
Abstract
Objective:
Little is known regarding the perceptions of parents about end-of-life care for their children. This study describes parental perceptions of the care of hospitalized, terminally ill children in the areas of (1) clinical management, (2) interdisciplinary support, and (3) pain and symptom management.
Methods:
Through a mixed methods design, researchers interviewed a representative sampling of bereaved parents via telephone.
Results:
Data provided evidence of areas which lack satisfaction with elements of end-of-life care of hospitalized children.
Conclusion:
Parental satisfaction with their child’s care during end of life indicates need for improvement in pain management, communication, and parental involvement in decision making. While education cannot guarantee desired changes in attitudes or behaviors, it may provide the essential foundation of knowledge, skills, and ethical understanding needed by professional providers.
Introduction
Each year in America, almost 60 000 children under the age of 20 years die, and many of them suffer from a lengthy illness. 1 Technological advances and medical expertise have led to improved overall outcomes, but incurable conditions continue to lead to early death. Diagnoses which affect the length of children’s lives include congenital anomalies, chromosomal defects, trauma, neurodegenerative disorders, cancer, and HIV/AIDS. A child’s death can be an emotionally and physically painful experience for the child, family, and members of their social support system, such as friends, extended family members, classmates, teachers, and community. Reported suffering at end of life (EOL) adds complexity to the challenges faced by health care providers in caring for dying children and their families.2–5 Since the Institute of Medicine first issued a report almost a decade ago emphasizing the need to address pediatric EOL care, some progress has been made, but this care is still less than optimal. 6 Palliative care embraces a philosophy of physical, emotional, social, and spiritual elements of care and is most effectively managed by an interdisciplinary team. While some studies have described certain aspects of caring for children at the EOL, there is limited research examining comprehensive EOL care in this population. 7 In our country, children are still often deprived of the coordinated services an interdisciplinary pediatric palliative care team can provide at EOL. 8
In an effort to assess the EOL care provided at our institution, a 2-part study was completed. First, we examined the medical records of all children who died at our children’s hospital during 1 fiscal year. Children admitted to an inpatient unit (neonatal intensive care unit [NICU], pediatric critical care unit [PCCU], or general pediatric inpatient unit), who stayed more than 24 hours were included (N = 105). Documentation of EOL care, family and child interdisciplinary support, pain and symptom management, communication, and decision making were described in a previous report (phase I). 9 Next, data on a subset of children from phase I was collected. The purpose of this study (phase II) is to describe parental satisfaction of their children’s care at EOL and to identify parental needs for the development and provision of pediatric palliative care services.
Methods
After Institutional Review Board approval, the research team sent a letter to all parents of children who died in the hospital during the previous year, asking for their participation in a phone interview with a grief counselor from a community hospice. The letter was signed by the principal investigator (a nurse researcher at the children’s hospital) and contained a self-addressed stamped response card, requesting the best time and telephone number at which to call the parents. Care was taken to avoid sending the letter or telephoning the parents on an anniversary of their child’s diagnosis, birthday, or death, or on Mother’s or Father’s Day. Research assistants from a local hospice, who had no prior relationship to the parents, obtained verbal consent via the telephone after verifying eligibility and interviewed the participants. Parents completed a modified FAMCARE survey 10 and then answered semistructured questions about information sharing and communication.
Participants
Twenty-one parents returned the response cards, indicating their availability and willingness to participate in the study. Of those, 15 (71%) parents who identified themselves as the primary caregivers were able to be contacted. All parents who were contacted did consent to participate and were interviewed. According to self-report, 55% (n = 6) of respondents were caucasian, 36% (n = 4) were African American, and 1 family checked “other.” There were missing data for 4 families related to race. Fourteen mothers and 1 father completed the survey/interview. Age of the deceased children ranged from infants to 14 years.
Based on admitting diagnoses of their children, parents were divided into 6 groups: cardiac diagnoses (47%), congenital defects (13%), neonatal-specific diagnoses (13%), infectious diseases (13%), and oncology diagnoses (13%; Figure 2). Most of the children died in either the PCCU or the NICU, and only 1 child died in a general care unit. Mean length of stay in the PCCU was 34 days, in the NICU 13 days, and the general care unit 2 days (Table 1).
