
Abstract
Reiki is a system of natural healing techniques administered by laying of hands and transferring energy from the Reiki practitioner to the recipient. We investigated the role of Reiki in the management of anxiety, pain and global wellness in cancer patients. Building on the results of a pilot project conducted between 2003 and 2005 by a volunteer association at our hospital, a wider, 3-year study was conducted at the same center. The volunteer Reiki practitioners received 2 years of theory and practical training. The study population was 118 patients (67 women and 51 men; mean age, 55 years) with cancer at any stage and receiving any kind of chemotherapy. Before each session, the nurses collected the patient's personal data and clinical history. Pain and anxiety were evaluated according to a numeric rating scale by the Reiki practitioners. Each session lasted about 30 min; pain and anxiety scores were recorded using a Visual Analog Scale (VAS), together with a description of the physical feelings the patients perceived during the session. All 118 patients received at least 1 Reiki treatment (total number, 238). In the subgroup of 22 patients who underwent the full cycle of 4 treatments, the mean VAS anxiety score decreased from 6.77 to 2.28 (P <.000001) and the mean VAS pain score from 4.4 to 2.32 (P = .091). Overall, the sessions were felt helpful in improving well-being, relaxation, pain relief, sleep quality and reducing anxiety. Offering Reiki therapy in hospitals could respond to patients' physical and emotional needs.
Introduction
Reiki is a system of natural healing techniques administered by laying of hands and transferring energy from the Reiki practitioner to the recipient. It claims to enhance the body’s natural ability to heal itself through the rebalancing of energy and thus restore physical, emotional, mental, and spiritual well-being.
Japanese master Dr Mikao Usui rediscovered the root system of Reiki in the early 1900s through his study of ancient Tibetan healing arts and the laying of hands healing tradition. Usui instructed Dr Chujiro Hayashi in the use of the technique, who then taught Hawayo Takato. She brought Reiki to Hawaii (and mainland United States) during the 1940s. Reiki was introduced to Europe in the 1980s.
Reiki is a Japanese word meaning universal life energy; it is composed of 2 syllables: rei, which means universal energy, the energy that permeates the entire universe, and ki, the life energy of all living creatures. The Reiki practitioner lays hands on or above the recipient’s body so that the universal life energy can flow naturally into the areas of the recipient’s body that need it most. Reiki can also be practiced as self-treatment (self-help). It is especially indicated in the helping professions, for people working in health or social services. It is also very helpful to prevent burnout, lack of motivation, and work-related stress in nurses.
The use of complementary alternative medicine in hospitals is attracting growing interest from health care providers working with patients with cancer. As Reiki requires no specific facilities, it can be practiced anytime and anywhere, making it particularly suitable for the hospital setting. Among relaxation techniques variously demonstrated to improve coping with cancer, Reiki has been shown to be an effective aid to alleviate pain and other symptoms such as anxiety, insomnia, and hyporexia, thus enhancing the quality of life in patients with advanced cancer. 1 In a pilot project conducted between 2003 and 2005 by the volunteer association Cerchiodiluce at the Medical Oncology Day Services Unit of the Hematology and Oncology Department, San Giovanni Battista Hospital, 27 patients (total of 94 treatments) reported experiencing improved sleep quality and relief of pain and anxiety. Building on this initial experience, a wider study involving a larger number of patients was conducted at the same center for cancer care.
With the present study, we investigated the role of Reiki in the management of anxiety, pain, and global wellness in patients with cancer with various stages of disease and attending a day oncology and infusion services unit. The study reports the results of a project presented and developed by the volunteer association, Cerchiodiluce, accompanying with Reiki, carried out in collaboration with the medical staff of the Medical Oncology Center, San Giovanni Battista Hospital.
Patients and Methods
Before being allowed to administer Reiki therapy in the hospital, the volunteer Reiki practitioners received 2 years of training: 1 year of internal workshops with the teaching staff of the Cerchiodiluce Association plus 1 year of in-hospital practice with skilled tutors.
