
Abstract
Aims and Objectives:
Sleep disorders are frequent in patients with advanced cancer receiving palliative care. The objective of this study was to demonstrate whether relaxation therapy can improve their satisfaction with sleep.
Background:
Few studies have investigated the effectiveness of relaxation in patients hospitalized with an advanced chronic disease.
Design:
Prospective randomized study with an immediate intervention group (IIG; relaxation days 3-6) and a delayed intervention group (DIG; relaxation days 6-9).
Methods:
The main measure was the overall satisfaction of sleep measured on a Numerical Rating Scale of Satisfaction of Sleep (NRSSS) between 0 and 10.
Results:
Totally 18 (IIG: 9; DIG: 9) patients were included in this study (mean age 66 ± 10.7). The NRSSS improved in both the groups (almost statistically significant) between the day of inclusion and day 2. Because of the dropout of the patients during the last days of the study, we analyzed the improvement in sleep satisfaction only between day 2 and 5. The NRSSS D5 for the immediate and delayed groups were 4.0 ± 23 and 3.8 ± 2.3, respectively. There was no significant improvement in both the groups.
Conclusion:
The results demonstrated the difficulty to include patients with advanced cancer in a randomized study with a DIG. We were not able to demonstrate the effectiveness of relaxation therapy on sleep satisfaction.
Relevance to Clinical Practice:
Techniques that can be easily used to improve sleep in patients with an advanced cancer should be developed and used already early in the disease.
Introduction
Sleep disorders are frequent in patients with advanced cancer, ranging from 24% to 95%, according to the criteria of sleep disorders used and the studied population. 1 –8 They may generate a further burden of distress to patients with impairment in their health-related quality of life and symptoms, such as depression, anxiety, pain, and fatigue. 3,9 Multiple aspects of sleep can be disturbed, including difficulty falling asleep, difficulty staying asleep, early awakening, and excessive daytime sleepiness. 10 Current treatment approaches for sleep disorders include the management of precipitating or aggravating symptoms, pharmacotherapy, and psychological interventions. 11 Pharmacotherapy may be beneficial in the management of transient or short-term sleep difficulties, but its use is often burdened with numerous adverse effects such as daytime drowsiness in particular for this type of population. Therefore, some nonpharmacological approaches must be promoted in this population. Few studies have investigated the effectiveness of relaxation in patients hospitalized with an advanced chronic disease. 12,13 Two randomized studies have measured the effect of different relaxation techniques to promote sleep only in patients hospitalized in intensive care units. 14,15 Effects of the relaxation on sleep were small; however, there was an important bias as both groups benefit from sleep hygiene training.
Another study examined the effects of progressive muscle relaxation and autogenic training for patients with cancer in a rehabilitation program. 16 They could not find any differences between the 2 intervention groups.
The objective of this present pilot study is to measure the efficacy of relaxation training for hospitalized patients with advanced cancer in a randomized study with an immediate intervention group (IIG) and a delayed intervention group (DIG).
The main research question for this pilot study was therefore can relaxation therapy improve satisfaction with sleep of hospitalized patients with an advanced cancer and sleep disorders?
Methods
The study had a 9-day randomized design with each participant assigned to an IIG (relaxation from day 3 to 6) or to a DIG (relaxation from day 6 to 9). This design was selected to minimize all the placebo effect related to the inclusion in the study. Over a 12-month period, notes of patients hospitalized in the division of palliative medicine were screened to determine whether they met up with the inclusion criteria: a diagnosis of metastatic cancer with an estimated prognosis of less than 6 months, sleep disorders defined according to International Classification of Sleep Disorders, hospitalized at least for 5 days, Mini-Mental Status Examination >20, pain controlled during the last 48 hours or less than 4 of 10 on Numerical Rating Scale (NRS), dyspnea controlled during the last 48 hours, or less than 4 of 10 on NRS, speaking French fluently. 17 The exclusion criteria included the following: last days of life and hearing loss. If the inclusion criteria were met, the patient was given information by the first author and was invited to take part in the study. Randomization was done by blocks of 5, using the Latin square method. The local research ethics committee approved the study.