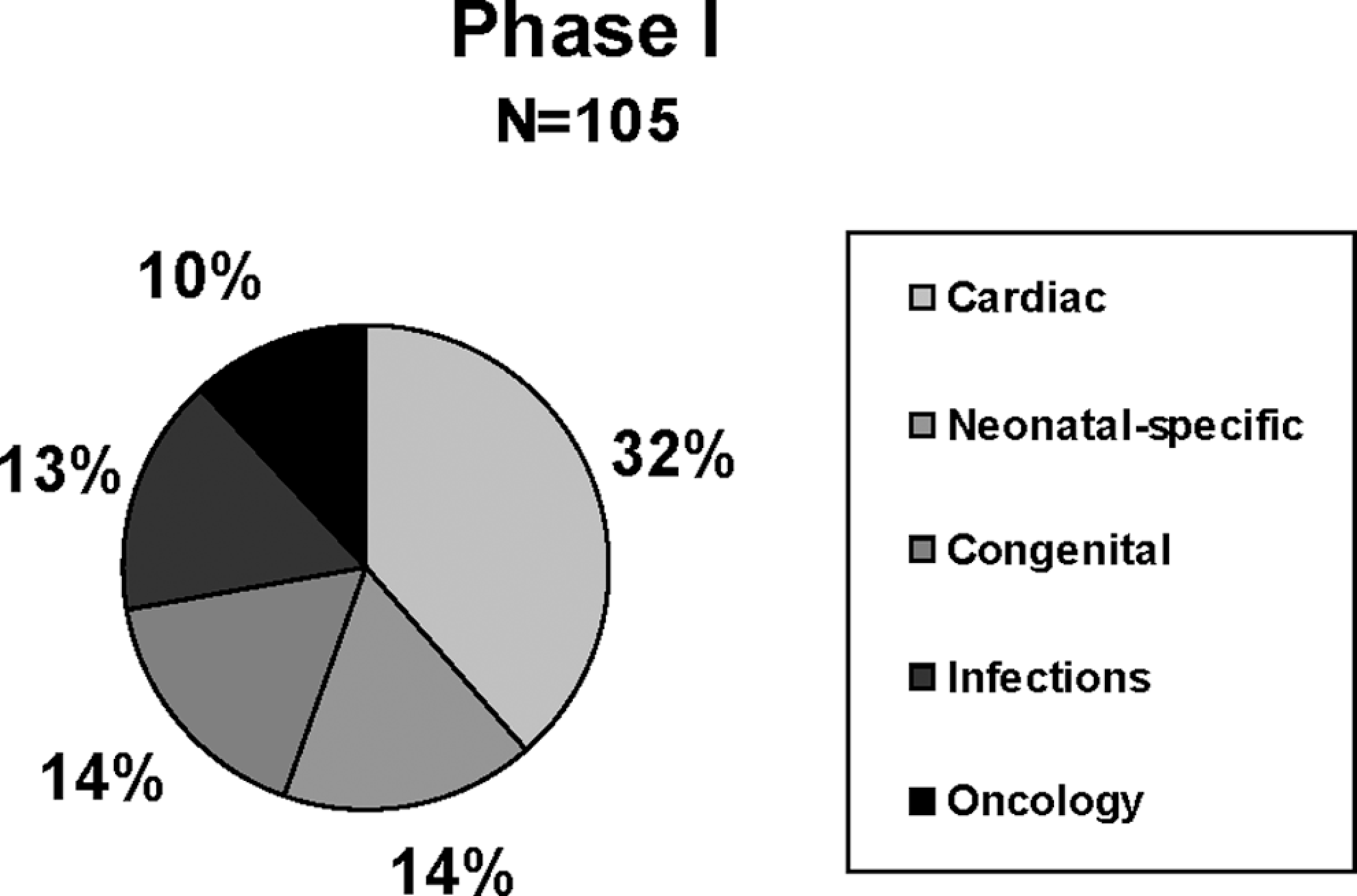
Diagnostic categories for phase I. Admitting diagnoses were divided into 5 groups. The remaining diagnoses included only 1 to 2 children (eg, sudden infant death syndrome (SIDS), metabolic conditions), and were therefore not included in the figure.
