
Abstract
Background:
Palliative care consultations teams (PCCTs) promote comprehensive health but only if the PCCT can influence actual care. The purpose of this study is to document the types of recommendations made by a PCCT, determine the rates at which recommendations are implemented, and identify the factors related to implementation.
Results:
The mean number of recommendations per patient was 1.44 (standard deviation = 1.81), and 57% of the recommendations were implemented. Discharge and goals of care recommendations were significantly more likely to be implemented than recommendations for pain, symptom management, and consultation of other services.
Conclusions:
Although PCCTs may have suggestions about how to guide care, many of those recommendations are not implemented. Future research is needed to understand how to maximize the impact of PCCTs.
Keywords
Palliative care programs are increasingly common in hospitals around the United States 1 and research has begun to document the utilization and efficacy of palliative care consultation teams (PCCTs) within this system of care. One avenue of research has characterized the types of recommendations made by PCCTs. Chong et al 2 studied the work of a PCCT in a VA medical center and found that team recommendations most often focused on pain and symptom management, discussion about goals of care/prognosis, advance directives, patient and family support, and discharge plans. Examining a PCCT in an academic medical center, Manfredi et al 3 found similar results. In both studies, recommendations involving discharge planning were the most common, whereas recommendations regarding advance directives were least common.
Another line of research has investigated the rates at which PCCT recommendations are implemented. The PCCTs must navigate the professional politics of providing consultation to other medical teams, yet they cannot have an impact on quality of care if their recommendations are not followed. In their VA study, Chong et al 2 reported that the PCCT made an average of 2.84 recommendations per patient, and an average of 2.39 (84%) was implemented. Similarly, the team studied by Manfredi et al 3 made an average of 4.2 recommendations per patient, and 91% of them implemented. These high implementation rates suggest that PCCTs make recommendations that consulting teams find appropriate and useful. Yet to date, previous studies have not undertaken a more detailed analysis of recommendation implementation to investigate whether implementation rates differ depending on the type of recommendation, the professional discipline making the recommendation, or the characteristics of the patient. In order to improve the effectiveness of PCCTs, it is important to understand why recommendations may or may not be implemented.
The goal of the current study was to add to the growing research literature on the utilization of palliative care teams. We conducted a retrospective chart review to document the number and type of recommendations made by a PCCT to the original care team and implementation rates by type of recommendation and discipline making the recommendation. We also conducted multivariate analyses to identify patient and organizational factors that predict whether recommendations are made by the PCCT and whether they are implemented.
Methods
Data Source
This electronic medical records review study was conducted at a Midwestern, urban Veterans Affairs Medical Center. The medical center has a 5-person PCCT consisting of a physician, nurse practitioner, psychologist, social worker, and part-time chaplain. We reviewed consultations to the PCCT that occurred between January 1, 2009, and December 31, 2010, when the PCCT was in its second and third year of operation. The PCCT was consulted on 657 unique patients, and a random sample of 200 patients was chosen for these analyses. The sample size was based on a power analysis conducted using G*Power 3.1 based on a moderate effect size of .3 4 and α set at .05 to maintain power at .80.
If a patient had multiple palliative care consultation requests within the time frame of the study, only the first consultation was included. We documented recommendations from the first visit of each PCCT member within 1 week of the initial request for consultation. Only recommendations that suggested an action be taken by the original treatment team were recorded. This excluded recommendations for future involvement by the PCCT itself (eg, ongoing psychotherapy by the palliative care psychologist, palliative care social worker will obtain forms to complete advanced directives), conditional recommendations (eg, “If patient’s progress continues to deteriorate, recommend nursing home placement”), and recommendations that would not likely appear in the medical record if ever implemented (eg, “Discontinue nonessential activities”).
In total we reviewed 208 patient charts; 8 patients were excluded because the PCCT never had the opportunity to see the patient, because the patient was discharged, transferred, or died. Consultation requests from inpatient psychiatry (n = 1) and hospice (n = 1) services were excluded because of their infrequency, leaving 198 cases in the final analyses.
