
Abstract
A qualitative study was conducted with semistructured interviews to explore the experiences of stress in 20 palliative care providers of University Malaya Medical Centre in Malaysia. The results were thematically analyzed. Nine basic themes were generated: (1) organizational challenges, (2) care overload, (3) communication challenges, (4) differences in opinion, (5) misperceptions and misconceptions, (6) personal expectations, (7) emotional involvement, (8) death and dying thoughts, and (9) appraisal and coping. A total care model of occupational stress in palliative care was conceptualized from the analysis. This model may inform the development of interventions in the prevention and management of stress in palliative care.
Introduction
Stress is a universal experience that affects all human beings. It is a constellation of physiological, cognitive, emotional, and behavioral reactions as a person is confronted with perceived threats and challenges. 1 Sources of stress can be external, such as major life events and daily hassles, or internal and self-generated. 2 –5 According to the Transactional Model of Stress and Coping, as a person transacts with the source, cognitive appraisals occur in which the relative significance of the source as a threat is judged (primary appraisal), and the capacity of the person to cope with the threat is evaluated (secondary appraisal). 6 Therefore, stress can be defined as a particular relationship between the person and the situation, which is appraised by the person as threatening his or her own well-being and exceeding his or her resources to cope. 6
Regarding primary appraisal, the situation is evaluated from 2 aspects: motivational relevance and motivational congruence. When evaluating motivational relevance, the individual appraises the relevance of the situation to his or her own well-being. When evaluating motivational congruence, one appraises the congruence of the situation with one’s goals. 7 Hence, stress can also be defined as a perceived discrepancy between what one has in a given situation and what one wants in that situation. 8 For secondary appraisal, 2 ways of coping are described: problem-focused and emotion-focused coping. Problem-focused coping refers to one’s capacity to improve the situation so that it is more congruent with one’s goals. Emotion-focused coping refers to one’s capacity to adapt to the situation when the situation remains incongruent with one’s goals. 7
In a review study by Vachon, stressors identified in the palliative care context were grouped into personal factors and work factors. Examples of personal factors were age, sex, ethnicity, family status, financial status, work experience, qualifications, personal values, coping styles, and social support. Examples of work factors included work environment problems such as communication problems within the organization, inadequate resources and unrealistic expectations of the system; role problems such as role strain, role ambiguity, and role conflict; and patient–family problems such as dealing and communicating with dying patients, young patients, and noncoping family members. 9
Primary appraisals described in palliative care included a perceived mismatch between the person and the environment and a perceived imbalance between job demands, job resources, and workplace support. 9,10 For secondary appraisals, good communication with patients, families, and coworkers, being connected with patients, practice of exquisite empathy, optimism, self-efficacy, and receiving social support were reported in problem-focused coping; positive reinterpretation, meaning making, humor, practice of mindfulness, healthy lifestyle engagement, turning to religion, praying, and taking a break were mentioned in emotion-focused coping in palliative care. 11 –15 Regarding adverse consequences of stress in palliative care, vicarious traumatization, compassion fatigue, and burnout were described. 16 –18
Although there is a substantial body of literature on staff stress in hospice and palliative care, most of the studies applied quantitative methods and primarily focused on nurses. 9,19 –22 Therefore, we conducted this qualitative study to explore the subjective experiences of stress of both doctors and nurses providing palliative care in Malaysia.
Methods
The study was approved by the ethics committee in University of Malaya and was conducted in the University Malaya Medical Center, a tertiary hospital in Kuala Lumpur, Malaysia, from January 2012 to May 2013. Participants were recruited through convenience sampling. All participants provided informed consent. Semistructured interviews were carried out with palliative care providers by the principal investigator using a voice recorder and a set of questions (Table 1). The 8 questions were designed by using the biopsychosocial–spiritual model of suffering as a guide. 23 A total of 10 doctors and 10 nurses were interviewed. The average interview time for each participant was 13 minutes. Eighteen interviews in English were transcribed verbatim. Two Malay transcripts were translated into English. Transcription and translation were done by the principal investigator and a medical student who are both proficient in the 2 languages.
Questions in the Semistructured Interviews.
The interview transcripts were imported into a qualitative software called NVIVO 9 (QSR International Pty Ltd, Victoria, Australia) for thematic analysis based on Braun and Clarke. 24 First, repeated reading of the whole data set was done to enable familiarization with data. Second, segments of data were organized into initial codes. Third, codes were sorted into potential themes via identification of meaningful patterns across all codes. Fourth, themes were reviewed with the reading of all codes in each theme for pattern coherence, followed by reading of the entire data set in relation to each theme to confirm the validity of individual themes. These themes were used as basic themes that were structured into organizing themes based on the principles of thematic network analysis. Organizing themes were linked to form a global theme that captured the concluding results of the data as a whole. 25 Fifth, the themes were named and defined. Sixth, the report was written with the support of literature review. The entire process was conducted by the principal investigator, a palliative care physician. A trained research assistant with a master of science degree in mental health studies was involved independently in data coding and thematic generation. The reviewing and revision of themes were independently carried out by another palliative care physician, 2 psychiatrists, 1 psychologist, and 1 nursing lecturer.
