
Abstract
Objective:
To investigate whether do not attempt resuscitation (DNAR) orders can be implemented in a standard nursing home in Japan, where routine DNAR orders are not yet common in many facilities including hospitals.
Method:
Ninety-eight residents in a 100-bed nursing home were evaluated. All of the eligible residents and/or their family members were asked whether they wanted to receive resuscitation, including mechanical ventilation.
Result:
The residents were 54 to 101 years of age (mean 83.3), with 27 males and 71 females. After administering the questionnaire, 92 (94%) patients did not want resuscitation and mechanical ventilation.
Conclusion:
In a nursing home, it was possible to obtain advance directives by which most residents/families rejected resuscitation and mechanical ventilation. This could avoid unnecessary and undesirable resuscitation procedures.
Introduction
Although euthanasia is not legally recognized in Japan, social problems were seen when physicians and other medical staff removed mechanical ventilatory support according to the wish of the patient’s family, after starting mechanical ventilation on elderly patients. 1 These problems may occur because of the lack of advance directives, especially when patients and their families have never discussed end-of-life issues. It is reasonable that the lack of advance directives provides no opportunity to talk with each other; talking about end of life is regarded as taboo, especially among elderly individuals in traditional Japanese culture 2 as in other Asian countries such as China which believe in Buddhism. 3 In the United States, the health care staff in hospitals, nursing homes, and other skilled nursing facilities are required by the Patients Self-Determination Act of 1991 4 to ask patients and residents whether they have any advance directives for their health care, including do not attempt resuscitation (DNAR). However, in Japan, getting advance directives is not a common practice in many hospitals, nursing homes, or other skilled nursing facilities. Frequently, the reason resuscitation and other heroic measures are initiated is because no one knows the wishes of the patient/resident or the family. This is particularly problematic in Japan because once mechanical ventilation has been instituted, it cannot be terminated unless the patient/resident fully recovers and does not require mechanical ventilation 4 or the patient/resident dies. 5 Advance directives from terminally ill patients and the elderly patients can help avoid unnecessary and undesirable resuscitation techniques, including mechanical ventilation, as well as reduction in medical cost. Although this kind of issue is inevitable, it has been thought to be taboo in Japan because of the traditional culture, as mentioned above.
Due to an aging society in Japan, the number of elderly individuals who live by themselves increases each year, 6,7 necessitating the establishment of a protocol for getting advance directives. This is the first report demonstrating advance directives in a Japanese nursing home. It is hoped that this will provide assistance for clinicians to help improve rapport with patients and their families to discuss advance directives.
Methods
Ninety-eight residents, who stayed more than 1 week between May 2006 and September 2006 in a 100-bed nursing home, were studied. The residents were asked the question, “Would you like to receive mechanical ventilation to save your life when necessary?” Of the 98 residents, 80 had mild to moderate or severe dementia and were not questioned as to their wishes for resuscitation; however, their next of kin were asked the question, “Would you like him or her to be on a ventilator when necessary?” This study was approved by the institutional review board.
Results
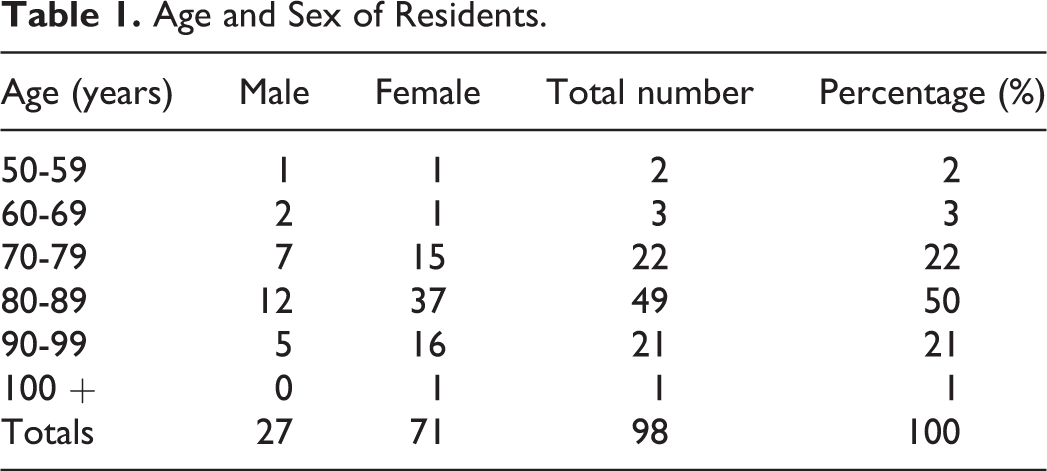
The residents were 27 males and 71 females. The mean age was 83.3 (range 54-101) years. The proportion of age and sex of the residents is shown in Table 1. The primary reasons for admission to the nursing home are cerebrovascular disease 40 (41%), including trauma, dementia 32 (33%), orthopedic diseases 22 (22%), and 4 others (arteriosclerosis obliterans, rheumatoid arthritis, disuse atrophy of muscles, and multiple myeloma). The Mini-Mental State Examination (MMSE) was used to classify dementia. It is a reliable and valid measure of cognitive impairment and is used to assess memory, concentration, and other cognitive skills.
