
Abstract
Background:
In Muslim countries, end-of-life practices in Muslim brain-dead patients are unknown. We conducted this study to evaluate this issue.
Results:
We identified 42 brain-dead patients between 2001 and 2011. The expectant terminal extubation occurred only in 5. Largely due to family opposition, 2 patients remained “full code,” and rests were “do not attempt resuscitation” with varying usage of “life-sustaining” therapies. Only 2 out of 24 eligible patients donated organs. There was minimal involvement of social worker, palliative team, or Muslim chaplain in the end-of-life discussions.
Conclusion:
In Muslim patients, the concept of terminal withdrawal and organ donation after brain death is still not well accepted. Future multicenter studies, involving palliative teams, should focus on improving these issues.
Introduction
The idea of brain death after its introduction in 1959 by Mollaret and Goulon has evolved into a commonly accepted concept, even though there may be disagreement on the particulars of specific diagnostic criteria. 1,2 In United States, the first guidelines to diagnose brain death in patients were formulated in 1968 and were later followed by other countries with some differences. 3,4 The current diagnostic practices in United States are mainly derived from the “The American Academy of Neurology” guidelines 5 and specific protocols are individualized by the institutions. 6
The first religious ruling among Muslims equating brain death as whole body death came as a result of the Third International Conference of Islamic Jurists in 1986. 7,8 The Fourth Session of Council of the Islamic Jurisprudence Academy in 1988 allowed (under certain conditions) the retrieval of organs from brain-dead patients. 8,9 This did pave the way for partial acceptance of organ transplantation in Muslims. 10,11 However, the controversy surrounding the issue has not, by any means, settled to date. There have been numerous subsequent assessments in this regard by different Muslim organizations, and these have varied in their determinations and remain controversial. 12 Some Islamic scholars and organizations consider futile measures to be inappropriate in terminal patients, while others would want everything to be done for the patient under any given circumstances. 12 –15 These conflicting opinions have an impact on the individuals and cause confusion among the families of the brain-dead patients. Social attitudes and beliefs also differ from one society to another and sometimes overwhelm the medical and religious aspect of decision making. 16,17 The combination of all these factors could influence the treatment after brain death determination of Muslim patients. 16,18
Even though we have some data regarding religious beliefs and social issues in terminal Muslim patients, there is scarcity of information regarding the end-of-life practices and extent of medical care delivered to them before and after brain death confirmation. End-of-life practices in brain-dead patients in United States and Europe are usually protected by medicolegal laws, which allow them to harvest consenting donors and immediately take others off life support even without family’s consent. Such medicolegal laws are lacking in Muslim countries, including Saudi Arabia, despite the abundance of supportive religious rulings or “fatwas.” 19 This can put the physicians in Muslim countries in a tricky situation where withdrawal of care in brain-dead cases without “legal” backing could be problematic and more so when patients’ families are in disagreement.
We conducted this study to evaluate the above issues among Muslim brain dead patients in our hospital in Saudi Arabia, particularly looking at the aspects of withholding and withdrawal of therapies in them.
Methods
The ethical and scientific approval for the study was granted by the Institutional Review Board of the hospital. The study was conducted at King Faisal Specialist Hospital & Research Center, Jeddah. The hospital is a 320-bed nontrauma tertiary care referral hospital. The intensivists, internists, neurologists, and neurosurgeons in the institution are trained and board-certified North Americans. They are the ones predominantly involved in the overall medical care of the patients who end up being brain-dead. However, because of a “closed” intensive care unit model, the attending intensivists are the ones who manage and are fully responsible for the end-of-life care in the brain-dead patients. All the intensivists were involved in terminal withdrawal of brain-dead patients during their training and practice in North America before coming to Saudi Arabia.
Data Collection
The data were collected retrospectively. The information was gathered from the electronic medical records and patient’s files. Because of convenience in accessing the medical records from 2001, data were collected from January 2001 till August 2011.
Diagnosis of Brain Death
To define brain death in our study patients, we followed our institution guidelines. In our hospital, the definition and diagnosis of brain death is derived in a modified form from the 1995 American Academy of Neurology guidelines. 5 Brain death is determined to be present when there is acute and irreversible cerebral nervous system insult with the absence of all brain and brain stem functions. This is confirmed by 2 attending physicians on 2 separate occasions by clinical examination. The interval between the 2 tests is supposed to be 24 hours; however, the second clinical testing can be done after 6 hours in adults if an ancillary test is positive. Apnea test is a mandatory requirement. An ancillary test, either an electroencephalogram or a cerebral perfusion scan, is also compulsory. Once there is documentation of 2 clinical examinations reflecting no brain and brain stem functioning, combined with an apnea test and an ancillary test, only then the patient is declared as brain-dead.
