
Abstract
Investigations have shown that symptom prevalence varies according to the place of death. We sought to assess the symptom prevalence of chronically ill people in Germany and how this prevalence differs depending on the place of death. We sent questionnaires to 5000 bereaved people in Rhineland-Palatinate (Germany), whose relatives died between May 25 and August 24, 2008. In all, 3832 questionnaires were delivered and 1378 completed (response 36.0%). Most decedents had moderate-to-severe weakness (94.5%), fatigue (93.5%), need for help in daily activities (87.9%), and appetite loss (87.4%). Pain and dyspnea were most severe in hospitals; fatigue, confusion/disorientation, and problems with wound care in nursing homes; and need for help in daily activities and overburden of family at home. Associations persisted after adjusting for potential confounders.
Introduction
Examining and improving the process of dying have become major objectives in recent investigations of palliative care. Numerous investigations have shown that the symptom burden experienced by the dying and the overall assessment of the dying process by relatives vary widely according to the place of death. 1 Recent studies revealed evidence that dying at home or with hospice care is related to a more positive overall assessment of the dying process 2 –4 compared to death in a hospital or in a nursing home. 2,5 Other studies showed a higher symptom burden, especially higher proportions of pain and fatigue, and more social and emotional problems, in hospitalized patients compared to outpatients. 6,7
In Germany, some studies exist which examined symptoms of patients, mainly with cancer, hospitalized in palliative care units. 8,9 However, there are no data available focusing on symptom prevalence of dying people in different settings of care in one comprehensive study in Germany.
The following analyses are part of the so-called EPACS study (Research Accompanying the
Methods
Data Collection
The process of data collection has been previously described elsewhere in detail. 10 Briefly, the EPACS study was carried out in the form of a cross-sectional, written survey between September 2008 and January 2009. The base of the survey was a random sample of 5000 addresses of deceased inhabitants with principal residence in the German federal state of Rhineland-Palatinate (4 million inhabitants), who had died between May 25 and August 24, 2008. A standardized and anonymized questionnaire was sent out to the former address of the deceased, asking the bereaved to complete the questionnaire. Our study was approved by the ethical committee of the medical association of Rhineland-Palatinate.
Questionnaire
Our questionnaire gathered information on sociodemographic variables of the deceased and the respondents, symptom and social burden in the last 2 days of life, several disease-related variables, quality of in- and outpatient care, and (preferred) place of death.
Variable Construction
Symptom burden
The overall outcome variables in our analyses were 16 different symptoms from which the deceased suffered at the end of their life. These variables were assessed by asking the bereaved to judge the symptom and social burden of their deceased relative in the last 2 days of life. These items were derived from the Hospice and Palliative care Evaluation (HOPE), a standardized basic documentation tool, developed and evaluated by a multiprofessional working group since 1996, which has been used in several epidemiologic surveys in Germany. 11 The original aim of the HOPE documentation tool was to evaluate the symptom intensity of patients in palliative care settings. We adapted this tool to measure the symptom and social burden of the dying. For the subsequent analyses, we included the symptoms such as pain, nausea, vomiting, dyspnea, constipation, weakness, appetite loss, fatigue, problems with wound/decubitus care, depressiveness, anxiety, tension (emotional strain), confusion/disorientation, need for help in daily activities, problems with organization of care, and overburden of family. The bereaved could choose between “no (burden) at all,” “slight,” “moderate,” and “severe.” We afterward subsumed “no (burden) at all” and “slight,” as well as “moderate,” and “severe” into 1 item category, respectively.
Sociodemographic Variables
For our analyses, we included information on age, sex, marital status, nationality, and proxy type to describe the sociodemographic background of the deceased. Apart from proxy type, information on the aforementioned variables was directly provided by the local registry offices of the federal state of Rhineland-Palatinate and not surveyed by the questionnaire. We used information on the relationship between the respondent and the decedent to set up a variable on proxy type with the following 3 categories: “wife/husband, daughter/son, and other.” Age was classified into 5 categories: 0 to 59, 60 to 69, 70 to 79, 80 to 89, and 90+ years.
Place of Death
The actual place of death was surveyed by the question: “Where did your relative die?” Participants could choose between “at home,” “at the intensive care unit of a hospital,” “at a standard hospital unit,” “in a hospice,” “in a palliative care unit of a hospital,” “in a nursing home,” or “somewhere else.” These options were classified as “at home,” “in a hospital,” “in a palliative care facility,” and “in a nursing home.” The category “hospital” contained standard hospital wards and intensive care units. The category “palliative care” comprised both palliative care units in hospitals and hospices. All places of death not assignable to 1 of the 4 categories (n = 23) were not considered in our analyses.