Consultation Data Extracted
For each patient we recorded date of the consultation, date of admission, date of death, age at consultation date, sex, primary diagnosis, location within the hospital at the time of consultation, age at death, and location where the death occurs. Date of consultation was coded from 1 to 24 based on what month in the 2-year time period the consultation occurred. For each recommendation made by the PCCT, we recorded the professional discipline making the recommendation and verbatim text of the recommendation. The research team independently coded each recommendation into thematic categories; discrepancies were resolved in a consensus conference. Characteristics of the response to each recommendation included the details of the action taken by the original team and the fidelity of implementation. Fidelity of implementation was coded 0 if the recommendation was never implemented, 1 if the recommendation was implemented in a way that was consistent with the intent of the recommendation but not the specific action recommended (eg, hydrocodone was administered for pain relief when morphine was recommended) or 2 if the implementation was consistent with the original recommendation in intent and action (eg, Senna was recommended as a laxative, and Senna was prescribed and administered).
Data Analysis
Descriptive statistics were used to characterize demographics of the patients, the location of the patient at the time of consult, and the number of recommendations generated and implemented. A binomial logistic regression was used to investigate which patient and consultation characteristics predicted whether recommendations were offered by the PCCT. Location at consultation was dichotomously dummy coded using “general medical inpatient unit” as the reference category in contrast to “intensive care unit.” Patient diagnosis was transformed into a dichotomous dummy-coded variable with cancer as the reference category in contrast to all other diagnoses combined. Interactions between age and diagnosis, and between location and diagnosis, were tested but dropped from the final model because they were not statistically significant.
Results