Inclusion and Exclusion Criteria
All Muslim adult patients (18 years or older) who were declared brain-dead as per the above definition during the 10-year study period were included. We did not differentiate Muslims based on their sect. Those patients who were in a persistent vegetative state or coma, those without at least 1 clinical confirmation examination of brain death, patients younger than 18 years old, and those with no apnea test or ancillary testing confirmation according to the institution’s guidelines were excluded.
Parameters Collected
The data were gathered on all the brain death patients including their age, gender, underlying etiology causing brain death, admission Glasgow coma scale, diagnosis of brain death, therapies including nutrition delivered before and after brain death, withholding or withdrawing of treatment, code status, terminal withdrawal after confirmation of brain death and organ donation. Withholding treatment was defined as a decision that included not to start or increase a life-sustaining intervention (excluding cardiopulmonary resuscitation [CPR] which was assessed independently). Withdrawing treatment was defined as a decision that was made to actively stop a life-sustaining intervention being given.
Data Analysis
The data were evaluated in terms of descriptive statistics, and the results reported as such or in percentage. Results were analyzed using “unpaired t test,” or “Pearson chi-square test,” as appropriate.
Results
Patients
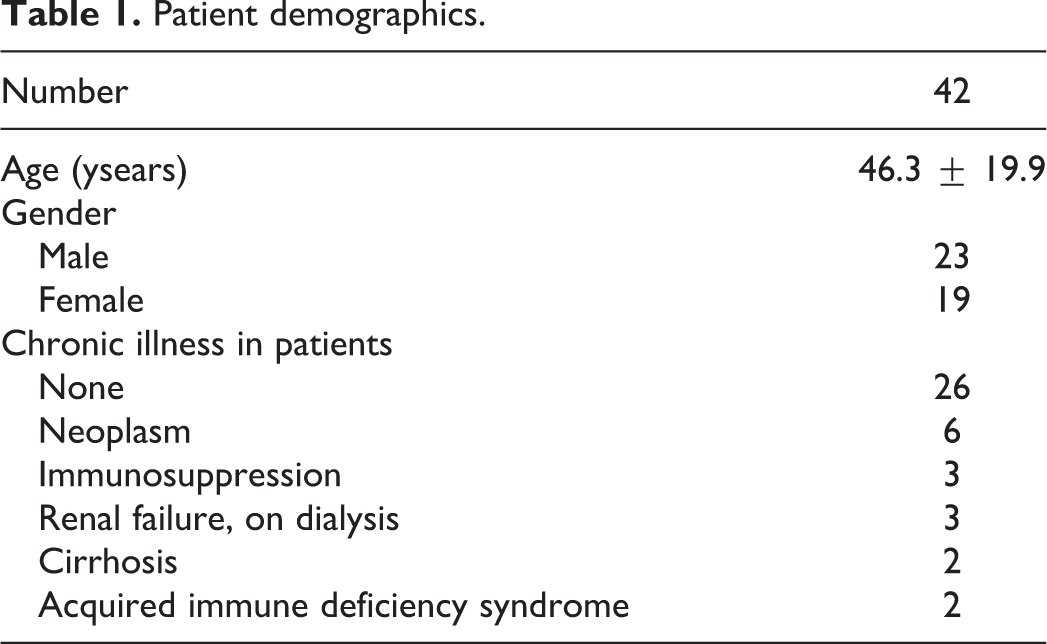
There were a total of 2908 deaths in the study period. Out of these, 42 patients (1.4%) who met the study criteria were identified and included in the analysis. The mean age was 46 years and there was no difference in gender. More than half of the patients had no known preexisting chronic illness (Table 1). The patients were admitted to the hospital either via emergency room or by direct transfer from another hospital.
Patient demographics.