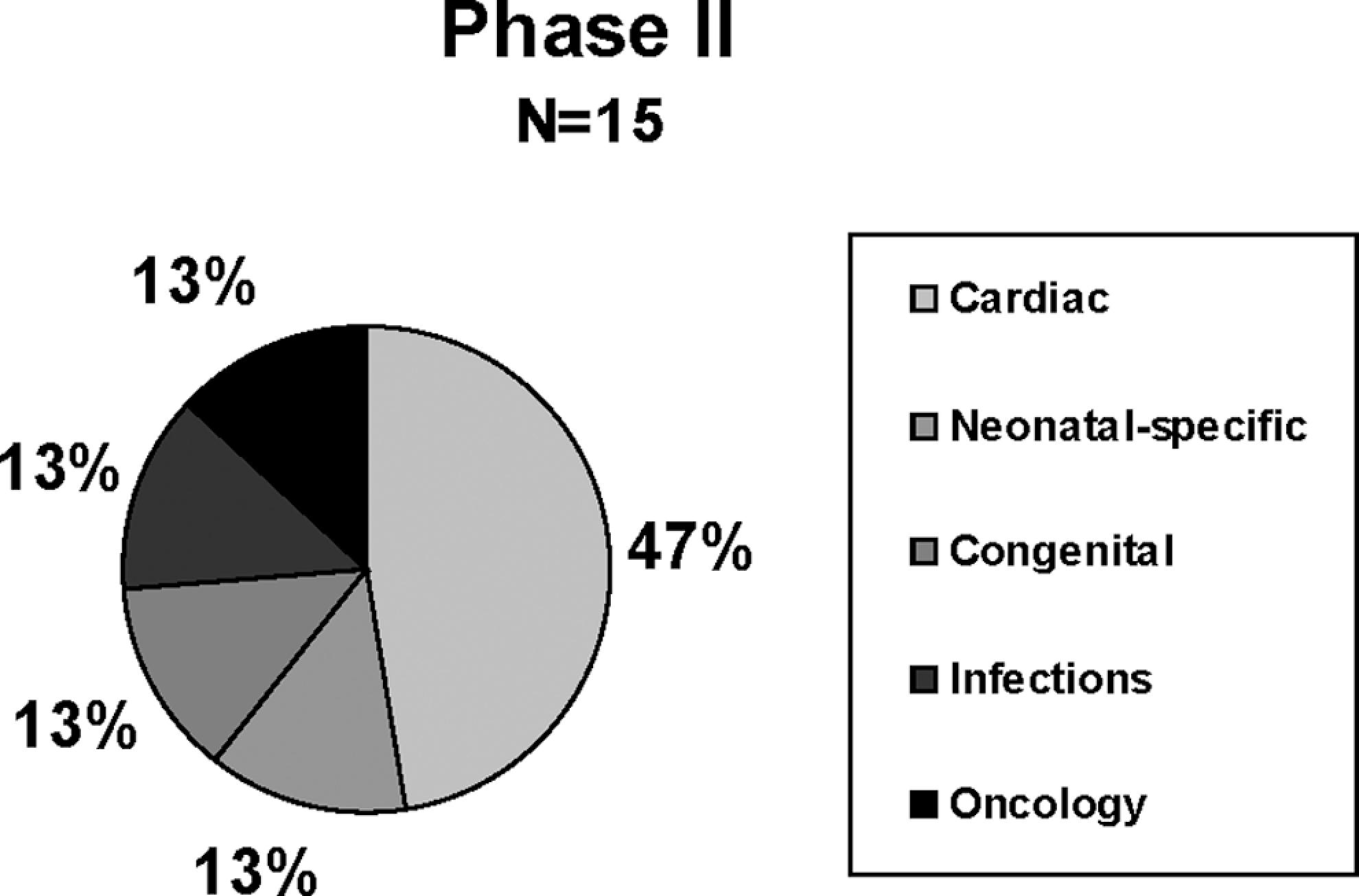
Diagnostic categories for phase II. Due to rounding, percentages total less than 100.
Location of Child’s Death.