Results
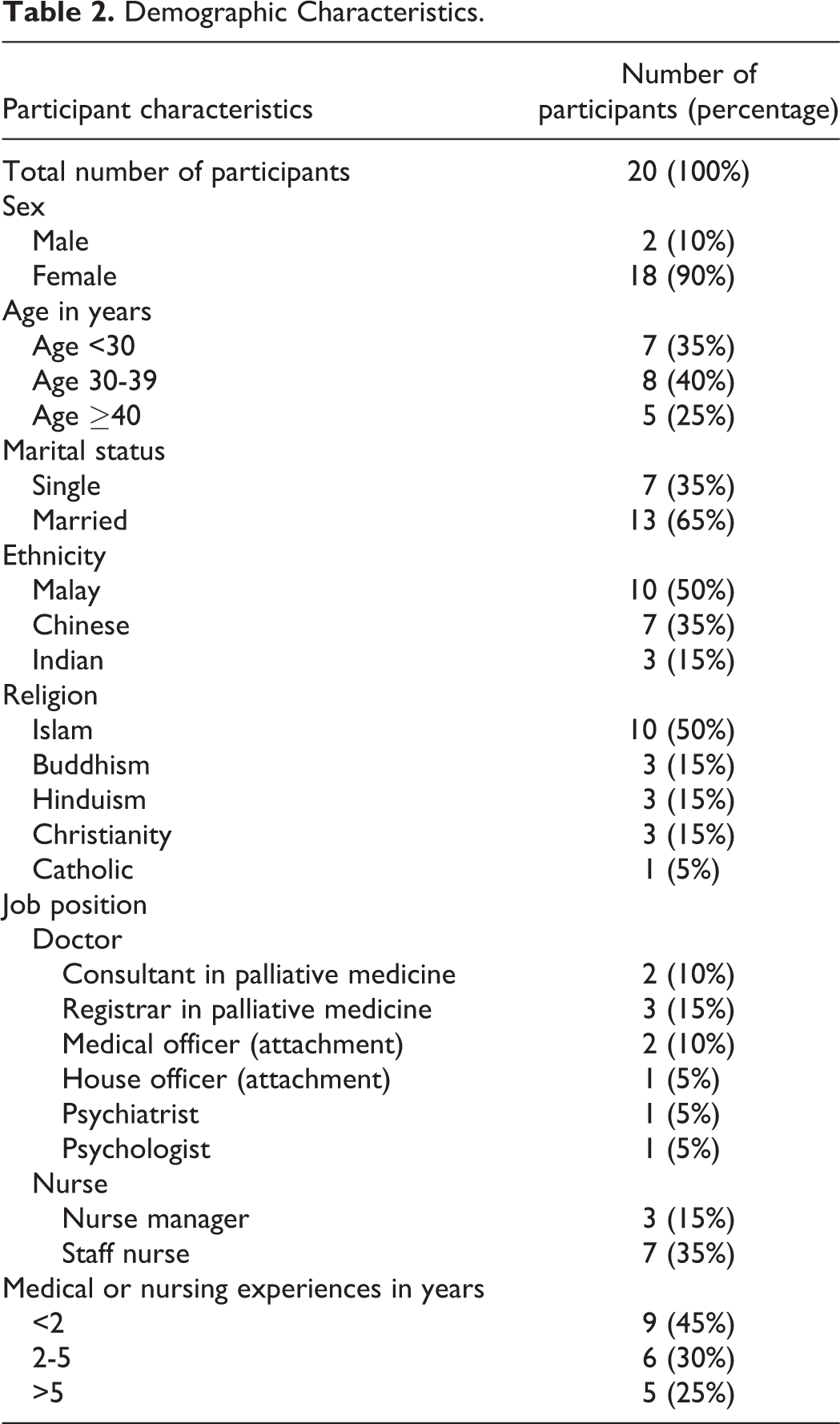
Demographic characteristics of the 20 palliative care providers are presented in Table 2. After repetitive reading of all interview transcripts, coding was performed by screening all the data for experiences of stress. A total of 378 codes were generated. These codes were categorized into 9 basic themes: (1) organizational challenges, (2) care overload, (3) communication challenges, (4) differences in opinion, (5) misperceptions and misconceptions, (6) personal expectations, (7) emotional involvement, (8) death and dying thoughts, and (9) appraisal and coping. Regarding data saturation, all 9 themes were represented within the first 8 interviews. The final theme of death and dying thoughts was generated during the eighth interview. Calculated interrater reliability in percentage agreement was 72% ([8 + 13]/[9 + 20] × 100). 26 Using thematic network analysis, 3 organizing themes were developed that strung the first 8 basic themes together to form a model of palliative care stress, as shown in Figure 1. The 3 organizing themes were (1) health care, (2) interpersonal care, and (2) self-care. These 3 organizing themes were linked to form the global theme of “total care” that captured the principal message of the results. The model was named the Total Care Model of Palliative Care Stress (TC Model).
Demographic Characteristics.
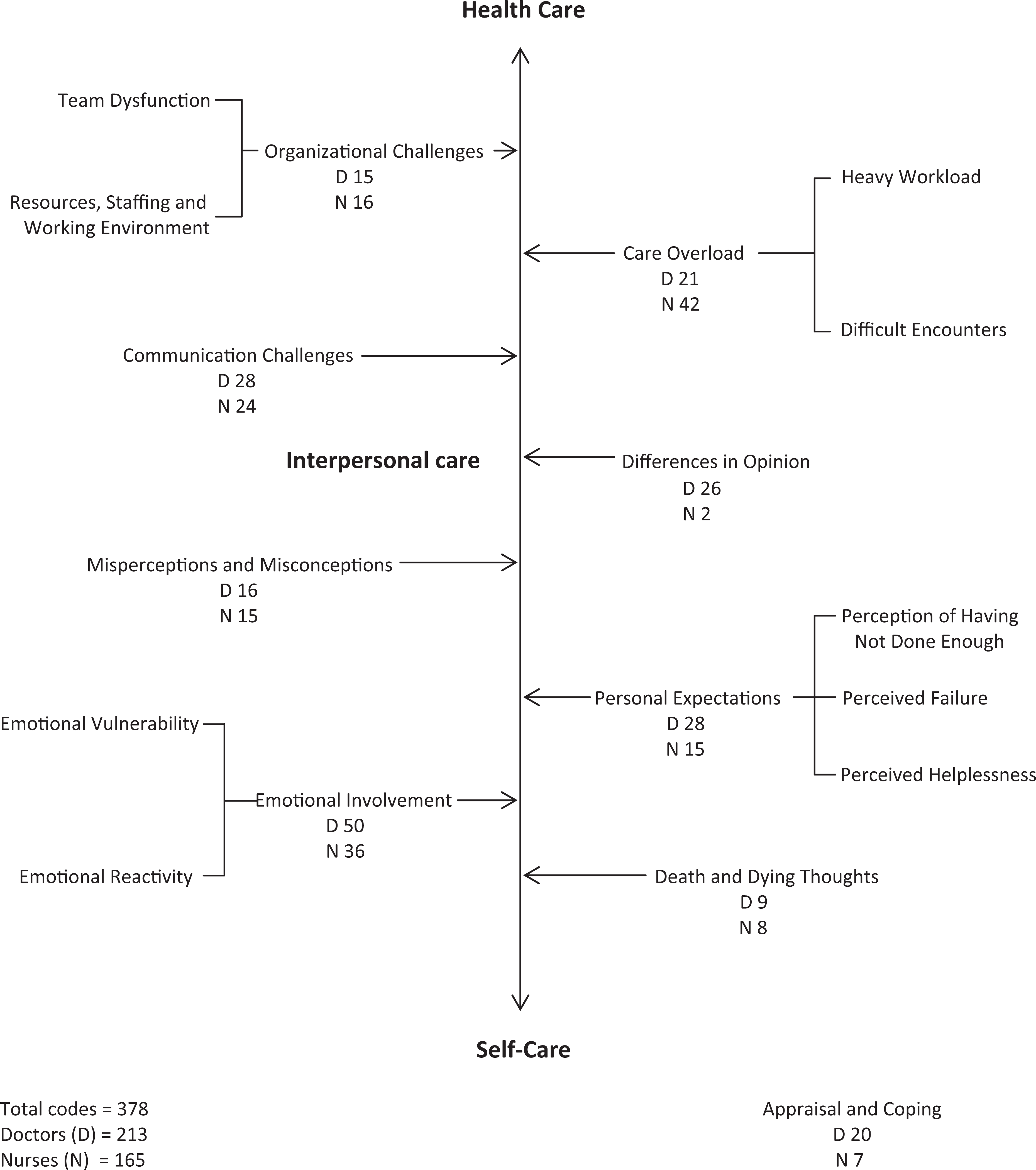
The Total Care Model of Palliative Care Stress (the TC Model).
