
Abstract
Reason for the Study:
Studies on methylphenidate for cancer-related fatigue showed conflicting results. This prospective study aims to determine whether methylphenidate is useful for relieving fatigue in Chinese patients with cancer. Chinese Version of Brief Fatigue Inventory (BFI-C) was administered on days 1, 8, and 29. Methylphenidate dose on day 1 was 5 mg daily then adjusted after day 8 according to response and side effects tolerance.
Main Findings:
Only 48% of the 25 recruited patients were on methylphenidate by day 29. Overall, no significant improvement in fatigue level was observed after methylphenidate, though benefits were shown in subgroups with age ≤ 65 and higher baseline BFI-C values.
Principal Conclusions:
Methylphenidate may be useful for management of cancer-related fatigue in selected Chinese patients.
Introduction
Cancer-related fatigue is defined as a distressing, persistent, subjective sense of tiredness or exhaustion related to cancer or cancer treatment that is not proportional to recent activity and interferes with usual functioning. It is usually more severe, more distressing, and less likely to be relieved by rest compared with fatigue experienced by healthy individuals. 1 Cancer treatment-related fatigue is reported in 14% to 96% of the patients undergoing cancer treatment and in 19% to 82% of the patients posttreatment. 2 The mechanisms responsible for fatigue in people with cancer are not known, and each individual may experience multiple possible causes of fatigue simulta-neously. 2
Various means (both pharmacological and nonpharmacological) have been attempted to deal with cancer-related fatigue. Methylphenidate, a central nervous system stimulant structurally related to amphetamines, is probably the most widely studied drug in this aspect. It has been shown to improve cancer-related fatigue in at least 5 open-label studies, 3 and a Cochrane Review concluded that there is increasing evidence that psychostimulant trials provide evidence for improvement in cancer-related fatigue at a clinically meaningful level. 4 However, so far there are few randomized controlled trials that yielded conflicting results. Although Lower et al 5 reported improvement in fatigue and impaired memory after chemotherapy in adult patients with cancer, Bruera et al 6 found methylphenidate not significantly superior to placebo after 1 week of treatment. A recent phase III, randomized, double-blind placebo-controlled study 7 also concluded that methylphenidate did not improve cancer-related fatigue, though a subset analysis suggested that patients with more severe fatigue and/or with more advanced disease did have some fatigue improvement with methylphenidate. There were increased levels of nervousness and appetite loss in the methylphenidate arm.
From clinical experience, fatigue is likely a significant clinical problem in local Chinese patients with cancer receiving palliative care. However, data on use of methylphenidate in Chinese patients for cancer-related fatigue are lacking. Published experience may not be directly applicable to local patients, as they are of different races and with different social background. Therefore, it would be desirable to conduct a local trial to evaluate use of methylphenidate in local patients receiving palliative care.
The objective of the study is to determine whether methylphenidate is useful for management of fatigue in Chinese patients with cancer in the palliative care setting.
Methods
This is a prospective study for evaluating the effectiveness of methylphenidate for management of fatigue in Chinese patients with cancer in the palliative care setting. Patients seen in the palliative care outpatient clinics or receiving inpatient hospice care in 1 of the 6 participating centers (organized under Hong Kong Society of Palliative Medicine) in Hong Kong Special Adminstrative Region, China, were approached to participate in this study. The main reason for each patient who had refused to join study was recorded. The following inclusion criteria (modified from Bruera et al
6
) were used: Local Chinese patients with cancer. Fatigue score of at least 4 on a scale of 0 to 10 (0 = no fatigue, 10 = worst possible fatigue) during the previous 24 hours (question 2 in the Chinese Version of the Brief Fatigue Inventory [BFI-C]
8
will be used) and lasting for the minimum of 4 days. Normal Mini-Mental State Examination (MMSE; defined as a score of ≥24 of 30), a Cantonese version of which is available.
9
Palliative Performance Scale (PPS) level ≥70, according to PPS version 2.
