
Abstract
Objective:
To examine the associations between palliative care types and hospital outcomes for patients who have or do not have advance directives.
Method:
Using administrative claims and clinical data for critically ill older adults (n = 1291), multivariable regressions examined the associations between palliative care types and hospital outcomes by advance directive status.
Results:
Integrative palliative care was associated with lower hospital costs, lower adjusted probability of in-hospital deaths, and higher adjusted probability of hospice discharges. There was no difference in hospital outcomes by palliative care types in those with advance directives.
Conclusion:
Significantly lower hospital costs and in-hospital deaths with higher hospice discharges were observed in integrative palliative care compared to consultative palliative care, but these findings were diminished with the presence of advance directives.
Keywords
Introduction
The growing literature on the benefits of palliative care has covered diverse areas including financial outcomes. 1–5 By reducing hospital length of stay, palliative care has been shown to reduce costs 1–5 by 25% to 66%. The cost-saving benefits of palliative care are attractive to both health care administrators and insurers to overcome today’s financial struggles across the health care industries. 6 –8 Previous literature has attempted to explain how palliative care can reduce length of hospital stay and achieve cost-saving benefits: Palliative care enables the consultation team to narrow the communication gaps between providers and patients or families. 1–5 This allows them to forego treatments that will not meet their goals or prolong life in a meaningful way. 6 –9 The cost-saving benefits of palliative care on decedents have been reported to be larger than those of live discharges. 3,5,8,9 However, numerous questions as to how palliative care has directly reduced hospital length of stay have not been explored thoroughly or answered fully in the literature to date.
The limitations of palliative care research (eg, difficulty in defining the comparison group and prolonged hospital length of stay as a trigger of palliative care involvement) may have contributed to the relative lack of conceptualization related to the cost-saving benefits of palliative care. 5,8,9 These dilemmas have been thought to come from the traditional palliative care delivery model: the consultative model. 10,11 Consultative palliative care has is only delivered when specifically requested by the primary care team and in settings where a consultation team is available. Recent efforts have suggested shifting the palliative care delivery type from the traditional consultative model to the integrative model. 10,11 The integrative model is expected to overcome the aforementioned dilemmas by embedding palliative care into the daily practice of intensive care unit (ICU) primary teams when treating all patients who face critical illnesses. 10 –14
A few studies that have been limited to hospice enrollees have demonstrated that the presence of advance directives was associated with lower rates of hospital deaths and related Medicare expenditures. 15,16 This has been explained by the facilitating role of palliative care: earlier and more frequent establishment of advance directives. 15 –18 It has been sometimes overlooked that advance directives may influence hospital costs and discharge destinations of critically ill patients who are vulnerable to becoming medically futile. Thus, we hypothesize that palliative care services in acute care settings promote more advance directives, which may navigate medically futile patients through more hospice discharges and reduce in-hospital deaths. Therefore, although research has not fully examined the interactions between palliative care types and advance directives in acute care settings, this knowledge may widen our understanding of whether palliative care recipients’ utilizations across health care systems vary by palliative care types and advance directive status. Because the integrative model provides patients with easy access to palliative care compared to their consultative model counterparts, integrative palliative care recipients would be more likely to facilitate communications between health care professionals and patients or families, which would further reduce hospital costs through fewer in-hospital deaths and have hospice discharges from the hospital. In addition, integrative palliative care's impact would be substantial compared to those without advance directives who are more likely to inflate hospital length of stay than are those with advance directives. Moreover, research on critically ill older adults is urgently needed because they are most vulnerable to becoming medically futile from even a severe acute illness. In addition, this situation commonly inflates hospital margin deficits by prolonging hospital length of stay and is more pronounced among seniors than any other age group. 19,20
Using administrative and clinical data for critically ill older adults, the aims of the present study are to (1) compare hospital outcomes (hospital costs, in-hospital deaths, and hospice discharges) by palliative care types and (2) examine the relationships between palliative care types and hospital outcomes by advance directive status.
