
Abstract
Although most patients with terminal heart failure (HF) prefer to die at home, the majority die in hospitals. To determine the impact of home inotropic support in the place of death among patients with terminal HF, this retrospective study compared the place of death in patients with terminal HF enrolled in an inotropic infusion program to place of death in a national sample of patients with HF. The rate of home death among program participants (64.5%; n = 217) was significantly higher (P < .001) than an age- and sex-adjusted rate of home death in a national sample (35.9%; n = 56 596). Patients with HF participating in home inotropic support can remain at home during the final stage of life and are less likely to die in hospitals.
Introduction
Heart failure (HF) was estimated to contribute to 11% of deaths in the United States in 2007. 1 Although treatment and management of HF have improved survival, half of the patients will die within 5 years of diagnosis. 1 Of every 6 patients with HF, 5 will be hospitalized; 2 of 5 will be hospitalized more than 4 times. 2 Heart failure (HF) causes more than 6.5 million days in the hospital in the United States each year 3 and accounts for 4% of all Medicare discharges. 4 Repeated admissions contribute substantially to the hospitalization rate, with up to half of the patients with HF having to be readmitted within 6 months of their initial visit. 5 Furthermore, a recent study found that more than 3 in 5 patients with HF are hospitalized within 30 days before death. 6 These high rates of hospital utilization translate into high costs. In fact, reimbursement for HF discharges accounts for 3.79% of all Medicare program payments. 4 In 2010, the total direct and indirect cost of HF in the United States was estimated at $39.2 billion. 7
Patients with terminal HF usually die in medical facilities. 6 ,8,9 However, patients who die at home often have a better quality of life during their final days than those who die in an intensive care unit or hospital. 10 While patient preferences may change over time as health status changes, research has shown that most patients remain favorably inclined to dying at home or in a hospice rather than in a medical facilities. 11 Preferences 12,13 for place of death vary across studies, with figures for home as the preferred place of death ranging from 43% to 94%. Paradoxically, national statistics show that between 1999 and 2007 only 22% of all deaths from HF occurred in a home or hospice setting. 4 Although not specific to HF, Gruneir and colleagues confirmed in a systematic review of the literature that “despite documented preferences for home death, the majority of deaths from terminal illness occurs in hospital.” 14
Other factors that influence the preference for place of death include local health care characteristics. Pritchard et al 15 analyzed data from 1992 and 1993 from the Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment (SUPPORT) as well as Medicare databases and found that while most patients expressed a preference for dying at home, the majority actually died in a hospital. Moreover, the likelihood of dying in a hospital was unrelated to patient preferences. Pritchard et al concluded that “whether people die in hospital or not is powerfully influenced by characteristics of the local health system, but not by patient preferences or other patient characteristics.” 15 Therefore, health systems can help patients with terminal HF fulfill their desire to die at home by providing programs that can prevent the need for readmission.
The American College of Cardiology/American Heart Association (ACC/AHA) Guideline addresses continuous inotropic therapy as “part of an overall plan to allow the patient to die with comfort at home.” 3 Inotropic infusion therapy can be provided in an outpatient setting. Inotropic infusion can be given continuously (ie, 24 hours/d) or intermittently (ie, less than 24 hours/d); however, this study focused on the use of continuous inotropic infusion. 16 Because dependence on inotropic therapy has been associated with increased mortality rates, continuous inotropic therapy is not meant to be curative and is not recommended for nonterminal patients unless as a bridge to heart transplant. 3 However, well-managed inotropic therapy can be a tool to prevent symptom exacerbation requiring readmission in terminal patients. 10 Therefore, the ACC/AHA clinical standard of care guidelines specify that patients who are on a transplant waiting list or approaching end of life would qualify for continuous inotropic infusion. 3 Per Medicare criteria, candidates must be end-stage HF and fully maximized on standard therapy to qualify for reimbursement.
Optimal continuous inotropic infusion at home requires special handling, administration, and patient support. An inotropic infusion support program strives to decrease exacerbations, emergency room visits, and hospital admissions through patient education, frequent assessments, and telephone contact, in order to detect adverse changes in health status. This type of integrated and comprehensive care allows patients to remain at home with an enhanced quality of life. While these programs include patients who have various treatment goals, only end-of-life patients are addressed in this article. For patients who qualify, continuous inotropic therapy combined with a patient support program offers them the opportunity to manage their condition, until the time of death, in the comfort of their own home. Thus, the purpose of this study was to assess whether patients with terminal HF who are provided with continuous inotropic infusion and related support are more likely to die at home than are patients receiving usual medical care.