Age and Sex of Residents.
Desire for Mechanical Ventilation Prior to Questioning
Eighteen residents or their next of kin (18%) expressed their wish not to be resuscitated if it became necessary before being questioned and, therefore, they were not asked their opinion again. Among the remaining 80 residents, the next of kin of 6 (6%) residents had expressed their wish to initiate mechanical ventilation to prolong his or her life. The family of 1 (1%) resident requested mechanical ventilation only until another family member, who was away at the time, was able to see the resident before he expired. Once this family member saw the resident, they wanted mechanical ventilation to be withdrawn. There were no records of the wishes for the families of 73 (74%) residents, as shown in Table 2.
Desire for Mechanical Ventilation; Before, and After Questionnaire.a
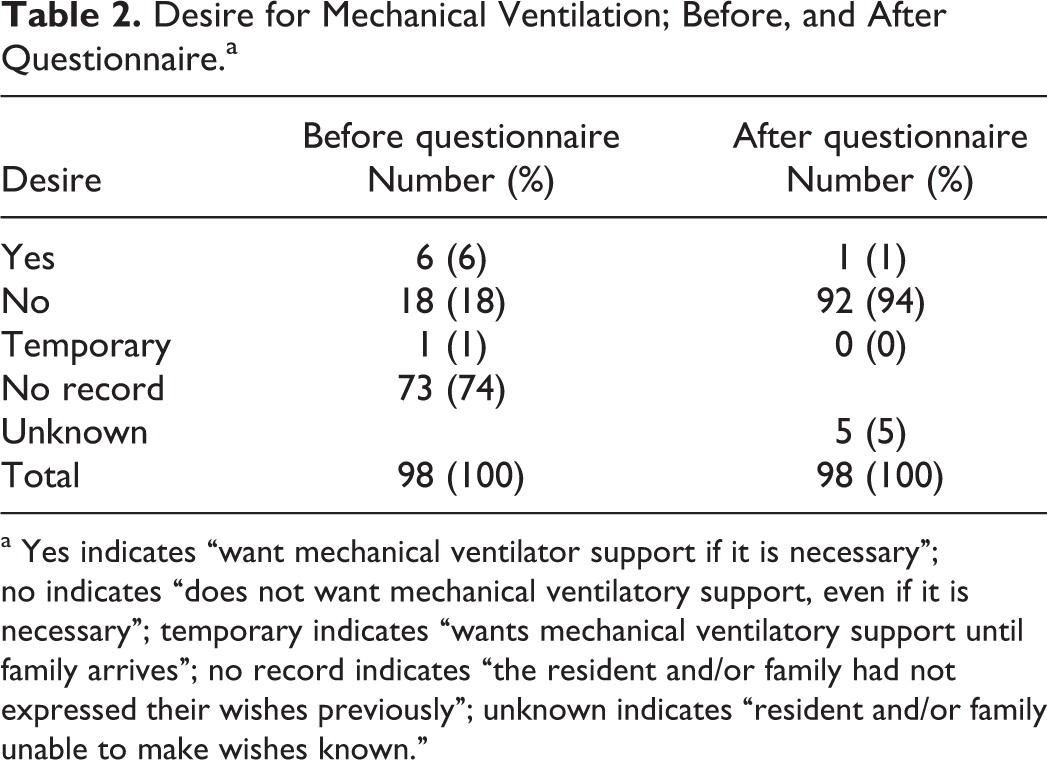
a Yes indicates “want mechanical ventilator support if it is necessary”; no indicates “does not want mechanical ventilatory support, even if it is necessary”; temporary indicates “wants mechanical ventilatory support until family arrives”; no record indicates “the resident and/or family had not expressed their wishes previously”; unknown indicates “resident and/or family unable to make wishes known.”