Patients
In total, 118 patients gave their written informed consent to Reiki therapy after having received explanation about the technique from the hospital nurses and the Cerchiodiluce Association volunteers who administered the treatments.
The study population was composed of patients with cancer at any stage and receiving any kind of chemotherapy (CT). Reiki treatments were offered during hospitalization in day-hospital rooms. Before each session, the nurses collected the patient’s personal data and clinical history: site of primary tumor, date of diagnosis, site of metastasis, number of CT cycles, and performance status (PS) according to Eastern Cooperative Oncology Group (ECOG) scores. Pain and anxiety were evaluated according to a numeric rating scale by the Reiki practitioners.
Methods
Reiki sessions were offered to patients while in hospital for CT infusion. Patients were fully dressed, seated on a chair or lay on a bed during the treatment session. A maximum of 4 treatments were administered during 4 CT infusions. Each Reiki session lasted about 30 minutes, during which the practitioners held their hands above the patient or gently touched his or her body, from head to legs, focusing on the patient’s energy centers (chakra) and sites of pain or discomfort. Unlike some other alternative healing practices, Reiki does not involve the use of pressure, massage, rubbing, or instruments.
At the end of the treatment session, pain and anxiety scores using Visual Analog scale (VAS) were recorded together with a description of physical feelings the patients perceived during the session, such as warm/cold, relaxation/stress, well-being/discomfort, referring specific sites, if any.
Statistical Analysis
Data were entered into a dedicated access database and processed using Epi Info software and Windows 2000 for Statistics.
Results
Over the 3-year study period, Reiki therapy was administered to 118 patients: 67 (57%) women and 51 (43%) men (Table 1); mean age 55 (range, 33-77); 16 (14%) patients were receiving adjuvant CT, 56 (48%) first-line CT, 21 (18%) second-line CT, 3 (2%) third-line CT, 5 (4%) fourth-line CT, and 11 (9%) were off therapy; for 6 (5%) patients, these data were missing. Tumor site distribution was colon 15 (13%), breast 30 (25%), lung 21 (18%), stomach 12 (10%), head and neck 11 (9%), bladder and kidney 22 (19%), and other sites 7 (5%). Site of metastases was liver in 15 patients (13%), bone in 11 (9%), lung in 9 (8%), brain in 4 (3%), lymph glands in 7 (6%), and other sites in 10 (8%). The PS according to the ECOG score was 0 in 71 (60%) patients, 1 in 31 (26%), 2 in 10 (8%), 3 in 4 (3%), not evaluated in 2 (1%). All 118 patients underwent at least 1 session of Reiki therapy, 61 (48%) received 2, 37 (30%) received 3, and 22 (17%) received 4 treatments, for a total of 238 therapy sessions (Table 2).