Methods
Study Site and Data Collection
The study site was a nonprofit community hospital (total 280 hospital beds and 35 ICU beds) in a US metropolitan area. Administrative claim data and electronic medical records (clinical data) were matched by name and date of birth. Inclusion criteria were (1) admission to ICU, (2) age 65 years or older, and (3) Medicare beneficiaries; thereby, we intended to equalize the patients’ opportunities for public health insurance coverage for current hospital and future potential hospice care. Exclusion criteria were (1) hospice enrollee prior to ICU admission, (2) advance directive specifying comfort care, and (3) principal diagnoses specified by the International Classification of Diseases, Ninth Revision (ICD-9) containing the complications of pregnancy, childbirth, and puerperium (630-679), congenital anomalies (740-759), and certain conditions originating in the perinatal period (760-779). The present study had 3 phases: phase 1 (January to December 2005), the transitional phase (January to December 2006), and phase 2 (January to December 2007). During phase 1, palliative care in the ICU was delivered with the consultative model. The palliative consultation team comprised 2 attending physicians, 1 social worker, and 1 chaplain who rounded on weekdays. The social worker and chaplain did not exclusively devote their time to the palliative consultation team. From the transitional through phase 2, the integrative palliative care for all older adults was introduced to the ICU. Expanded palliative team manpower comprised 5 physicians (3 attending and 2 resident physicians), a palliative care director (nursing background), and a chaplain all of whom reviewed the medical records of all ICU-admitted older adults and identified their urgent needs for palliative care: (1) relieving physical and emotional distress, (2) resolving questions and conflicts between caregivers and health care providers, and (3) establishing goals of care by ensuring advance care planning. Once the palliative team had identified the need for palliative care, the palliative team informed the primary team and continued to provide palliative care with the permission of the primary team. The social worker and chaplain exclusively devoted their time to the palliative consultation team.
Administrative claim data and electronic medical records (clinical data) were matched by name and date of birth. The authors reviewed data together regularly. We collected 1478 eligible individuals. If a patient had more than 1 distinct ICU admission, each admission was included. Because of the relatively small numbers (n = 49, less than 4%) of Hispanic, Native American, and Asian patients, we restricted our analyses to African Americans and Whites only. Given a relatively small number of mild severity of illness (n = 71, less than 5%) and difficulty in interpreting the statistical analysis, individuals with mild severity of illness were excluded. Due to missing or insufficient data, less than 5% (n = 67) were excluded.
Main Outcome Measures: “Hospital Costs,” “In-Hospital Deaths,” and “Hospice Discharges”
Hospital costs were defined as hospital charges to the Centers for Medicare and Medicaid Services. All costs were converted into 2007 US dollars by adjusting for inflation rates based on the Consumer Price Index of the Bureau of Labor Statistics, Department of Labor. 21 In-hospital deaths were defined as deaths at either the ICU or another place in the hospital. Hospice discharges from a hospital included home hospice or hospice general inpatient care.
Predictors
Predictors were independent variables including age, gender, ethnicity, advance directive status, severity of illness, education, marital status, private health insurance, and principal diagnoses at time of hospital admission. Social workers interviewed patients or families at the time of hospital admission and documented advance directive status, education, and marital status in the medical records. Advance directives were defined whether either living will was written or durable power of attorney (DPOA) was designated. Living will was defined as the statement that allows persons to state the kind of health care they do or do not want under certain circumstances if they are unable to make the medical decision for themselves. The designation of DPOA was defined as the statement that identified someone who can make health care decisions. The All Patient Refined Diagnostic Related Group (APR-DRG) severity of illness classification system was used to estimate the severity of illness. The APR-DRG data were gathered based on the 3M Health Information System (Wallingford, Connecticut). The APR-DRG data were collected from the Department of Medical Operations, which was unaware of the study objectives and was abstracted by the authors. The validity of APR-DRG severity of illness in acute palliative care has been discussed elsewhere. 22,23 Private health insurance meant additional “out of pocket” health insurance coverage beyond public health insurance. Advance directives meant whether either living will was written or the DPOA had been designated in the electronic medical records. Social workers were responsible for clarifying the documentation status of living will and DPOA of all patients at the time of admission. Principal diagnoses were classified into the following 8 groups by the ICD-9: (1) infectious and parasite diseases (001-139), (2) cancer and diseases of the blood and blood-forming organs (140-239, 280-289), (3) endocrine, nutritional, and metabolic diseases and immunity disorders (240-279), (4) diseases of the nervous and sense organs (320-389), (5) diseases of the circulatory systems (390-459), (6) diseases of respiratory systems (460-519), (7) diseases of the digestive and genitourinary systems (520-579, 580-629), (8) diseases of the skin and subcutaneous, musculoskeletal system, and connective tissue (680-709, 710-739) and mental disorders, others combined by systems, signs, and ill-defined conditions, injury and poisoning, external causes of injury and supplemental classification (290-319, 780-799, 800-899, E and V codes). For ease of interpretation, the predictors were categorized like the followings: age (65-79 years and 80 years or older), gender (male and female), ethnicity (African Americans and Whites), severity of illness (moderate, major, and extreme), education (high school education or less and high school graduation or higher), marital status (married and never married/widowed/divorced), private health insurance (yes and no), any advance directives (yes and no), and principal diagnoses. This study was approved by the Institutional Review Board of the Cleveland Clinic Health System.