During thematic network analysis, the first 8 basic themes that represented stress in palliative care providers were recognized to be related to problems in caring for others and the lack of caring for oneself. Hence, total care was conceptualized as a continuum of caring for others at the top end and caring for oneself at the bottom end, as represented by the 2 organizing themes of “health care” and “self-care” in Figure 1. The themes near the top, such as organizational challenges and care overload, emphasized the problems in caring for others; and the themes below, such as personal expectations, emotional involvement, and death and dying thoughts, focused on the importance of taking care of oneself. In the middle, the organizing theme of “interpersonal care” consisted of the themes of communication challenges, differences in opinion, and misperceptions–misconceptions that emphasized equal significance of both. Following the construction of the TC Model, the themes were named and defined, followed by a literature review and writing up of the report. The themes are elaborated subsequently together with selected segments of transcripts that represent each theme.
Organizational Challenges
Organizational challenges are problems related to deficiencies of the structure or function of the organization. The 2 subthemes were (1) team dysfunction and (2) resources, staffing, and working environment. Regarding team dysfunction, health care providers expressed frustration when other team members did not share a similar team philosophy. The lack of a caring attitude was noted in some team members. There were those with a couldn’t-care-less attitude, and those who were not performing their duties. Some performed their duties reluctantly, some rushed to complete their tasks, and some were not cooperating with the team to deliver care to patients. Patients who called for attention were ignored. Team members were more worried about writing reports rather than the actual care of patients. Additionally, complaints made to superiors were ineffective as no action was taken.
Competence issues were also reported, such as the unsatisfactory capability of other team members to palliate patients’ suffering or to communicate effectively with patients. The lack of team communication was mentioned, such as incomplete clinical handover during night shifts. The lack of team support was also mentioned, such as the late arrival of doctors when help was needed. Apart from attitude, competence, communication, and support problems within the team, interteam issues were described too. These included disagreement between teams with respect to active or conservative treatment, absence of follow-up reviews from other teams, and reluctance of other teams to admit patients from the emergency ward.
For resources, staffing, and working environment, health care providers complained of inadequate hospital resources, for example, infusion pumps, ripple mattresses, and wound dressings. It was tough to borrow medical equipment from other wards, and staffing was inadequate. Inefficient use of time, resources, and manpower was described when health care providers were asked to see patients, carry out research, and teach students at the same time. As for the working environment, the stress of integrating into the system to understand how things work was also reported by a new staff. Some team members are not cooperative. They do their own work. They never help others. This makes me a bit stressed. (Nurse 2) So far we don’t have any conflict within our team, but when other nurses come to cover for palliative care, that is a stress for me because they don’t know anything about palliative care, and they don’t do their duties well. (Nurse 7) Some of the nurses, they just don’t care. If I talk to them, they just walk away. I complain to the nurse manager, but I think they won’t change. I think that’s how they are trained, that’s how their attitude is. (Doctor 6) Especially the juniors, I feel sometimes they are like, no feeling. They just follow orders, but no feeling to the patients. And then when patients request for something, they take time to attend to patients. They want to finish their reports, because they are afraid that they cannot finish their work. (Nurse 3) Working in the team, I would say definitely nothing is perfect, especially working with different disciplines, doctors, nurses or therapists. I used to feel a lot of stress when other disciplines haven’t really achieved what we wanted them to do. (Doctor 2) I have problems borrowing infusion pumps from other units. And our budget for Duoderm dressing is finishing. Everything is money. We can’t help without money. Even simple thing like Ripple mattress, we don’t have. We’ve to loan it from other units. (Nurse 1) It’s not that I feel stressed, but it’s like because of staffing problems, the patients cannot get good quality care. (Nurse 8)
Care Overload
Care overload refers to the excessive burden of care (quantitative overload) or having to deal with complex care situations (qualitative overload). The 2 subthemes were (1) heavy workload and (2) difficult encounters. Due to the lack of staff, health care providers described their incapacity to attend to all distressed patients. They could not provide enough attention to patients or attend to them immediately when patients called because of other commitments. Sometimes they received simultaneous calls from a few patients and some of the calls were perceived as unnecessary. Health care providers reported that there were too many things to do and too many orders from the superiors. Too much time was needed to see patients. There were some that could not finish their work quickly because it was necessary to be very gentle and polite.
Regarding difficult encounters, problems with patients or relatives were reported. Health care providers expressed their stress when patients remained in pain despite analgesia. They were in a dilemma when patients continued to ask for analgesia before the minimum interval. They worried that patients might collapse during medication administration. Some were stressed when patients scolded them for failed branula insertions, while some were unhappy when patients regarded them as being rude despite their best effort to be gentle. It was difficult when patients asked for definitive treatment when they refused treatment in the beginning and came back after widespread metastases. It was also difficult to deal with patients who refused to accept their dying because of their unrealistic expectations for cure or prolongation of their lives. Conversely, patients with suicidal ideas created difficulties too.
Relatives can be a source of stress too. Health care providers were often asked by relatives to continue close monitoring and do everything for dying patients, including futile treatment. They expected health care providers to do more. Some tried to interfere with treatment decisions and even gave instructions for health care providers to follow. They were impatient while waiting for doctors to arrive and for medications to take effect. It was challenging to deal with relatives who were not able to accept patients’ death. It was also hard when relatives begged health care providers to hasten the death of patients. Other than these, nurses said that it was difficult for them to carry out their nursing work when too many relatives were around. Sometimes there were excessive numbers of visitors that came to the hospital when patients were dying. Not enough time to see patients in need is my main stress. For example, if we have three calls at the same time, three calls all together, and we know like someone is in pain, we need to titrate medication; someone is clearly dying; and family calls for help. We cannot be present in different places at one time. I find this a bit stressful, that is, not able to attend to all patients at the same time. (Doctor 2) Here we have four staff per shift, but we are taking care of twenty patients. Sometimes the patients are very ill. Sometimes they want more attention, but we can’t help. (Nurse 2) I mean, in palliative care, you had difficult patients, where, whatever you do doesn’t seem to be helping. I guess that is stressful, in that you want to try to relieve it as best as you can. But everything just seems so refractory and pointless. (Doctor 9) Sometimes I do my best for them but they’re still not satisfied. They complain that we don’t attend to them but in fact we’re attending to them regularly. Sometimes it’s because they call us when we’re in the middle of doing a procedure, we can’t attend to them immediately. Therefore, they get angry with us, and then they get angry with everything we do in the ward. That makes me stressed. (Nurse 9) Sometimes the relatives are too fussy. We are doing our best, but they are still not satisfied. For example, there was a patient, his mother always complained that we were rude to her son, though we have tried to be as gentle as we could, but in her eyes we were still very rude to her child. We apologized to her but she still complained to our nursing manager. (Nurse 10) When patients are dying, some relatives ask us to do something more. Even though doctors have explained everything, to make patients comfortable, but the relatives still ask us to do something more. For example, they ask us to resuscitate patients with fluid or oxygen, and they ask us to call the doctors stat. And they keep on asking, “Where is the doctor? Where is the doctor?” (Nurse 2) Some family members they can’t accept what is happening. They blame doctors for not doing the right thing. That’s why, sometimes their children are dying, they say, “Oh. Doctor. Not yet,” like in denial stage. They can’t accept that their children are in the process of dying. So they are not happy. I’ve even seen a father, like going to quarrel with the doctor, like going to punch the doctor, because he’s in the denial stage. (Nurse 6)
Communication Challenges
Communication challenges are problems that arise in the process of information exchange. The following are a few examples of communication challenges reported in the study. Some health care providers found communication of prognoses challenging. They had problems finding the right words to say when they discussed about prognoses. They were concerned that patients might become highly emotional when the truth was told. Meanwhile, they were cautious in not giving false reassurance. Dealing with difficult questions from patients could be stressful. For example, it was not easy to answer patients when they asked why their lives could not be extended. A lot of time and patience were required in end-of-life conversations. Health care providers complained about not having enough time to build rapport with patients. Time was needed to explain patients’ situations in details, at times in multiple occasions. Their patience was tested when dealing with patients who were angry, fussy, or in strong denial. Some felt overwhelmed to listen repetitively to patients’ suffering. Language barrier complicated end-of-life discussion for some staff. Lastly, communicating with patients who could not communicate or who were not keen to communicate was a great challenge too.