Desire for Mechanical Ventilation After Questioning
The families of the 6 residents who initially wanted to use mechanical ventilation and the 1 family who had been wishing to prolong the resident’s life until members arrived changed their mind and expressed their intention not to use mechanical ventilation after understanding the characteristics of the machine and learning that it is not legal to terminate the machine while the heart is beating, even when there is very little hope for recovery. Among the 73 families who had not expressed their wish, 1 family expressed their desire to use mechanical ventilation when necessary. Among the remaining 72 families, 5 could not make a definite conclusion and 67 expressed their wish not to use mechanical ventilation. Thus, eventually after asking the question related to receiving mechanical ventilation, 92 families (18 + 6 + 1 + 67 = 92) were against the use of mechanical ventilation (see Table 2).
Interval Between Initial Questionnaire and Final Response
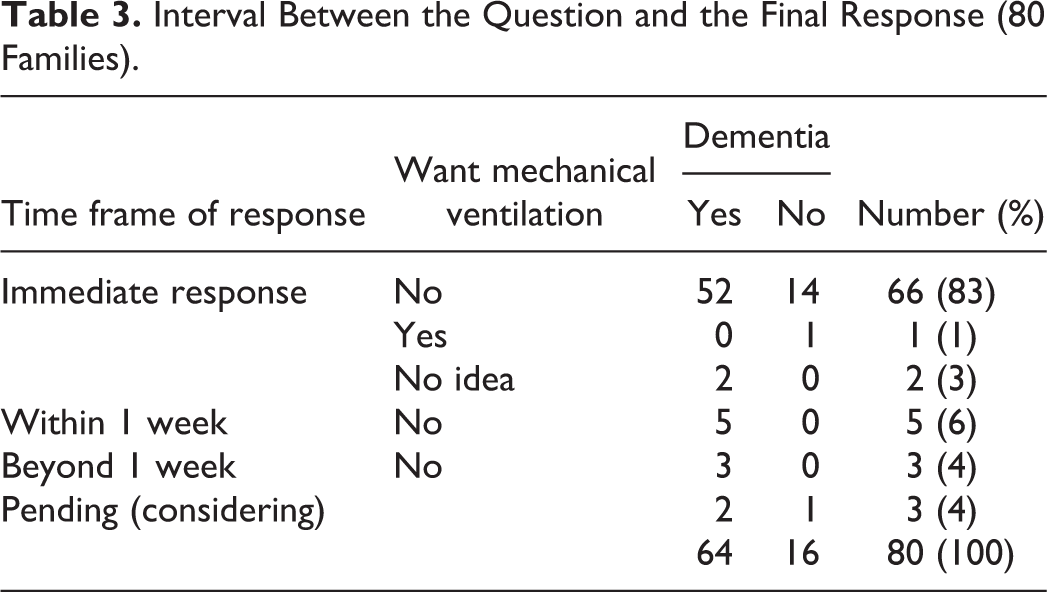
The majority (84%) of the families made a decision immediately at the time of questionnaire as to whether they wanted mechanical ventilation or not. Five families had to discuss the issue with additional family members and thus responded several days later. Two families had to consider the question longer and responded after 1 week. Three families could not come to a decision at the time of this writing. Two families responded immediately saying “I have no idea.” Thus 5 (3 + 2 = 5) families could not make a decision to decline mechanical ventilation, resulting in a “yes” for the use of mechanical ventilation when necessary (Table 3).
Interval Between the Question and the Final Response (80 Families).