10
No history of arrhythmia, uncontrolled hypertension, heart disease, glaucoma, known depression/anxiety disorders, or substance abuse. No administration of monoamine oxidase inhibitors, tricyclic antidepressants, or clonidine. Methylphenidate not otherwise medically contraindicated. Estimated survival ≥3 months. No ongoing systemic cancer treatment or radiotherapy. Blood tests performed within 2 weeks before or on the day of screening: Hemoglobin level of ≥9 g/dL Albumin-adjusted serum calcium level within ±5% of normal range (treatment allowed) Serum sodium level ≥125 mmol/L (treatment allowed) Serum potassium level ≥3.0 mmol/L (treatment allowed) Serum creatinine ≤200 µmol/L Serum total bilirubin ≤3 times upper limit of normal
A numeric rating scale from 0 to 10 has been used by the BFI, and those patients rating their worst fatigue at 7 or greater can be categorized as having “severe” fatigue. Those rating their worst fatigue at 4 to 6 can also be categorized as having “moderate” fatigue, though the cutoff point between 3 and 4 is less pronounced according to the original study. 11
Patients who agreed to participate in the current study have signed the informed consent, completed the BFI-C, MMSE, and have been evaluated in terms of eligibility criteria. Patients not meeting the study criteria were excluded from the study as screen failures and not included in the analyses.
The BFI-C, which has been validated, 8 was administered by a qualified medical staff to patient at baseline before starting methylphenidate, and then on days 8 and 29 (for those continuing methylphenidate beyond day 8 only). The MMSE 9 was done on screening.
Demographic data including age, gender, PPS level as measured by PPSv2, 10 concomitant diseases, and concurrent medications were recorded at the time when patients were recruited into the study and on days 8 and 29. Blood pressure and pulse were monitored during each visit. Any changes in the doses of the medications during the study period were recorded.
Methylphenidate doses were dispensed from the pharmacies of the participating centers. Patients eligible for this study received oral methylphenidate 5 mg daily (to be taken early morning to avoid night-time arousal) on day 1 (screening). Patients were assessed by the physician in charge on days 8 and 29 ± 3 days (if the patients were still on study on day 29). In patients subjectively finding it useful and expressing a wish to continue the drug after 7 days of treatment, methylphenidate was continued unless contraindicated. The dose to be continued with, the frequency of follow-up (in addition to the day 29 visit), and the total duration of treatment were determined by the physician in charge according to the clinical condition. Methylphenidate was stopped for patients experiencing intolerable side effects.
The final approved protocol and the informed consent statement have been reviewed by properly constituted ethics committees/institutional review boards of the various participating centers. Informed consent was obtained from individual patients.
Definition and Statistical Analysis
All prescription and nonprescription concomitant medications that were ingested, applied, or injected from the time of recruitment as well as changes in such concomitant medications, and any new concomitant medications taken while the patient was on study, were recorded till day 29 or after the completion of the study medication whichever was later. All diseases that occurred on screening and all adverse events that occurred during the study period were recorded and assessed for their relationship to the study drug. Adverse events were recorded according to Common Terminology Criteria for Adverse Events (CTCAE) grade as soon as they were known to the investigators. Patients were not given diaries to record side effects, but any adverse events were routinely inquired during the scheduled follow-up visits of the study.
As stated in Bruera’s preliminary open study, 12 entering 30 patients into the study would allow us to declare differences as large as or larger than 2 points between scores before and after taking methylphenidate with a 2-sided significance level of 1% and 80% power. The BFI was designed in a way that a mean BFI fatigue score could be calculated from the 9 BFI items. 11 A difference of 2 or more points was considered a clinical success based on the generally accepted clinically meaningful difference.
The nonparametric Mann-Whitney statistical method was used to compare the difference in the BFI score values between baseline and day 8 scores and between baseline and day 29 scores. Subgroup analyses were also performed to reveal whether methylphenidate was effective in reducing patient fatigue during the course of the treatment. The software used was Statistica, version 11 (StatSoft, Tulsa, Oklahoma). Values of P ≤ .05 were considered statistically significant.
