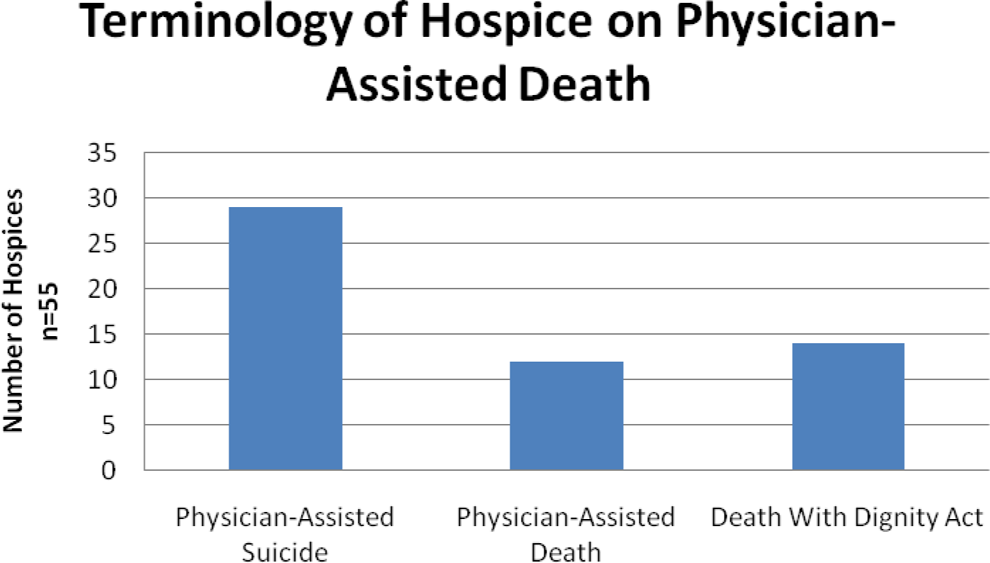
Terminology of hospice on physician-assisted death
All hospice programs that have opted not to participate in the Oregon law, as well as most that describe themselves as opposed to “active” or “direct” participation, use the language of physician-assisted suicide in their program policies. If a hospice frames the life-ending process through the concept of “suicide,” then questions of participation become very problematic because the hospice would appear to be complicit in an act that the hospice movement has sought to avoid from its historical origins. 9 By contrast, hospice programs that use the language of PAD or death with dignity are generally more inclined to some degree of collaboration with both patients and physicians, even though, as indicated below, other boundaries may be drawn to ensure that the process remains one of physician-assisted death rather than hospice-assisted death. The relationship of language and program position is thus a context within which hospice programs manifest modes of hospice identity and integrity to their mission.
Patient and physician interactions
As illustrated by case 2, hospice staff, and hospice programs generally, can experience perplexity when a patient makes an inquiry about or request for PAD.
Case 2
A hospice program has a stated policy that it “does not actively participate” in Oregon’s death with dignity law because such participation would violate a long-standing hospice commitment to “not hasten death.” A patient enrolled in the hospice with a diagnosis of terminal cancer indicates in conversation with a trusted spiritual care counselor that he or she has questions about and interest in death with dignity. Given the hospice policy and the hospice commitment to quality care for all patients, the counselor considers what steps he or she may take with the information the patient has confided.
The question illuminated by this case is the meaning of “participation,” and especially what is considered “active” participation. As noted, the law stipulates that health care providers, including hospice, have no legal duty to participate, but ethically, should “participation” be understood to mean involvement in the specific act of medication ingestion that leads to hastened death, or does it have a broader meaning of involvement in the process that facilitates the action, such as communication with patients and physician notification?