Methods
Overview
A quasi-experimental, nonequivalent group design was used to assess the place of death among patients with terminal HF enrolled in the Walgreens Inotropic Infusion Program (WIIP) and compare the rate of home death for this intervention with a national sample. The study group included patients with terminal HF that were enrolled in a home inotropic infusion program. To provide a comparison to represent the typical rate of home death (ie, usual care), aggregate national data from death certificates were used. The following section describes the intervention, group selection criteria, and the analysis plan.
Description of the Intervention
Patients were supported by a network of specialty infusion pharmacies that provide education, care coordination, and infusion therapy at lower cost settings, usually at home. Patients were taught to self-administer infusion medications, operate infusion pumps, and detect signs and symptoms of infections or side effects. Support involved specially trained nurses, clinical pharmacists, technicians, and credentialed infusion nurses as resources.
The Home Inotropic Infusion Program included 7 components: patient teaching initiated in hospital; transition to home infusion pump and medications prior to discharge; home nursing visits as needed; clinical staff training specific to managing inotropic therapy patients; clinical pathways for nursing and pharmacy; follow-up assessment scripts and algorithms to detect changes in health status; and collaboration with managing HF specialist
Patients were given various educational tools such as a patient education booklet, self-monitoring tools and logs, and a reminder magnet of warning signs and symptoms to report. Additionally, each participant was given a program admission kit containing an automated blood pressure monitor, a scale, a thermometer, a tape measure, a graduated cylinder, and a pill organizer.
Selection Criteria
Intervention group
To enter the program, patients were identified by their managing cardiologist who ordered outpatient therapy and initiated a referral to a home infusion pharmacy. Patients in the WIIP program are receiving therapy either as “bridge to transplant” or as “bridge to end of life”; this study focused on the latter. Therefore, additional inclusion criteria were applied, whereby patients who (a) did not qualify for transplant, (b) chose not to pursue transplant, or (c) chose not to receive a ventricular-assist device (VAD) were included in the analysis. Nurse assessment confirmed that this group of patients chose, as stated in the current guidelines, to “die with comfort at home.” 3 The study sample included 217 patients with terminal stage D HF who were enrolled in the inotropic infusion intervention between 2007 and 2009, had sufficient data, and met all inclusion criteria.
Comparison group
To compare the rate of home death in program participants, secondary data from the Centers for Disease Control and Prevention (CDC) were used. The most current publicly available data for place of death for the US population who died of HF were the 2007 National Center for Health Statistics Vital Statistics Cooperative Program. 17 The CDC data files 18 comprise aggregated state data from individual state registration offices. These data provide the location of death rates by age, gender, and cause of death as reported on the death certificate by funeral directors, physicians, and medical examiners. The data include information from all death certificates filed in the United States. The identification of HF as the primary or underlying cause of death was determined based on the CDC's definitions and reported in International Classification of Diseases, Tenth Revision (ICD-10). 17
In the national data, location of death was categorized into 1 of 8 categories: residence/decedent's home/hospice facility; nursing home/long-term care; inpatient hospital, clinic, or medical center; outpatient hospital, clinic, or medical center/admitted to emergency room; dead on arrival at hospital, clinic, or medical center; patient status, unknown hospital, clinic, or medical center; unknown, or; other.
Among HF deaths, only a small proportion of national records reported unknown (0.2%; n = 903) or other (3.8%, n = 19 491), so they were excluded from analysis.
Because WIIP rarely enrolls patients in nursing homes, deaths in nursing homes or long-term care (category 2) were excluded from analysis to be more comparable. After excluding this category, the comparison group yielded 56 596 patients with HF who died either in the home/hospice or in the hospital. All hospital, clinic, or medical center locations (categories 3-6) were aggregated to calculate the national estimate of HF deaths in hospital.