Type of Disease
The respondents were asked to state the diseases of their deceased relative during the last 4 weeks before death. Of that we created a dichotomous variable “type of disease” with the categories “cancer,” for people who had cancer before death, and “other,” for other diseases.
Statistical Analysis
All statistical analyses were carried out by STATA/IC 10.1 (StataCorp LP, College Station, Texas). Absolute and relative frequencies were calculated to describe the basic characteristics of the deceased. In bivariate analyses, we examined the association between symptom prevalence and place of death. Associations were considered significant, when P < .05 for Pearson chi-square test. In order to investigate the adjusted influence of place of death on symptom prevalence, 16 multiple logistic regression models were estimated. Adjustment was done for age, sex, marital status, proxy type, and type of disease. The dependent variables were defined as suffering moderately/severely from the respective symptom (1) versus suffering slightly/not at all from the respective symptom (0).
Results
After removing duplicates from our random sample of 5000 deceased people, 4967 questionnaires were sent out. In all, 3832 questionnaires were actually delivered, 1135 returned as undeliverable. In sum, 1378 questionnaires were completed, leading to a response rate of 36.0% (considering only those questionnaires that actually were delivered). For the subsequent analysis, information on 990 persons is used, since questionnaires concerning people whose death was not related to a chronic, incurable disease (n = 365) and/or contained “elsewhere/missing” as a place of death (n = 23) were excluded.
As depicted in Table 1, the mean age at death in our sample was around 77 years, with <9% having died at the age of 59 or younger. We had slightly more females (54.0%) than males (46.0%) in our sample. Decedents were mostly the spouses (38.9%) or children (45.9%) of the respondents.
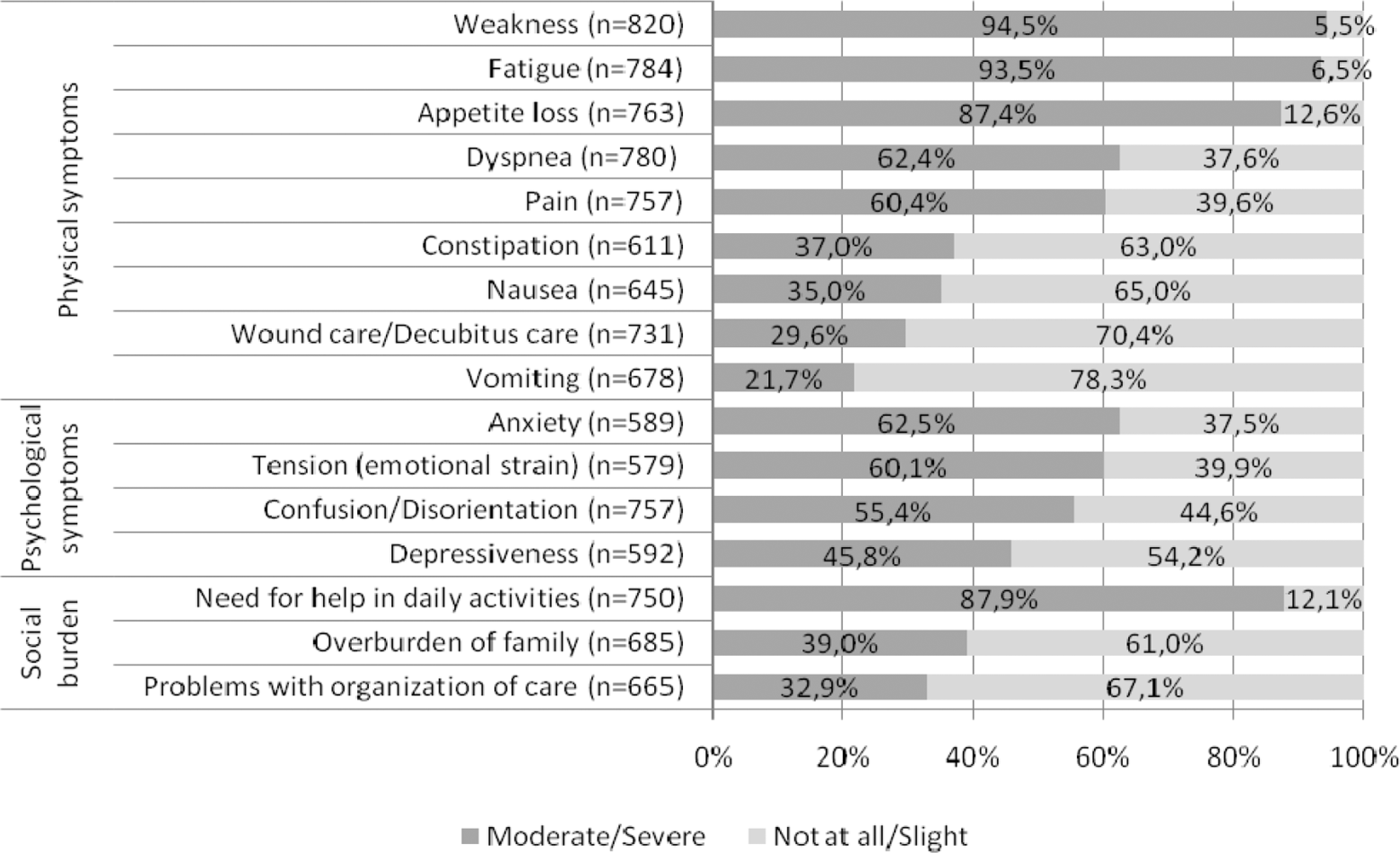
Overall symptom and social burden of deceased people with a chronic disease 2 days prior to death, in Germany. Percentages refer to respondents to the respective symptom.
Basic Characteristic of 990 Deceased People With a Chronic Disease in Rhineland-Palatinate, Germany, 2008
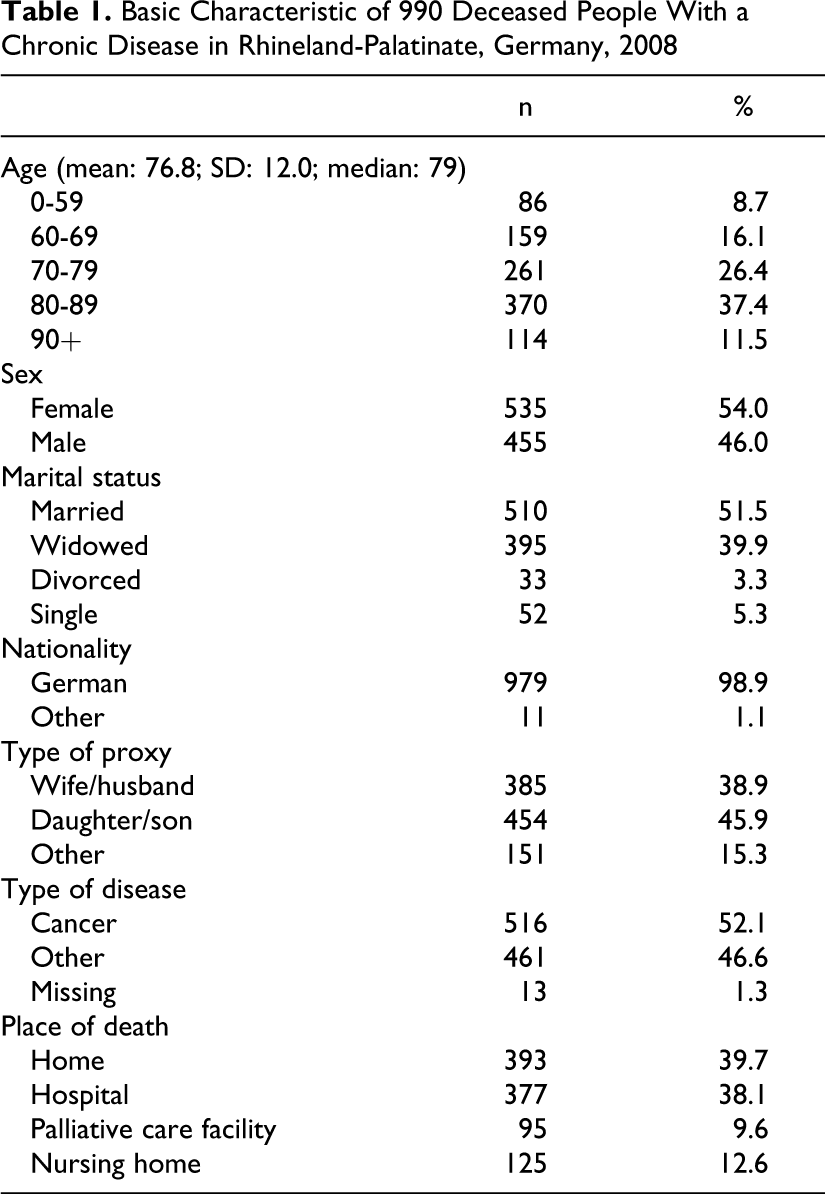
About half of the patients had cancer prior to death. Regarding the place of death, most people died at home (39.7%) or in a hospital (38.1%).