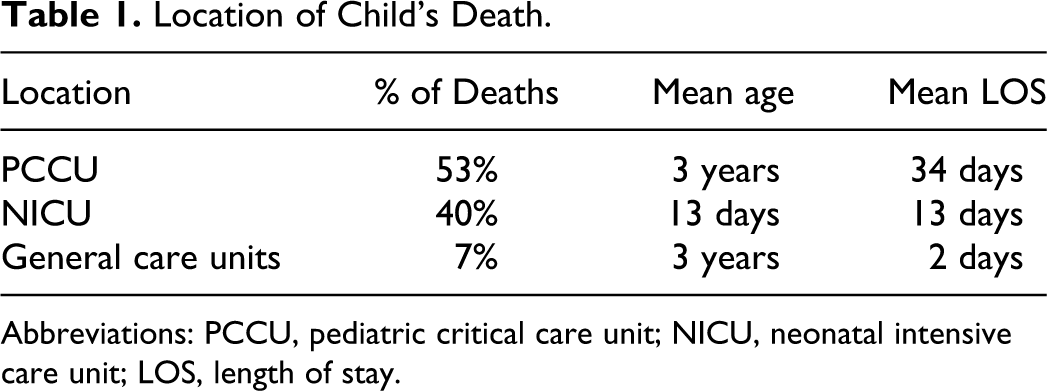
Abbreviations: PCCU, pediatric critical care unit; NICU, neonatal intensive care unit; LOS, length of stay.
Data Collection
The FAMCARE Survey was developed at the University of Manitoba, Canada, to measure family satisfaction with cancer care.
10
Approval was obtained from the FAMCARE authors for its use and adaptation for parental satisfaction with EOL care of children with input from 5 content experts. Categories of investigation coincided with categories of investigation of the chart review completed previously in phase I: (1) clinical management, (2) interdisciplinary family and child support, and (3) pain and symptom management. The adapted survey included a 10-item Likert scale with 5 data points—very satisfied, satisfied, undecided, dissatisfied, and very dissatisfied. It measured the degree to which family members were content with health care provider behaviors directed toward the care of their child and themselves. In addition, 3 EOL care-specific items were asked of parents: Were you, or your child, told of the imminent death? Were parental wishes and desires for your child’s care discussed with you, and by whom? Were you provided spiritual, emotional, and expressive therapy support?
Finally, 1 open-ended question asked the parent, “Is there anything you would like to add about the care (child’s name) received?”
Data Analysis and Results
Both quantitative and qualitative data were included in the analysis. Responses to the adapted FAMCARE Likert scale survey were analyzed, and themes which emerged from the responses to the semistructured questions were described. Data were collected during the telephone interviews, but some parents even wrote their responses (3-4 pages) and mailed them to the researchers after the phone conversations, although this was not requested. Two researchers independently coded data from the open-ended question through qualitative content analysis. Similar themes were clustered and preliminary categories emerged. Researchers reviewed the initial coding scheme, extracted quotes, and regularly discussed the rationale for emerging categories. Data were reexamined as additional interviews were analyzed until consensus was reached and no new categories emerged.
Quantitative Data
Survey results of parental satisfaction with care of their child at EOL are displayed in Table 2. All respondents indicated that they were satisfied or very satisfied with the availability of health care providers. Parents felt that physicians provided a thorough assessment of the status of their child. Of interest, however, is that 20% felt that they had not been included in decisions about their child’s care at EOL.
Survey Results: Parental Satisfaction With Care at Child’s End of Life.
