
Abstract
Emergency department (ED) visits are made by cancer patients for symptom management, treatment effects, oncologic emergencies, or end of life care. While most patients prefer to die at home, many die in health care institutions. The purpose of this study is to describe visit characteristics of cancer patients who died in the ED and their most common chief complaints using 2008 ED visit data from the North Carolina Disease Event Tracking and Epidemiologic Collection Tool (NC DETECT). Of the 37,760 cancer-related ED visits, 283 resulted in death. For lung cancer patients, 104 died in the ED with 70.9% dying on their first ED visit. Research on factors precipitating ED visits by cancer patients is needed to address end of life care needs.
Background
Emergency departments (EDs) face overcrowding while simultaneously coping with the increasing clinical needs of patients with acute and chronic illnesses such as cancer. 1 Cancer is the second leading cause of death in the United States, with an increasing number of older adults with cancer having complex health needs. 2 Better treatments and supportive care are prolonging life among patients with cancer, resulting in an increased number of ED visits for symptom management and end-of-life cancer care. 3 In addition to addressing the acute care needs of patients, EDs have become a place where chronic conditions are managed, including palliative treatment for serious ongoing health problems. Medical efforts are made to alleviate symptoms and, at times, initial discussion of end-of-life care planning may be addressed during the ED visit.
Excessive use of EDs by patients with cancer at the end of life may be indicative of limited services in the community (eg, home health or hospice). For example, respiratory distress is a common presenting symptom for patients with cancer, specifically patients with lung cancer, which can be a difficult event for both the patient and family members. 4 Although studies have described end-of-life care in the ED, 5,6 little is known about presenting chief complaints (CCs) of those who actually die in the ED. The purpose of this study is to describe patient and visit characteristics of patients with cancer who died in EDs in North Carolina (NC) during 2008, using data from the NC Disease Event Tracking and Epidemiologic Collection Tool (NC DETECT).
Methods
Using population-based ED visit data from NC DETECT, we performed a descriptive analysis of visits occurring in 110 of the 112 civilian, acute care EDs in NC during 2008. This study received institutional review board (IRB) exemption after a data use agreement was completed. The 2008 NC DETECT ED visit data set was obtained with de-identified patient data. The study sample included ED visits with a diagnosis of cancer, identified using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), listed in diagnosis position 1 through 5. Further details on the sampling procedures are described in Mayer et al. 7 Analyses included descriptive statistics for visit demographics including sex, age, insurance, cancer type, visit category (hour, day of week, and month). The chief complaint (CC) is a brief free-text statement of the patient’s reason for the visit to the ED. The CCs were cleaned and categorized manually. Since CC categories were not exhaustive, nor completely inclusive (ie, some CCs were left uncategorized), counts and percentages are approximate for CCs. Available triage notes, which provide an expanded reason for visit and history of present illness, were also analyzed when available for more detailed clinical information regarding the visit.
Results
All Cancers
In 2008, there were 4 190 911 ED visits captured in NC DETECT and, of those, 37 760 had a diagnosis of cancer. Of the cancer-related ED visits, 283 resulted in death. Of the cancer patients who died, 201 (71%) died on their first visit, 52 (18.4%) died on their second visit, 17 (6.0%) on their third visit, and 13 (4.6%) on their fourth, fifth, or sixth visit (Table 1). Males accounted for 177 (62.5%) of cancer-related ED deaths and the average age at death was 66 (standard deviation [SD] 14.3) years. More than half (56.2%) of cancer visits resulting in death had an ICD-9-CM code for cancer listed in diagnosis position 1 or 2. By cancer type, 104 (36.7%) of cancer-related ED visits resulting in death had an ICD-9-CM code for lung cancer, while ICD-9-CM codes for breast, prostate, and colorectal cancer were listed in only 2.1%, 2.8%, and 7.1% deaths, respectively. Almost half (47.3%) of the 283 cancer visits resulting in death had Medicare listed as their expected source of payment.
Characteristics of Cancer ED Visits Resulting in Death (N = 283), North Carolina, 2008.