Regarding patients’ relatives, health care providers reported stress when they were asked a lot of questions by the relatives. Sometimes, relatives came at different times and asked the same questions. It was especially difficult to deal with big families because health care providers were concerned about misinterpretations when too many relatives were involved. They were also concerned about different opinions from different relatives. It was hard to please patients and all their family members equally. Some relatives were fussy and remained unsatisfied despite explanation. There were those who prevented health care providers from delivering bad news to patients. Relatives who grieved intensely or agitatedly were not easy to deal with.
For team members, a lack of communication between colleagues and a lack of consideration for colleagues’ feelings were described. For example, some health care providers did not listen to their colleagues; some gave instructions without considering their colleagues’ feelings; and some did not follow instructions. It was frustrating to see team members communicating with family members rather than patients. It was also frustrating to see team members communicating without empathy. I think communication is the main challenge. Our patients tend to be more sensitive compared to other patients because they know that they are in the final stage of their lives, but a lot of them they don’t want to accept it. That’s why I think my challenge is like how to approach them in a right way. (Doctor 8) If you want to help patients or their relatives you must know them well. For me, it takes time, not just one hour, not just one day. You must have good rapport. It’s not easy. (Nurse 1) When patients talk to us, we listen to their problems. Sometimes I want to say, I feel like it’s a bit of a burden. I’ve to let go, talk to other people and share the burden. Other than that I am ok. (Doctor 4) Aside from that, you know full well I find communicating in other languages is quite stressful … I think the listening part is easy. I can listen to someone speaking Chinese and maybe understand snippet of it, but I think sometimes when you try to give answer or explanation, if you don’t have the vocabulary and the words, I find it incredible, I find it quite a significant barrier. I mean you can express the empathy and the care, you can express that nonverbally but I think when people are asking for answer or explanation, it’s a bit hard, I find it a little bit harder to do. (Doctor 9) Some of them didn’t want to communicate. They were not keen, and they said, “No need. No need. I don’t want to talk to you.” … That’s why I think working in palliative care; communication is the most challenging thing. It’s not the medication. It’s how to deal with their emotions. (Doctor 8) I am stressed when I have to deal with a lot of relatives. I mean not the primary relatives like husband and children, but more of the relatives like uncle, aunt, cousin-in-law, etc. (Doctor 4) Some relatives can be very fussy. “Oh, nurse, how is the situation? How about this one?” or “Nurse, why is it like that?” They call us and ask, “Why? Why? Why?” on everything! We explain to them but they are still not satisfied. They still can’t understand. (Nurse 4) A lot of time we do have family that says, “Oh. Don’t tell the patient that he is dying.” “Don’t tell him he has cancer, whatever.” … I had this family who got angry with me because I told patient that she has not much time left. I can’t remember whether the son or the daughter was angry. But then the patient wanted to know and I spoke to her husband and he also said yes. (Doctor 6) I found a lot of other teams; they are not actually giving adequate information to the patients. I think this creates a lot of problem. Like the patient I saw just now, he didn’t know what’s wrong with him. (Doctor 8)
Differences in Opinion
Differences in opinion refer to interpersonal issues that arise due to differences in beliefs or perspectives. Disagreement among health care providers was described. Health care providers expressed unhappiness when their superiors gave unnecessary treatments to dying patients. Some were unhappy when they disagreed with the management from other teams. Health care providers were annoyed when primary team insisted patients to continue treatment despite wishing to stop. They were also confused when different specialists had different opinions. Differing views on patients’ prognoses, treatment options, and goals of care among health care providers were described. At times, orders were not followed due to disagreements.
Disagreements between health care providers and patients or relatives were also reported. Health care providers were frustrated when patients disagreed with treatment at early stage but came back late. They felt stressed when they disagreed with relatives who asked them to do everything necessary to save patients who were imminently dying. They were unhappy when patients or relatives disagreed with their treatment recommendations; this was made worse when there were conflicting views between patients and relatives or between different relatives. Health care providers said it was difficult to ignore the relatives because patients needed their support. Apart from treatment options, sometimes patients and relatives had different views on end-of-life discussions. For example, some patients wanted to talk about end-of-life preparations, but their families objected to it. It’s a dilemma because two sides go together. For the palliative side we are focusing on symptomatic treatment and we help patients to understand their conditions, but the oncology side they keep on giving treatment. (Nurse 8) We explain that the condition is actually quite bad, and the survival is not so good. But some relatives are so much attached to patients that they don’t want to accept it. They want us to do everything. There goes the conflict. (Doctor 5) I think it’s a unique thing here in this culture, because it’s less individualistic and then it’s a lot more about what family members expect you to do or things like that on behalf of the patient. I do experience that sometimes where the patient wants this and the family members want that. It’s hard to please everybody, sometimes it’s a true dilemma of who do you listen to and what should you do, but I think so far when I encounter this I always try to remind myself this, of course I mean if we can solve the problem amicably is the best, but who do we have more responsibility toward, I think the patient is the patient, and is our patient, and of course, is patient which comes first, exactly speaking. Again it is easier said than done, but it’s always, it’s situation by situation, sometimes I do think we can get so gray, you know not black and white, can get so gray that, it’s a unique situation. (Doctor 10) We follow whatever the patient says if he is compos mentis. But then, over here, I think sometimes they gave way to what the family wants, not what the patients want. This is a bit of problem for me to adjust to. (Doctor 3) We feel that we can do better in terms of pain control. For example, sometimes patient told us, “I’m willing to try whatever medication that can relieve my pain.” But family perceived that, “You’re quite good already. You shouldn’t change your pain medication.” Obviously what we want and what family wants are very different. (Doctor 2) I feel that I was in a very difficult situation because of the family conflict. I know that the patient is actually my duty rather than the family. But I do understand that the family are the one who are supporting the patient and who’s been there for the patient. So I should take into account what they think and what they express. (Doctor 3) Like one previous patient, divorced, and she wanted to see her son, but the husband didn’t allow her son to come. Even when she was dying, terminal, and gasping, she still wanted to see her son, but her husband wouldn’t allow. (Nurse 3)
Misperceptions and Misconceptions
While misperceptions refer to mistaken first impressions, misconceptions are mistaken beliefs after substantial thinking. It is easier to rectify the former than the latter. Misperceptions and misconceptions about the role of the palliative care team as well as the timing of referrals were highlighted by several palliative care providers. Instead of referring patients to the palliative care team based on the needs of patients and their families, many patients without palliative care needs were referred to palliative care because they were dying and the primary team did not know what to do for them. Sometimes they were referred because there were no caregiving relatives. The admission of patients who were gasping to the palliative care ward and their demise shortly after their transfer resulted in significant distress for a few palliative care staff. It was as though the palliative care ward was a “dumping site” for the dying. Inappropriate referrals, late referrals and the absence of a guideline for referrals were sources of stress for several members of the palliative care team. Other misperceptions and misconceptions from colleagues included seeing do not resuscitate orders as equivalents to withholding all treatments, seeing continuation of aggressive treatment in dying patients as a form of nonabandonment, and not seeing spiritual care as a responsibility of the health care team.