Patient Characteristics
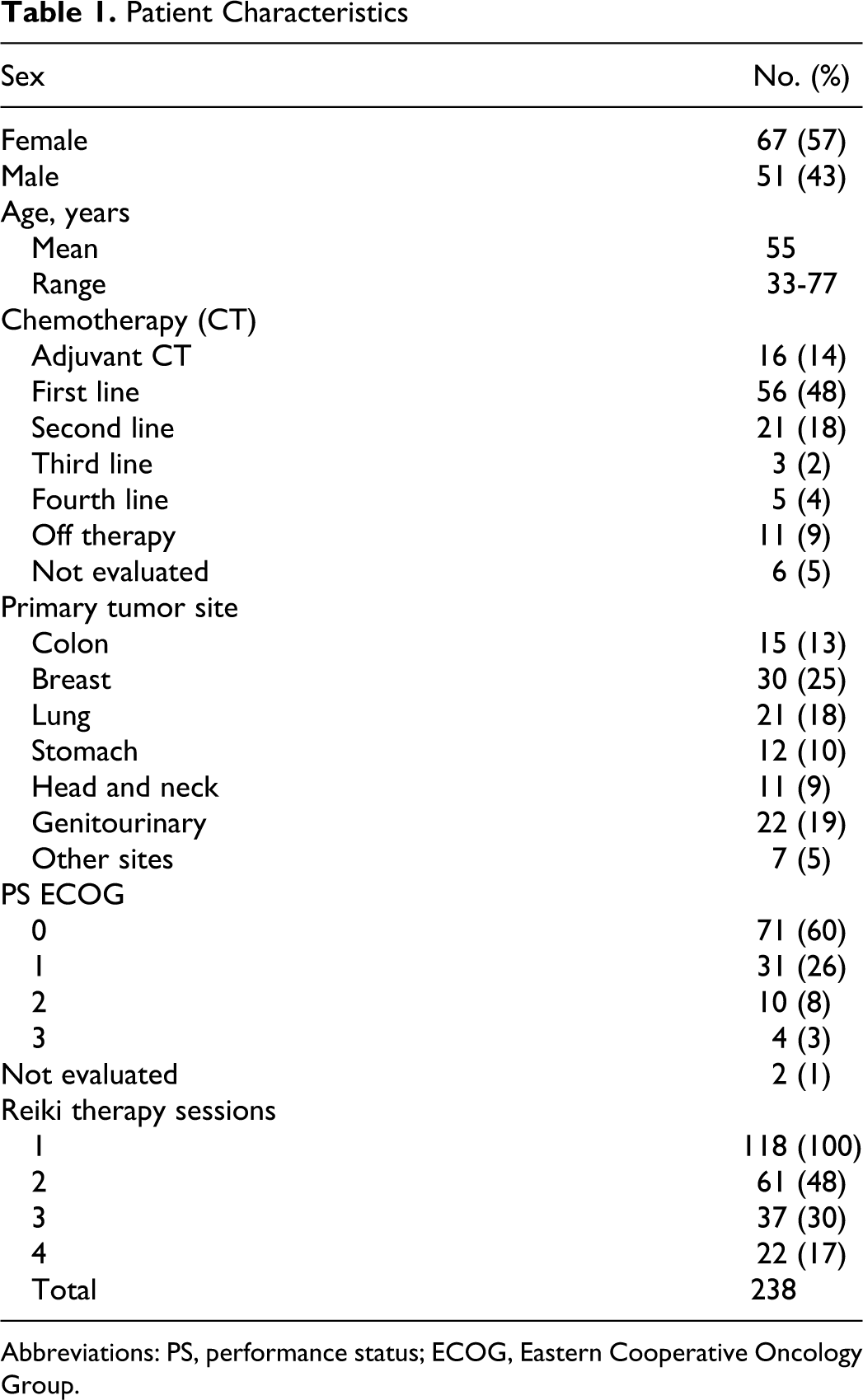
Abbreviations: PS, performance status; ECOG, Eastern Cooperative Oncology Group.
