
Abstract
Introduction:
Low creatinine and albumin are found among the chronically ill patients. This study retrospectively reviewed albumin and creatinine levels for survival in patients upon admission.
Methods:
Records of patients admitted over 2 months were reviewed. Recursive partitioning analysis (RPA) identified cutpoints in albumin and creatinine that predicted survival. Kaplan-Meier survival, Cox proportional hazards, and stepwise Cox analyses identified prognostic factors.
Results:
Of 83 patients, 81 were assessable. Variables for worse survival were albumin <3.1 g/dL, creatinine >0.93 mg/dL, and male gender. Albumin by continuous, median, RPA, and tertiles was significant; creatinine by RPA. Hazard ratio for albumin >3.1 was 0.28 (P < .001) and for creatinine >0.91 mg/dL was 1.8 (P = .046).
Discussion and Conclusion:
Albumin and creatinine are prognostically important.
Introduction
Low creatinine and albumin are commonly found among patients with advanced chronic illnesses. Creatinine is derived from muscle creatine through creatine kinase. Creatinine levels are influenced by lower muscle mass, creatine kinase activity, glomerular filtration, and renal secretion. 1–4
Albumin is a globular serum protein. Albumin levels are affected by transcapillary leak, lymphatic return, hydration, synthesis and metabolism rate, and external losses through skin, urine, and gastrointestinal tract. 5–8 Albumin synthesis is regulated by hepatic interstitial oncotic pressure. Both cytokines and acidosis blunt albumin synthesis. 6–7 Cytokines modulate albumin gene expression, albumin catabolism, and transcapillary leak. 9–10 Transcapillary escape of intravascular albumin is normally 4% per hour and reflects hemodynamic stability and normal endothelial function. Transcapillary leak can increase 100% to 300% with injury, with chronic illnesses, during sepsis, and with cigarette smoking. 11–13 Normally, 12 to 15 g of albumin are catabolized daily. During starvation, albumin production and catabolism are simultaneously reduced. 6–7,14 Low serum albumin in inflammatory diseases and cancer is due to increased transcapillary leak and redistribution and not due to reduced synthesis. 15 Under normal conditions, 50% to 70% of total albumin is located in extravascular spaces, primarily interstitial spaces of muscle and skin. This distribution is drastically altered during an inflammatory response, with trauma, cancer, and renal disease. 16–19
In hospitalized and critically ill patients, the adjusted risk of dying is 2.6-fold higher for those with low serum albumin and 3.8-fold higher for those with low serum albumin and elevated C-reactive protein (CRP). 20 A low serum albumin in hospitalized patients predicts hospital-acquired infections, longer length of stay as well as increased mortality. 21 In a general review, for each 2.5 g/L decrease in albumin, mortality increases 24% to 56%. 19,22
There have been claims that the association of albumin with mortality meets the causal criteria of temporal sequence, reproducibility, strength of association, dose–response relationship, and biologic possibility.19,23 Biologically, albumin protects vascular endothelial cells and removes reactive oxygen species.25–31 Albumin reduces platelet aggregation and is associated with improved wound healing and bowel function.10,31 Albumin promotes neuron survival. 32 However, cause and effect are not truly established. Infusions of albumin do not consistently improve outcomes. 33–36
Serum albumin and creatinine levels have not been used as prognostic indicators in inpatient palliative medicine patients. We retrospectively studied consecutive patients (both cancer and noncancer patients with terminal illnesses) admitted to the inpatient palliative medicine unit to determine whether albumin and creatinine levels were prognostically important. The secondary objective of this study was to determine whether albumin and creatinine levels predicted disposition at discharge from the hospital that is yet to be completed.