Analysis Plan
For both the intervention and comparison groups, the dependent variable was a dichotomous indicator—home/hospice versus hospital—of the physical location of death. The independent variable was a nonrandomized group as previously described. Covariates included age and sex. Because age at death was categorized by decade of life in the vital statistics data, the study sample was calculated to match. Compared to the intervention group, the comparison group were older (aged 70 and older = 89% vs 44%) and contained fewer men (38.8% vs 72.4%). These differences in age and sex varied significantly (P < .001) between the intervention and comparison groups (Table 1). To account for differences in age and sex distributions between the intervention group and comparison group, the national rate was age- and sex-adjusted using the direct standardization method as recommended by the World Health Organization. 19
Comparison of Demographics in Intervention Group and National Sample Before Standardization a
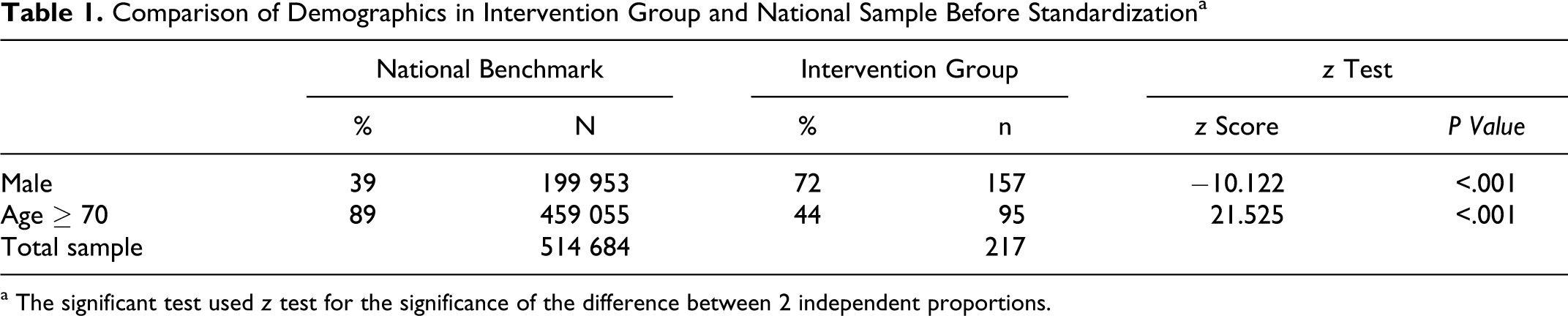
a The significant test used z test for the significance of the difference between 2 independent proportions.
The study focused primarily on descriptive statistics. All statistical analyses were performed with Microsoft Excel 2007 and SAS statistical software, version 9.2 (SAS Institute Inc, Cary, North Carolina). A z test was used to determine whether significance differences exist between the program and national distributions, and P values are reported assuming 2-tailed tests.
Results
In the unadjusted national data, patients with HF were more likely to die in the hospital (37.4%) or in a nursing home or long-term care facility (36.7%) than at home or in hospice (25.9%). After adjusting the national data to similar age and sex distributions as the intervention group, the proportion of death for patients in home (or hospice) and hospitals were 35.9% and 64.1%, respectively (N = 56 596). As shown in Table 2, patients with terminal HF in the WIIP program were more likely to die at home (64.5%, N = 217) than in patients in the national CDC sample of patients with HF. This difference was statistically significant (P < .001).
Place of Death Among Patients With Terminal HF in a Continuous Inotropic Infusion Therapy Program Compared to a National Sample (ie, Usual Care)
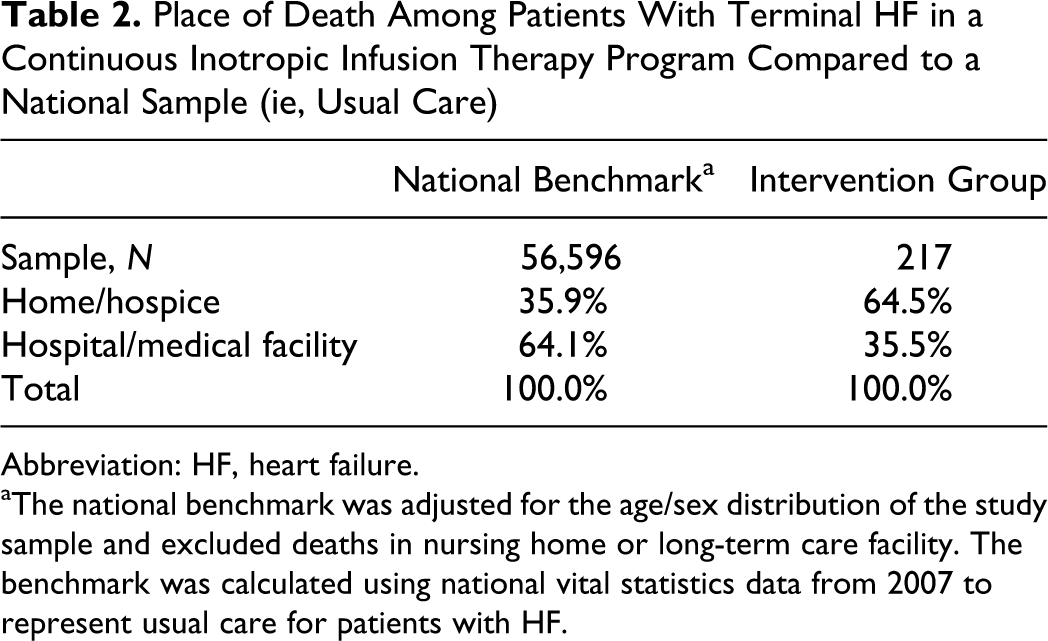
Abbreviation: HF, heart failure.
aThe national benchmark was adjusted for the age/sex distribution of the study sample and excluded deaths in nursing home or long-term care facility. The benchmark was calculated using national vital statistics data from 2007 to represent usual care for patients with HF.