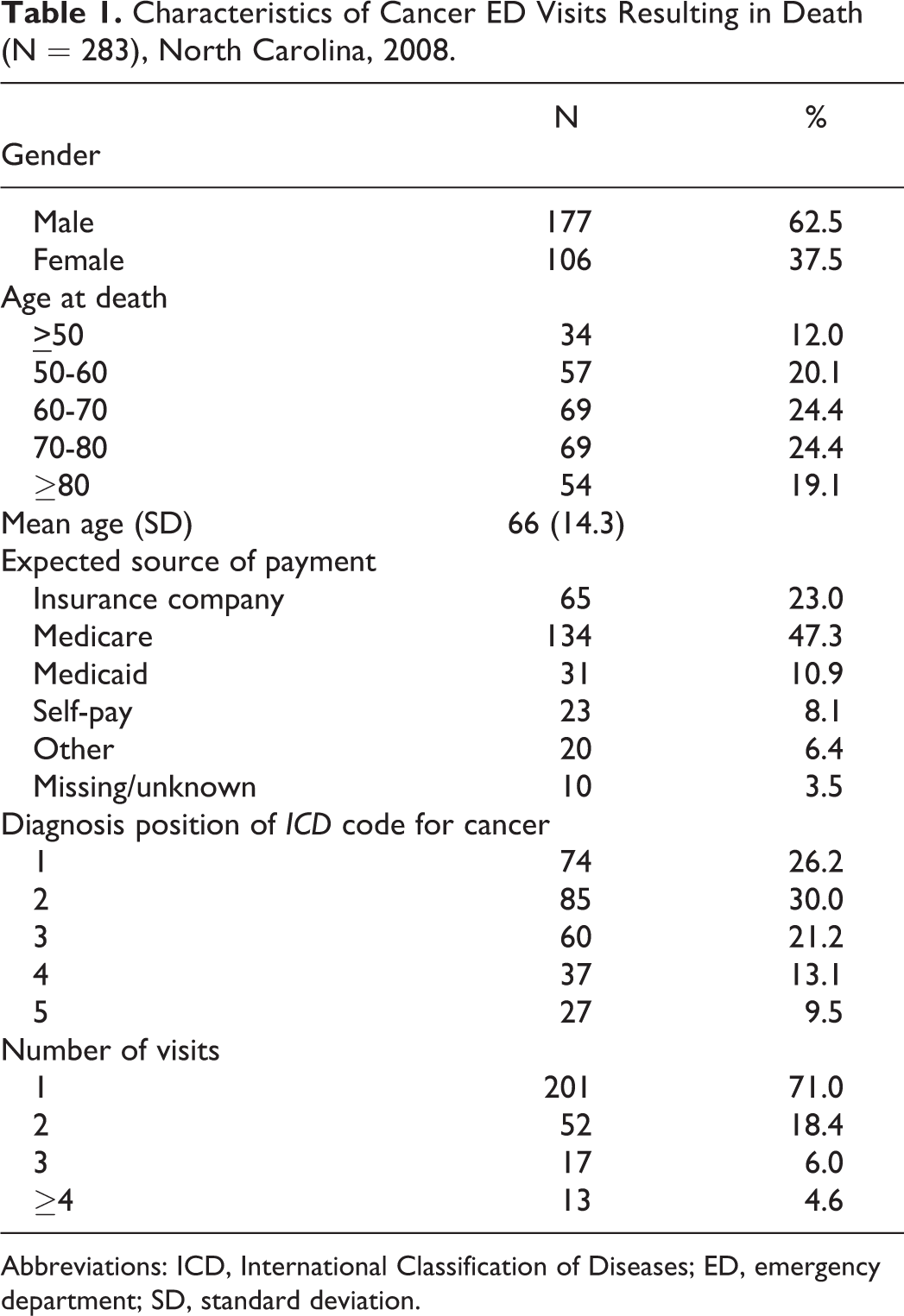
Abbreviations: ICD, International Classification of Diseases; ED, emergency department; SD, standard deviation.