Methods
This was a retrospective review of the medical records of patients admitted to the Harry R Horvitz Center for Palliative Medicine inpatient unit over 2 months (from November 1 through December 31, 2011). Due to the retrospective nature of this chart review, the study was deemed as “IRB Exempt.” Patient diagnosis and social security number, age, gender, albumin and creatinine levels upon admission, discharge plan, placement in skilled nursing facility or extended care facility, hospice referral or inpatient death, and survival from the time of admission were collected. Eligibility included admission or transfer to the palliative medicine unit, serum creatinine and albumin levels upon admission to the unit, and over 18 years old. Patients were followed through discharge. The protocol adhered to the policies of the Cancer Center Data and Safety Monitoring Plan, version 3 guidelines in accordance with National Cancer Institute regulations. Study data were managed using Research Electronic Data Capture (Redcap). This study met the criteria for a waiver of consent, and there was no direct interaction with the patients. The results obtained did not impact patient’s clinical care. Data were extracted from the electronic medical record (EMR). Physician notes in the EMR were reviewed by investigators. Once data had been collected, all identifiers were removed prior to permanent archival. Survival data were collected over 3 months after the end of the study (December 31, 2011). Survival was determined from the date of initial admission to the unit.
Statistical Analysis
Data analysis was performed using SAS statistical software (Cary, North Carolina). Albumin and creatinine were analyzed as continuous variables, 2 groups based on median and 3 groups based on tertiles. Categorically, variables were summarized as frequency, counts, and percentages; continuous variables as means, standard deviation, median, and range for albumin and creatinine, and various groupings based on recursive partitioning analysis (RPA). Kaplan-Meier survival curves were generated for survival by albumin and creatinine cutpoints. Continuous medians and tertiles and RPA by a log-rank splitting method were used to identify cutpoints in albumin and creatinine levels that predicted survival. Cox proportional hazards analysis was used to identify prognostic factors for survival. Stepwise Cox analysis with variable entry criterion of P ≤ .10 and variable retention criterion of P ≤ .05 was used to identify multivariable prognostic factors. The hazard ratio (HR) >1 indicated a greater risk of death; HR <1 indicated a lower risk of death or better survival.
Results
Of the 83 patients admitted over 2 months, 81 (97.6%) were entered on the study. One exclusion was due to a duplicate record and the second for missing data. Demographics and albumin and creatinine levels are shown in Table 1, and the overall survival is illustrated in Figure 1. Variables associated with a worse survival (HR > 1) were albumin less than 3.1 g/dL, creatinine greater than 0.93 mg/dL, and male gender (Table 2 and Figures 2 and 3). Through RPA, patients with albumin >3.1 g/dL had better survival than those with <3.1 g/dL (P< .001). Individuals with a creatinine <0.91 mg/dL had better survival than those >0.91 mg/dL (P = .035). Every variation in albumin (continuous, median, RPA, and tertiles) was significant, whereas creatinine was only significant by RPA cutpoints (Table 2). In multivariable analysis, only albumin and creatinine were prognostic. Hazard ratio for an albumin greater than 3.1 was 0.28 (95% confidence interval 0.15-0.52; P < .001). For a creatinine >0.91 mg/dL, the HR was 1.8 (95% confidence interval 1.01-3.21; P = .046).