Overall Symptom and Social Burden in the Sample
The distribution of symptom and social burden in our sample is illustrated in Figure 1. Regarding physical symptoms, the vast majority of decedents had moderate-to-severe weakness (94.5%), fatigue (93.5%), and appetite loss (87.4%). High proportions were also found for moderate-to-severe dyspnea (62.4%) and pain (60.4%).
As to psychological disorders, people most frequently had moderate-to-severe anxiety (62.5%), followed by tension (60.1%), confusion/disorientation (55.4%), and depressiveness (45.8%). Concerning the social burden, almost all proxies stated that their deceased relative needed moderate-to-severe help in daily activities (87.9%). Comparatively less people mentioned a moderate-to-severe overburden of family (39.0%) or problems with organization of care (32.9%).
Moderate-to-Severe Symptom and Social Burden Stratified by Place of Death
The symptom and social burden stratified by place of death is shown in Table 2. There were significant associations between the physical symptoms such as pain, dyspnea, fatigue, and wound care/decubitus care and the place of death. Pain and dyspnea occurred most frequently in hospitals and fatigue and problems with wound/decubitus care in nursing homes. Regarding psychological symptoms, place of death was significantly associated with tension (emotional strain) and confusion/disorientation. Tension was highest in hospitals and confusion/disorientation in nursing homes.
Decedents Suffering From Moderate-to-Severe Symptom and Social Burden in Different Places of Death
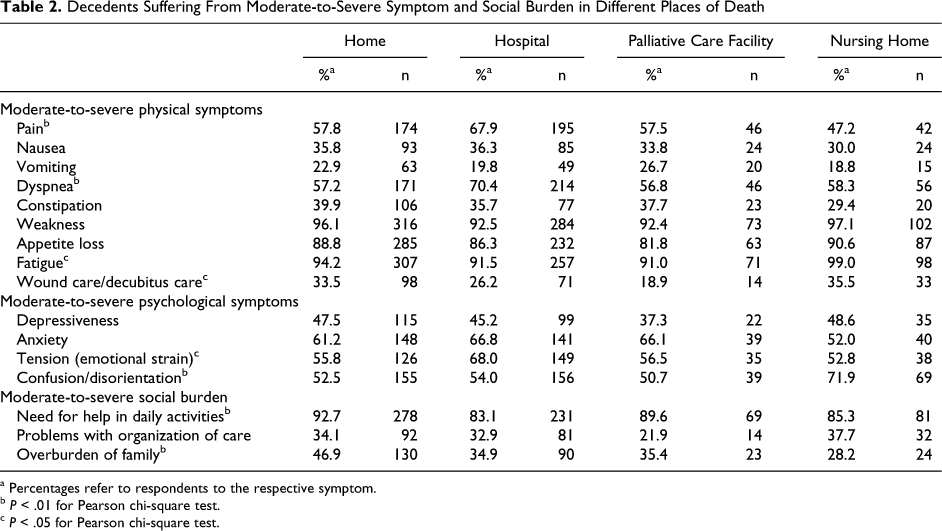
a Percentages refer to respondents to the respective symptom.
b P < .01 for Pearson chi-square test.
c P < .05 for Pearson chi-square test.
Concerning social burden at the end of life, there were significant associations between need for help in daily activities and overburden of family with the place of death. Both were highest when home was the actual place of death.
Multivariate Analysis
In order to investigate the adjusted influence of place of death on symptom prevalence, 16 multiple logistic regression models were estimated. Adjustment was done for age, sex, marital status, proxy type, and type of disease. The results are listed in Table 3 and show that place of death significantly influenced the symptoms such as pain, dyspnea, problems with wound/decubitus care, tension (emotional strain), confusion/disorientation, need for help in daily activities, and overburden of family. When people passed away in a hospital, there was a higher probability to suffer from moderate-to-severe pain (adjusted odds ratio [aOR]: 1.59; 95% confidence interval [CI]: 1.12-2.24), dyspnea (aOR: 1.65; 95% CI: 1.17-2.32), and tension (emotional strain; aOR: 1.61; 95% CI: 1.08-2.38) compared to people dying at home.