The ED visits were also categorized by hour of day, day of the week, and month of year in 2008. Cancer-related deaths in the ED occurred most frequently in April or June (10.6%, respectively) and on Fridays (17.3%). Time of arrival to the ED was observed most commonly at 10 to 11
The CCs were available for 258 patients (92%) and were clustered using major categories (Table 2). Some of the ED visits had more than 1 CC listed and all were included in Table 2. The most common CCs noted by patients with cancer included respiratory (17.6%), gastrointestinal (16.2%), and neurological (14.1%; Table 2). The most common CC among patients with lung cancer was respiratory distress. Twenty-five patients who died were missing CC data (8%). Eighty-one (28.6%) patients with cancer who died in the ED had CCs recorded and were either actively being resuscitated or dead on arrival(DOA) when they arrived to the ED, as recorded in the CCs (Table 2).
Frequency of Categorized Chief Complaints Among Cancer ED Visits Resulting in Death (N = 283), North Carolina, 2008.
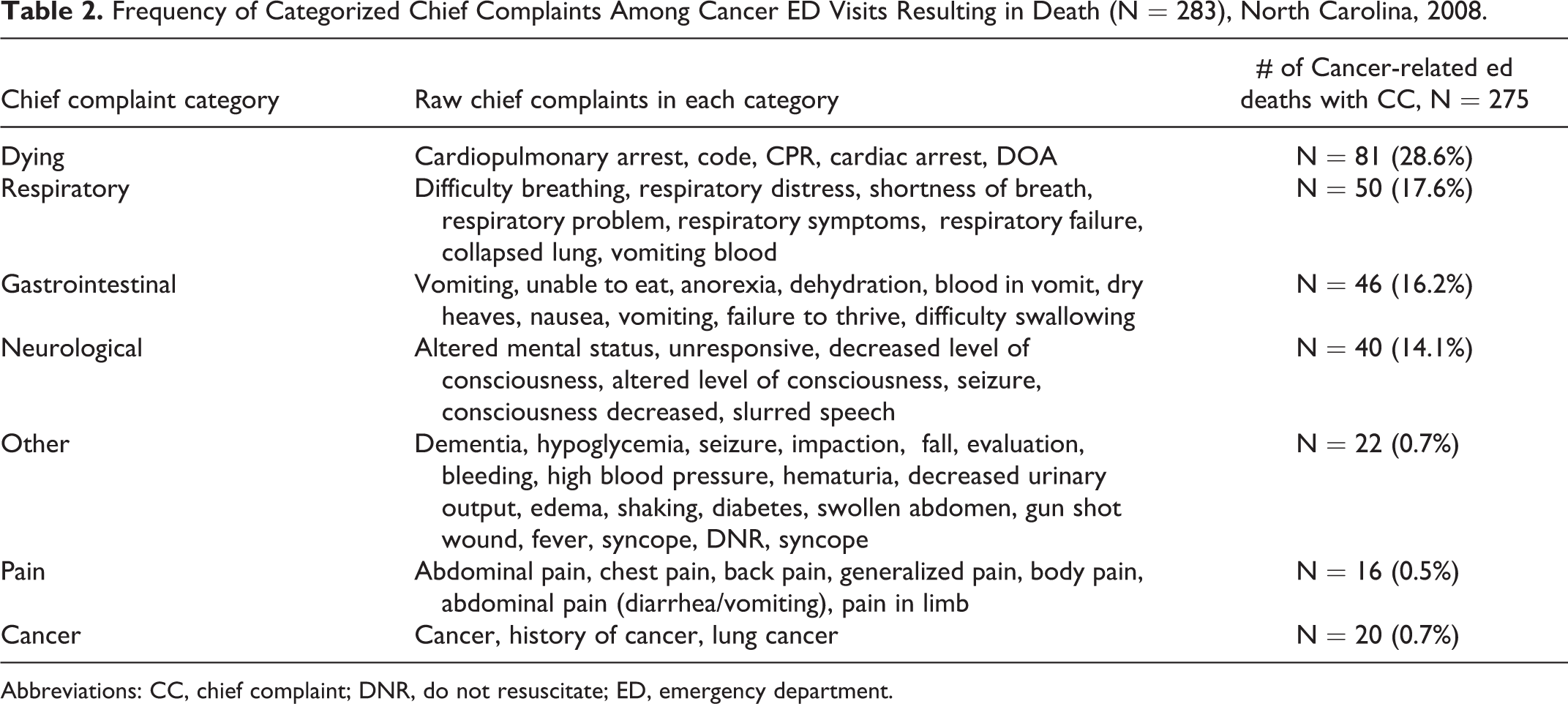
Abbreviations: CC, chief complaint; DNR, do not resuscitate; ED, emergency department.