Reason for the Change in Decision
The families of 6 of the 7 residents who wanted mechanical ventilation prior to the questionnaire came to the nursing home and discussed with the physician, in person, the use of mechanical ventilation. Each of the families decided immediately to decline the usage of mechanical ventilation after understanding its nature. The daughter of the seventh resident had expressed the desire for the use of mechanical ventilation when asked over the phone, since she could not come to the nursing home at that time. Five months later, she visited her mother at the nursing home. She was asked again, in person, and she decided to decline the usage of mechanical ventilation. One resident’s husband passed away after the decision to accept mechanical ventilation had been made and the remaining family member, her brother-in-law, did not wish for mechanical ventilation. The family of one resident had not intended to wish for mechanical ventilation, but their desires were misunderstood, resulting in the conclusion that the resident wanted full resuscitation efforts.
In general, family members are not well aware of the negative nature of the ventilator for the aged. Once they fully understand the significance of mechanical ventilatory support, they tend to decline the mechanical ventilation (see Table 4). Two residents did not have dementia and expressed their wish as “I let the family decide.”
Reason for Change in Decision to Accept Mechanical Ventilation.
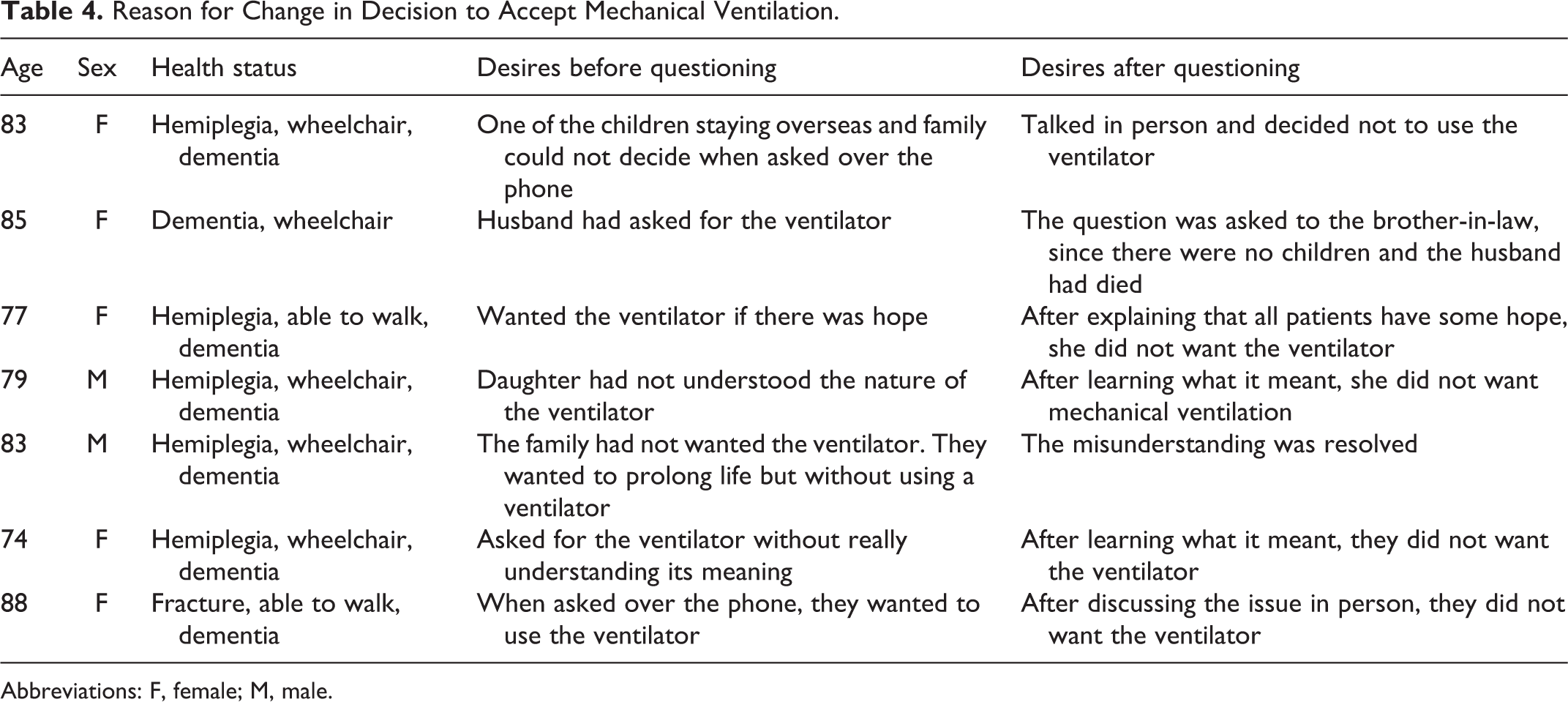
Abbreviations: F, female; M, male.