Analytic Strategy
Bivariate comparisons of sample characteristics and main outcome measures between palliative care types (study phases) were examined using chi-square tests. All reported P values were 2-sided throughout, and P < .05 was considered statistically significant. We used generalized linear models (GLMs) with a log link function and gamma distribution to fit skewed hospital cost data. 24 The dependent variable was hospital cost, and the independent variables included age, gender, ethnicity, education, marital status, severity of illness, private insurance, principal diagnoses, advance directive status, and the key independent variable, palliative care types (phase 1, consultation; phase 2, integration). The average predicted hospital cost difference (phase 2 minus phase 1) with the corresponding 95% confidence intervals was derived from GLMs controlling age, gender, ethnicity, education, marital status, severity of illness, private health insurance, principal diagnoses, and advance directive status. We estimated multivariate logistic regressions of in-hospital deaths and hospice discharges controlling for the sample characteristics described above to compute odds ratios (ORs) along with corresponding 95% confidence intervals (CIs) were computed. 25,26 The OR >1 indicated that the predicted probability in the integrative palliative care phase (phase 2) was higher than that in the consultative palliative care phase (phase 1). All data manipulation and analyses were performed using SAS statistical software version 9.2 (SAS Institute, Inc, Cary, North Carolina).
Results
Sample Characteristics
Our sample included 1291 admissions. Among them, 673 admissions occurred in the consultative model (phase 1) and 618 admissions occurred in the integrative model (phase 2). Table 1 presents the sample characteristics of phases 1 and 2. Individuals aged 80 or older were 44% and 46% in phases 1 and 2, respectively. Females represented 57% and 59% of the sample in phases 1 and 2, respectively. African Americans accounted for 67% of the sample in phase 1 and 68% in phase 2. Of them, 33% were at moderate, 54% were at major, and 13% were at extreme severity of illness in phase 1; 37% were at moderate, 51% were at major, and 12% were at extreme severity of illness in phase 2. High school graduation or higher education represented 42% and 44% of the sample in phases 1 and 2, respectively. Those who never married, widowed, or divorced were 38% and 41% of the sample in phases 1 and 2, respectively. Forty-eight percent were private health insurance holders in phase 1 and 44% in phase 2. In phase 1, 38% had any advanced directives. In phase 2, 55% had any advanced directives. The sample characteristics by study phases were not statistically different except for the character of advance directives (P < .001).