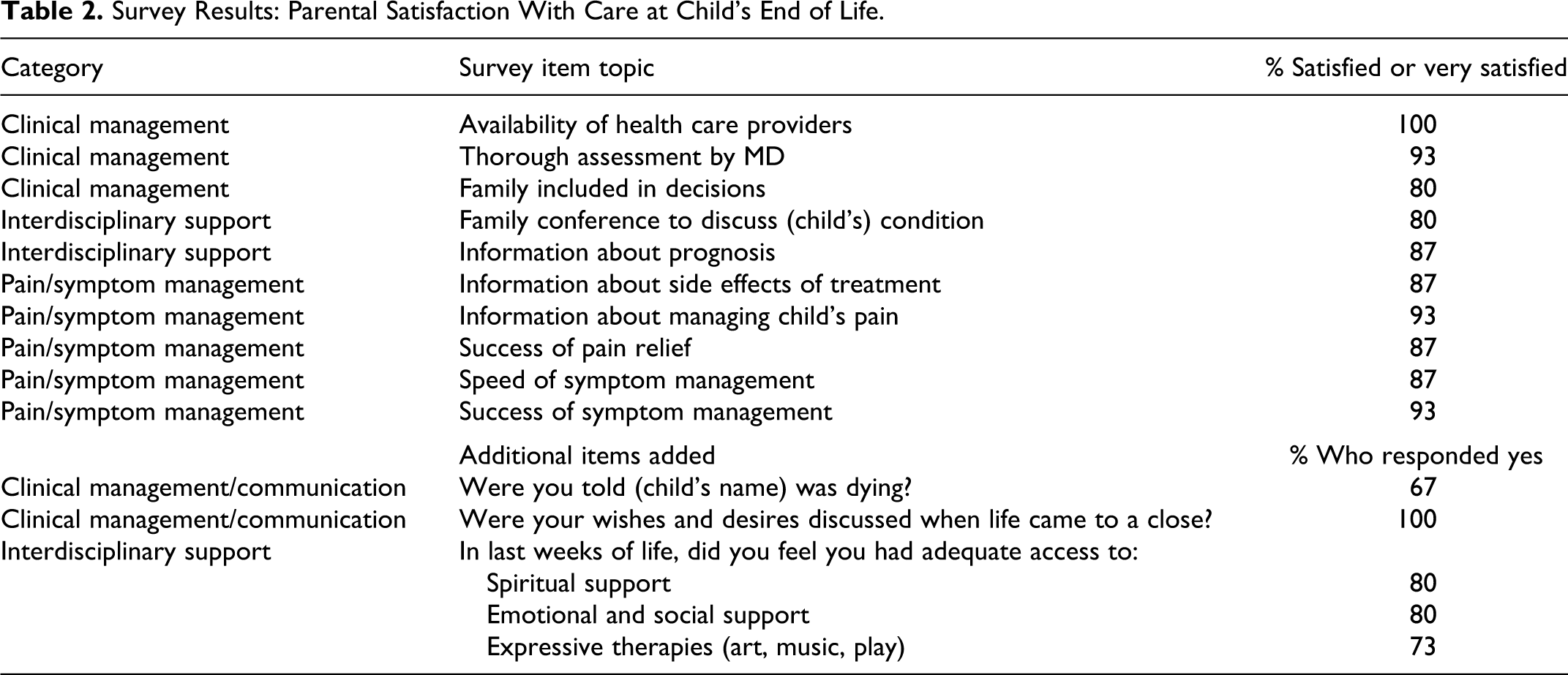
Eighty percent of parents interviewed were satisfied with family conferences which had occurred to discuss their child’s illness. Most participants (87%) also felt they received adequate information about their child’s prognosis. Most parents (93%) were satisfied with the relief of their child’s symptoms; however; parents were less satisfied with pain relief (87%) and the speed of symptom management (87%). Communication of information about managing the child’s pain (93%) was slightly higher than communication of information about side effects of treatment (87%).
After the survey, parents were also asked whether they were told their child was dying. Sixty-seven percent said they were told, and the 4 mothers who were not told indicated the child died very suddenly and without warning. One parent did not respond to this question. While interviewers asked whether the child was told she or he was dying, results were not included in this analysis, because most children in this sample were infants, so they were not informed about how sick they were. The 14 year-old and 3-year-old patients represented had advanced brain tumors, and the 8-year-old patient endured a cardiac arrest related to keto-acidosis; thus, these children were comatose during their last days. All families reported their wishes and desires were discussed most often with nurses and social workers, followed by physicians, and then chaplains. While most parents indicated they had adequate access to support, 2 mothers mentioned that support was offered but not recommended strongly enough.
Qualitative Data
Families graciously told their stories and were willing to help health care providers understand how they could improve the quality of care. Researchers independently identified themes in their responses. Content areas which emerged from the qualitative data included clinical management and communication, interdisciplinary child and family support, and pain and symptom management. Communication was added to the first theme as parents discussed the importance of that construct as a factor in clinical management.