Table 1 summarizes the patient and consultation recommendation characteristics. The mean patient age at consultation was 69.55 years (standard deviation [SD] = 11.65, range = 39.28-91.93). The sample was predominately male (97%), which reflects the patient population overall at this VA. The most common diagnosis among the patients was cancer (59%), and 51.50% of the patients were seen in the general medical inpatient unit. For over half (55.50%) of the consultations, the PCCT made at least 1 recommendation to the providing physician. A total of 287 unique and traceable recommendations were made, and the average number of recommendations per patient was 1.44 (SD = 1.81, range = 0-10).
Demographic and Recommendation Characteristics (n = 200).
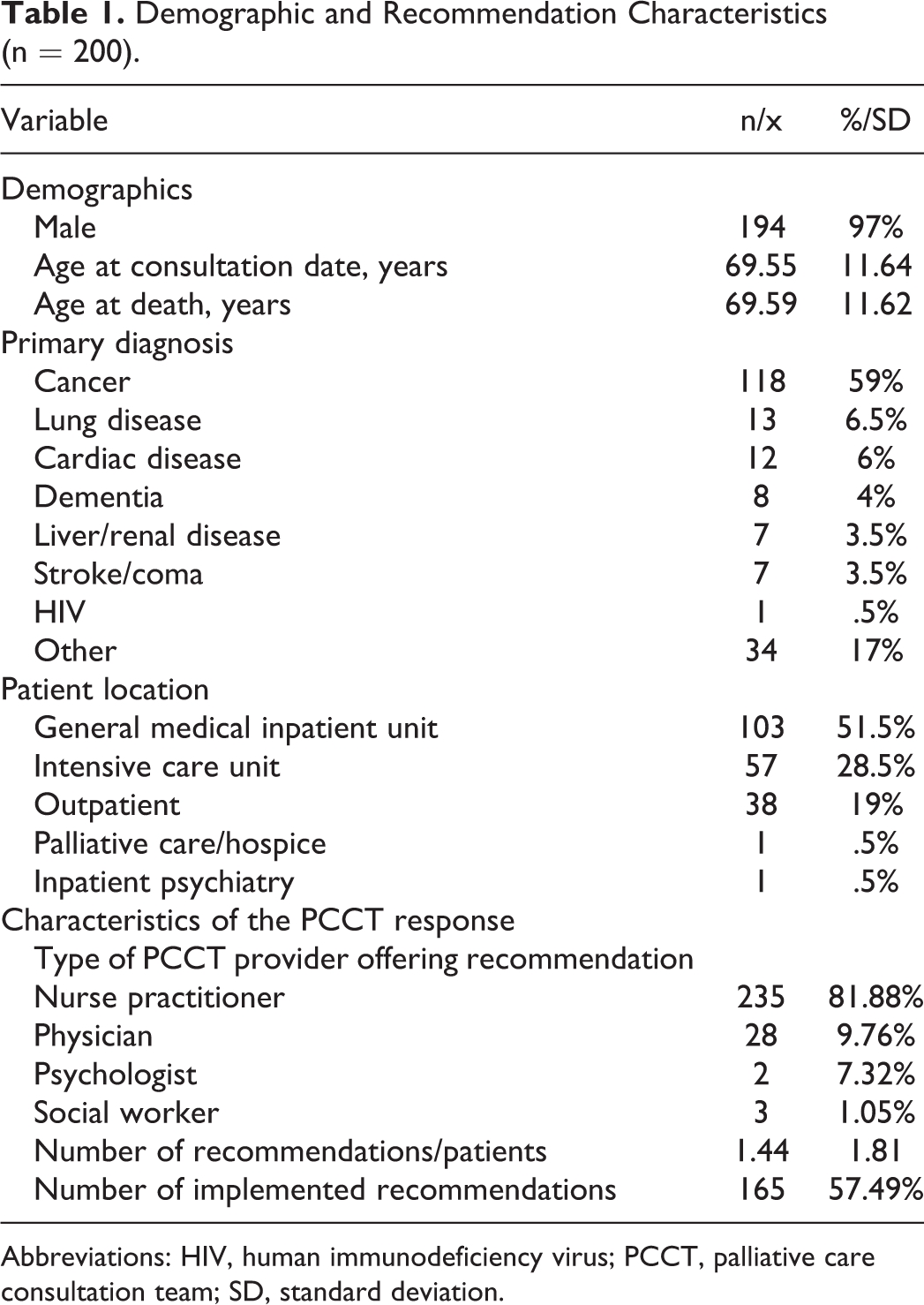
Abbreviations: HIV, human immunodeficiency virus; PCCT, palliative care consultation team; SD, standard deviation.
Table 2 shows the results of a logistic regression predicting whether a recommendation was made, based on the age of the patient, the patient’s diagnosis, and the location of the patient (other independent variables were tested in earlier models, were not statistically significant predictors, and were therefore dropped from the final model). Location of the patient at the time of consultation was the only significant predictor; the odds ratio for intensive care unit (ICU) compared to general medical inpatient unit was .42, and the odds ratio for the outpatient setting compared to the general medical inpatient units was .20 (P = .01 and P = .000, respectively). To interpret these odds ratios, ICU patients and outpatients were 58% and 80%, respectively, less likely to receive a recommendation than general medicine inpatients.
Logistic Regression Results.
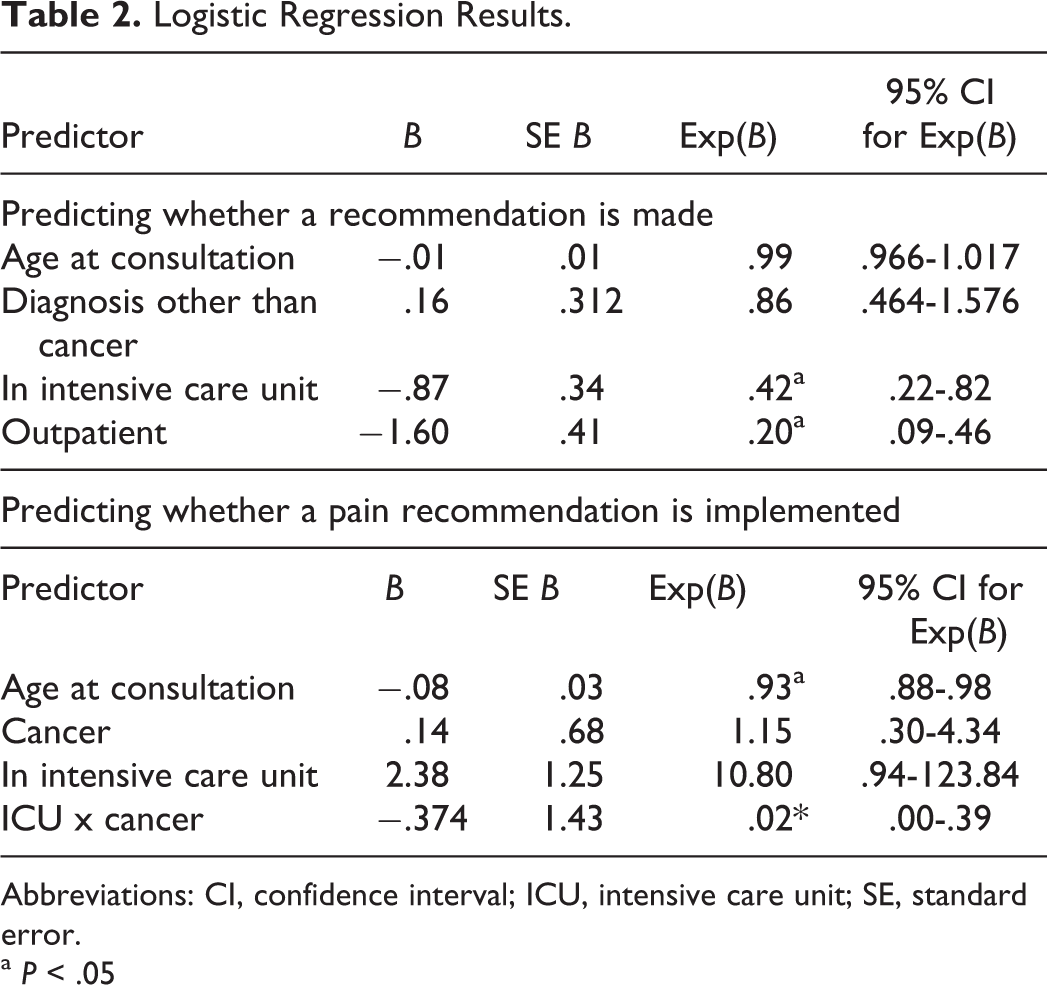
Abbreviations: CI, confidence interval; ICU, intensive care unit; SE, standard error.
a P < .05