Diagnosis of Brain Death
Five patients expired before completion of the second clinical confirmatory test but did fulfill all other prerequisites for brain death diagnosis. In rest of the patients, for completion of the brain death protocol, 1 attending physician was always the intensivist and the second physician was a neurologist (64%) or a neurosurgeon (36%). The average time from admission to the diagnosis of brain death was 7.83
Etiologies of Brain Death and Therapies Used
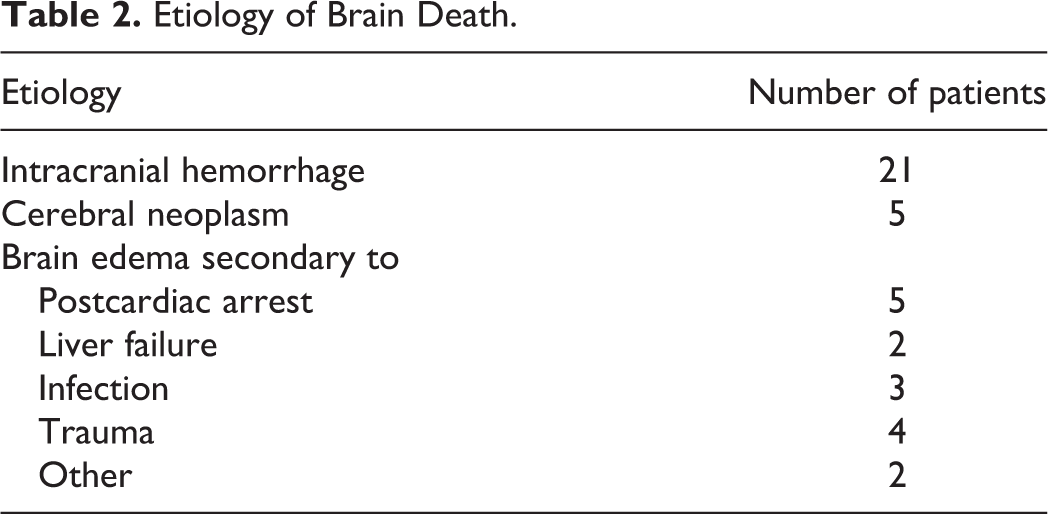
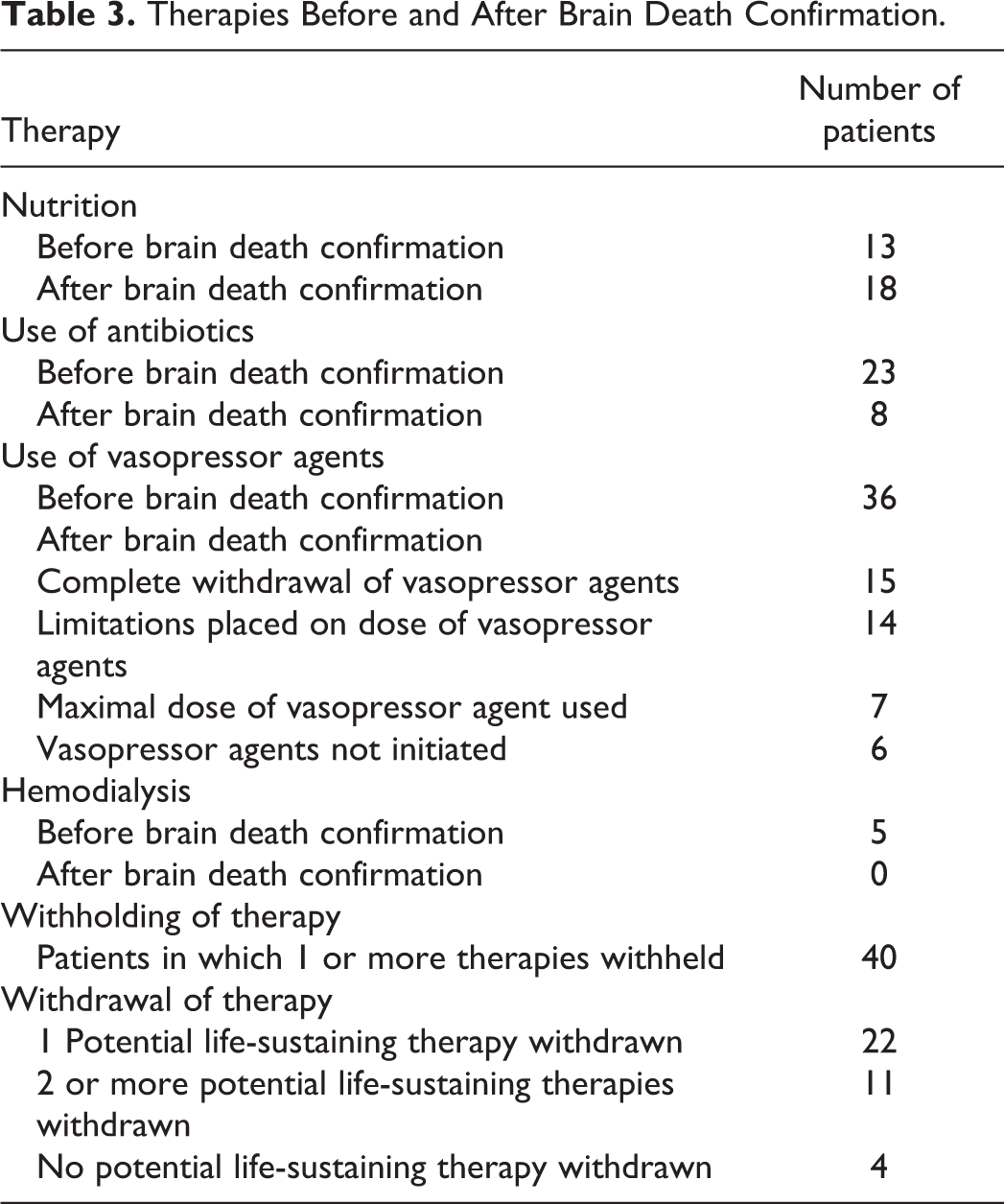
The different etiologies causing brain death are listed in Table 2. The predominant reason of brain death was intracranial hemorrhage. These patients had the worst presenting GCS score as compared to other etiologies (P < .0001). All the patients who were diagnosed as brain-dead were obviously intubated and supported by mechanical ventilation. Four therapies including vasopressor or inotropic agents, antibiotics, nutrition (including enteral nutrition and/or intravenous fluids), and dialysis were identified as life-sustaining therapies. There was variable utilization of vasopressor agents, from none to maximal dose of a given agent (Table 3). There was a tendency to discontinue or limit the use of antibiotics, vasopressor agents, and hemodialysis after the brain death confirmation but not nutrition (Table 3). The use of antibiotics was strongly associated with the use of vasopressor agents (P = .003).
Etiology of Brain Death.
Therapies Before and After Brain Death Confirmation.
End-of-Life Care After Brain Death
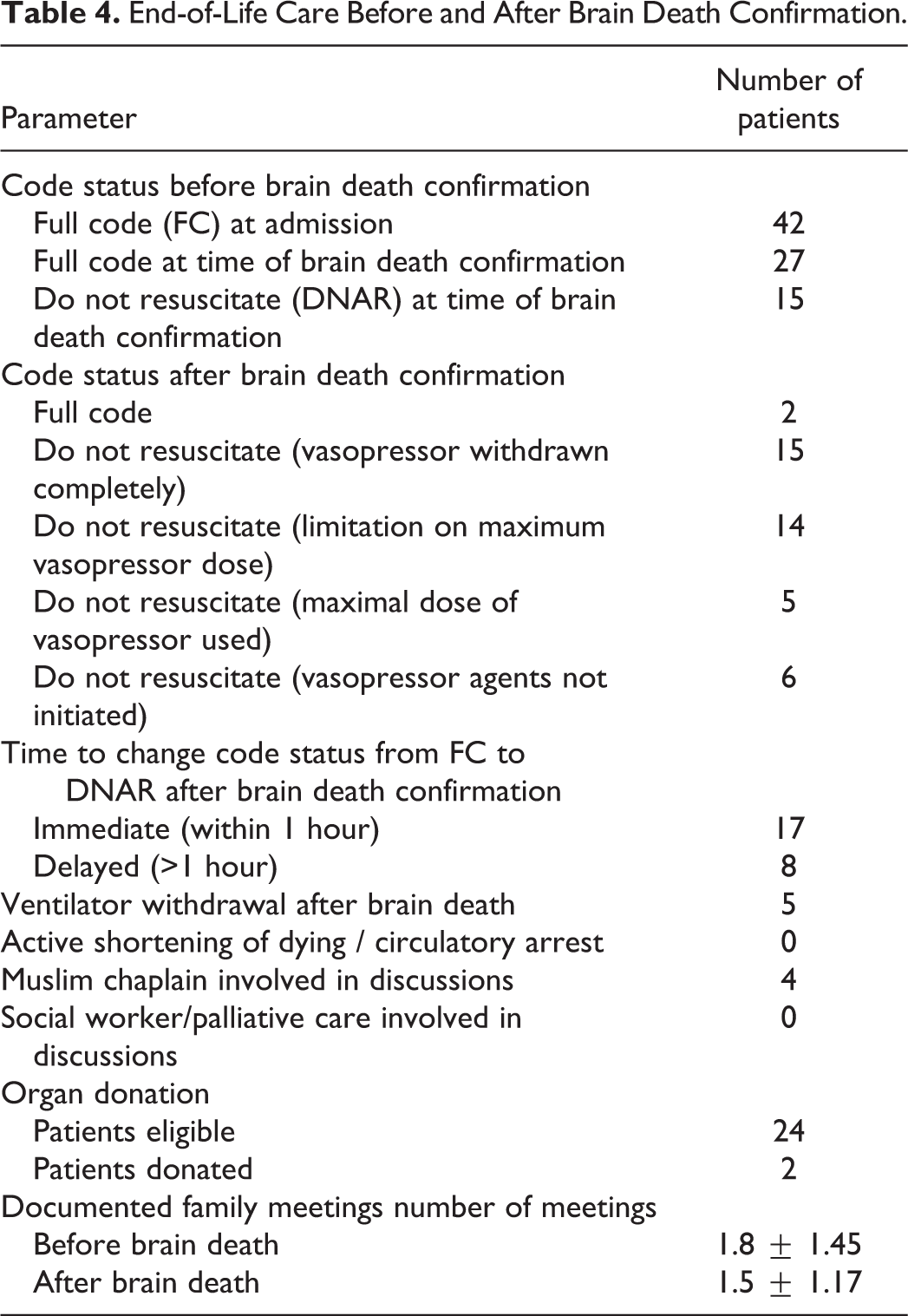
All the patients were admitted to the hospital as “full code.” However, about one third (15 of 42) had their code status changed to “do not attempt resuscitation (DNAR)” before the brain death confirmation. After brain death confirmation, 2 patients remained as full code. The remaining patients were made DNAR but had variations in the usage of the vasopressor agents (Table 4). They were DNAR with