Sample Characteristics
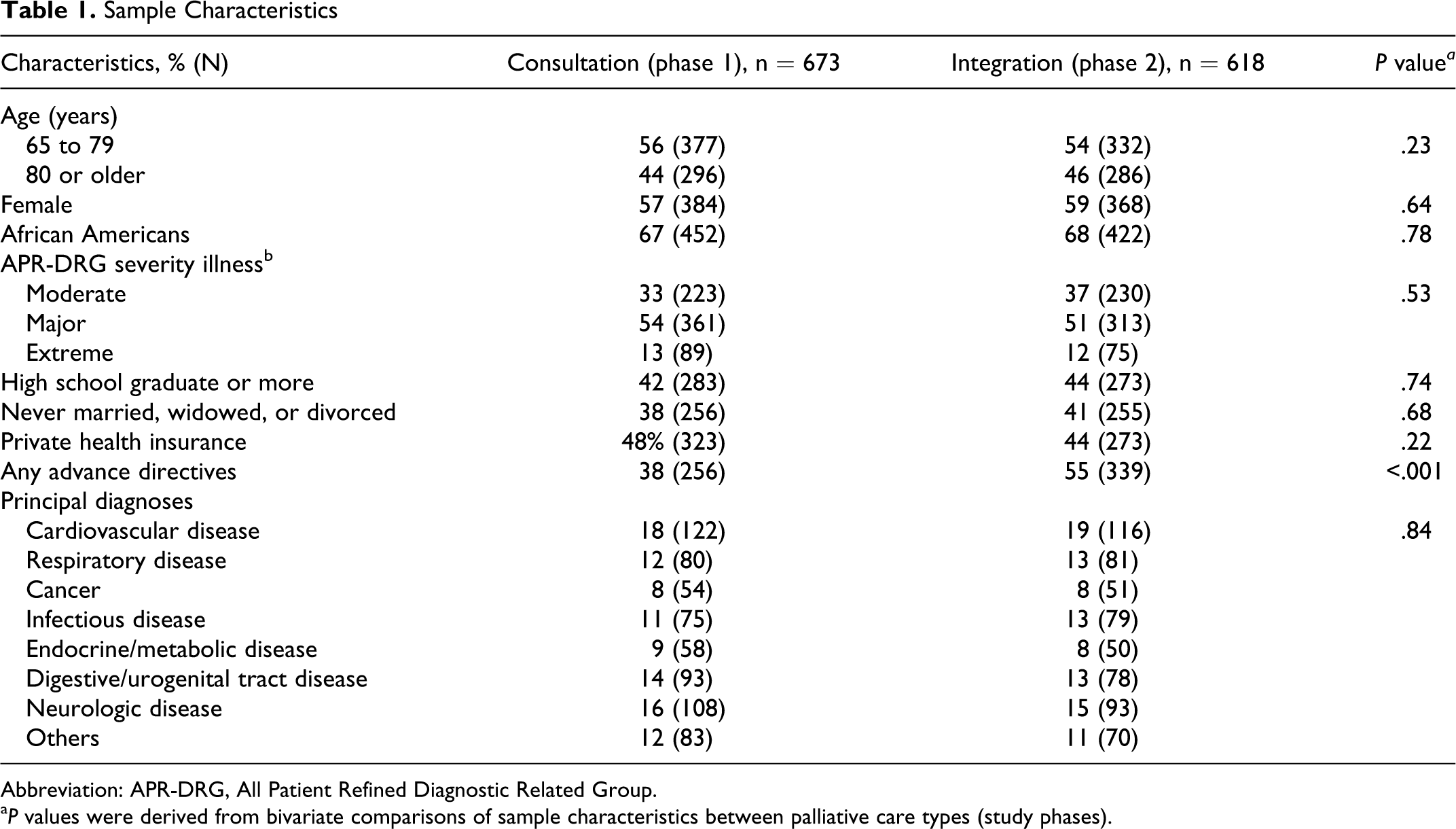
Abbreviation: APR-DRG, All Patient Refined Diagnostic Related Group.
a P values were derived from bivariate comparisons of sample characteristics between palliative care types (study phases).
Main Outcome Measures
Table 2 presents the main outcome measures by study phases. In the overall sample (n = 1291), the hospital costs in phase 2 (median $50 715; interquartile range [IQR] $46 352-$55 193) were significantly lower than those in phase 1 (median $58 531; IQR $54 349-$63 838; P = .02). In the absence of advance directives (n = 696), the hospital costs in phase 2 (median $54 871; IQR $51 421-$59 108) were significantly lower than those in phase 1 (median $64 268; IQR $61 534-$69 773; P < .001). In the presence of advance directives (n = 595), there was no statistically significant difference in hospital costs by study phases. In the overall sample, the in-hospital deaths in phase 2 (13%) were significantly lower than those in phase 1 (18%; P = .003). In the absence of advance directives, the in-hospital deaths in phase 1 (16%) were significantly lower than those in phase 1 (23%; P < .001). In the presence of advance directives, there was no significant difference in in-hospital deaths by study phases. In the overall sample, the hospice discharges in phase 2 (14%) were significantly higher than those (9%; P = .007) in phase 1. In the absence of advance directives, the hospice discharges in phase 2 (12%) were significantly higher than those in phase 1 (6%; P < .001). In the presence of advance directives, there was no significant difference in hospice discharges by study phases.