In the documents that we have analyzed, some hospice programs with clear policies of nonparticipation do not provide information to patients, but instead request patients to respect their programmatic position. However, this approach to information disclosure remains the exception: most programs, at a minimum, provide information about the law and the qualifications stipulated by the law for patients to obtain medication. The provision of basic information is construed as integral to the hospice commitment to informed decision making by the patients. Some hospice programs endorse a more substantive dialogue, permitting appropriate staff to “explore” with the patient their interest in PAD. This “exploration” also provides a procedural safeguard to ensure that the patient’s request has not been fostered by inadequate hospice care. The content of what such an exploratory conversation might consist of is thoughtfully developed by the AAHPM in their “Position Statement” on PAD. 6
Nonetheless, issues of integrity to hospice mission emerge regarding information disclosure. Prior studies indicate that hospice social workers and nurses, rather than spiritual care advisers, are most frequently involved in information provision. 13 Second, numerous Oregon programs stipulate that staff members who engage in information provision (or other discussion) with patients about PAD requests must adhere to a posture of “neutrality.” The goal of staff discussion with patients is an informed choice by the patient in consultation with family members, according to the patient’s values, not those of hospice staff. Staff members are not to persuade nor dissuade patient choices about PAD. The idea of neutrality thus is the communication analogue to the hospice philosophical commitment that death is neither to be hastened nor to be postponed.
Physician notification and collaboration
Under the legal statute, it is entirely possible that the process by which a patient obtains information about and medication for PAD can bypass a hospice program altogether. Even apart from the 11.3% of patients who are not enrolled in hospice, some hospice patients prefer hospice noninvolvement as a matter of personal privacy. This reality in part underlies the view expressed in many hospice documents that the decision regarding PAD is “a matter between the patient and his or her physician.”
However, hospice programs may also participate in the process by encouraging contact with an attending physician or organization that provides education and counseling for patients. A substantial majority of hospice programs state a willingness to refer a patient who has made inquiries about the Oregon law to their attending physician. Furthermore, hospice programs that allow staff to have exploratory conversations with patients are, provided the rationale for a patient inquiry is not inadequate hospice care, also willing to refer a patient to education and advocacy organizations; the most common referral prospect is Compassion & Choices of Oregon.
Nonetheless, hospice programs limit their participation on physician notification and referral: Ultimately, the responsibility for coordinating a visit to a physician to pursue informed consent processes and to prescribe the medication is assumed by the patient. Nine hospice programs express the view that facilitating a patient–physician meeting or making a patient referral violates their policies. The remaining hospice programs are silent on this matter, which means there is no hospice with a stated policy that it will coordinate patient and attending physician discussion. While this boundary is consistent with the value of respecting the integrity of the physician–patient relationship, it also reflects a concern to ensure the process remains physician-assisted as contrasted with hospice-assisted.
Nonabandonment and presence
As illustrated by case 1, an evident challenge of integrity for hospice programs concerns allowing staff members to be present at the time of medication ingestion to provide support for the patient and/or for family members. There is no legal requirement that any person, including any health care provider, be in attendance when the patient takes the medication. State reporting indicates that during 2001-2010, a prescribing physician was in attendance in just over 20% of cases; another provider besides the prescribing physician was in attendance in 50% of the cases, and in approximately 3 (29.2%) of 10 cases, either no provider has been present or there is no knowledge as to who was present at ingestion. 2
During our site visit conversations, some hospice staff contended that the core value of nonabandonment means that hospice policy should not only permit staff members to be present upon request at ingestion but also make the presence of staff members mandatory for the hospice program (though the legal right of any staff member to not be present would be respected). Nonetheless, among the hospice programs represented in this analysis, very few have a policy allowing (not mandating) staff presence, while the majority of hospice programs, including all those self-designated as nonparticipating or noncooperating programs, have stated prohibitions against staff presence. This profile is illustrated in Figure 4.