The lack of palliative care awareness among patients and relatives was also described. Some patients and their relatives did not know what palliative care was and perceived referrals to palliative care as sign of giving up. They also perceived conservative management as doing nothing for patients. Therefore, some patients and relatives rejected palliative care right at the beginning. There were also those who feared morphine. They rejected the use of morphine despite explanations, resisted dosage adjustment, and requested health care providers to stop the use of it. As for sedation, some relatives asked why patients were not waking up once sedation was given; and some requested to taper or discontinue sedation because they wanted to talk to patients for the last time. One common perception was that cancer being misinterpreted as suffering or death. Some believed that telling patients about cancer or dying could generate depression, instigate giving up, and expedite death. I think some colleagues don’t know our actual role and they refer patients to us simply because the patients are dying, or simply because they don’t know what to do, or simply because patients have no relatives. (Doctor 4) I don’t like when they said, “The patient is dying. Can I transfer the patient to your ward?” It’s like our ward is a “dying ward,” for dying patients only. (Nurse 1) I think we need to have a guideline for referral, because if we don’t have one then people won’t know what our role is, and then our ward will be like a “dumping site.” (Doctor 4) Say for example we believe that the patient is not for active resuscitation, and then the patient is admitted under the medical team, for example, and when they see the patient is not for active resuscitation, for them it means no treatment at all, when we believe that all the possible causes that could be reversed should be treated. (Doctor 3) Yes, stressed, especially when patients don’t want to receive the kind of care that we are giving. When they are in pain, they have misconceptions about the medications, misconceptions about palliative care. So they reject our service right at the beginning. (Nurse 5) Patients and relatives are always afraid of the side effects of morphine. When we say, “This is morphine. I want to give morphine for you as a painkiller.” They will say, “Oh! Morphine?” They will go home and check the Internet about the side effects of morphine. Then they come to the ward and say, “Oh, we don’t want morphine.” And then they tell another patient or another relative. So in the end they all refuse morphine. It happens. (Nurses 4) She’s in great pain. Everyday she’s screaming in pain, but the husband has very strong perception about painkillers, it’s something not good for her, because he has gone through a major surgery himself, so he rejected all kinds of painkillers, including morphine, even tramadol! He said tramadol doesn’t help. So he asked us to stop everything and what we could do was just sat there and watched her in pain. But we couldn’t do anything else. So that was quite stressful for us, to see patient that way…. Despite our explanation and everything he just rejected all painkillers very strongly, very strong perception about what he believed, and what he believed was this kind of disease was doomed to suffer, and suffering was something that was a must for cancer. It’s a must for this kind of disease. So there’s nothing and no way to change that kind of perception, thus it’s quite a difficult situation for her, even for her children as well. (Nurse 5)
Personal Expectations
The stress of personal expectations refers to discrepancies between one’s expectations and the clinical reality. Three subthemes were identified: (1) perception of having not done enough, (2) perceived failure or incompetence, and (2) perceived helplessness. Health care providers expressed feeling stressed when they did not have enough time to see patients in need, they could not attend to distressed patients or relatives immediately, they were not able to see patients more frequently, and they did not know whether they had done enough. Some wished to do more for patients, or were upset because they could not help patients go home, while some felt sorry because they could not fulfill patients’ requests, such as giving patients privacy with single rooms or allowing patients to eat and drink when instructions were given to keep patients nil by mouth. This guilt of not doing enough was made worse when relatives criticized health care providers for not doing anything.
Perceived failure or incompetence reported by health care providers included failure to prevent the death of young patients, failure to delay death of patients who were expecting their family members to come home from abroad, or failure to reduce the suffering of patients who refused medications. Failure to keep promises was described when one doctor was unable to fulfill the wish of a patient who wanted to go home for festive celebration as the patient passed away before the discharge. Failure to change perceptions of patients and families about palliative care and morphine was mentioned. Some doctors felt that they failed to make a significant difference for patients. Some said they failed to help no matter what they did. It was frustrating when health care providers did not know the cause of their patients’ groaning when their patients were confused or in a semicomatose state. It was difficult when one did not know how to help patients in strong denial. Confusion about whether to manage some patients actively or conservatively was expressed. The problem of not knowing how to improve palliative care services was also communicated.
The perception of having not done enough and perceived failure were associated with a sense of helplessness. Health care providers felt helpless when they could not help patients with young children to live longer or help patients to see their loved ones. They felt powerless when patients wanted to end their lives. Some of them were helpless when they realized that there was nothing much that they could do except to keep their patients comfortable, while some articulated their incapacity when dying patients gasped for breath. I feel I’m not doing enough like especially now for the motor neurone disease patients, we are not providing enough home visits for them. Because they need more monitoring, but most of the time we are just waiting for their distress calls, and when they make their distress calls I find that they have been kind of trying to cope, or stressed for some time. (Doctor 2) Occasionally you have patients whom you know they are on the way of dying and those you are close to. Sometimes you feel you want to do more, but obviously you can’t do more except to keep them comfortable. (Doctor 6) He kept on asking me, “Can I go home for Raya?” And I kept telling him, “Yes, we’ll help you.” And then I was away for a week. Yeah, he passed away. These are the patients you feel that something could have been done. (Doctor 1) It’s always difficult because you see patients who are dying and then they are still in the 4-bedded room. I asked nurses to arrange for a single-bedded room but then it’s always difficult. I don’t think they actually have a nice place to die. (Doctor 6) She told me she wanted to taste a bowl of noodle soup. I remember that I couldn’t allow her that because the primary team said to keep her nil by mouth. So she died in the end…. It was the biggest blow for me. Yeah, it was the biggest blow for me…. We should just, the dying, the last day, we should just let them do whatever they want, especially eating. (Doctor 7) Sometimes I feel sad because I can’t help all of them. Even though we have only 8 patients, I can’t see them for the whole day … I feel stressed when I can’t help them to fulfill their needs…. What I do is I just avoid her. I can’t help her. I’ve tried my best but I can help her much. It’s difficult. (Nurse 1) I feel stressed when I fail to relieve patients’ symptoms, like when they remain groaning or screaming in pain despite our medications. (Nurse 9) I feel like I can’t do anything for them. I can only make them comfortable. If they’re in pain, I give them painkiller. If they can’t breathe, I give them oxygen. If they’re dying, gasping, I cannot do anything. (Nurse 4) Let’s say you’ve given patients their medications, and patients still continue to groan, the noise, whoever is with him or her would feel uncomfortable. You can see their relatives moving about, but you can’t help them. You give painkillers, or midazolam to relieve patients’ restlessness, but sometimes it doesn’t work. We also don’t know how to help the relatives. Sometimes I feel so helpless. (Nurse 1)
Emotional Involvement
The stress of emotional involvement refers to the unpleasant emotional participation of health care providers when they journey with palliative care patients and their families. The subthemes were (1) emotional vulnerability and (2) emotional reactivity. Emotional vulnerability is defined as one’s susceptibility to emotional injury. In most cases of emotional involvement, health care providers described their vulnerability in seeing pain and suffering, such as seeing patients’ devastation after receiving bad news, seeing patients develop problem after problems, seeing patients get confused because of different information from different doctors, seeing patients get stuck in emergency ward for a long time because of bed constraints, seeing dying patients undergo unnecessary blood investigations, and seeing patients feel hungry due to fasting prior to investigations or treatments. Some health care providers became emotional when patients were tearful or were upset seeing patients give up. It was hard to bear the groaning of dying patients. It was also difficult to see grieving relatives.