The Main Outcome Measures Specified by Advance Directive Status
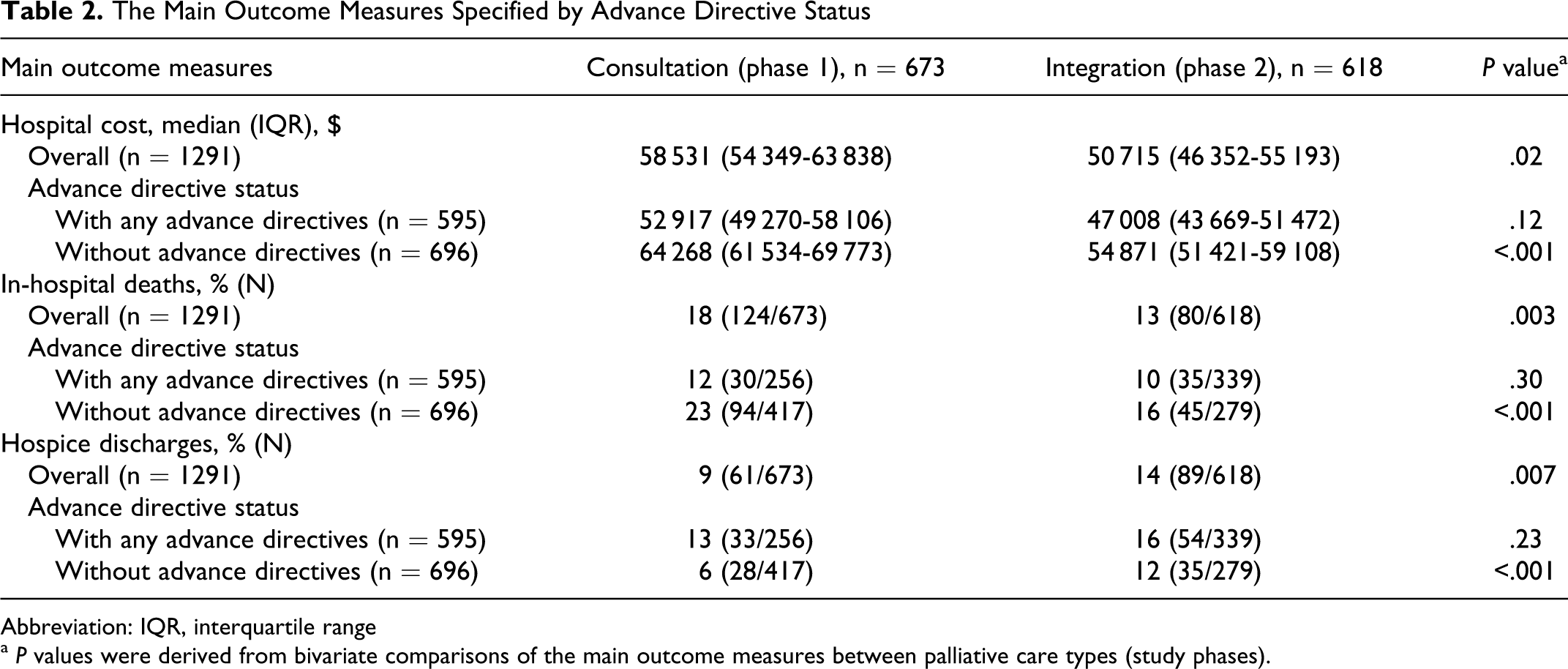
Abbreviation: IQR, interquartile range
a P values were derived from bivariate comparisons of the main outcome measures between palliative care types (study phases).