no vasopressor limitations (n = 5), limitations on the dosages (n = 20), or complete vasopressor withdrawal (n = 15). Most of the patients who had their code status changed to DNAR had it converted immediately after confirmation of brain death. Terminal withdrawal from the mechanical ventilator occurred only in 5 patients. There was documentation in 9 other patients in whom terminal withdrawal was not done because of refusal by the families. No documentation was found in the remaining patients to explain the reason for not performing terminal withdrawal. In most brain-dead patients, circulatory arrest occurred quickly, within 2.14
End-of-Life Care Before and After Brain Death Confirmation.
Discussion
There is a dearth of literature regarding the end-of-life practices in Muslim patients. Islam is a religion that has spread worldwide and Muslims are becoming a part of communities globally. 7 As per a conservative estimate, only 18% of the 1.1 billion Muslims live in the Arab countries. 20 Muslims residing outside Islamic countries usually do not have a choice in cases of terminal withdrawal after brain death confirmation. And it is a perception that most Islamic countries now accept brain death after which intensive care equipment can be withdrawn. 7 However, the later is a statement based on observation and not backed by evidence. In our study, we try to explore these dynamics in one of the conservative Islamic societies 21 of the world.
The number of patients identified as brain-dead among the total number of deaths in our study (1.4%) is similar to what has been reported before in other nontrauma tertiary care centers (0.99%). 22 The etiologies of brain death in our patients are also similar to the ones reported commonly in nontraumatic brain-dead patients. 23