Here are some of parents’ descriptive words:
Clinical management and communication. The whole nightmare culminated in the surgeon coming into the general waiting room to deliver the bad news. He just blurted it out in front of all of our family members and everyone else in the room…. And then we were left with the task of taking [child] off life support. No one came to talk to us. (mother of 14-year-old daughter) I actually don’t think any of the staff knew my daughter was close to death. (mother of 3-year-old daughter) Sometimes they would move [3 month-old son] arbitrarily and not tell us ahead of time. It would be unsettling to see another baby (or no baby) in his space and instantly, think he had died. (mother) They had a chaplain who knew some Spanish. They were able to communicate. (mother of 6-month-old daughter)
Interdisciplinary child and family support. When they knew [6-day-old] was dying, they gave us a chance to have every minute with her. Didn’t make us get out of the room, even at shift change. (mother of 6-day-old daughter) This experience would not have been bearable without the support of the nursing staff of the NICU. (mother of 2-month-old daughter) We were pleased with everything! We’ve always received GREAT care at [the hospital].(mother of 16-month-old son) I also want to say that the nurses were wonderful and that all physicians were really nice to us …. (mother of 5-month-old daughter) [Hospital] needs major work on palliative care issues with children who are seriously or terminally ill. No one was cluing into our situation. (mother of 3-year-old daughter) They took pictures of [dying infant], and we have those, which is nice. (mother of 6-day-old daughter) I love the cards I get in the mail from the hospital. I keep them all. My husband continues to read them over and over. (mother of 4-month-old son)
Pain and symptom management. At that time, I was very sick and I did not know what to do, but the doctor just wanted to get my son out of his way. I feel technology was bad, and I think miracles could happen. (mother of 2-week-old son) When [7½-year-old] symptoms flared up, some home care visits from the hospital would have been helpful close to end-of-life. (mother)
Discussion and Practice Implications
Parental feedback of their perceptions of the care provided at their child’s EOL is extremely informative. Comments from parents, such as those elaborated on the FAMCARE survey, may assist health care providers to maintain some of the care essential to help parents during the last days of their child’s life. Responses elaborated in this study addressing children of all ages and diagnoses are similar to previously reported themes found in other reports with different populations. Parent interviews in 1 study identified aspects of care important to parents: honesty, empowered decision making, parental care, environment, faith/trust in nursing care, physicians bearing witness, and support from other hospital care providers. 11 Hechler et al found that parents’ perspectives on their child’s death and related EOL decisions highlighted the importance of communication among parents and the health care team. 12 Other comments challenge nurses, physicians, and interdisciplinary providers to improve comprehensive care which includes better communication and clinical management, interdisciplinary child and family support, and pain and symptom management.
Clinical Management and Communication
Discussions related to changes in goals of care require interpersonal communication skills that are sensitive to families’ emotional distress. Members of the health care team can anticipate potential sources of stress and intervene accordingly. Examples of this important interaction involve keeping parents informed of new orders, changes in the child’s condition, or if their child will be moved to another location/room. Clinical management of the care for a child at EOL needs to be multidimensional, culturally based, and dynamic over the illness trajectory. 13 Research has shown that children often have fatigue, pain, anorexia/vomiting, dyspnea, cachexia, and drowsiness.4,14,15 Not all suffering caused by life-threatening medical conditions can be prevented and not all goals of families can be met, but communication about the plan of care and monitoring its implementation, as well as adjusting goals as needed, can go a long way to support the family through this very difficult time. At least 1 hospital-based model for pediatric palliative care has demonstrated the positive impact of focused communication and decision support on parental satisfaction and quality of life. 16 Nurses are in an ideal position to help coordinate this communication among members of the health care team, including interdisciplinary care providers, family members, and the ill child.
Interdisciplinary Child and Family Support
Family systems, as well as stress and coping theories, suggest that all family members are affected by a child’s life-threatening illness.17,18 The care of a seriously ill child can impact parents’ sleep, quality of life, and level of fatigue.19,20 Despite the risk of bereaved parents, little is known about how to best support parents of children at EOL. While parents reported satisfaction with the availability of health care providers, they were less satisfied with the quality of support they received for themselves. Health care providers report inadequate training, poor support from hospital administration, and overall discomfort managing EOL care for children and their families. Studies have shown that most health care providers learn about EOL care through trial and error. 21 Health care providers should strive to implement national clinical practice guidelines and develop and implement institutional protocols and procedures for EOL care. 22 Education about legal and ethical underpinnings of EOL experiences is crucial toward improving the care of these vulnerable families. 23 Curricula in undergraduate education that provide a basic foundation of knowledge about pediatric palliative care are essential as work continues to change the organizational climates to embrace the care of dying children. Some caregivers have been fortunate enough to have good role models, but clearly, educational experiences that begin early can help. Graduate education that does include pediatric palliative care should include specific attention to dying children’s EOL, as this sensitive time period is often overlooked in curricula.6,24–26 Nurses need to provide interdisciplinary educational experiences and role-modeling in communication with families in palliative, EOL, and bereavement care. By itself, education cannot guarantee desired changes in attitudes or behaviors, but it must provide the essential foundation of scientific knowledge, skills, and ethical understanding for all professionals who treat infants, children, and adolescents.