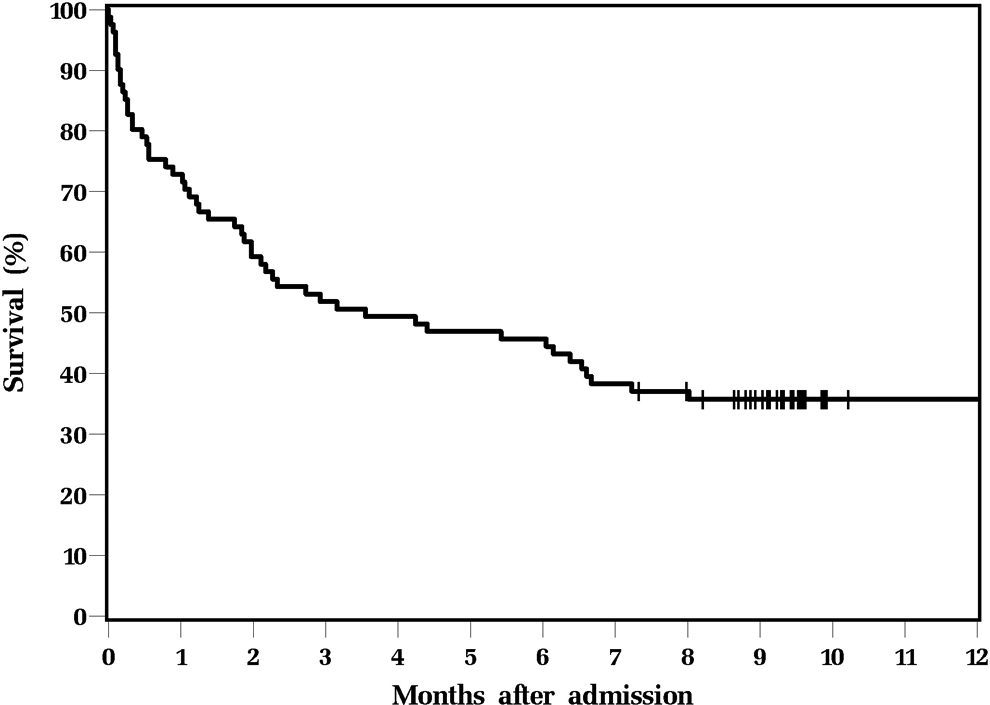
Survival of the Cohort.
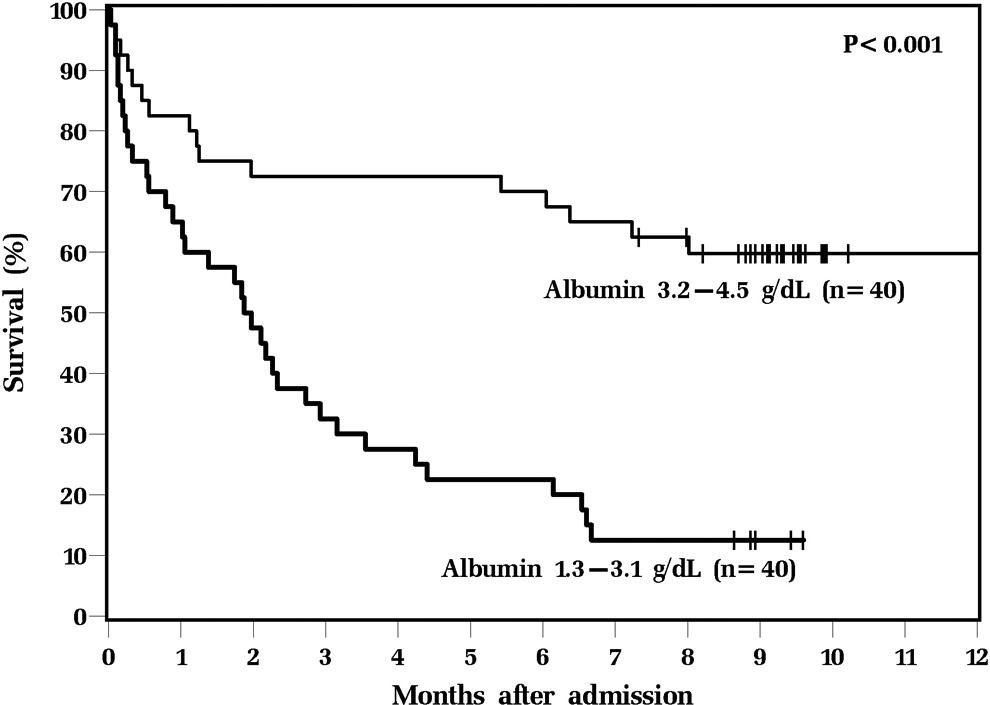
Survival Based on Serum Albumin Levels.