The code status findings in our brain-dead patients provide us with an interesting perspective. As mentioned in Table 4, all patients except 2 were DNAR at the time of circulatory death. The code status was changed to DNAR either before or soon after the confirmation of brain death. But, what is astounding is that 2 patients ended up receiving CPR even after brain death confirmation and only 5 (12%) patients had terminal withdrawal of the ventilator. This is something in contrast to practice in North America and Europe where all of them would have been disconnected from the ventilator. From the medical records, it was unclear whether terminal ventilator withdrawal was attempted in all the cases. However, the fact that it was performed in 5 patients, and refused by families in other 9, does imply that there was some effort from the physicians in this regard. Failure to proceed with terminal withdrawal in 88% of the patients does allude to the fact that physicians either were reluctant to do it themselves or faced resistance from the families. The later notion seems more plausible as all these physicians had been involved in terminal withdrawal of brain-dead patients in North America. Whether, it is the result of the cultural influence, 24 or lack of medicolegal and ethicolegal laws, or combination of factors, is unclear. But the fact that none of the 9 documented cases, where families disagreed, were terminally withdrawn supports the opinion that lack of “legal” rulings in Muslim countries make this an extremely difficult task for the physicians. 12,14,25 In the absence of organ retrieval, this puts an economic and social burden on the health care system which ends up catering to these “dead” patients. Our results show that families do accept the fact that the brain-dead patients are “terminal” and do not object to the idea of withholding or withdrawing treatment. But what are the factors that prevent them to agree to the idea of terminal withdrawal need to be explored further. Whether it is contradiction to ones religious beliefs, 26 or influence of a person’s social attitudes, 16 or disagreement between the patient’s extended families commonly seen in the society, 18 or a combination of all, remains an avenue for future research.