Following written consent from the patient, demographic data were collected (age, main diagnosis, and comorbidities). History of sleep disorder, associated precipitating factors (ie, incidental pain or dyspnea, factors linked to hospitalization: uncomfortable bed, environmental noise, and disturbance from other patients for example) and perpetuating factors (ie, maladaptive sleep behaviors: excessive amount of time spent in bed, irregular sleep–wake schedule, and napping), and previous experience of relaxation were also noted. Prescribed hypnotic and sedative as well as the effective use of as needed drugs were collected daily.
Assessment Instruments
Global satisfaction of patients with their sleep measured with an NRS rating from 0 (best sleep) to 10 (worst sleep) was collected daily from day 1 to day 9. This measure is very close to the “ESAS sleep” recently validated by Delgado-Guaye et al. 18 We decided not to use scales, such as the Pittsburgh Sleep Quality Index, because of the fatigability of this population. 19 The use of Actiwatch has limitations in this population who often stay in bed, and the use of polysomnography was not feasible. 20,21 A sleep diary was completed by the patient daily. Pain and dyspnea were also rated from 0 to 10 on an NRS part of the Edmonton Symptom Assessment completed daily. 22 During the inclusion of patients, the Hospital Anxiety and Depression Scale was also completed. 23
Intervention
All interventions were conducted by the first author (D.D.), a specialized nurse with a certification in relaxation. The IIG had the intervention from day 3 to 6 and the DIG had the intervention from day 6 to 9. At day 3 for the IIG and day 6 for DIG, the patient benefit form =1-hour training session. Each session began with deep breathing exercises and instruction in somatic tension release. Following muscle relaxation training, participants were instructed how to maintain a state of somatic relaxation. Participants were given an audio recording (CD and CD recorder) of the training program that they had to listen during the night before falling asleep or as needed during the night.
Statistics
A comparison between the 2 groups was conducted by nonpaired t test. The improvement in NRS satisfaction was determined by paired t test or Wilcoxon test. According to the inclusion difficulties and the dropout of the patients during the last days of the study, we analyzed the improvement of satisfaction of sleep only at day 5. Because of the lack of study with a design similar to ours with this population, we were not able to achieve a power calculation “lege artis.” This pilot study had therefore included approximately 20 patients. All analyses were performed using STATA version 6.03.
Results
Over a 12-month period, 357 charts of patients’ notes were screened (Figure 1). A total of 18 patients were finally included in the study. They were included after a median 7 days of admission. Main characteristics of the patients are described in Table 1. There was no significant difference between both the groups (P > .05). The inclusion mean intensities (± standard deviation [SD]) of pain and dyspnea measured by the NRS were 2.7 ± 2.0 and 1.2 ± 1.5, respectively. Seven patients had a score on the Hospital Anxiety and Depression Scale (HADS) anxiety that was higher than 7 and 13 patients at the HADS depression. All patients but 2 received benzodiazepines or benzodiazepines-like drugs at night (lorazepam [n: 4]; oxazepam [n: 4]; midazolam [n: 3], and zolpidem [n: 4]), 1 patient received queitapine. Two patients had the treatment only on request. Eight (7 of them has a suspicion of depression on the HADS) received antidepressant. Only 1 patient in the DIG had already experienced relaxation.