Residents Who Received Mechanical Ventilation
For the 6 residents who resulted in receiving mechanical ventilation, only 1 family (a son of the resident) expressed his wish clearly and said “yes” when asked whether he wanted mechanical ventilation. The remaining 5 residents resulted in the implementation of mechanical ventilation, because they could neither decide nor give a definitive response as to whether or not they wanted to institute mechanical ventilation (see Table 5).
Residents Who Resulted in Mechanical Ventilation When It Was Necessary.
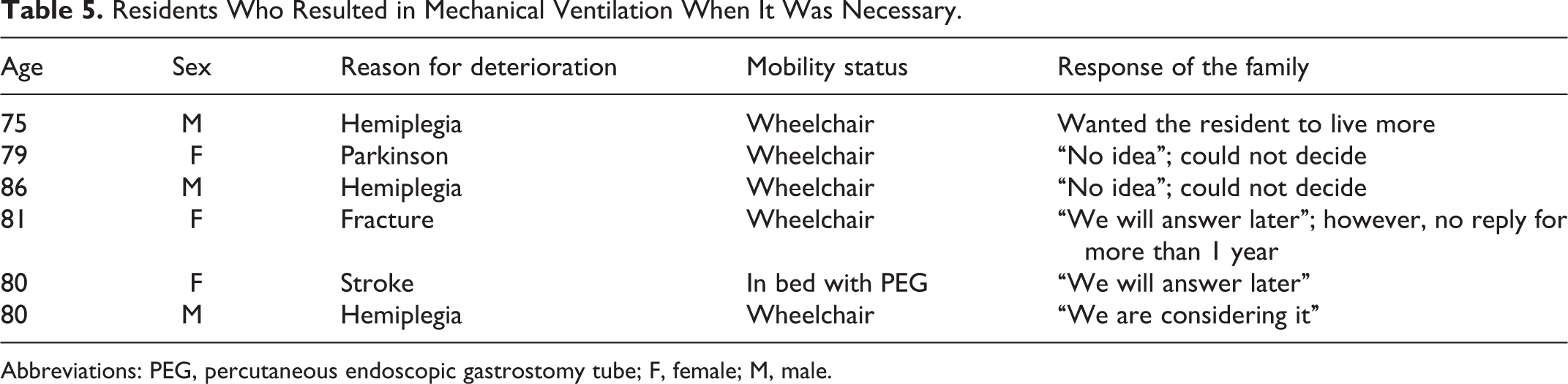
Abbreviations: PEG, percutaneous endoscopic gastrostomy tube; F, female; M, male.
Discussion
Having advance directives, with or without DNAR orders, in nursing homes as well as in hospitals is common in the United States. Messinger-Rapport reported that 40% of the nursing home residents have DNAR orders, 5 and Terry reported that the figure is over 60%. 8 In contrast to this, advance directives are very rare in Japanese nursing homes and not yet common for many Japanese hospitals. Of the 115 nursing homes in Japan’s Chiba prefecture, including the facility in this study, none of the 20 randomly sampled nursing homes routinely obtained advance directives or resultant DNAR orders.
It has been demonstrated that there is a misunderstanding among physicians when asked about advanced directives. Physicians tend to think that patients who are not so severely ill or old do not like to discuss this issue. In fact, patients do not want to discuss this kind of issue, regardless of age and medical condition. 9 We speculate that these misunderstandings by clinicians may prevent the discussions related to advance directives. In such cases, no one knows the residents’ and/or next of kin’s wishes for the adoption of resuscitation procedures including tracheal intubation followed by mechanical ventilation. In urgent situations, this (not asking or not knowing their wishes) results in the routine administration of resuscitation, which occasionally ends up being against the resident’s or the families’ wishes of allowing the residents to pass away as a natural consequence without such intervening procedures. This is especially a problem in Japan because termination of mechanical ventilation while the patient is still alive, regardless of the prognosis, is regarded as murder by the legal system.
One way to avoid such a tragedy is to get advance directives routinely in nursing homes and hospitals. Thus, the physicians in the facility in which this study was conducted started getting advance directives in terms of the use of mechanical ventilation for all of the residents in the nursing home.