Emotional vulnerability in seeing death and dying was described by many health care providers. Some of them felt depressed knowing that patients were deteriorating. Some were depressed when they spoke about disease progression and felt sad to see patients having very little time left. Witnessing dying was described as a sad and painful experience. One nurse reported her fear of caring for dying patients when she first joined the service. Individual differences in emotional vulnerability were noted. Health care providers were emotionally more vulnerable when they were emotionally attached to certain patients. It was harder to see the death and dying of patients with whom they related well and had good rapport. Emotional involvement was reported to occur more during their junior years. Children, young patients, young patients with children, and patients who were breadwinners were reported to increase emotional vulnerability of individual health care providers. One doctor expressed her vulnerability in seeing elderly patients because of her personal bereavement experience. A nurse expressed her vulnerability in seeing relatives who were very sad and who could not accept the dying of their loved ones. Circumstantial vulnerability mentioned included sudden death, sudden disappearance of patients from the ward, and multiple deaths in a short period of time.
In this study, emotional reactivity refers to unpleasant emotions that arise when one is emotionally involved, such as feeling sad when patients were suffering or dying, feeling angry with demanding family members, feeling frustrated when patients presented late, feeling guilty when patients died during nursing care, feeling helpless when not knowing what to do, and feeling puzzled not knowing why patients had to die. Many health care providers reported that they could not control their emotions. They could not stop themselves from crying in front of patients even when they were consoling patients. They felt that it was incompetent and unprofessional to cry. They said that they could not help patients when they were emotional but it was hard to hide their emotions. As a result, they could not spend a long time with dying patients because of their emotional involvement. Some of them cried every time they remembered their patients who were dead. Some could not sleep because they were thinking about a patient’s death. Some even dreamed of their dying patients and became scared. It took a long time for health care providers to forget their patients who were dead with whom they were close to. The memories of the dead patients stayed at the back of their minds even though it was not affecting their work. Typically the stress involved, for me, it’s more of the emotional burden. Because we are dealing with people who are going to die, and there is always at the back of your mind that they are going to go soon. So, with that in mind, you have to be ready for this emotional experience with this person who you know it’s not going to live for very long. (Doctor 10) I feel like sometimes I am slightly too involved emotionally. They said that with time it will get better. But I don’t think that is the case. I don’t think that it will ever get easy for me. (Doctor 3) It’s very difficult for me to see patients’ suffering, suffering from pain, sometimes I don’t know what patients’ suffering are, because I just know that they are groaning, the sound is not nice, it makes me feel uncomfortable. (Nurse 1) When patients are dying, gasping, you can see their families grieve. Sometimes you’re reminded of your own experience that makes you feel difficult because when you’re emotionally affected, you can’t really help the patients or their families at that time. (Nurse 1) You’re not supposed to have “favorite” in terms of your patients, but there will be certain patients that I feel I’m much closer to them, not because of particular reason, maybe because I can relate better to them … I will get more depressed when I know they are going downhill … I keep thinking about them even after I go home. It is stressful but I don’t think it’s ever affected my work. I can still function but they’re still at the back of my mind. (Doctor 3) We do come across a lot of patients who are still young, or patients with family members that are depending on them, and toward their end of lives, when they got very little time, at those kind of time there will be some … as human we always have some, you know, we are affected emotionally though we are not their relatives. (Doctor 1) I can have more emotional burden toward older people. Especially that, the example that I gave were the older gentleman held my hand, started crying, there’s no family around, they were dying alone, you know, that really got to me. So that was my emotional burden. (Doctor 10) When he talked, he became tearful. The wife said, “Don’t cry. Don’t cry.” Then the wife also cried. I also nearly cried. That kind of situation, if I became tearful in front of them it’s no good, because I think, so unprofessional, the doctor also cried like that. So that kind of scenario made me very hard to handle. I became very emotional. I felt sad. But I think as a professional I shouldn’t cry in front of them. This is my opinion, but sometimes very hard, very hard to hide it. (Doctor 8) I had insomnia for 1 week because of patient’s death. I slept. And then I dreamed about patient. Patient is already dead, but I dreamed about them. I felt so scared. It made me feel stressed but I still can control. When I got insomnia, I took lorazepam. I also saw a counselor because I just wanted to rest. Then I am ok. (Nurse 4) When I first joined the service, I felt scared to see dying patients. (Nurse 9)
Death and Dying Thoughts
Death and dying thoughts refer to reflections on mortality triggered by encounters with palliative care patients. Being reminded of one’s personal mortality could be stressful for health care providers. Many health care providers worried about their own death after seeing their patients’ deaths. They worried about how they were going to die in the future, about getting cancer, and about dying with pain and suffering, like many of their patients. These dying thoughts could happen all of a sudden. Fears of death, suffering, and separation with family were described. Fear of family member’s death was also reported. Some health care providers worried that their family members might go through similar sufferings like their patients. Some imagined themselves dying like their patients while some were reminded of their personal bereavement experiences in the past. The awareness of the certainty of death and the unpredictability of the time and trajectory of dying caused a great deal of distress to many health care providers. Sometimes I think about how I am going to die. Once or twice I have been thinking about that. Initially I felt just a bit sad. After that I expressed it to my friends, and then I was ok … To me, death is a worrying thing. I don’t know whether I’m going to die a peaceful death or a painful death. I don’t know how I am going to die. That is what I was thinking. (Doctor 4) Last 2 days, patient was alright. He could talk. And then suddenly he is dying. Yesterday, I talked to him he was very happy … Because I have many medical problems as well, I think maybe I can also be like that. I have to be aware, like today we are happy, we are still alive, I can do my work, and then tomorrow, I can change very fast. (Nurse 3) I feel very sad because my mother also had cancer, so I think I have a higher chance to get cancer, right? So when I see patients die, it makes me think about my own dying, and I don’t want to die from cancer, with so much suffering, so much pain. (Nurse 7) The patient had breast cancer, with lung and brain metastases. When she’s admitted, she’s ok. Then suddenly she had a lot of difficulty in breathing. I gave her medication, but she’s still uncomfortable. I felt depressed. I talked to a doctor. He told me to rest, but I couldn’t rest. My aunty also has breast cancer, so I think is my aunty going to be like that? (Nurse 4) I am not stressed, but it’s like having empathy, and fear, because we take care of patients, right? We look at their progress, and then suddenly they’re gone, like, how to say, I feel like suddenly I am thinking about my family, like that. Fear, scared, I don’t know, I don’t know what to say, sad, fear, but not stressed, worry also. Worry about my family. If one of my family passes away, how? Myself, I am also scared, scared about death. (Nurse 10)
Appraisal and Coping
Health care providers demonstrated various appraisal and coping methods in facing stress. Stress was described to escalate to a limit from time to time before eventually returning to normal. To deal with care overload, health care providers reported prioritization of visits based on patients’ needs, helping patients bit by bit, trying to understand patients’ and relatives’ perspectives during difficult encounters, trying not to hold grudges and guiding grieving relatives to pray or to do something good for their patients. One nurse explained that sometimes she had to avoid seeing patients whom she could not help despite trying her best. One doctor said she would distance herself from the patients’ relatives when she was too distressed by them, and only returned to see them later.