Triage notes were available for 57 (20%) of ED deaths since many EDs did not submit triage notes electronically into NC DETECT. When available, the triage notes provided much more detail about the reasons for the visits than CC. Most factors leading to ED visits at the end of life included respiratory distress, mental status changes, unresponsiveness, or cardiac arrest, as described by the family member or nursing staff. Some patients had hospice care or do not resuscitate (DNR) status documented in the triage notes (n < 10).
Lung Cancer
In the 2008 NC DETECT ED visit data, 10 308 ED visits had an ICD-9-CM code for lung cancer in diagnosis position 1 to 5 (Table 3). 7 Among these lung cancer-related visits, 104 (1.0%) resulted in death, while 9627 (93.3%) did not (excluding 577 visits where discharge information was not available). Among the 104 patients with lung cancer who died in the ED, 74 (71%) died on a first visit, 17 (16.5%) on a second visit, and 13 (12.5%) on a third or subsequent visit. Further, 68 (65.4%) were male with a mean age at death of 64.7 years (SD 13.3).
Characteristics of Lung Cancer ED Visits, North Carolina, 2008.
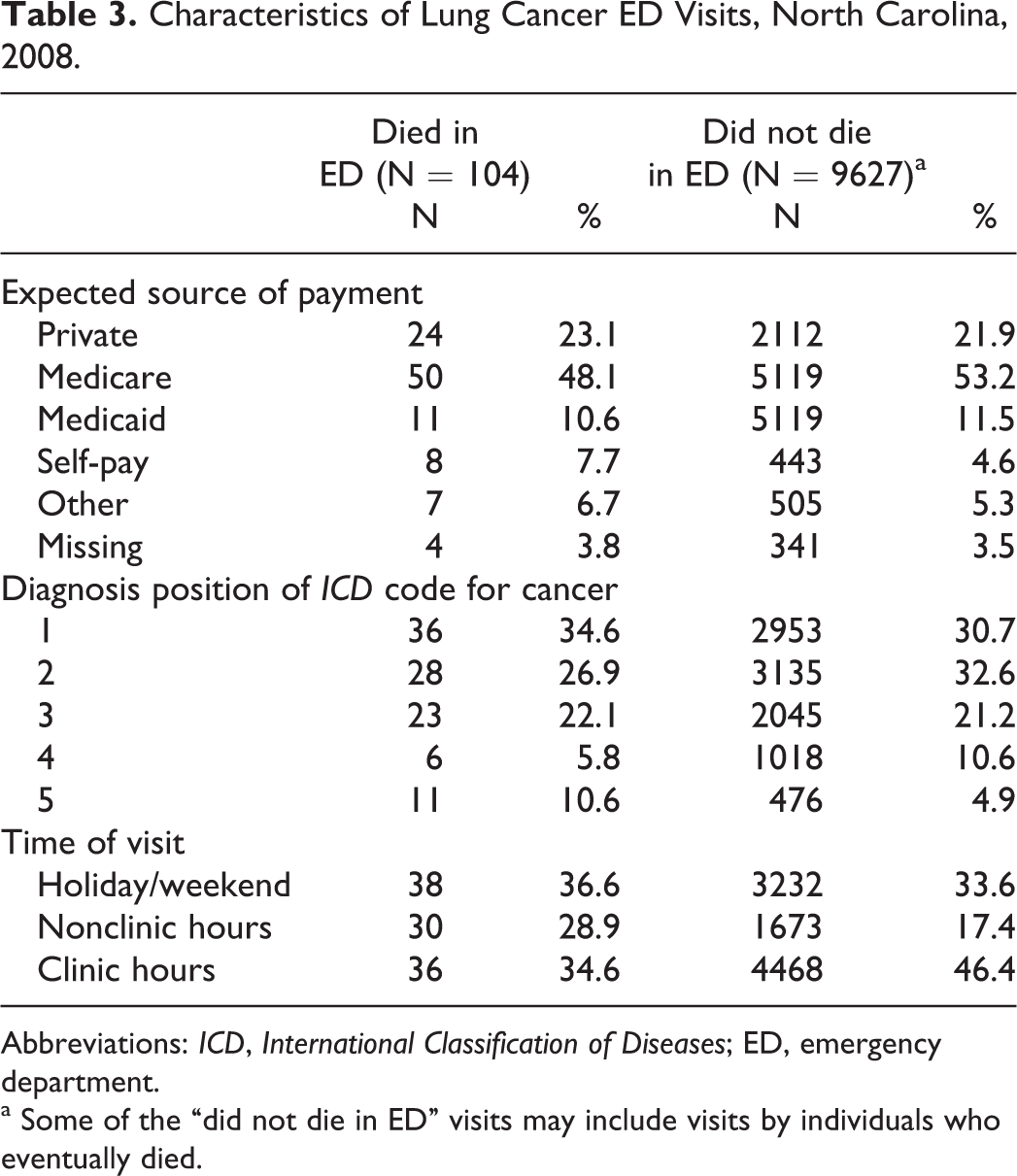
Abbreviations: ICD, International Classification of Diseases; ED, emergency department.
a Some of the “did not die in ED” visits may include visits by individuals who eventually died.
Discussion
To the best of our knowledge, this is the first study to describe visit characteristics of patients with cancer who died in the ED. An emergent event led these individuals to the ED, with the most commonly cited CC being respiratory distress. The 3 most common CC categories among patients with cancer who died in the ED were respiratory, gastrointestinal, and neurological. These findings are similar to other studies that explored common reasons for patients with cancer visiting the ED, with the most common reason being respiratory distress/dyspnea. 4,8 Given that the frequency of respiratory distress was high in those who died, the potential of a pulmonary embolus (PE) or venous thromboembolism (VTE) in this cancer population must also be considered. One plausible reason for a change in respiratory status may be the sudden onset from a PE or VTE. Venous thromboembolism is the second leading cause of death in patients with cancer, and this likelihood increases with older age, those receiving treatment, recurrent PEs or VTEs, and those with limited mobility. 9,10 It is also important to note that respiratory distress is often a clinical indication of disease progression, such as advanced lung cancer or exacerbations of dyspnea. 4