Recommendations fell into 6 main categories (see Figure 1): pain management (eg, “consider dexamethasone, may be effective for bone pain”), other symptom management (eg, “needs bowel routine, order daily Senna”), discharge recommendations (eg, “this patient may benefit from short term rehab”), suggestion to transition to comfort care measures only (eg, “consider stopping simvastatin in light of comfort measures only”), consultation for other services (eg, “evaluation by psychiatry to clarify diagnosis and assist with medical management of depression/anxiety”), and miscellaneous (eg, “attempt to avoid restraints,” “transfer to private room”). A chi-square (χ2) test of independence revealed significant differences in the frequency of types of recommendations, χ2 (5, N = 287) = 88.07, P = .00. Pain management recommendations were the most frequent, followed by recommendations for other symptom management, consultation for other services, discharge, and transition to comfort care. The majority (82%) of the recommendations were generated by the nurse practitioner on the PCCT, with the remainder generated by the physician (10%), psychologist (7%), and social worker (1%).
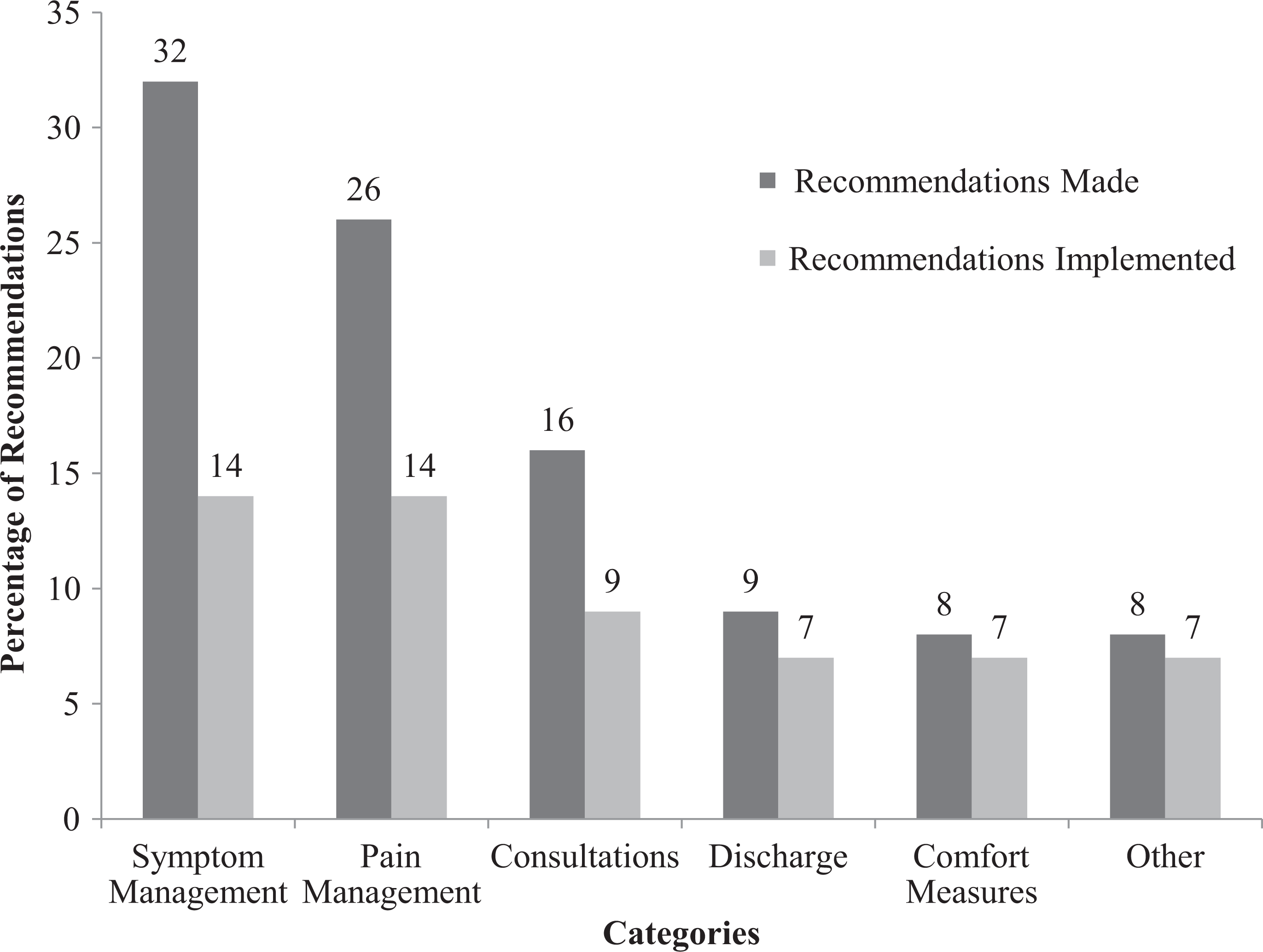
Percentage of recommendations made and implemented, by category (n = 287).
In all, 57% of the recommendations were implemented. Of those, 90.5% were consistent with the original recommendation in intent and action and 9.1% were consistent with the intent of the recommendation but not the specific action. The implementation rate per recommendation type is illustrated in Figure 1. There was a significant difference in implementation rates across the types of recommendations, χ2(5, N = 287) = 19.681 P = .00. Recommendations regarding discharge, comfort measures, and “other” were implemented more frequently than recommendations regarding pain or other symptom management and consultation of other services. In contrast, there was no significant difference in implementation rates across different team members, χ2(3, N = 287) = 2.44, P = .49.
Among the 43% of the recommendations never implemented, we attempted to identify factors associated with nonimplementation in the 3 categories with lowest implementation rates, pain management, symptom management, and consultations for other services. There were no significant associations in regression models predicting the implementation of symptom management or consultation recommendations. The results of the logistic regression for pain