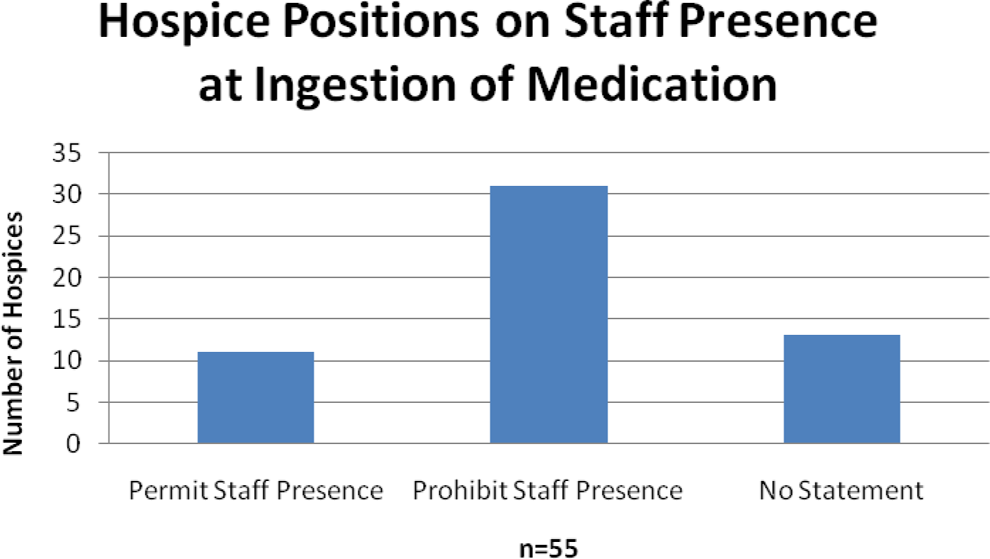
Hospice positions on staff presence at ingestion of medication
While the values of nonabandonment as well as respect for patient choice ground a case for hospice staff presence, it is not clear from programmatic statements of hospice philosophy or policy what particular value is so compromised by staff presence that it warrants the prohibition of presence. The presence of a staff member does not itself violate the commitment to not hasten death; nor does the prohibition of presence at patient ingestion mean the cessation of hospice care since virtually all hospices specifically indicate that they will provide postmortem bereavement support to the family of a patient with PAD, a form of care implicit in the promise of providing standard hospice services. Hospice staff would typically attend the death of any other patient if requested as part of customary hospice care. Hence, for hospice programs that do not permit staff presence in cases of PAD, the question is how this kind of death is morally and vocationally different than any other kind of death that hospice attends.
In our site visit conversations about perplexing scenarios and cases, 3 primary responses emerged from hospice staff about concerns with participation through staff presence at ingestion. First, hospice staff and program directors are concerned that presence can foster public perceptions that hospice encourages or endorses the PAD process, or even that the hospice program is responsible for ensuring that the patient’s death occurs without any complications. Hospice restrictions on presence are portrayed as maintaining organizational distance of hospice from direct participation, or at least avoiding a misleading perception that hospice condones PAD for its patients.
Second, some hospice nurses with whom conversation ensued over case 1 indicated that notwithstanding the policy of their hospice, they would attend the patient at their request, but as a friend, not as a hospice staff member. As one nurse commented, “I would go, but not be ‘on duty.’” Differentiating between roles as friend and roles as a hospice caregiver can provide a compromise whereby staff can maintain fidelity to both the patients and the hospice program.
Third, in approximately 1 of every 20 PAD deaths, a postingestion complication has occurred, primarily the regurgitation of the medicine by the patient. 2 Were a hospice care provider present in circumstances of complication, hospice staff claim they may feel compelled to intervene and provide, for example, antinausea medication, so that the patient’s dying would be free of further complications. However, in this scenario, the hospice staff member could plausibly be understood to have assisted or participated directly in the act bringing about death, thus violating a hospice prohibition on assistance, and potentially contravening the law. Thus, prohibiting presence at the time of medication ingestion avoids what could be organizational mission and legal compromise should patient assistance with medication be required.
We have thus far discussed 4 caregiving considerations hospices encounter in responding to patient requests about PAD—linguistic usage, information disclosure, physician referral, and staff presence at ingestion—about which there is divergence among Oregon hospice programs. These differences help explain the plurality of 8 organizational stances identified in Figure 2. Through these caregiving considerations, and the procedures that they entail, hospice programs define the boundaries of their participation with the Oregon law, and also their own sense of organizational mission and integrity.