Multivariate Regression Adjusted Hospital Costs
Table 3 presents the multivariate regression adjusted “hospital costs.” Although significant correlations between study phases and advance directive status (coefficient = .57, P < .01) and between advance directive status and ethnicity (coefficient = .45, P < .01) were observed, variance inflation factors were less than 2.5; thus, all of ethnicity, advance directives, and study phases remained in regressions. Significant interactions among sample characteristics and hospital costs were tested. None of the interaction terms was statistically significant; hence, they were not included in regressions. In the overall sample (n = 1291), after adjusting for age, gender, ethnicity, education, marital status, severity of illness, private health insurance, principal diagnoses, and advance directive status, the hospital costs in phase 2 were significantly lower than those in phase 1 (predicted difference, $6236; 95% CI, $12 371-$302; P = .02). There was important heterogeneity in the relationships between palliative care types and hospital costs by advance directive status. In the absence of advance directives (n = 696), hospital costs in phase 2 were significantly lower than those in phase 1 (predicted difference, $8109; 95% CI, $15 362-$318; P = .004). In the presence of advance directives (n = 595), there was no statistically significant difference in hospital costs between study phases. The total variance of hospital costs explained by regressions was 28% (overall sample) and 32% (sample without advance directives). Our results were consistent across numerous alternative specifications including an ordinary least squares regression. 24
Multivariate Regression Adjusted “Hospital Cost”
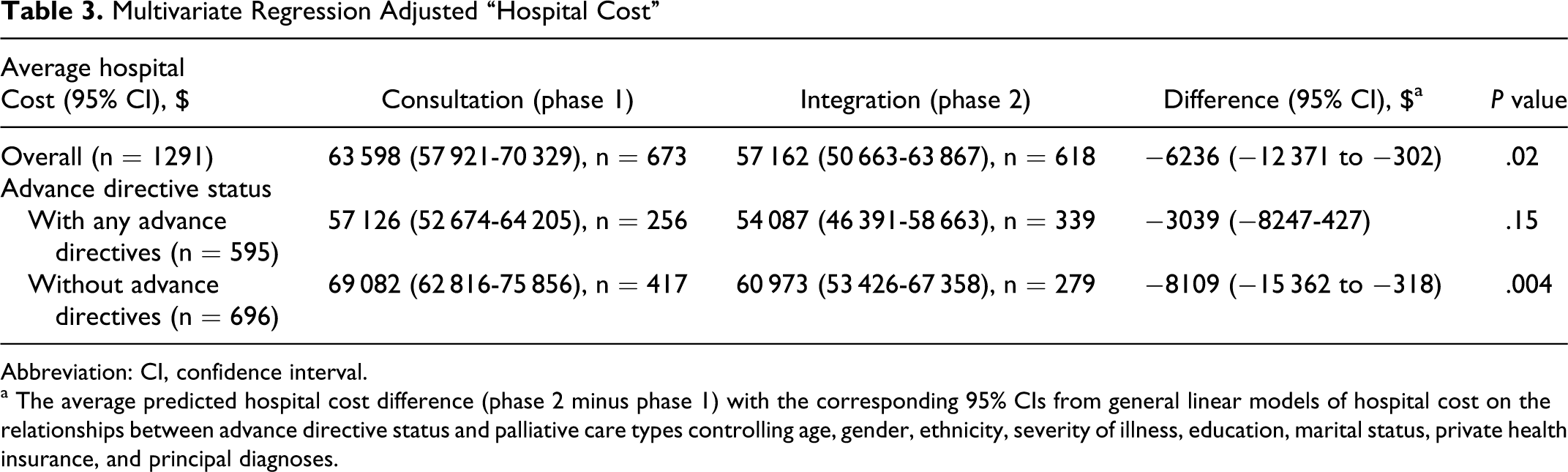
Abbreviation: CI, confidence interval.
a The average predicted hospital cost difference (phase 2 minus phase 1) with the corresponding 95% CIs from general linear models of hospital cost on the relationships between advance directive status and palliative care types controlling age, gender, ethnicity, severity of illness, education, marital status, private health insurance, and principal diagnoses.