management recommendations are shown in Table 2. There was a significant effect of age, P = .01, Exp(B) = .93, and a significant interaction between location of patient at the time of consultation and diagnosis, P = .01, Exp(B) = .02. For each 1-year increase in age, the likelihood of having a pain recommendation implemented decreased 7%. Patients in the ICU with cancer were less likely to have pain recommendations implemented than patients in the ICU without cancer (29.40% implemented vs 70.6%). In contrast, patients in general inpatient medical units with cancer were more likely to have pain recommendations implemented than patients with other illnesses (60% implemented vs 40%).
Discussion
Palliative care services improve the quality of life in patients with life-limiting illness 5 and reduce overall health care costs. 6 Yet, PCCTs can only accomplish these goals if they find a way to contribute their expertise to patient care. For a PCCT, this often comes through the recommendations they provide in their consultations. Results from the current study suggest, however, that although PCCTs generally offer several timely recommendations for the patients they evaluate, their recommendations may not be implemented at ideal rates.
The PCCTs offer a range of recommendations that address issues relevant to patient care. 2,3 Pain and symptom management are by far the most frequent types of recommendations perhaps reflecting the most common, easily assessed issues for patients. 7 Less frequent, but no less important, are recommendations that address consultation to additional health care providers and suggestions regarding transitions in care and discharge. Patient location also seems to matter, as the PCCT may be less likely to offer recommendations for patients in the ICU than other settings, perhaps because assessment is more difficult or patient needs are already maximally managed. Similarly, the recommendations may be less necessary for relatively healthy outpatients. The PCCTs do appear to offer relevant, comprehensive suggestions in their consultation recommendations, but there may be ways to enhance the reach of their work in some settings and with some kinds of patients.