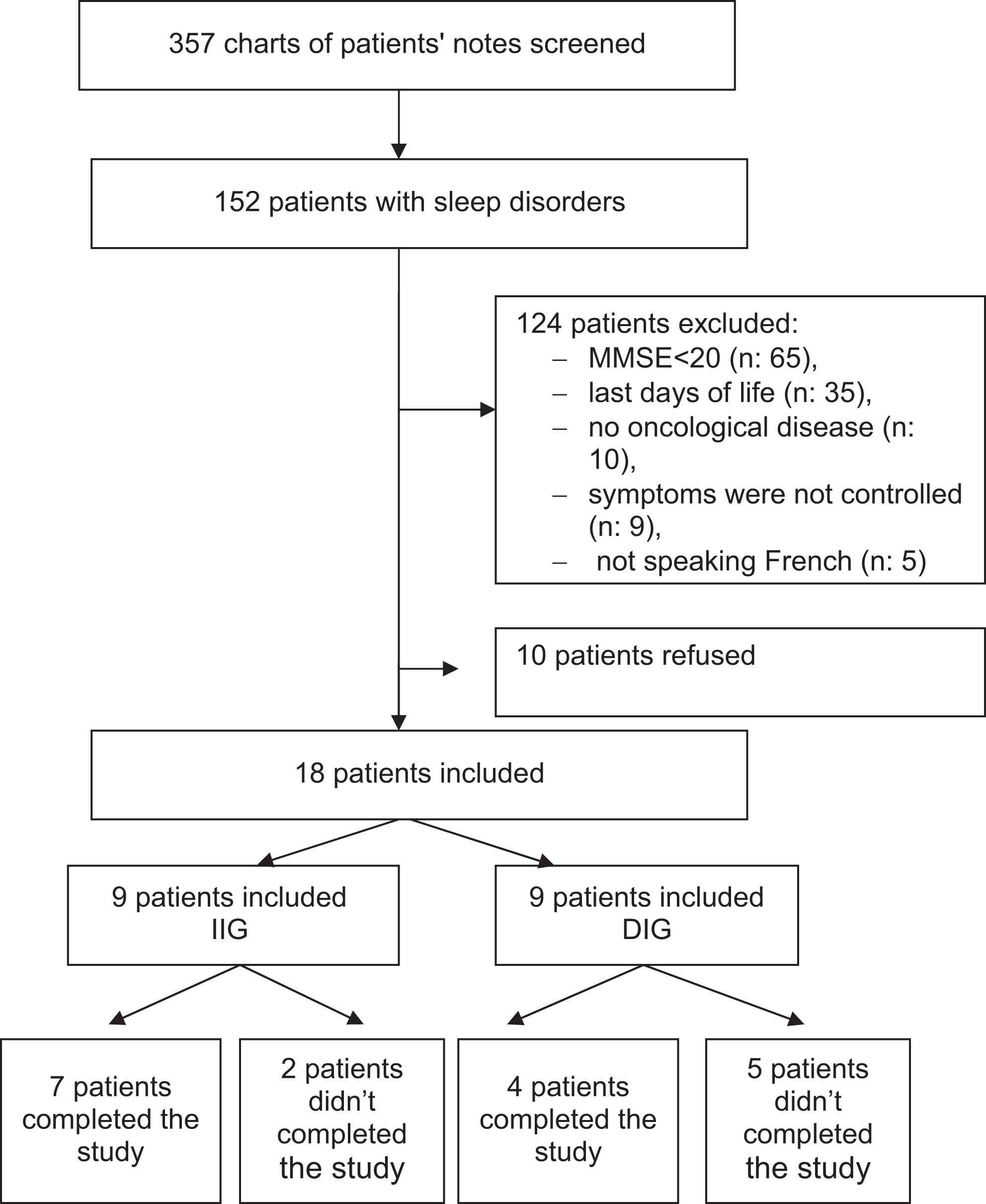
Flowchart of the patients.
Characteristics of Patients.
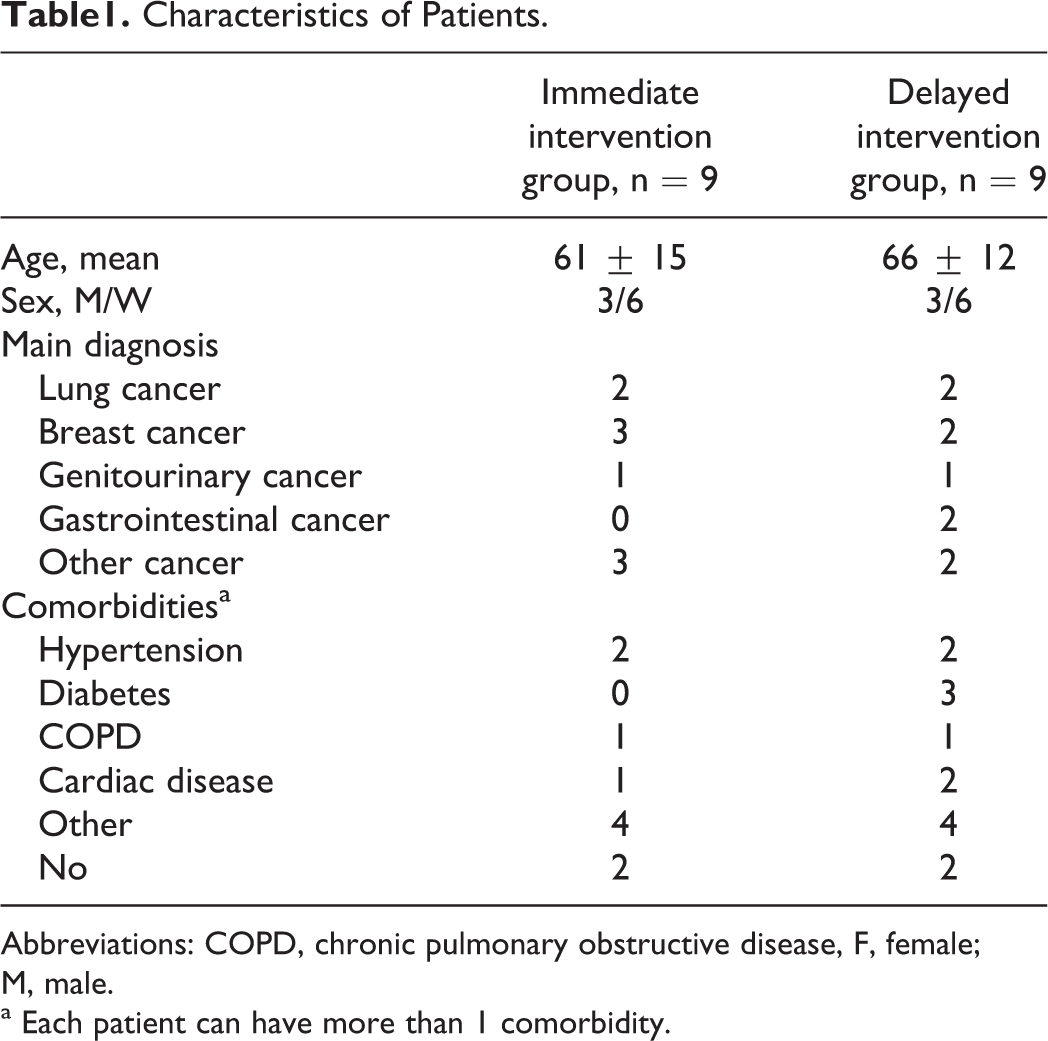
Abbreviations: COPD, chronic pulmonary obstructive disease, F, female; M, male.
a Each patient can have more than 1 comorbidity.
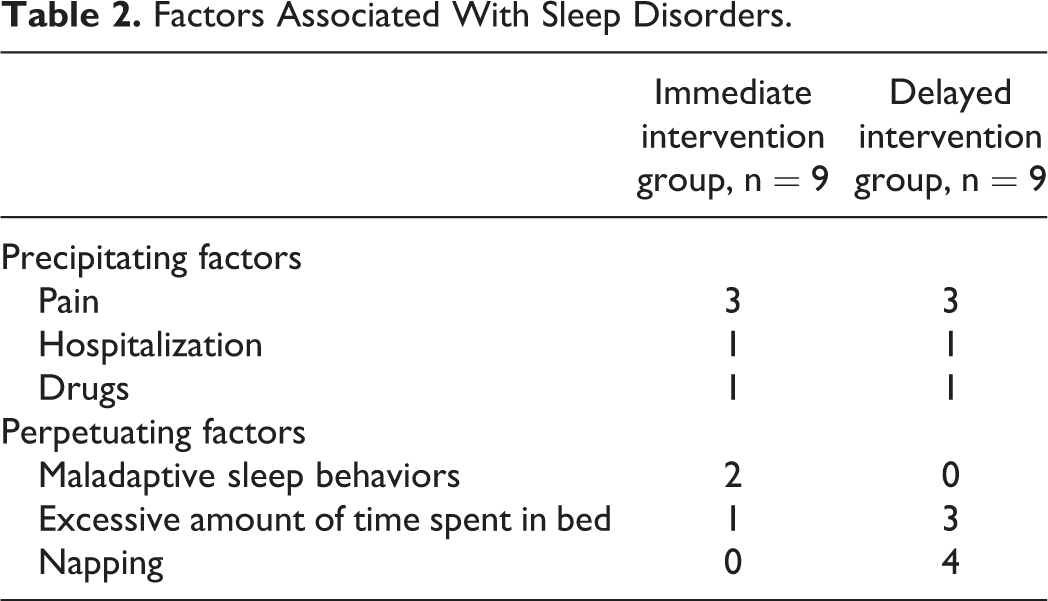
At inclusion, patients reported sleeping an average of 8.5 ± 1.2 hours per night for the IIG and 7.2 ± 1.8 for the IDG (P > .05). Satisfaction with sleep measured by the patient with the NRS sleep with a mean (±SD) was 6.1 ± 2.4 for the IIG and 6.5 ± 2.2 for the DIG. Eight patients stated that they had sleep problems before their cancer diagnosis. Ten patients had difficulties initiating sleep. Nine patients complain of nocturnal awakening and 3 of early awakening. Precipitating and perpetuating factors are described in Table 2. According to the patients, the main reasons for 3 patients for waking up during the night were going to the toilet, for 6 patients it was secondary to incidental pain, for 2 patients it was associated with the noise linked to the care, for 7 patients it was related with anxiety, and 2 patients had no explanations. There was no association between the numbers of hours that the patients slept and the satisfaction with sleep measured by NRS (P > .05).