Results
A total of 56 patients have been approached to participate in the study, and 25 patients agreed to be recruited in total during the period from January 2009 to January 2011. The reason of discontinuing patient recruitment before reaching the target number of 30 participants was slow recruitment and high rate of refusal to join the study. The most common reason for refusing to join the study was that the patient was not willing to take medication for fatigue (Table 1). The recruited patients were predominantly male (20 of 25) with a mean age of 64 (range 47-81). Table 2 tabulates the demographic data of the patients at the time of recruitment.
Reasons for Patients Refusing to Join the Study Using Methylphenidate for Cancer-Related Fatigue.

Patient Demographic Data at the Time of Recruitment.
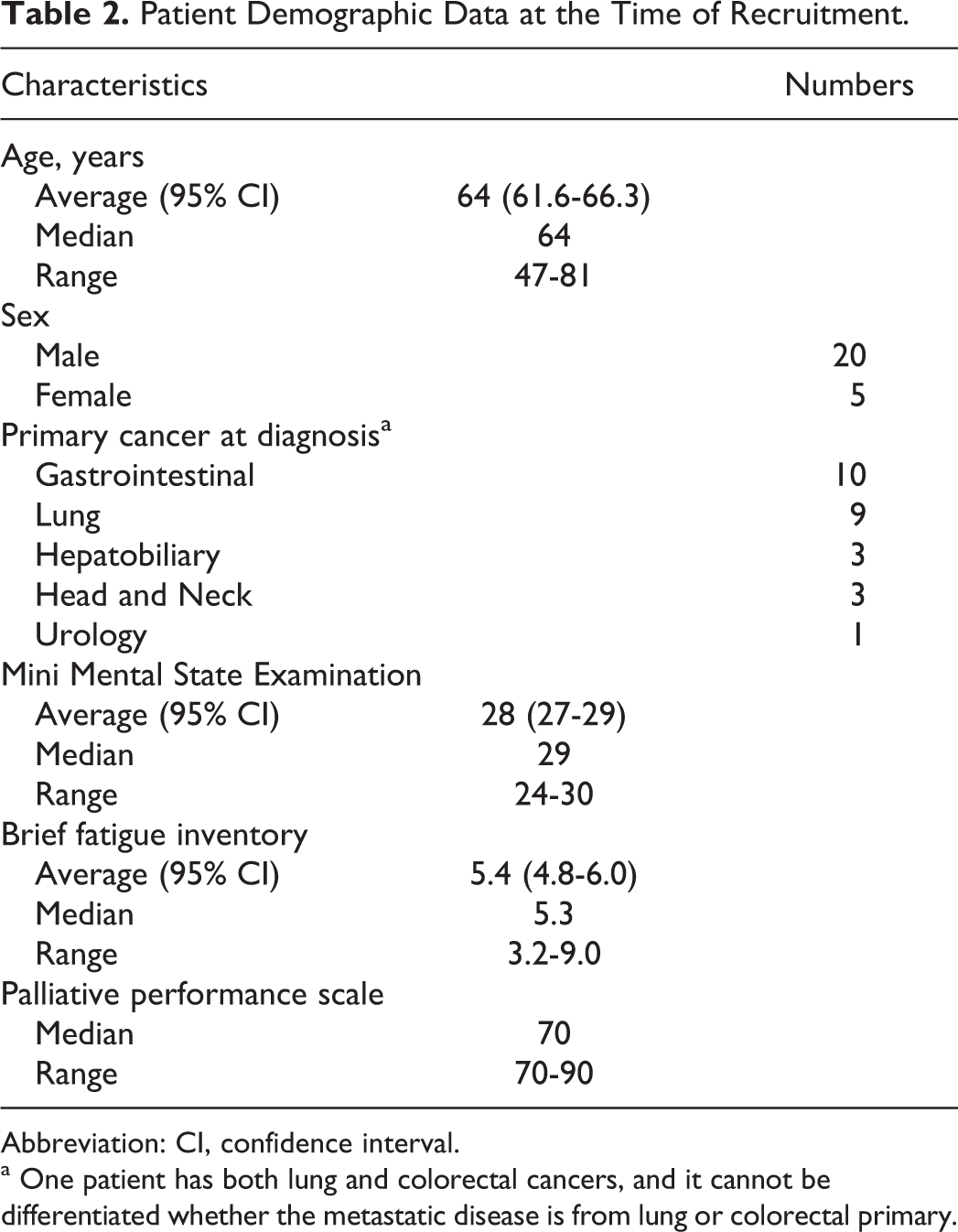
Abbreviation: CI, confidence interval.
a One patient has both lung and colorectal cancers, and it cannot be differentiated whether the metastatic disease is from lung or colorectal primary.