Multiple Logistic Regression Models Estimating the Influence of Place of Death on Suffering Moderately/Severely (1) Versus Not at All/Slightly (0) from 16 symptoms in the last 2 Days of Life, Adjusted for Age, Sex, Proxy Type, Marital Status, and Type of Disease
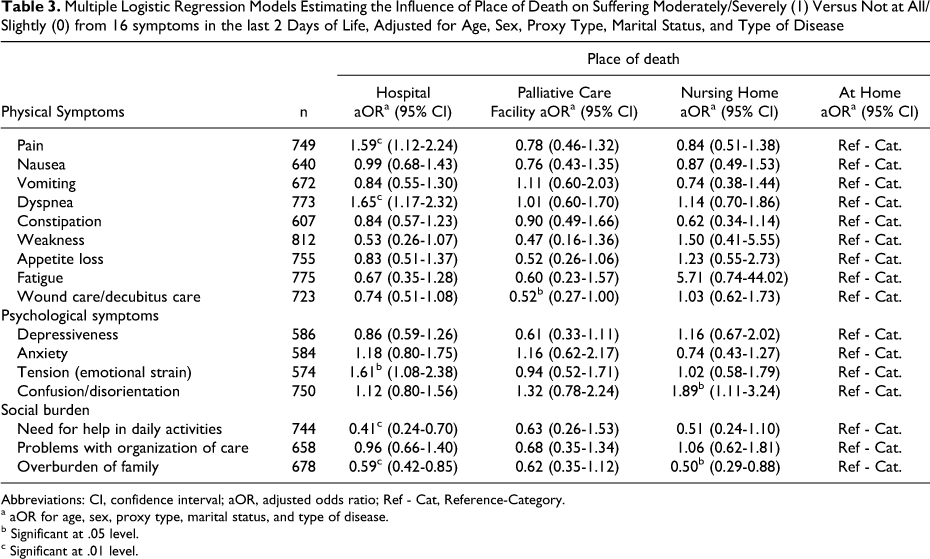
Abbreviations: CI, confidence interval; aOR, adjusted odds ratio; Ref - Cat, Reference-Category.
a aOR for age, sex, proxy type, marital status, and type of disease.
b Significant at .05 level.
c Significant at .01 level.
On the contrary, the probability to suffer from need for help in daily activities (aOR: 0.41; 95% CI: 0.24-0.70) and overburden of family (aOR: 0.59; 95% CI: 0.42-0.85) was significantly lower, when hospital was the place of death. Dying in a nursing home significantly increased the probability to suffer from moderate-to-severe confusion/disorientation (aOR: 1.89; 95% CI: 1.11-3.24) and decreased the probability of an overburden of family (aOR: 0.50; 95% CI: 0.29-0.88). Dying in a palliative care facility significantly decreased the probability to suffer from moderate-to-severe problems with wound/decubitus care (aOR: 0.52; 95% CI: 0.27-1.00) compared to people dying at home.
Discussion
Main Findings
In the present article, symptom prevalence of chronically ill patients in different places of death in Germany was investigated. Nearly all decedents suffered from moderate-to-severe weakness, fatigue, appetite loss, and need for help in daily activities in the last 2 days of life. More than half of the decedents suffered from moderate-to-severe dyspnea, pain, constipation, anxiety, tension (emotional strain), and confusion/disorientation. The study further showed that the symptom and social burden significantly differs depending on the place of death. Compared to patients dying at home, people who passed away in a hospital had a higher probability to suffer from moderate-to-severe pain, dyspnea, and tension (emotional strain) and a lower probability to suffer from need for help in daily activities and overburden of family. People dying in nursing homes suffered significantly more from confusion/disorientation and significantly less from overburden of family. Patients in palliative care facilities suffered significantly less from problems with wound/decubitus care compared to people dying at home.
Relevance of the Findings and Implications
Studies regarding symptom burden of dying people are often limited to specific types of diseases (especially cancer) and care settings (mostly hospice and palliative care facilities). To the best of our knowledge, this is the first report on symptom and social burden at national and international level, comparing symptom prevalence across different care settings and independent of the disease type.