Anxiety Scores Before and After Each Reiki Therapy Session
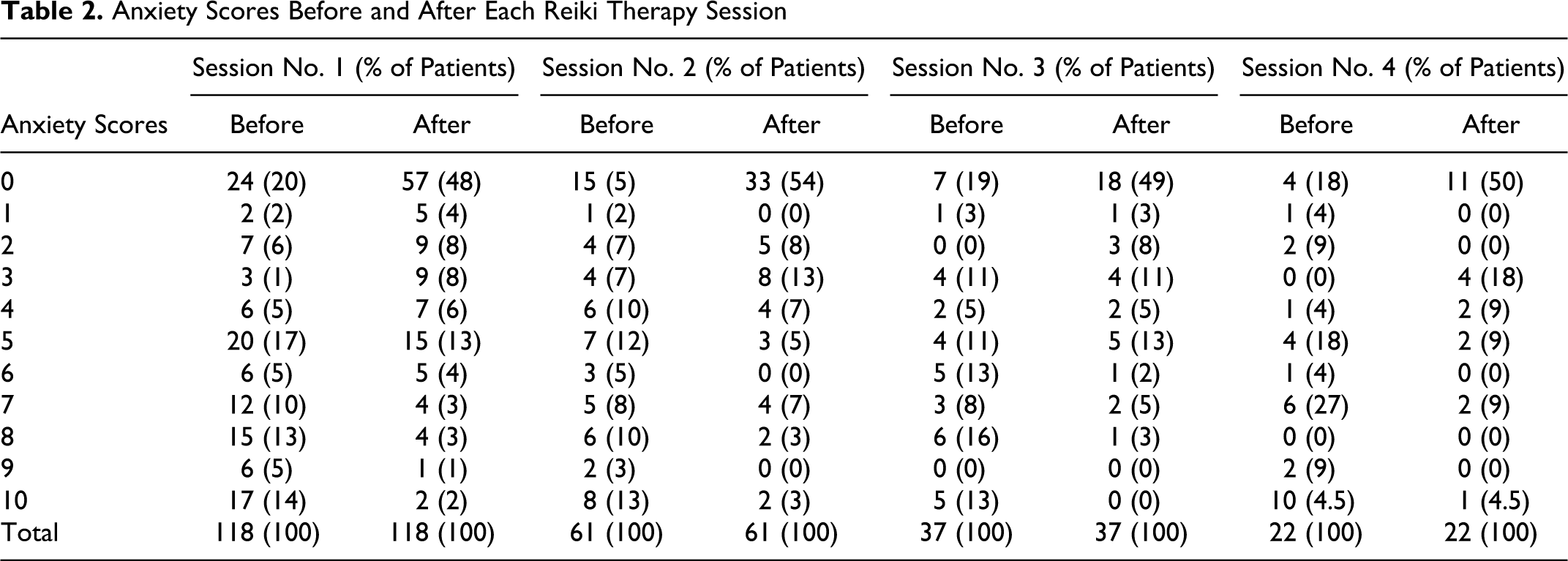
Anxiety was noted at baseline in 92 (78%) patients (mean VAS score, 6.3); 12 (10%) had received prior therapy to control anxiety; 45 (38%) patients had advanced stage disease and 47 (40%) early stage disease. A VAS score >5 for anxiety was recorded in 56 patients (47%) before and in 16 (14%) after the first treatment session; 19 (86%) patients were noted to have anxiety before and 3 (14%) after the fourth treatment session. Statistically significant changes in the mean anxiety scores before and after each treatment were observed (Table 3).
Mean Anxiety Scores Before and After Each Reiki Therapy Session a

a Plus-minus values are mean ± standard deviation.
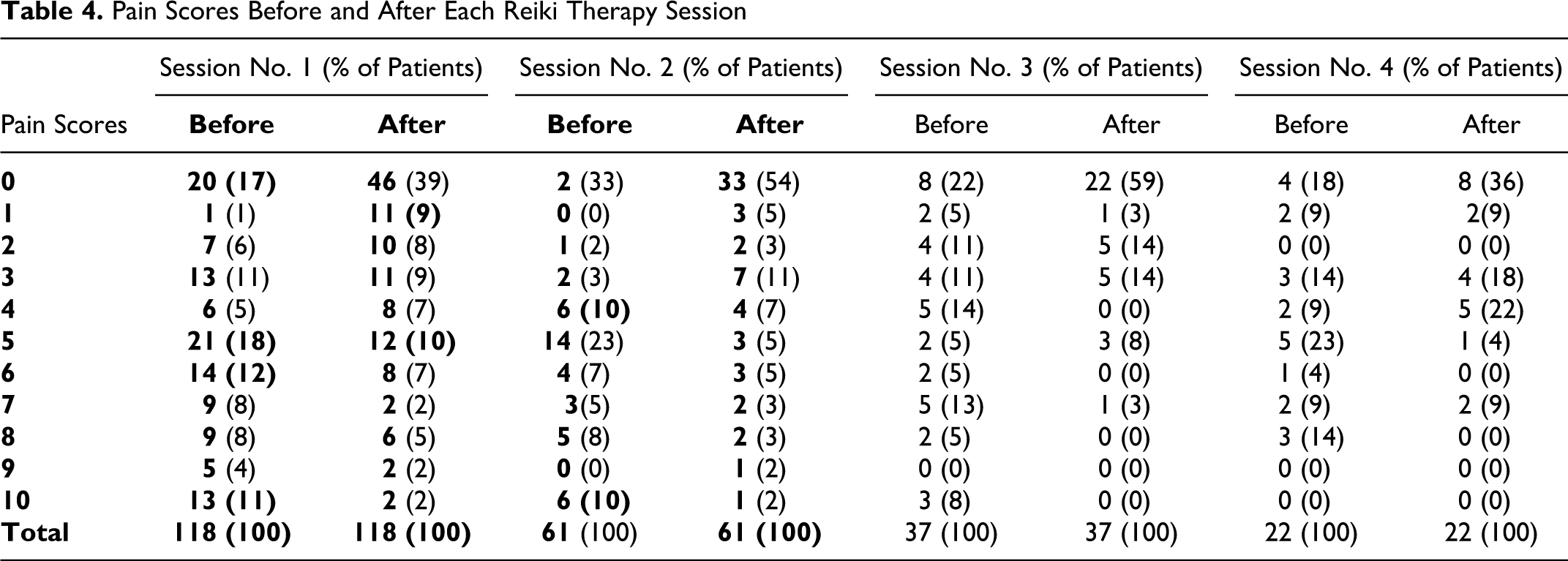
Pain was referred at the baseline interview with the Reiki practitioners by 98 (83%) patients (mean VAS score 3.7) and contrasted with the PS according to the ECOG scores recorded by the physicians. This discrepancy might have been due to the empathy between patients and Reiki practitioners that encourages more open communication of symptoms and emotions. Only 20 (17%) patients were pain free, 43 (37%) on pain therapy, and 75 (47%) not taking any drug in spite of having pain. The site of perceived pain was the same as the tumor site in 54 (46%) patients and different in 36 (31%). A VAS pain score >5 was reported by 50 (42%) patients before and by 20 (17%) after the first treatment session. Among the patients who had received 4 Reiki treatments, 6 (28%) recorded a VAS score >5 before the session (no one >8) and only 2 (9%) recorded a VAS score >5 (no one >7; Table 4). Changes were observed in the mean VAS pain scores before and after the first, second, and third Reiki treatment session (Table 5).
Pain Scores Before and After Each Reiki Therapy Session
Mean Pain Scores Before and After Each Reiki Therapy Session a

a Plus-minus values are mean ± standard deviation.
On further analysis of the subgroup of 22 patients who underwent the full cycle of 4 Reiki treatment sessions (Table 6), the mean VAS anxiety score decreased from 6.77 to 2.28 after 4 treatments, and this reduction was statistically significant (P < .000001); the mean VAS pain score decreased from 4.4 to 2.32 (P = .0191).
Mean Anxiety and Pain Scores at Baseline and After 4 Reiki Therapy Sessions a
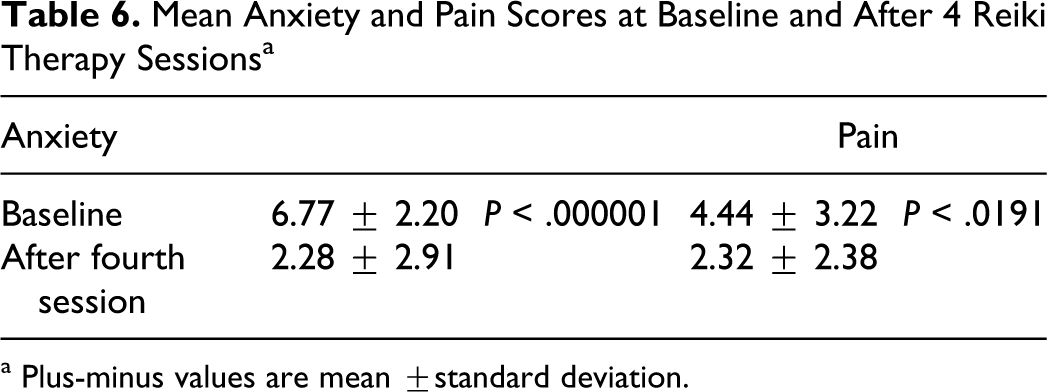
a Plus-minus values are mean ±standard deviation.