Health care providers coped with communication challenges by exploring the preferences of patients and families to make things easier. They coped with demanding family members by putting themselves in those families’ situations. They spoke to emotional relatives nicely and in layman terms to assist relatives in understanding the situations. To address differences in opinions, one doctor said that she avoided stress by having learnt to agree to disagree. One junior doctor expressed that she felt relieved when patients died while undergoing unnecessary treatment from other teams.
The stress of emotional involvement was compensated when patients appeared to be more comfortable or when patients’ wishes were fulfilled. Letting go was practiced by some doctors and nurses to cope with the burden of listening to each patient’s problems. One doctor tried to be emotionally detached to avoid getting emotionally involved. Although one doctor said she became less affected emotionally with experience, another doctor said her emotional involvement did not decrease with experience. Regular staff meetings were helpful according to one staff member. In order to be less affected by patients’ deaths, health care providers tried to imagine that their patients would be in a better place. Occasionally, the ward sister organized praying rituals for her staff when too many patients died in a short time. Many health care providers reported feeling a little upset the days their patients died, but they moved on quickly. With regard to death and dying thoughts, health care providers achieved peace of mind by having faith in their religions, praying, and expressing their problems to their friends. I have a lot of priorities, in the sense that if my patients need me more, I will spend more of my time there, but if I think this patient is quite well, he doesn’t need much of my attention, I will not spend that much time there. (Doctor 4) I always try to look back and try to understand especially from the psychology point of view, all the process that the family is going through, how much hurt they are going through and all that stuffs and, so I would try and examine back and try to understand their frame of mind, and I try really not to hold grudges, it’s not about holding grudges, it’s not about you as a professional, they are not yelling at you, they are just venting frustrations. So actually that is very important to know, the psychology of it. And not making it personal. (Doctor 10) I think most of the time I try to remind myself if I were in their places, how would I feel? So in that way I try to think that all their arguments or demands are actually quite justified. (Doctor 3) I think the other thing I find helpful is, as professional we must learn to agree to disagree, because different people look at things in different perspectives. Sometimes we might not agree on the same thing, but if we can see each other’s perspectives, I think it’s ok to be different. (Doctor 2) I would try to be more solution-focused. You cannot run away from people, things that are out of your control. If someone doesn’t do their work then too bad, that’s their issue. But for the sake of the patient, for the sake of the situation, the family, the patient, everything involved, we are professionals, and if you see somebody else is not doing their job, maybe a gentle reminder in a nice way, but you don’t need to be frustrated because of that and keep it inside, and then resulting in a bad environment to work. (Doctor 10) For Muslims, we recite Yasin every Friday, or once a month, or whenever we see a lot of patients die in our unit. (Nurse 1) So far so good, because of my belief in Christianity. There are certain understandings about afterlife and how people deal with their lives, and what do we expect from our lives we are given, when we are alive and afterlife that kind of thing. So, for our belief, there is an eternal life. There is an afterlife which this part of life on earth is not everything. It’s just a short journey that we run and finish with colorful and beautiful results, or with regrets and guilt. It makes me reflect a lot about how I want to live this life for sure, and what do I expect for my afterlife. (Nurse 5) Every time when someone dies, it makes me aware of impermanence, and makes me treasures whatever I have, treasures more on what I have. (Doctor 2) To me, it’s more of learning, yeah, growing opportunity. And I think that, I mean I am biased, coming from myself, but I think this is a better way to approach, working in palliative, dealing with palliative patients, it’s not learning about what that stresses you out so much. But how can you learn and grow as a person, take the positive out of those experiences which you can argue with the most negative experience ever. But you can still gain something positive out of it for yourself and then you can pass it on in your own clinical work onto other people, isn’t it? (Doctor 10)
Discussion
The conceptualization of the TC Model as a continuum of problems in caring for others at one end and problems in caring for oneself at another end highlighted the concept of total care presented in the World Health Organization (WHO) definition of palliative care in 1990. 27 Total care is conceived as an approach that integrates self-care into the caring for others. The concept supports the description of mutual suffering or the interrelated suffering of patients, families, and health care providers in relation to the care of the dying patient. 28,29 In caring for others, caring for oneself should be practiced concurrently. Additionally, interpersonal care was conceptualized from the results to underscore the significant importance of interpersonal factors in the caring for others and oneself. From this current study, the problems of caring for others were represented chiefly by organizational challenges and care overload, as presented at the top of Figure 1.
Organizational challenges were further divided into team dysfunction and issues of resources, staffing, and working environment. Factors crucial to multiprofessional cooperation in palliative care, such as high team commitment, competence in dealing with death and dying, close communication, good interpersonal relationships, autonomy, and team philosophy, were consistent with the stress of team dysfunction due to issues of attitude, competence, communication, support, and disagreement. 30 The lack of resources and staffing affected the ability of palliative care providers to provide good palliative care. Therefore, it was not a question of not wanting to provide good care but was a question of not being able to do it due to resources and staffing restrictions. 31 To improve care, the functioning of the interdisciplinary palliative care team needs to be strengthened systematically based on its deficiencies. Multiprofessional collaboration requires mechanism-based improvement. Issues of resources, staffing, and working environment need to be addressed by the organization.
Care overload was categorized quantitatively into heavy workload and qualitatively as difficult encounters. Not having enough time to complete all tasks and dealing with difficult patients and relatives were ranked in the list of most common stressors of palliative care nurses in Australia. 32 In one survey, heavy workloads were reported to contribute to unnecessary tests and procedures, reduced overall quality of care, and increased complications and mortality. 33 Instead of using “difficult patients” or “difficult relatives,” “difficult encounters” were used in the present study to avoid misinterpretation that patients and relatives were trying to be difficult, when in actual fact they were victims of difficult situations. 34 –36 Considering that most of the descriptions of care overload were caused by difficult encounters, hospitals need to incorporate the qualitative aspect of palliative care workload into the evaluation of staffing restriction. Contemporaneously, training to improve skills and knowledge in handling complex and difficult encounters needs to be provided.