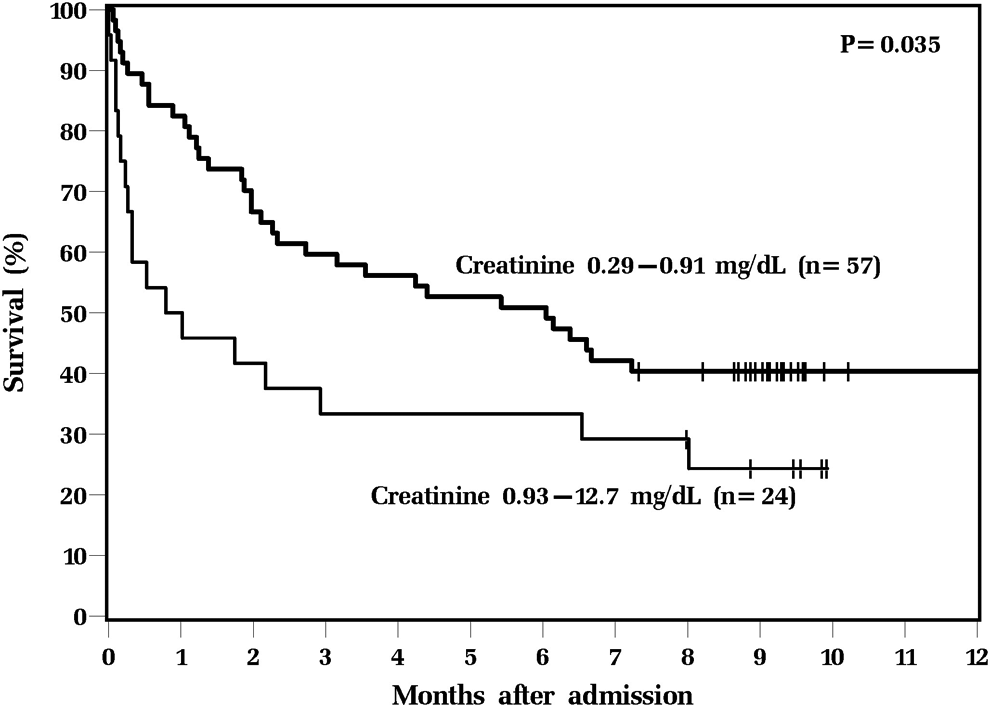
Survival Based on Serum Creatinine Levels.
Descriptive Information for 81 Patients.
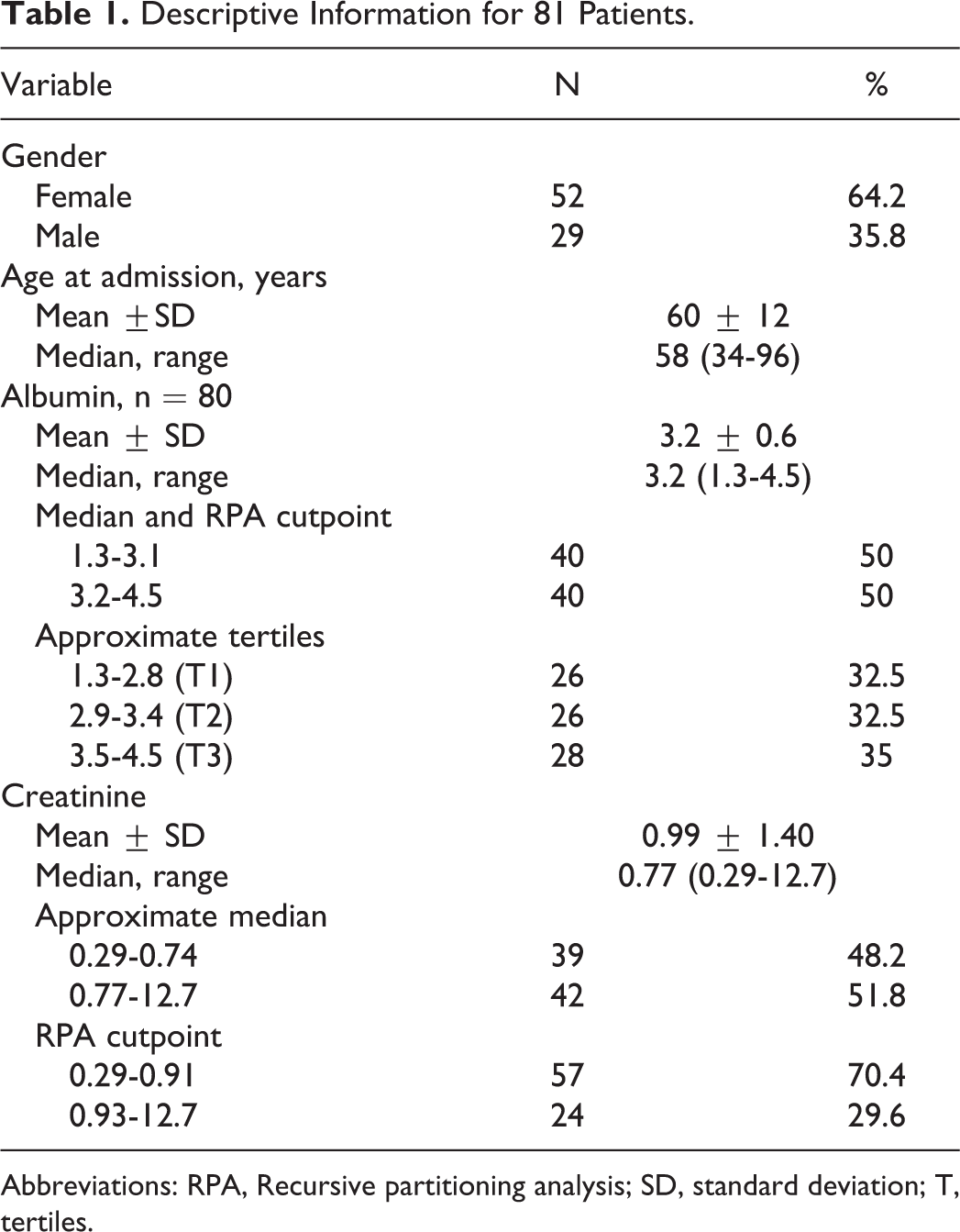
Abbreviations: RPA, Recursive partitioning analysis; SD, standard deviation; T, tertiles.
Prognostic Factors for Overall Survival.
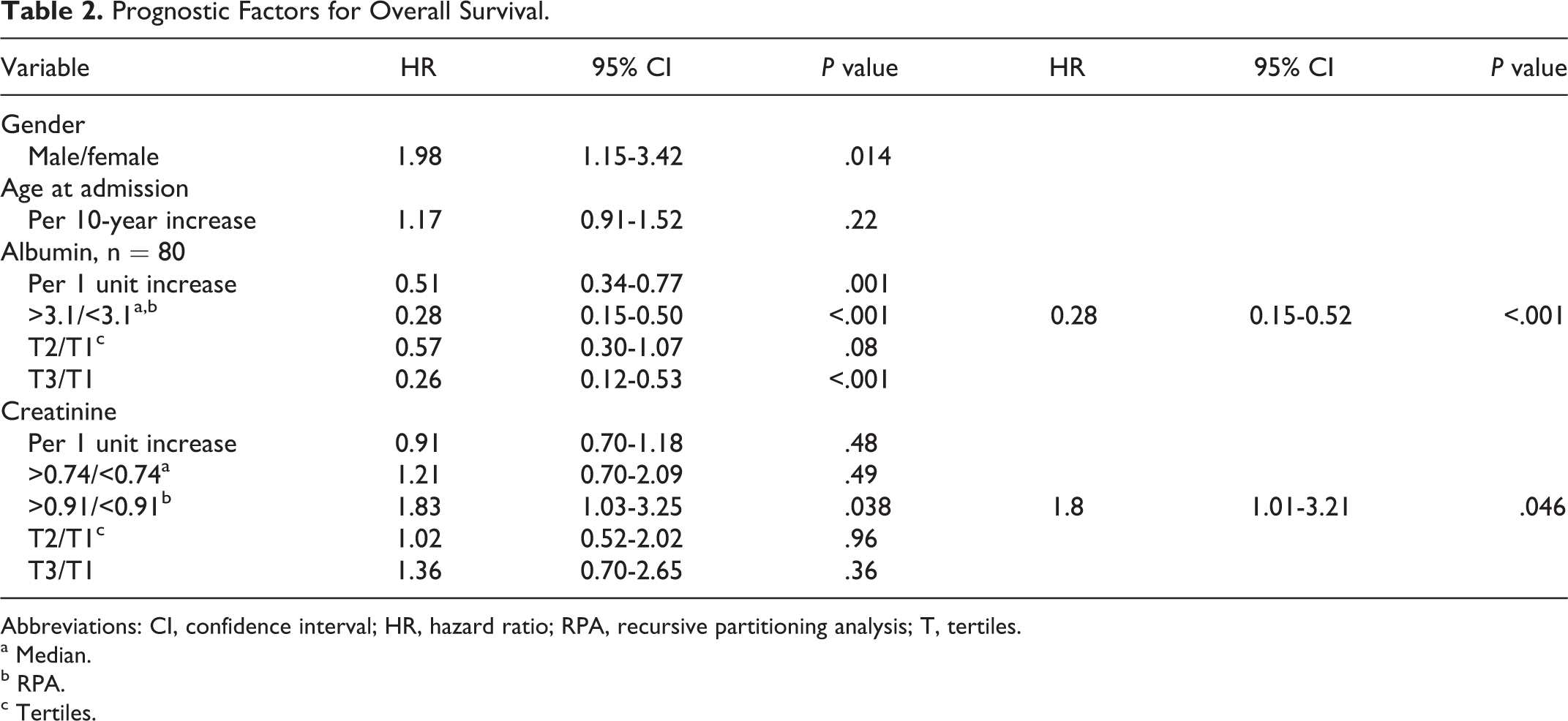
Abbreviations: CI, confidence interval; HR, hazard ratio; RPA, recursive partitioning analysis; T, tertiles.
a Median.
b RPA.
c Tertiles.
Discussion
This is a hypothesis-generating retrospective study. A prospective study should be done to confirm these findings. Correlations should be made with various known prognostic markers such as palliative prognostic scores and indices, CRP, lymphocyte and WBC levels, handgrip, and measures of muscle mass using bioelectrical impedance analysis, DEXA scans, ultrasounds, computed tomography scans, or magnetic resonance imaging. Correlations