Lung cancer is the second most common malignancy and second leading cause of cancer death in the United States for both men and women. As lung cancer progresses, physical functioning declines and activities of daily living require maximum patient support,
11,12
so understanding respiratory distress is important for optimizing symptom management. The majority of patients with lung cancer who died (n = 104) were male (65%), older (64.7 years), and almost half (49%) listed Medicare as their source of payment. Most of these visits occurred on the weekend or during clinic hours. Our findings are consistent with Kurtz et al
13
who reported patients with lung cancer are more likely to be male,
The symptoms of patients with cancer can be managed by a palliative or hospice care team (eg, respiratory distress, nausea, and vomiting) who have expert knowledge in caring for dying patients. The expertise of these specialty teams could potentially reduce the number of patients who come to the ED for end-of-life care needs. Patients who die in the hospital or intensive care unit have increased physical and emotional distress compared to those who die at home. 14 The patient’s preference for location of death and the actual place of death is often incongruent. A few studies have investigated this contrast; 50% to 90% of individuals preferred to die at home, while 50% to 60% actually died in the hospital. 15 –18
There were variations in the time of arrival to the ED, with a third occurring on the weekend and over a third during weekday clinical hours. Potential reasons that visits resulting in death occurred on the weekend include emergent situations that could not be managed at home or in the clinic or reduced resources such as transportation. The ED visits resulting in death during clinic hours may be explained by a patient or caregiver perception that the medical situation is too severe to be managed in a doctor’s office or clinic, hence the reason for the ED visit.