In this study, 92 (94%) of the 98 residents/families chose to request a DNAR order after the questionnaire. One possible explanation for this high percentage might be due to the information provided to help make sure that the residents and/or next of kin were fully informed of what it means to be resuscitated and receive mechanical ventilation. The following comments related to mechanical ventilation were explained to the patients and/or their families.
Mechanical ventilation can cause pain and discomfort to the resident, especially at the time of intubation. Mechanical ventilation does not cure heart or lung dysfunction. It supports ventilation and gas exchange but does not return the lung to normal function. This situation is similar to kidney dialysis that has no power to improve renal function no matter how many years you rely on it. Thus, naturally, there is no guarantee that the resident will recover, even if he or she remains on mechanical ventilation. In fact, realistically it is unlikely the resident will return to a normal healthy state because of the age and relatively limited vital organ function.
In addition to the pain and discomfort at the time of intubation and initiation of mechanical ventilation, the need for a tracheostomy may arise. A tracheostomy is generally considered if the patient requires mechanical ventilation for more than 2 or 3 weeks. This is a surgical procedure with complications of its own.
These hardships the resident has to endure could be mental torture for themselves and for their family members, especially when this situation may last for months or even years and he or she still may not be able to fully recover.
The medical expenses incurred from the intensive care unit (ICU) and mechanical ventilation are far from negligible, while you may say you are rich enough and can afford it.
In Japan, and in other countries throughout the world, once mechanical ventilation has been initiated, it cannot be stopped legally until the patient improves or dies. Even if the family is aware of the hardship the patient has to endure and they may want to stop it, they are not able to because it is illegal.
Previous studies reported that knowledge of the elderly individuals regarding life-sustaining procedures was poor, and that they overestimated the effectiveness of cardiopulmonary resuscitation. 10 –14 However, they tend to choose a DNAR order after they received and understood more information related to the procedures. In addition, most residents appear to either have their own experiences of admission in acute care wards or have friends/relatives admitted into a hospital due to critical illness. These personal experiences of such procedures and exposure to the ward might have affected their attitudes toward end-of-life decisions to avoid possible futile procedures.
Several problems were encountered before, during, and/or after the process of explaining the situation to the residents and families. Family members of 15 residents did not want to come to the nursing home for the meeting because they lived very far away. In these 15 cases, the physician discussed the situation with them over the phone. This is not optimal, since clear communication without seeing each other is often difficult, especially on such delicate topics. It is important to establish rapport and trust with the resident and family before discussing this issue. When trying to setup a phone call to have an appointment for the conversation, some family members appeared to avoid the meeting. Such avoidance may be their way of expressing their thought that they do not want to consider the option of DNAR. It is important to respect their avoidance, and it should be interpreted as a sign to initiate mechanical ventilation when it is needed.
Some family members did not like discussing this topic; it was obvious from their facial expressions. Because an elderly person and his or her family could easily get nervous when talking about issues related to death, getting advance directives is stressful, even for attending physicians. Thus, it is reasonable that physicians tend to be reluctant to discuss these issues with the residents and their family members.
In the United States, there is a low frequency of a living will (LW) in patients admitted to adult ICUs (0%-13%) 16 –18 and in units for the chronically critically ill (16%-38%), 19,20 even though all of the patients should be given the opportunity to discuss advance directives according to the Patient Self-Determination Act. Nevertheless, obtaining advance directives allows many residents/family members to be free from undesirable mechanical ventilation.
One possible way to decrease or overcome the discomfort in talking about the issue is to explain, thoroughly, the necessity and importance of asking the question.
The discomfort of asking the question “Would you want him or her to be mechanically ventilated when necessary?” may be diminished with the following questions and statements:
I apologize in advance for asking the following question, but it is very important to ask you to avoid unnecessary and/or undesirable procedures which you may not want.
The reason to ask the question is to fulfill your wishes and the wishes of your family member. Unless we know what those wishes are, we cannot meet them. However, answering the question is a right, not a duty. You have no obligation to answer. You only have the right to answer. We have a duty to decide, but you do not. When you do not decide it means we have to go ahead and start mechanical ventilation, when it is deemed necessary.