Factors Associated With Sleep Disorders.
A total of 11 participants completed the treatment phase of the study. Of the 7 noncompleters, 2 were in group IIG (1 refusal and 1 delirium) and 5 were in group DIG (D 2 delirium and 3 refusals).
Both groups improved (almost statistical significant) their satisfaction of sleep measured by the NRS (NRSSS) between day of inclusion and day 2 (see Table 3). There was no significant improvement between day 2 and day 5 in both the groups, P > .5.
Satisfaction of Sleep in the Immediate Intervention Group (IIG) and the Delayed Intervention Group (DIG).

a Numerical Rating Scale of Satisfaction of Sleep.
Furthermore, there was no change in benzodiazepines treatment during the 9-day study. However, 2 patients asked to take the CD home at discharge.
Discussion
Clinical research in patients with advanced cancer is associated with particular difficulties in regard to recruitment and accrual of patients and outcome measures, in particular whether the study should meet the criteria for sufficient methodological rigor. This study demonstrated the considerable effort required to recruit patients. Furthermore the design of the study that should limit as much as possible the placebo effect with the DIG made the inclusion of the patients more difficult and caused an important dropout of patients during the last nights of the study.
Despite a large proportion of the patients complaining that they did not sleep well, both groups reported sleeping an average of, respectively, 7 and 8 hours per night. There was no association between the number of hours slept and the satisfaction of patients with their sleep. This may indicate that those patients who complained of not sleeping well despite an average of 8 hours of sleep per night did not have restorative sleep during the time that they reported being asleep. Sleep fragmentation could also explain these results. These results are similar to the recent study and highlight the importance of assessing patient’s quality of sleep. 21,24
Although both groups showed an improvement in their satisfaction with sleep the day after inclusion, we could not demonstrate in our pilot study that a simple relaxation therapy improves satisfaction with sleep in patients with advanced cancer hospitalized in a palliative care unit. Different reasons can be raised. First, sleep disorders were not only due to acute stress related to the disease and environmental changes secondary to hospitalization, as approximately half of the included patients have chronic insomnia. This proportion of patients was higher than the existing literature. 25 Furthermore, approximately half of the patients had possible associated depression and/or anxiety, despite an antidepressant treatment. We cannot determine whether these symptoms are the causes or the consequences of their sleep disorders. However, the improvement in the patients at the inclusion in the protocol underlines the importance of the validation of sleep disorder. While many recommendations about sleep disorders emphasize the importance of nonpharmacological interventions, all included patients but 1 received systematically benzodiazepines and only 1 patient had benefit from relaxation before the inclusion in the study. 3
In conclusion, the assessment and management of sleep disorder should be integrated early in the disease as suggested by patients in a recent qualitative study. 26 Further work is required to develop techniques that can be easily used, to improve sleep in patients with an advanced cancer and further studies are necessary to determine whether relaxation therapy has an effect on sleep satisfaction.
Footnotes
Acknowledgments
The authors would like to thank the patients who took part in this study for taking time to complete the sleep diaries and questionnaires.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.