Pain and Symptom Management
Effective prevention, timely assessment, and treatment of physical and psychological symptoms and other forms of distress have been recommended by the Institute of Medicine, as parents in other national surveys have cited their frustrations in coordinating the care needed by a very ill child. 6 Quality of life is a multidimensional construct which includes physical and emotional pain and symptom management. Researchers have suggested for many years that physicians inadequately prescribe analgesics, and nurses may also play a role in minimizing children’s pain.27–29 Proxy reports are helpful, but parents may not adequately describe multiple domains of comfort at EOL. The validity of proxy measures in palliative care has been questioned. 30 Tasks such as reducing the burdens of care coordination and improving the continuity of care present challenges in managing children with complex conditions. Nurses who are at the bedside are in a key role and can make important contributions to management of the child at EOL. They can open the door for family members to share their perceptions about the care their child is receiving. Even though some proxy measures have been questioned, parents have a great deal to offer in assisting health care providers in understanding ways to care for children and their families during their last days of life. 30 Parents have insight nurses may find beneficial in improving care at EOL, but parents may be reluctant to offer their perceptions unless asked.
Conclusions
This study found through the use of both quantitative and qualitative methodologies that parents can have positive feelings about their child’s EOL care in the modern tertiary children’s hospital setting. Findings indicate that families were pleased with the overall bedside symptom management, communication with nurses, and communication in family conferences when experienced. However, the finding that many parents desired to have greater active involvement in decision making about their child’s EOL care deserves further study and may have implications for caring for future children and their families. A representative sampling of parents contributed to this study—from across hospital units of care. The diagnoses and location of EOL care in these patients were diverse and indicated a representative sampling of the families of children previously reported (Figures 1 and 2). 9 An additional strength of the study was that interviews were conducted by a hospice agency outside of, and unaffiliated with, the hospital—thus minimizing bias and any real or potential conflict of interest in the responses of participants.
Clearly, opportunities exist to enhance communication and deliberations regarding goals of care as they transition at EOL. This study is limited by its retrospective design and the small sample size. Small sample sizes and low return rates among eligible parents are characteristic of similar published studies.11,12 It is conceivable that a biased sampling was obtained in this study, though that was not the intent, as parental participation may have reflected parents having a favorable opinion of their child’s EOL care. Nonetheless, qualitative responses indicate balanced experiences in this cohort. The difficulty in recruiting participants using an opt-in approach for families may have posed an undue burden in acquiring a larger sample. Future studies could request potential participants to “opt out” of the study by sending a card to request they are not queried by telephone or contacted through the mail to participate. The use of a response card in this study was made in an effort to not be intrusive with this vulnerable bereaved population, but a future opt-out design may result in an improved response rate.
This study provided parental insight into the care of their children at EOL. Further research is needed to learn more about pain and symptom management and quality of life from the child’s perspective at EOL. In addition, more work is needed from multiple informants regarding the perceived care of children at EOL. This may include a longitudinal study, looking at perceptions 6 months, 12 months, and 2 years after the death of a child. Interviews with both parents in a family may also result in a more complete analysis of perceptions. This first multimethod step toward learning more about perceptions of palliative care at EOL can lead to future improvement in the management of care, interdisciplinary team support, and pain and symptom management.
Footnotes
Acknowledgment
This work was supported in part from a grant from the Initiative for Pediatric Palliative Care, Center for Applied Ethics and Professional Practice, Educational Development Center. We appreciate the contributions of Matt Howenstein and Emily Brown to the chart review process and to the staff at Alive Hospice for their assistance with the interviews. We are deeply indebted to the families who gave from their hearts in efforts to improve the care of children with life-limiting conditions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.