Two caregiving considerations, by contrast, command close to universal consensus among hospice programs regardless of practices on the other 4 considerations. They are notable because they both concern involvement with the patient’s act of obtaining or ingesting medication, rather than the process required to receive a prescription, and they both demarcate boundaries of nonparticipation. We refer to the first consensus consideration as representing a prohibition on assistance regarding medications, while the second consensus consideration addresses the contingency of complications.
The Prohibition of Assistance
Virtually every hospice policy document, including those hospices who otherwise participate to some measure in the process, contains a statement that (with minimal variation) reads “Hospice X will not provide, pay for, deliver, administer or assist with medications intended for [PAD].” Hospice programs affirm restrictions on both the organization and staff on assistance with procuring medication the patient will use and on staff assistance with a patient’s act of self-administration of the medication.
We contend that for the majority of Oregon hospice programs the prohibition on assistance, while perhaps reflecting some moral sentiment grounded in the commitment not to hasten death, represents accommodation to legal and practical realities. Many hospice policies situate the prohibition on staff and programmatic assistance following prefatory statements acknowledging PAD as a legal end-of-life option for Oregon hospice patients and a choice ultimately determined within the relationship of patient and attending physician. Put another way, the hospice prohibition on assistance presumes the implementation of statutory provisions that effectively insulate hospice programs from the decision-making process. Furthermore, since by law the medication must be self-administered by the terminally ill patient, a sympathetic and compassionate hospice staff member cannot provide assistance in the death of his or her patient without taking the risk of violating legal statutes against assistance in suicide, mercy killing, active euthanasia, or homicide (ORS 127.880.s.3.14). The law also stipulates that it is the responsibility of the attending physician to either dispense the medication directly or, with patient consent, contact a pharmacist with a prescription that the pharmacist will dispense (ORS 127.815 s.3.01).
The prohibition on assistance is the most explicit and direct mode of hospice nonparticipation, but it is a boundary stipulated by law. By contrast, the 4 caregiving considerations discussed previously display choices individual programs make in the context of balancing patient requests, staff presence, and organizational mission and integrity. We concur that it is in the best interests of a patient with a terminal diagnosis to be enrolled in a hospice program rather than seek out PAD on their own; it is tragic that in a major national survey of physician attitudes and participation in patient requests for a lethal prescription, the researchers reported that “virtually all the patients died in the hospital.” 14 We contend the high quality of hospice and palliative care programs is a significant contributor to the relatively small number of patients who have used the Oregon law between 1998 and 2010. Still, while over 88% of the patients who exercise their legal right to PAD are enrolled in hospice care, it is important to note they most likely do not receive assistance from hospice programs in decision making, or in facilitating contacts with providers, or procuring or administering medications, and patients most likely will not have hospice staff members present when ingesting the medication. It cannot be inferred from extensive patient enrollment in hospice programs that hospice participation in the Oregon law is extensive and substantively meaningful.
The Contingency of Complications: Medicinal and Moral
As illustrated by case 3, circumstances of complications following patient ingestion of the medication generate challenges for hospice programs to find an appropriate balance between the core hospice commitment to quality care and the prohibition of assistance.
Case 3
A hospice nurse has received a request from her patient to be in attendance when she takes a lethal prescription to end her life as permitted by the death with dignity law. The nurse and patient have formed a meaningful bond with each other, and the nurse is inclined to accept the patient’s request. In consulting the policy of her hospice program, she finds that her program permits her to be present when her patient ingests the medication and to provide standard hospice care for the patient and the family through the period until death occurs. Upon ingestion of the medication, the patient experiences complications and regurgitates the medication. The hospice nurse now wonders what modes of assistance she can provide to help alleviate the patient’s distress.