of albumin levels with cancer-related complications such as venous thromboembolism, gastrointestinal symptoms, dyspnea, hemoglobin levels, and prevalence of decubitus ulcers would be of interest. Further investigation will require a larger population.
This retrospective study agreed with the primary hypothesis that serum albumin and creatinine are prognostically relevant in palliative medicine patients. We assumed that a low creatinine would reflect lower muscle mass and predict a shorter survival. We found the opposite to be true. We found a robust correlation of survival, particularly with low albumin.
There are multiple weaknesses to this study. This is a retrospective review that cannot account for all confounding variables that are known to predict survival such as the CRP, WBC, and lymphocyte counts, nor was albumin compared with prognostic indices such as the Palliative Prognostic Index. Significance could be diminished or lost taking into account these variables. The patient population was heterogeneous and consisted of patients with cancer and noncancer terminal illnesses. However, this reflects the usual population on our inpatient palliative care unit.
This study is especially applicable to inpatient palliative care population due to minimal exclusions made. Participants in this study were reflective of typical inpatient palliative care population and exhibited common diagnoses, symptoms, and creatinine and albumin levels found in patients.
Conclusions
This retrospective review found that albumin and creatinine levels are prognostic indicators in an inpatient palliative care unit. Further investigation is needed to confirm these findings as well as to provide further explanation of creatinine and albumin as prognostic factors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.