One of the recruited patients had never started methylphenidate treatment for fear of side effects, thus making the number of recruited patients who have received methylphenidate treatment being 24. Ten (40.0%) patients (including the one who had never started treatment) stopped methylphenidate treatment before day 8. In all, 8 of them complained of intolerable side effects, and 1 died before day 8 (the death was considered unrelated to methylphenidate). Among the remaining 15 patients (9 of whom were above 65 years old), 1 was unwilling to continue study, and so only 14 patients were continued methylphenidate (Table 3). All patients were taking methylphenidate at 5 mg daily on day 8, except 2 patients who had self-increased the dose of methylphenidate to 10 mg daily (as 2 divided doses).
Patient Status on Days 8 and 29 of the Study.

a Based on total number of 25 patients recruited into the study.
On day 29, only 12 (48.0%) patients were still on methylphenidate, 8 of whom were above 65 years old. Two patients stopped methylphenidate due to admission to hospital (reason of admission considered unrelated to methylphenidate). In the remaining patients, 7 of them were taking a total daily dose of 10 mg methylphenidate (as 2 divided doses), and 5 of them were taking single 5 mg daily dose without dose escalation. None of the patients who had continued methylphenidate till day 29 felt side effects of methylphenidate intolerable, but 4 of them decided not to continue methylphenidate beyond day 29, as they subjectively did not find it effective in relieving their fatigue (Table 3). Of the remaining patients, only 1 was allowed further dose escalation to total daily dose of 15 mg. No adverse events of CTCAE grade 3 or above were recorded.
When patients undergoing methylphenidate treatment at baseline and on day 8 were selected, there was a statistically significant difference between BFI values at baseline and on day 8 for patients aged ≤65 (P = .03), with corresponding difference in the median BFI in this subgroup being 2.1. This indicates that methylphenidate medication would reduce the BFI scores on day 8 for patients younger than 65 years old (Figure 1). However, when these subgroup analyses were repeated for baseline versus day 29, there was no significant difference in the BFI scores between patients at screening and on day 29 even for those still taking methylphenidate (Table 4).
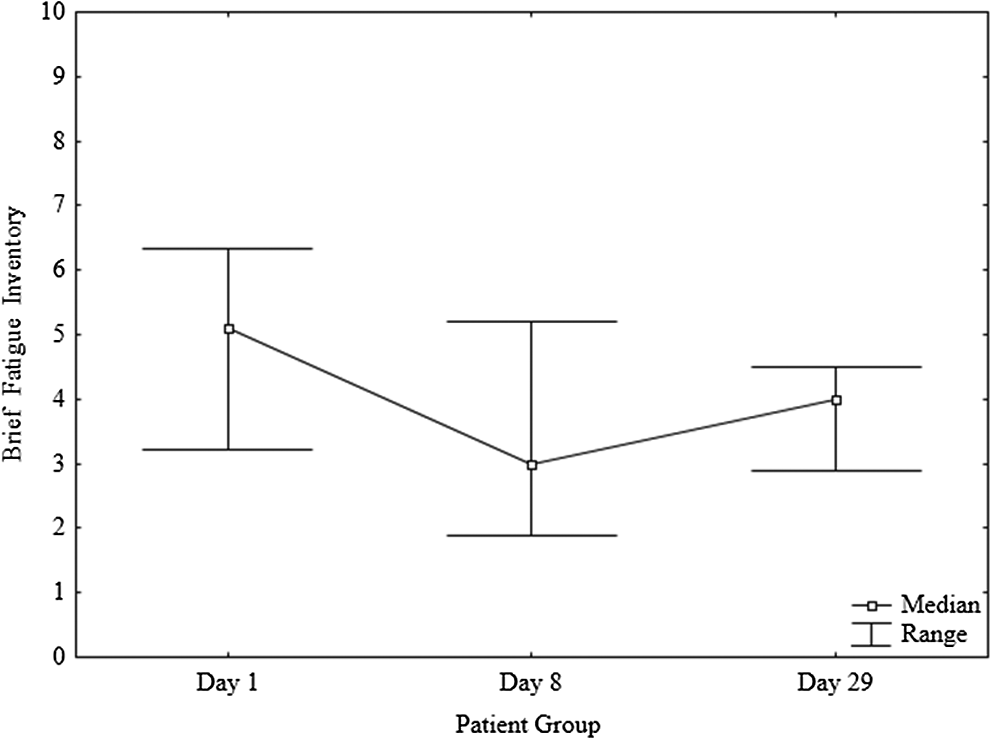
Variation in median brief fatigue inventory (BFI) for patients with methylphenidate and age of less than 65 years old on screening (day 1), day 8, and day 29. The reduction in median BFI between patient at screening and on day 8 was greater than 2 units.