Predicted Probability of In-Hospital Deaths and Hospice Discharges
Table 4 presents the predicted probability of in-hospital deaths and hospice discharges using multivariate logistic regressions controlling the sample characteristics described above. Bivariate correlations between predictors were assessed to detect multicollinearity. Although significant correlations between advance directive status and study phases on in-hospital deaths (coefficient = .43, P < .01) and hospice discharges (coefficient = .54, P < .01) were observed, the variance inflation factors were less than 2.5; thus, both advance directive status and study phases remained in logistic regressions. Significant interactions among sample characteristics and both outcomes (in-hospital deaths and hospice discharges) were tested. None of the interaction terms were statistically significant; hence, they were not included in the logistic regressions. In the overall sample (n = 1291), the adjusted probability of in-hospital deaths in phase 2 (13%; 95% CI, 8%-18%) was lower than that in phase 1 (18%; 95% CI, 13%-23%; OR = 0.63; 95% CI, 0.37-0.92; P = .02). In the absence of advance directives (n = 696), the adjusted probability of in-hospital deaths in phase 2 (16%; 95% CI, 11%-21%) was lower than that in phase 1 (24%; 95% CI, 20%-29%; OR = 0.49; 95% CI, 0.23-0.84; P = .004). In the presence of advance directives (n = 595), there was no statistically significant difference in in-hospital deaths between study phases. In the overall sample, the adjusted probability of hospice discharges in phase 2 (14%; 95% CI, 9%-19%) was higher than that in phase 1 (9%; 95% CI, 5%-14%; OR = 1.92; 95% CI, 1.05-3.14; P = .01). In the absence of advance directives, the adjusted probability of hospice discharges in phase 2 (12%; 95% CI, 9%-16%) was higher than that in phase 1 (6%; 95% CI, 3%-10%; OR = 2.56; 95% CI, 1.12-3.93; P = .001). In the presence of advance directives, there was no statistically significant difference in hospice discharges between study phases. All logistic regressions were assessed with goodness-of-fit testing procedures, which confirmed that these were not violated. 25,26
Predicted Probability of In-Hospital Deaths and Hospice Discharges
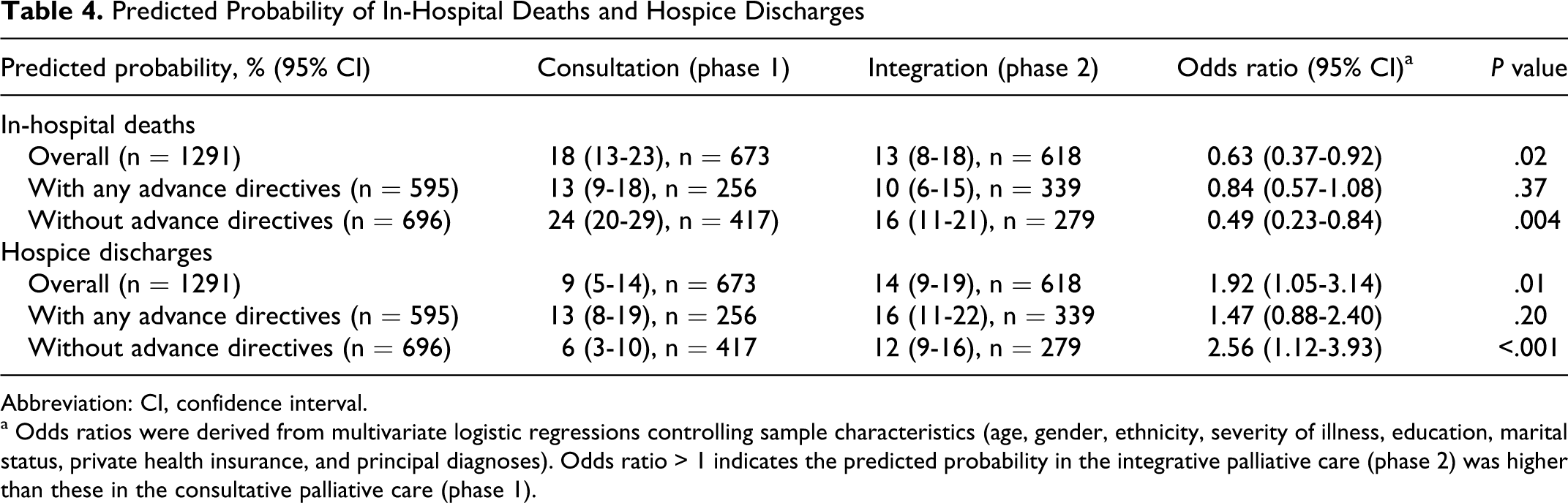
Abbreviation: CI, confidence interval.
a Odds ratios were derived from multivariate logistic regressions controlling sample characteristics (age, gender, ethnicity, severity of illness, education, marital status, private health insurance, and principal diagnoses). Odds ratio > 1 indicates the predicted probability in the integrative palliative care (phase 2) was higher than these in the consultative palliative care (phase 1).
Discussion
Using linked administrative claim and clinical data on critically ill older adults, we found that integrative palliative care was more likely to reduce hospital costs than consultative palliative care. Although integrative palliative care was more likely to have any advance directives compared to consultative palliative care (55% vs 38%; P < .001), the difference of palliative care consequences by palliative care types (decreases in in-hospital deaths and reciprocal increases in hospice discharges in the integrative model) was observed after controlling sample characteristics including advance directive status.