The major strengths of this study include a large, comprehensive population-based data source (N = 27 760 cancer-related ED visits) that was representative of NC (all 100 NC counties and 110 of 112 hospital-affiliated acute care EDs), which provides a detailed description of those who died in the ED (N = 283). Systematic data captured electronically and automatically by NC DETECT, including concrete clinical information, was also an advantage. With any study there are limitations, and our primary limitation was the difficulty in defining ED visits as cancer related. Due to the varying nature of cancer, we may have missed visits that were cancer related or included some visits that were not cancer related, depending on how distally or proximally related the cancer diagnosis was to the reason for the ED visit. The researchers attempted to examine this issue through analyses of diagnosis positions and V-codes. 7 Another limitation was defining CC categories. As noted above, CC categories were not exhaustive nor were CCs within a given category completely inclusive, leaving some CCs uncategorized. Therefore, counts and percentages are only approximate. A third limitation included analyzing data for 1 year (2008) instead of multiple years to assess utilization of ED services and ED deaths. Multiple years of data could potentially be used to discern whether patients who died in the ED in 2008 utilized the ED before this fatal event.
Other challenges included location of patient before ED admission (eg, home, long-term care facility, oncologist office, outpatient clinic). Mode of transportation to the ED was missing for about 20% of all visits overall. Platts-Mill et al 26 examined ED disposition using the NC DETECT ED visit data and found approximately 60% of patients >85 years used Emergency Medical Services (EMS) transport from their location to the ED, with an increase in age associated with increased use of EMS. Although triage notes were available for some patients who died and provided some detailed accounts of the arrival mode, location of patient before admission to ED, type of cancer, and reasons for ED use, the triage notes lacked uniformity and detailed accounts that could inform a more comprehensive clinical picture of the emergent situation. Further research linking population-based studies with administrative claims data can augment the biases and limitations of the findings. 27 Identifying quality performance measures using SEER-Medicare or other administrative data to capture and profile quality indicators at end of life for patients with cancer may address the NCI research agenda focused on cancer outcomes research. 3,28
Identification of gaps in resources and services for patients with cancer is the first step in addressing areas for improving the quality of cancer care. Seow and colleagues 19 found early homecare utilization and services were strongly associated with fewer acute care services in a population-based cohort study. Randomized-controlled studies support this association; a reduction in acute care services at the end of life was primarily related to palliative care and homecare services focused on symptom management and family education. 20 –22
Conclusion
Our study provides a description of patient and visit characteristics of cancer patients who died in the ED. More research is needed to understand precipitating factors in order to identify strategies for finding alternatives to the ED as the place of death when possible, especially among patients with lung cancer. Were family members or health professionals unable to manage the symptoms that precipitated the ED visit? If so, educating family members, caregivers, and medical staff is critical in ensuring they understand the changes that might occur at various times during the illness trajectory, including at the end of life.
Assisting the caregiver and health care facility to expect and manage the changes (eg, change in respiratory rate and depth, altered level of consciousness, and fatigue) at the end of life will help them recognize that this is an expected response and may not always require an ED visit. Preparation for end of life can be distressing but can lead to a more peaceful death for the patient. 23 Providing awareness and education are important roles for health professionals, and encouraging family members to consider advanced directive planning and discussion about code status will assist in facilitating medical decision making. Surprisingly, only a small percentage of patients with cancer actually complete an advanced directive before their death. 24,25 Informing and educating all members of the health care team, including the patient, about this gap in long-term planning may potentially narrow this clinical and legal divide.
This study has implications for health professionals as they assist patients and their caregivers in anticipating emergent situations, preparing for death, and other concerns associated with end of life. Patients with cancer have the right to die in an optimal location for appropriate end-of-life care. Ensuring that patients with cancer receive quality end-of-life nursing care is essential in any setting, including the ED. More needs to be understood about precipitating factors that lead to these visits.
Footnotes
Acknowledgments
The authors would like to thank Clifton Barnett, MSIS, NC DETECT Data Quality Specialist for his assistance with this project.
Declaration of Conflicting Interests
The authors declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the NC TraCS Institute (TRaCS Award 2KR30903) and UNC’s NIH Clinical and Translational Science Award from the National Center for Research Resources (UL1RR025747) and National Cancer Institute 5R25CA116339. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.