Feelings Perceived During Reiki Therapy Sessions
Finally, at the end of each treatment session, the patients were asked questions regarding their perception of warmth, cold, relaxation, stress, well-being, and discomfort. Overall, the sessions were considered helpful to improve well-being (70%), relaxation (88%), pain relief (45%), sleep quality (34%), and reduce anxiety (70%; Table 7).
Discussion
There are different protocols of research with Reiki treatments in hospitals all around the world. In some hospitals, touch therapies have become a nursing practice to foster wellness, reduce stress, and increase relaxation. 2 Previous observations on the use of Reiki have found that it can bring about deep relaxation and well-being and decrease the use of pain medications after surgery. 3 Reports have also described shorter hospital stays and increased patient satisfaction, as well as a reduction in nausea and emotional distress, improved communication, less anxiety, and lower systolic blood pressure. 2,4 In one study, spontaneous regression of human papilloma virus (HPV) infection was noted in 27% of patients in the control group versus 83% in the Reiki-treated group.
The effect of Reiki therapy on chronic pain remains controversial. Two studies found no significant benefit after Reiki treatment but one did. 5 –7 Sampling criteria, methods, small sample sizes, and varied questionnaire usage with potential response bias all limit the generalizability of findings for Reiki therapy as an adjunctive pain strategy. To date, few investigations have demonstrated rigorous research design with attention to protocol integrity. Some measurement data show a trend suggesting that Reiki therapy can aid in pain relief and wound healing 7 but the overall findings did not reach statistical significance.
To our knowledge, the present study is the first in which trained volunteers administered Reiki therapy and collected data in collaboration with hospital staff nurses and doctors. Moreover, our results are certainly of interest as regards the number of patients treated (118), treatments delivered (238), and length of the project (3 years).
In agreement with the literature, 8 our study demonstrates that Reiki therapy has no side effects and is highly appreciated by all patients; it can make the patient’s stay in hospital/day hospital more acceptable by turning normally stressful waiting time into an opportunity to obtain relaxation and well-being. The analysis of the quality of feelings perceived during treatment sessions shows that deep relaxation was achieved relatively rapidly (approximately 20-30 minutes), reducing anxiety and hence improving the relationship and communication between patients and operators.
Reiki seems to be a promising aid in anxiety control, with a marked reduction in the mean score after each treatment and a decrease of one third after 4 treatments. Pain control was also evident, with reduction of 50% in mean scores after each treatment, although the statistical significance between the first and the fourth treatment was admittedly modest. This might have been due to the ad hoc selection of a small subgroup of patients with the highest starting anxiety and pain scores and symptoms that were harder to treat with a conventional approach. Moreover, since about one third of patients were receiving conventional pain therapy, this may have constituted a confounding factor. Despite this limitation, our investigation indicates that pain as an outcome variable of Reiki therapy can be measured and further research using this parameter is warranted.
In light of these results, Reiki therapy may be considered a useful aid in the management of anxiety and pain during day-hospital stay for cancer care; furthermore, offering Reiki therapy in hospitals could provide a global approach to cancer patients, which responds to their physical and emotional needs within a holistic vision of care.
Footnotes
Acknowledgments
We wish to thank the volunteers from the Cerchiodiluce Association and the staff of the Hematology and Oncology Department, San Giovanni Battista Hospital, for their collaboration in the project.
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.