Our findings may replicate the palliative care consequences for critically ill older adults as has been reported in previous literature including the landmark Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment (SUPPORT) from the 1980s: attenuating communication barriers between health care providers and patients or families, thereby optimizing the utilization of ICU beds and reducing hospital costs by decreasing in-hospital deaths and reciprocally increasing hospice discharges. 27,28 Our findings reflect prior evidence that the more accessible model of integrative palliative care reduces both hospital costs compared to the consultative model. 10,13 The percentage of cost saving in the present study (11%) was lower and the actual cost savings were higher ($6236) than those of other studies. These findings may be explained by the present study’s unique enrollees; older adults in an ICU receive more complex health services and utilize more resources than do patients in any other hospital unit.
In the integrative palliative model, these consequences of palliative care (decreases in in-hospital deaths and reciprocal increases in hospice discharges in the integrative model) seemingly penetrated the ICU earlier and more thoroughly than they did in the consultative model. 10 –14 Our findings may be explained by the fact that medically futile patients in the integrative model were more likely to be discharged to hospice rather than opting for life-sustaining treatments and facing in-hospital deaths. Previous studies have reported that the quality of death was higher for decedents who died at home or in a hospice care facility compared to those who died in hospital and nursing home settings. 9,13,29 In addition, caregivers reported worse overall physical and mental health following deaths characterized by use of aggressive treatment before death. 13,27,29 Thus, the integrative model has important implications because it may enable patients and caregivers to more proactively participate in establishing goals of care and discharge planning and lead to a higher level of satisfaction by utilizing hospice services when appropriate.
One interesting interpretation of these data is that the effects of palliative care types on hospital costs, in-hospital deaths, and hospice discharges vary by advance directive status. The greatest effects of integrative palliative care were observed among those who do not have advance directives compared to those who do. Subgroup analysis showed that the magnitude of palliative care consequences was aggregated when integrative palliative care was provided to those without advance directives. By contrast, the magnitude of palliative care consequences was diminished when integrative palliative care was provided to those with advance directives. Existing documentation of advance directives had important implications in that both health care providers and patients or families had prioritized the discussion of advance care planning implicating that palliative care had already been effective.9,17,18,28 The impact of integrative palliative care on those with advance directives was not able to change the main outcomes compared to the consultative model. On the other hand, for those without any advance directives, exposure to palliative care had not been enough to achieve documentation of advance care planning prior to the implementation of the integrative model, a more efficient palliative care delivery model. Therefore, for those who had little understanding of palliative care, with improved access to palliative care services, the impact of integrative palliative care was statistically significant in changing the main outcomes incorporating the consequences of palliative care compared to consultative palliative care.
In the era of Patient Protection and Affordable Care Act (PPACA), reducing in-hospital deaths may contribute to incentive reimbursements from Medicare because inpatient mortality has been one of the core components of the Agency for Healthcare Research and Quality’s (AHRQ) quality index composite. 30 –33 Starting in 2013, up to 2% of hospitals’ reimbursements will be increased when a hospital meets the AHRQ’s composite score including mortality rate (as known as, value-based incentive payments). 30 –33 Therefore, mortality-reducing effects of integrative palliative care (by 37% compared to consultative palliative care in the present study) have the implication that integrative palliative care can be used as one of diverse solutions to improve hospital’s reimbursements.
Our findings should be interpreted in light of several limitations. A major limitation is lack of generalizability. Because the data were collected from a metropolitan area and limited to African Americans and Whites, the results in rural areas and among other ethnic groups were not reflected. Because our study was observational, we were unable to assess causal effects between palliative care types and hospital outcomes. Furthermore, we did not interview patients or families as to their preferences and used secondary data, which had potential for the plausible observer variation. Due to collapsing data in order to ease the interpretation of analysis and missing data, about 12% of data were excluded from analysis; therefore, selection bias may have occurred. For these reasons, our findings should be interpreted with caution and considered preliminary until they are confirmed in future studies with more representative data.
Conclusion
Significantly lower hospital costs and in-hospital deaths along with higher hospice discharges were observed in integrative palliative care compared to consultative palliative care, but these findings were diminished with the presence of advance directives in critically ill older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: supported by the American Geriatrics Society Seed Grant Research Program.