Subgroup Analysis Between Brief Fatigue Inventory (BFI) at Baseline, Day 8, and Day 29.a
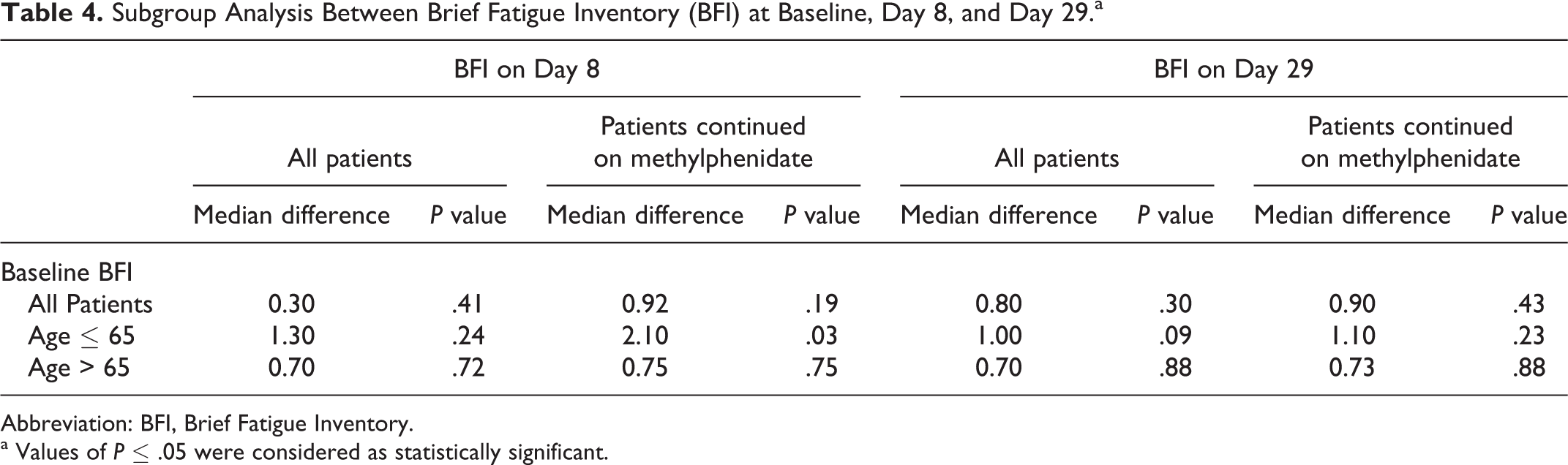
Abbreviation: BFI, Brief Fatigue Inventory.
a Values of P ≤ .05 were considered as statistically significant.
Other variables, for example PPS and the use of morphine, would not be a statistically significant predictor of any BFI score difference between baseline patient group and patient groups on days 8 and 29.