Although mechanical ventilation cannot be stopped once it is started, you can change your mind as many times as you like before we initiate it.
Some family members could not answer clearly and told the physician they would inform him or her later and ended up giving no answer. Two or three phone calls were placed to ask whether a decision had yet been reached; however, if they still could not decide, it was decided that it was not appropriate to ask further, since they have no duty to decide and no answer is one kind of answer.
Getting advance directives does not result in the reduction of medical care. Halpern et al have demonstrated that medical procedures and survival times in patients at an oncologic ICU did not correlate with whether LWs were confirmed or not. 21
As for medical economics, expansion of medical expense is a serious problem in every country, especially where an aging society is developing. In Japan, unfortunately, unnecessary intubations and admissions to the ICU are widely performed without the patients’ and/or their family member’s sufficient consent. Osakabe et al documented that medical cost for the elderly patients in emergency medical care unit was 2.5 to 3 times more expensive than for younger patients. Medical expenses needed for the elderly patients to be completely recovered would cost as much as $80 000 (US dollars) per person, which is 50 times more expensive than nonelderly patients’ admission cost in the emergency unit. 15 Although the survival rate is controversial, 22 –24 ventilated elderly patients seem to have higher disability compared with otherwise identical patients who survived without mechanical ventilation. 25
Discussing the problems related to the medical cost for terminally ill elderly patients has been taboo in Japan. These problems, as well as the one we encountered and mentioned above, are the possible reasons physicians tend to be reluctant to discuss these issues with the residents and their family members. Physicians must understand these facts and provide the patients and their family members correct information, which should result in getting advance directives.
It is believed that getting advance directives would result in the reduction of unnecessary procedures and medical staff labor as well as saving medical costs, without a decline in quality of medicine. Although some families are well informed by mass media or other methods about the meaning and the character of resuscitation and mechanical ventilation, others are quite ignorant about it. In such cases, the physician needs to explain the situation thoroughly and patiently. This is time consuming but should be rewarded by the avoidance of possible future problems. This is especially rewarding socially in terms of saving the limited medical resources when the resident and or family members change their opinions and end up not desiring the use of mechanical ventilation. Taking the time to discuss this issue with the resident and family should allow for advance directives and reduce the number of times family members object to continuation of mechanical ventilation once it has been initiated.
After this study, the authors decided to be flexible at the time of the residents’ admission and accept the family members’ wish not to ask the same question to the resident if he or she was over 80 years of age and quite disabled, even if the resident did not have dementia. As a result, the patient was placed on a DNAR list to avoid the presumably rare, but possible, conflict between the resident and the family members on this matter. Although there could be criticism for ignoring the autonomy (self-determination, a basic human right) of the resident, the rationale would be the following: It is the family members who have to bear the burden of taking care of the resident, even when he or she remains in a persistent, vegetative state receiving mechanical ventilation[AQ: Please approve edits to the sentence “It is the family members who have to bear the ….”]. It is not felt that the potential benefit to the resident being mechanically ventilated can be greater than the hardship the family members face because of the age and the poor organ function, in addition to the well-known poor outcomes of mechanically ventilated aged patients. In other words, residents are not losing much when being deprived of their autonomy. It is felt that they could gain a lot by not having to experience the hardship of mechanical ventilation. The low percentage of survivors (1%) for residents who arrest while in a nursing home (4) should support this idea[AQ: Please check the sentence “The low percentage of survivors (1%) for residents who arrest …” for clarity.]. Thus, it would still be ethical not to abide by the principle of respecting the resident’s autonomy and avoid being a fundamentalist, considering the family members’ mental and possibly economical hardship.
This study has one limitation. This is a retrospective study in a very small population. Retrospective studies may be less reliable in terms of the data collected.
Conclusion
It is possible to obtain advance directives in a nursing home without confronting extraordinary troubles or complaints. In most cases, aged residents and family members of the aged patients denied the initiation of mechanical ventilation. Implementing advance directives in the nursing home has a potential to enhance the residents’ and their family members’ satisfaction by conducting medical practice that is consistent with their wishes.
Footnotes
Acknowledgment
The authors are grateful for the diligent and thorough critical reading of the manuscript by Mr John Wocher, Executive Vice President and Director, International Affairs/International Patient Services, Kameda Medical Center (Japan).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.