In a previous German study, Ostgathe et al compared moderate-to-severe symptom burden between patients with cancer (n = 4035) and noncancer (n = 147) patients in a palliative care ward. 12 Generally speaking, reported relative frequencies for moderate-to-severe symptom burden in our sample were higher compared to the figures in the study of Ostgathe et al. For patients with noncancer and cancer diagnoses, they found 49%/55.8% suffering from moderate-to-severe pain, 17.1%/28.9% from nausea, 19.4%/8.2% from vomiting, 29%/40% from dyspnea, 33.8%/35.9% from depressiveness, 39.8%/45.9% from anxiety, 44.7%/51.9% from tension (emotional strain), and 17.2%/32.1% from confusion/disorientation, respectively. We suppose that differences can in part be attributed to the fact that the focus of our investigation was on the last days of life. The increase in confusion and dyspnea prior to death is well described in the available literature. 13,14
While the high prevalence of symptoms in dying patients as described by their relatives gives cause for serious concern for underassessment and undertreatment, it has to be kept in mind that information on symptom frequency based on information provided by the bereaved is subjective and prone to bias (see limitations). It is also worth noting that a high symptom burden is not necessarily attributable to differences in efficient treatment of symptoms in different care settings. For instance, pain and dyspnea were highest when hospital was the place of death. A quite reasonable explanation for this finding might be that patients who were initially cared for outside a hospital had been hospitalized before death because of the severity of upcoming symptoms. Another reason for higher ratings of pain might be that patients and family members are more frequently encouraged to report pain to physicians and nurses in hospitals than in other settings. 15 It is as well striking that the bereaved relatives also report a high symptom burden of their dying loved ones in specialized palliative care facilities. Again, a probable explanation could be that particularly burdensome symptoms are the reason that people are transferred into such a specialized facility.
As to the social burden, severe overburden of family was highest when people died at home. This is not surprising since caring for a loved one at home involves a lot of effort and time. Another interesting finding is that relatives stated that there were problems with organization of care even when patients died in an institution. We assume that this answer reflects the problem of people to organize appropriate care at home, which finally leads to hospitalization or prevents patient’s discharge from an institution.
It is quite probable that the symptom burden perceived by the bereaved relatives differs from the perception of the patients themselves and of health professionals. Death rattle, for instance, is frequently confused with dyspnea by the relatives. 16 Palliative sedation for severe dyspnea, agitation, or pain at the end of life can serve as another example for disparities in judgment; professionals may feel that symptom control was effective, while relatives may still keep in mind these symptoms as burdensome in the last days of life. Yet, regardless of whether health professionals or the patient judge the intensity of burden in a different way, the personal experience of family caregivers must be taken seriously. Dying is not only what the patient experiences but also what the family remembers 17 or as Dame Cicely Saunders puts it, “How people die remains in the memories of those who live on.” 18 Our results thus once again emphasize the necessity to support the relatives before and after death took place in all places of care and regardless of the type of disease. 19
Limitations
Regarding limitations, our questionnaire was not tested for its psychometric properties in advance, thus partly limiting the quality of the data. Since our study was an exploratory approach primarily aimed at gathering basic information, the questionnaire was not conceived as a tool with defined psychometric properties but rather as a first step in the assessment of different aspects in outpatient and inpatient end-of-life care.
Moreover, we cannot exclude selection bias, since people who are able to report on the dying experience of their loved one shortly after death, may be highly selected. 3
The possibility of recall bias should also be acknowledged throughout our retrospective study. The interrogation of the bereaved was carried out as fast as ethically tolerable after the death of the concerning relative. Thereby, we tried to minimize possible systematic errors due to memory, without unnecessarily molesting the bereaved relatives.
A further point of criticism consists in interviewing relatives of deceased persons, rather than asking the dying themselves prior to death. It has to be considered that the evaluation of symptom burden is always subjective, depending on different perceptions by patients, family members, and professional caregivers. 20 Hales et al summarized the criticism on family member interviews in their review as being dependent on “the subjective state at the time of the event and at recall, their own individual experiences, the time from event to recall, motivation, and the ability to take another’s perspective into account.” 21
Nevertheless, surrogate interviews are methodologically necessary, since a direct participation of patients is problematic due to the difficulty of prospectively identifying patients in the dying phase 21 and, of course, due to ethical considerations.
A further limitation is the possibility of bias due to the partly sizable proportions of missing values for physical, psychological, and social items. Possible explanation might be that the bereaved found it difficult to give a distinct judgment on the severity of symptoms in the last days of life or were not directly involved in the care process.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Fresenius Kabi Germany GmbH and the German Pharmaceutical Industry Association (BPI).