We evaluated 4 “life-sustaining” therapies (vasopressor agents, antibiotics, nutrition, dialysis) in our patient population. Enteral nutrition through a tube is regarded as a medical treatment that can be refused, withheld, or withdrawn. 27 However, withholding or removing it without the consent of the patient or their families, especially in vegetative states, is one of the most controversial medical and legal issues. 28 Even in the best situations, abatement of nutrition during the end stage of illness continues to be difficult, often colored by religious, cultural, and racial or ethnic perspectives. 29 In our brain death patients, we saw an increase in the utilization of nutrition even after brain death confirmation. This is probably because of the fact that continuation of enteral feeding satisfies the emotional needs and ethical views of the patient's family and caregivers. 30 In contrast to nutrition, there was a decline in the use of antibiotics and complete discontinuation of hemodialysis once the brain death was confirmed. This may be due to the fact that both infection and renal failure do not cause immediate hemodynamic collapse and may make it easier for the physicians to discontinue them. The exact reasons need to be further evaluated. On the contrary, as far as vasopressor agents are concerned, we saw variation in their usage; 36 (86%) of 42 of the patients were already hypotensive and on vasopressor agents before the confirmation of brain death. After brain death confirmation, 38% of these had them withdrawn and 50% had some sort of limitations placed on the dosages, based on the physician orders in medical charts. There is no evidence that dictates this variation, and one can hypothesize that it had to do more with the comfort level of the individual physicians and the response of the families. Overall, 79% of the patients had one or more life-sustaining therapies withdrawn. When compared to therapy limitation, only withdrawal of vasopressor agents was associated with quicker circulatory arrest. Stopping nutrition, antibiotics, or hemodialysis did not affect the duration of the circulatory arrest. Of note, there was no “active” shortening of the dying process before or circulatory arrest after brain death, as euthanasia is forbidden in Islam. 7
The importance of a multidisciplinary approach while dealing with families of brain death patients in different patient populations has been documented. 31, 32 However, in our study, the role of Muslim Chaplain, social worker, or palliative team was very minimal while interacting with families and in the end-of-life decision making. This could be due to their lack of appropriate training and experience in dealing with such patients. However, there can be several other social, religious, and cultural factors that could have played a role in this regard. Utilization of this multidisciplinary approach and its impact on patient outcome in Muslim patients need further evaluation.
Organ donation still remains a sensitive issue in Muslim patients. In Saudi Arabia, formation of the Saudi Center of organ transplantation (SCOT) has improved the donor ratio and successful retrieval of organs from both cadavers and brain-dead donors. 10 However, the ratio of successful donors to eligible donors remains much lower than that seen in developed countries. 10, 33, 34 In our study, out of an eligible 24 donors, only 2 actually donated their organs. This presents a daunting task for the SCOT and the physicians in general to devise and utilize new mechanisms that would result in better organ donations.
Our study has a few limitations. It is a single-center retrospective study from a tertiary care referral center and does not necessarily represent the general Saudi population en masse. The total number of brain death patients even though is appropriate to the number of total deaths but is still small. The physicians taking care of the patients are all North American trained. Cross-cultural issues play a major role in family disagreements and their poor understanding of the patient’s situation. 35 Whether locally trained physicians would be more or less reluctant to withdraw ventilator or other therapies is not known. There was significant lack of involvement of support services like social worker, Chaplain, or palliative care in our study patients. Whether such a multidisciplinary approach could be more conducive to families in accepting the idea of terminal withdrawal is also unknown.
Conclusion
Muslim brain-dead patients in Muslim countries have similar characteristics as patients elsewhere in the world. However, our experience suggests that the physicians in the absence of medicolegal laws find it extremely difficult to terminally withdraw such patients from the ventilator. The concept of withholding or withdrawing other life-sustaining therapies is relatively better accepted by the patients’ families. Prospective multicenter research in Muslim countries, involving palliative teams, should be carried out to validate these findings and find a solution so brain-dead patients are not unduly kept on life support.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.