Discussion
Evidence from the health literature revealed that the current paradigm of medical care is less than adequate in meeting the needs of terminally ill patients with HF 6 ,15 or reducing the cost of care at end of life. 8 ,9 The results from the current study propose that continuous inotropic infusion can be an effective palliative option for patients who would prefer to die at home rather than in a hospital or medical facility.
Like this study, Brumley et al 8 also found a higher rate of home death among patients enrolled in an interdisciplinary home-based palliative care program when compared to a usual care benchmark. Compared to this study, the rates of home death in both the invention group (71%, n = 220) and the usual care group (51%) were higher than reported in this study. Although beyond the analytical scope of the current study, Brumley et al used multivariate modeling to adjust for various other factors. In the adjusted model, patients in a palliative care program were twice as likely to die at home (odds ratio [OR] = 2.20, 95% confidence interval [CI] [51.3-3.7], P < .001) compared to patients in the usual care benchmark. This study also provided financial evidence supporting the provision of in-home palliative care for terminally ill patients with HF.
Using several secondary data sources including Medicare claims, Setoguchi and colleagues 6 reported that only 23% of patients with HF died in hospice, which is slightly lower than the unadjusted national benchmark and considerably lower than the current study's home/hospice rate. Moreover, the study demonstrated that hospice care was highly underutilized in patients with HF compared to patients with cancer (50.8%). In this Pennsylvania study, 60% of patients with HF were admitted to a nursing home before death. While the current study excluded nursing home deaths, an assumption from the literature was that the majority of patients would prefer to die at home rather than any medical facility, including nursing homes.
In a study of data from the Kaiser Permanente palliative care plan, Enguidanos et al 9 found that 87% of patients enrolled in an interdisciplinary home-based palliative care plan were more likely to die at home compared to 47% of patients in a comparison group. Both the treatment and control results are slightly higher than the results reported in this study (64.5% and 35.5%, respectively). As noted previously, the Kaiser results are consistent with the premise that health systems that are especially supportive of palliative care options would likely have a higher rate of home deaths. Furthermore, the Kaiser study found that treatment model reduced cost of care in the terminally ill patient cohort by 45% and increased patient satisfaction with care. 9 These findings imply that programs that can improve the likelihood of terminal patients being able to remain at home until death may also improve quality of life and decreased financial burden for patients with HF and their families.
Conclusion and Implications
Even though the expressed preference of most patients is to die at home, a majority of HF deaths occur in medical facilities. Despite the existence of hospice as a Medicare benefit for nearly 2 decades, home-based palliative care remains underutilized, especially by patients with HF. The results of our study connote that continuous inotropic therapy combined with a support program can help patients with terminal HF to remain within their homes, rather than a hospital, at end of life. Decisions surrounding end-of-life care are difficult for patients with HF and their families alike. Therefore, a patient-centric approach should focus on increasing and improving palliative care options to achieve patient's final wishes. Furthermore, treatment of terminal HF, either in a hospital or home setting, is resource intensive. When designing benefit plans and reimbursement strategies, policy makers should consider the ability of inotropic infusion programs to honor patients' wishes at end of life.
Limitations
There were several limitations in this study. First, this study design could not control for possible selection bias. Patients who were referred to the program were likely seeking end-of-life preparations at home, while the comparison group came from the general population. Second, the expected place-of-death rates were based on the available data that matched patients on age group and sex. It is highly likely there were other unmeasured characteristics that would influence the results. In particular, the CDC data did not indicate the stage of HF, while the intervention group comprised only patients with stage D HF. Furthermore, the benchmark rate could not exclude patients that may have been receiving inotropic infusion therapy. This study design did not allow for measurement of quality of life, patient satisfaction, or financial outcomes, which could have improved the evidence for program effectiveness. As a nonrandomized study, causation could not be inferred from the results. Finally, these results are based on the experience of one program, and it is unknown whether these findings can generalize to other inotropic interventions.
Footnotes
The authors of this manuscript are employed or contracted by Walgreens. Poster was presented at the 7th Annual Meeting of the American Association of Heart Failure Nurses (AAHFN), Seattle, June 23 to 25, 2011.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The program and related research were funded by Walgreens.