Yet, even when relevant recommendations are made by the PCCT, just under half are never implemented. In this study of a VA-based PCCT, 43% of the recommendations were not implemented, with rates variable across categories of recommendations. On one hand, the PCCT recommendations that advocate for a transition to comfort care and a specific discharge plan tend to be followed faithfully. Clinicians may readily accept these recommendations as being within the purview of palliative care teams, 8 enhancing the likelihood of their implementation. On the other hand, recommendations about pain, symptom management, and consultation by other disciplines are less often implemented. Physicians may tend to discount these recommendations from the PCCT, believing they themselves are competent to address pain and other symptoms and can care for patients adequately without involving still more providers. 9
Among patient and contextual characteristics associated with recommendation implementation, pain management recommendations are implemented less often for older patients. For every 1-year increase in age, pain management recommendations are 7% less likely to be implemented. Our results are consistent with previous studies that have documented that older adults receive less aggressive pain management than younger adults. 10,11 The reason for that discrepancy remains unclear, whether it is due to actual bias in the care of older adults or to the misperception of the complex pharmacokinetics and pharmacodynamics of pain medications in older patients. 12
We should point out that our implementation rate (57%) is substantially lower than the rate reported in 2 previous studies (84% 2 ; 91% 3 ). Methodological differences are likely the explanation, as we documented implementation of each unique recommendation suggesting an action be taken by the original care team, whereas previous studies documented implementation of entire categories of recommendations as well as recommendations the PCCT would likely implement themselves. Our methodology reflects our interest in how the PCCT functions in collaboration with other medical teams and are therefore less an indicator of the overall service the PCCT provides to patients, and more an indication of how the PCCT is affecting the care the original treatment team provides. Still, these differences highlight the importance of understanding methodological differences when comparing results from research in this area.
Several limitations of this study should be noted. First, we only tracked chartable recommendations whose response was likely to be documented in the medical record. Although “meticulous oral care” or “terminate all nonessential activities” are recommendations that address patient’s quality of life, they are not routinely documented in the medical record despite their value. Second, we do not have data on the type and frequency of services that the PCCT provides itself. Future research that documents all the services that PCCTs provide, not just recommendations to other providers, is needed in order to understand how broadly the PCCT influences patient care. Perhaps most importantly, we were unable to document why a recommendation was not implemented. Medical providers have many conversations that are not documented in the medical record, and we were not privy to informal communication that may have resulted in changes in care. Nor did we have information about other factors that could influence recommendation implementation, such as patient refusal of the recommendation, change in patient status, linguistic subtleties of how recommendations are framed, provider perceptions of palliative care services, and the integration of the relatively new PCCT in the hospital culture. All of these factors point to possible areas of exploration for future research.
Our study has several implications for practice. For example, when PCCTs educate hospital staff about their expertise, they may consider highlighting their specialty in pain and symptom management, as these recommendations are most frequently made but least frequently implemented. Furthermore, given that certain recommendations are less likely to be implemented, such as pain recommendations for older adults, palliative care medical providers might consider ways to increase their likelihood of implementation. For example, using stronger language or presenting a more extensive rationale for the recommendation in the consultation report could stress its importance and encourage implementation. Being part of a consultation team requires nuanced communication and collaboration skills, and members of any PCCT are only successful to the extent to which they find a way to operate effectively within the complex hospital culture. 13 Errors in communication, especially interprofessional communication, occur with moderate frequency in palliative care, 14 thus it is especially important for the interdisciplinary palliative care team to find effective communication strategies with the physicians charged with implementing their recommendations.
Palliative care teams are a relatively new specialty service within VA and other hospitals, and their roles are still being defined and developed. Although these teams have unique expertise that can help other care providers, their acceptance within medical systems has been gradual. The current study identifies several factors that are related to the effectiveness of PCCT consultations, but additional research is needed so that PCCTs can launch targeted initiatives to overcome interpersonal and institutional obstacles and provide effective recommendations that improve quality of life in patients with life-limiting illnesses.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.