In the interface of caring for others and caring for oneself, interpersonal stress caused by communication challenges, differences in opinion, and misperceptions–misconceptions were emphasized at the middle of the TC Model (Figure 1). Communication challenges reported in this study involved discussions of prognoses, dealing with strong emotions, interacting with noncommunicative patients, handling difficult questions, handling collusion, handling excessive questioning from relatives, dealing with large numbers of relatives and dealing with unconcerned colleagues. Although good communication is essential in the delivery of palliative care, many health care professionals who care for patients at their end of lives do not receive adequate preparation and training or emotional support to deal with the suffering and death of their terminally ill patients. 37 Furthermore, there were major regional differences in the attitudes and beliefs of physicians regarding communication at the end of life. 38 Therefore, assessment of communication deficiencies and provision of evidence-based communication training need to be implemented both individually and as a team to prepare palliative care providers to deal with various end-of-life communication challenges.
Reported differences in opinions included prognostic opinions such as the reversibility of a complication and the deferrability of a death; treatment opinions such as necessary versus unnecessary treatment; goals of care, such as life extension or quality of life improvement; and ethical opinions such as respecting patient autonomy versus family determination of treatment decisions or end-of-life discussion. Literature on end-of-life disagreements and conflicts in the palliative care context is scarce according to one systematic review. 39 A better understanding of end-of-life conflicts, combined with interpersonal respect, empathetic communication, and conflict-resolution skills such as negotiation and mediation, is vital in preventing or resolving the various end-of-life ethical dilemmas. 40 –42
Reported misperceptions–misconceptions comprised misperceptions–misconceptions about palliative care, such as the role of palliative care, the reason and timing of referrals, and the reason for stopping unnecessary treatments; about opioid and sedatives, such as phobias of using morphine and sedatives; and about cancer, death, and dying, such as believing that talking about cancer, death, and dying in front of patients could produce adverse problems. The lack of knowledge and misunderstandings about palliative care, morphine, sedation, cancer, death, and dying were identified as common barriers to provision of effective palliative care. 43 –47 To overcome these barriers, increasing public awareness and effecting organizational changes can be helpful. At an individual level, more awareness-focused communication can be practiced to address these misunderstandings.
The problems of lack of self-care were represented by issues of personal expectations, emotional involvement, and death and dying thoughts at the bottom of Figure 1. The stress from personal expectations occurred when palliative care providers experienced guilt for not doing enough for their patients and had a sense of failure and helplessness. There are very few studies in the palliative care literature that reported these feelings as opposed to guilt and helplessness of family caregivers. 48 –50 Nevertheless, the guilt and helplessness of not being able to help terminally ill patients recover or the inability to carry out the right course of action due to team or institutional obstacles have been described in previous research as medical failure and moral distress. 51 –53 Self-care strategies that target expectation mismatch and the resultant cognitive and emotional experience of guilt, failure, and helplessness can be developed and practiced to reduce stress from personal expectations.
The requirements to display or suppress emotions at work and be emotionally empathic were referred to as “emotion work” in the literature of workplace stress. 54 In this study, emotional involvement has the highest number of codes among all themes. The result of emotional vulnerability adds to the literature in illuminating the emotional “soft spot” of individual palliative care providers in dealing with different patients, relatives, and situations. Palliative care providers carry the risk of emotional exhaustion caused by intense or prolonged emotional reactivity in witnessing suffering, death, and dying. Self-compassion with its three components of self-kindness, a sense of common humanity, and mindfulness as opposed to self-judgment, isolation, and overidentification, can be applied to cope with the stress of emotional involvement. 55
Although repeated exposure to death and dying has been found to have a positive impact on experienced palliative care providers and leaders, a minority of codes from the study showed the opposite. 56 A total of 8 palliative care providers described their sadness, worries, and fears when they reflected on their own or relatives’ deaths. Even though they did not appear distressed when they talked about it, death anxiety of palliative care providers warrants specific attention to prevent secondary traumatization from happening.
In contrast to various occupational stress models in the literature, our TC Model emphasizes the problem of caring for others and the lack of caring for oneself. In the Role Stress Model, the concepts of role stressors, such as role overload, role ambiguity, and role conflict, are presented. 57 In the Person–Environment Fit Model, the emphasis is on the mismatch between the worker and the work environment. 58 In the Job Demands–Control Model, the emphasis is on strain caused by high job demands and low job control. 59 In the Effort–Reward Imbalance Model, the imbalance between effort and reward is described. 60 Although the 4 existing models of occupational stress described stress as a result of the person–work transaction, the attention was focused predominantly on work factors, namely work role, work environment, work demand, and work reward. In our model, other than work factors such as organizational challenges and work overload; the contribution of interpersonal factors such as communication challenges, differences in opinion and misperceptions–misconceptions; and the contribution of personal factors such as personal expectations, emotional involvement, and death and dying thoughts, are given equal significance.
Problem-focused coping and emotion-focused coping that were described in the Two-Function Model of Coping intersect with our model in a unique way. 61 The role of problem-focused coping increases from a bottom-up manner, whereas the role of emotion-focused coping increases from a top-down manner (Figure 1). Therefore, a combination of both approaches is required in dealing with stress in palliative care, but in different proportions as determined by the position in Figure 1. Additionally, dealing with interpersonal issues shown in the middle of Figure 1 corresponds to a third coping method called relationship-focused coping described in social psychology. While problem-focused coping emphasizes improving the problems of caring for others and emotion-focused coping emphasizes caring of one’s own emotions, relationship-focused coping refers to cognitive and behavioral efforts to manage and sustain relationship during stressful times. 62
The inseparable relationship between the stress of caring for others and the stress of lack of caring for oneself was highlighted in the study. Therefore, self-care strategies should be incorporated into health care practices in a more comprehensive manner. The TC Model can serve as a guide in the understanding of stress in palliative care providers and the development of stress management strategies, taking into account work factors (organizational challenges and care overload), interpersonal factors (communication challenges, differences in opinion and misperceptions–misconceptions), and personal factors (personal expectations, emotional involvement, and death and dying thoughts).
The study has several limitations. Most of the participants were female (90%). Therefore, it is difficult to generalize the findings to both genders. Community palliative care providers and palliative care providers from other hospitals were not included in the study. Findings were also limited by the scope of the questions asked and the length of the interviews. The average interview length was only 13 minutes because of the limited available time of participants during working hours. Transcriptions and translations of the 2 Malay interviews were limited by language barriers in which subtle descriptions of stress experiences could be missed. Intrinsic difficulty in differentiating stress from stressors posed another limitation. Additionally, the cultural aspects of the findings such as ethnicity and religion were not specifically addressed in this article. Future studies that focus on the sociocultural and religious aspects of stress are needed to understand the cultural differences between the various ethnic groups in Malaysia.
In conclusion, occupational stress in palliative care providers can be defined as a combination of problems of caring for others and a lack of caring for oneself. In the management of stress in palliative care providers, a triple approach that targets work factors (organizational challenges and care overload), interpersonal factors (communication challenges, differences in opinion, and misperceptions–misconceptions), and personal factors (personal expectations, emotional involvement, and death and dying thoughts) can be applied.
Footnotes
Acknowledgment
We would like to express our heartfelt gratitude to all nurses and doctors who participated in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: High Impact Research Grant (Cycle 3), University of Malaya, Ministry of Higher Education, Malaysia.