The early response to methylphenidate medication in the patient group on day 8 could be demonstrated by separating patients at screening into 2 subgroups, of which their BFI at screening was ≤ and > 5.41 (average score of the baseline BFI). For the subgroup whose BFI values were greater than the average BFI value at screening, the median BFI score was 6.28. The median BFI value was 5.00 for all patients on day 8. For those patients continually undergoing methylphenidate on day 8, their median BFI value was 4.67. Therefore, the effect of methylphenidate was demonstrated in patients continually taking methylphenidate, as the medication could have a trend to reduce the BFI score on day 8 for those patients whose baseline BFI values were greater than the average value of the patient group at screening. This medication effect was more obvious in patients aged ≤65 years. The median BFI value on day 8 for patients aged ≤65 years and continuing with methylphenidate was 3.00, indicating the difference in median BFI values was greater than 2 units. However, such early response was not observed in the patient subgroup with baseline BFI values less than the average BFI at screening even in patients aged ≤65 years (median BFI of this subgroup being 3.83). Similarly, such early response was not observed in patients in the day 28 patient group.
Discussion
Of the potentially eligible patients approached, 55% refused to join the study. One patient refused to start treatment after recruitment, and less than half of the patients recruited continued methylphenidate till day 29. One-third of the patients who had started to take methylphenidate complained of intolerable side effects and stopped treatment before day 8, even though they were taking only 5 mg daily that was quite different from what was being reported in other studies, while methylphenidate was considered quite well tolerated even at higher doses.6,12 It has been known that the percentage of eligible patients that were finally recruited into study is not high, and the percentage of patients that manage to continue study is relatively low. Ling et al 13 reported the Royal Marsden experience that only 64.8% of the eligible patients were recruited to palliative care clinical trials, and only 44.4% of the eligible patients managed to complete the study. The high percentage of patients refusing to join the current study and the even lower percentage of patients who managed to continue study till day 29 were probably worth for further discussion. As the main reason of eligible patients refusing to join this study was fear of side effects, it would be possible that patients who had joined the study felt less tolerable to the common side effects of methylphenidate, namely nervousness and insomnia, 14 both of which may be aggravated by the fear of having side effects.
A study reported that response to methylphenidate was associated with higher baseline fatigue but not with higher baseline depression or sedation. Additionally, day 1 improvement was highly sensitive as a predictor of long-term improvement. 15 In our study, we identified better response to methylphenidate in subgroup of patients and in patients ≤65 years old. The fact that younger patients responded better to methylphenidate is worth consideration. This may be because of better tolerance to side effects of methylphenidate in younger patients, and further study may be worth to look into this aspect. In this study, we also demonstrated early response to methylphenidate, as the significant difference in mean BFI score could be detected on day 8 of assessment. The finding that no statistically significant difference can be detected on day 29 might be due to the small number of patients that were still on methylphenidate. However, it may also be due to the fact that patient’s condition may have deteriorated further over time so that the beneficial effects of treatment may no longer be demonstrable after a prolonged period of time.
The current study indicated that clinical application of methyphenidate would be more appropriate to patients of younger age and to patients whose BFI score at screening was greater than the median BFI score, as described in this study (ie, patients with “more fatigue” before the start of treatment).
There are several limitations for this study. This is a single-arm study that limits conclusion about effectiveness. Recruiting less than the predetermined number of patients into the study may also affect the interpretation of results obtained, and the results of the subgroup analysis may have to be interpreted with caution. The dose of methylphenidate was low compared to other randomized trials and single-arm studies.6,7,12 The starting dose of methylphenidate for this study was determined by local experience, but dose escalation was allowed. The reason for most patients in this study taking no more than methylphenidate 10 mg daily may be worth or further exploration, for example, it may be interesting to interview patients who have joined or refused to join the study where there was a fear of methylphenidate or its side effects from cultural aspect.
Conclusion
In conclusion, although this study could not demonstrate a strong beneficial effect of methylphenidate for management of fatigue in Chinese patients with cancer, methylphenidate may still be useful in selected patients. Further study should be considered to better evaluate the factors predicting good response to treatment so as to better identify patient groups that may benefit from the treatment. Close monitoring of clinical beneficial effects and potential side effects are important when prescribing methylphenidate for relief of cancer-related fatigue.
Footnotes
Acknowledgments
The author would like to express gratitude to nurses and research assistants of the clinical departments involved, who have helped in patient recruitment, data collection, and data entry. The authors would also like to thank patients who have participated in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.