As noted previously, complications have been reported in nearly 5% of the cases. Irrespective of whether a hospice permits their staff members to be present at ingestion, several hospices have developed policies about both what acts are permitted and what acts are to be avoided by staff in circumstances when medical complications follow patient ingestion. Such direction is important whether a staff member is in the course of making a routine visit to a patient or is contacted by a patient or family member, or is already present at ingestion.
Hospice policies that address this contingency reaffirm the core commitment of hospice philosophy: the responsibility of the staff member in such circumstances is to render “appropriate quality hospice care.” This includes attending specifically to “human needs” regarding the comfort and safety of the patient, including addressing bowel and bladder care, nausea, or spiritual care. The conception of human needs, however, provides the limit to hospice staff involvement and invokes the prohibition of assistance. Hospice staff will care for “human” needs that apply to all hospice patients for comfort and safety even in circumstances of medical complications from ingestion, as contrasted with “medical” needs that pertain to the PAD request specific to the patient. Such medical needs are considered the domain of the prescribing physician, not hospice staff. Boundaries of integrity for staff are established by distinguishing “hospice care” from “medical assistance” in the dying process, thereby reiterating the moral differentiation between hospice-assisted death and PAD.
It can also be claimed that, insofar as hospice programs generally acknowledge that the relationship between patient and attending physician is the primary context for negotiating the PAD process, hospice programs understand that it is ultimately the responsibility of the primary health care professional to attend the ingestion and death. The difficulty is that if just over 20% of PAD deaths have been attended by the primary physician, this is not a responsibility participating physicians have accepted.
Conclusion
The passage of state laws permitting PAD and the demographic fact that most patients who use such laws are enrolled in hospice has necessitated reflection by hospice programs on identity and mission, values, statements of policy, and practical caregiving processes. Physician-assisted death becomes a crucible through which the boundaries of hospice and hospice care are forged, tested, and evolved. Though Oregon hospice programs share a prohibition on assistance in PAD, they diverge with respect to (a) the language they use to describe such actions; (b) the amount of information about PAD they disclose, by whom, and in what manner; (c) the degree of deference to physician involvement; and (d) the modes of presence of hospice staff at the time of medication ingestion.
We recognize certain limitations in our analysis. First, although we received responses from a geographically diverse cluster of hospice programs, including hospices in metropolitan areas where the frequency of PAD is significantly higher than in rural areas, we did not receive requested materials from all Oregon hospices. Second, apart from our site visits and explicit statements in documents primarily from religiously affiliated hospices, it is unclear in many instances what process a particular hospice engaged in to formulate its policy document. Third, as indicated by comparative scholarship of ethical codes, 15 we acknowledge that what is stated in policy and what happens in practice can be 2 quite different things. Practice can differ from policy because the documents are not used extensively in training of staff, or because no policy can be sufficiently comprehensive for all practical questions staff face in handling patient requests for PAD.
We find it significant that the positions and practices of hospice programs do not follow necessarily from their philosophy of care. While the values important to hospice care are named in the hospice documents, the correlation between the values important to the organization and the policies and procedures they follow is seldom direct. Core values (eg, nonabandonment, neither hasten nor postpone death) are necessarily in tension and do not lend themselves to a clear consensual conclusion for hospice providers. The explanation may be that hospice policies on PAD are a more telling reflection of concerns regarding legal compliance for hospice than of a philosophy of hospice care. It is thus important to acknowledge the dissonance between philosophy, policy, and practice. As hospice programs in Oregon, Washington, and other states (eg, Montana, Vermont) as well as national programs encounter the challenges to organizational mission and staff integrity we have identified in this analysis, each of these limitations suggests directions for further research and study. Promoting the caring context for a dying patient to experience a dignified death is a distinctive and meaningful commitment of hospice, and ensuring high-quality hospice care to all patients seems to diminish the frequency of requests for PAD, permitting hospice programs to manifest fidelity to constitutive values and caregiving practices.
Footnotes
This study was presented at the Colorado Healthcare Ethics Forum 2011 Conference, May 5, 2011; and at the Oregon Hospice Association Annual Conference, October 15, 2010.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.