
Abstract
Objective:
Physicians' religiosity affects their approach to end-of-life care (EOLC) beliefs. Studies exist about end-of-life care beliefs among physicians of various religions. However, data on Muslim physicians are lacking. This study explores the beliefs centering on aspects of end-of-life care among Muslim physicians in the US and other countries.
Design:
A 25 item, online survey was created and distributed via Survey Monkey®. The survey was targeted toward Muslim physicians in the US and other countries.
Results:
A total 461 Muslim physicians responded to our survey. The primary end point was if the Muslim physicians thought that making a patient DO NOT RESUSCITATE (DNR) is allowed in Islam?. Nearly 66.8 % of the respondents replied yes as compared to 7.38 % of the respondents who said no. Country of origin, country of practice, and if physicians had talked about comfort care in the past had the most impact on the yes vs. no response (p=0.0399, p=0.0092 and 0.0023 respectively).
Conclusion:
Muslim physicians' beliefs on EOLC issues are affected more by the area of practice, country of origin and previous experience in talking about comfort care than the religious beliefs.
Introduction
End-of-life care (EOLC) issues represent unique and challenging situations. There is extensive literature on how patients’ religious and spiritual attributes influence their health. 1 Available data suggest that country of origin and religious and cultural background influence physicians’ knowledge, attitudes, and practice of medicine, including issues related to EOLC as well. 2 –4 Islam represents the second largest religion. Studies including small numbers of Muslim physicians from the United States suggest that the physicians from this religious group have higher odds of objecting to the concepts of physician-assisted suicide, terminal sedation, withdrawal from life support, 5 and withholding or withdrawing from artificial nutrition. 6 There is a gap of knowledge on EOLC beliefs with respect to do not resuscitate (DNR) orders and advance directives in this group of physicians. Even the studies examining the issues regarding the withdrawal of care included relatively smaller numbers of Muslim physicians who were practicing in the United States. 5 We therefore conducted a survey to study the association between acceptability of DNR among Muslim physicians as a primary outcome. As a secondary analysis, we evaluated various factors pertaining to the withdrawal of care to elucidate influences on DNR attitudes.
Methods
An online survey containing 25 questions was distributed through “Survey Monkey,” an online survey response collecting software. The survey was targeted toward Muslim physicians practicing in the United States, Pakistan, India, Bangladesh, United Kingdom, and Kingdom of Saudi Arabia. Survey targeting was performed by sending an introductory e-mail explaining the purpose of the study and requesting participation through the Islamic Medical Association of North America central server, an association of 2445 Muslim doctors practicing in the United States. A similar e-mail was also sent to 2 Internet-based medical school blogs, Army medical college, Pakistan and Allama Iqbal Medical College, Pakistan. The number of physicians in these blogs is unknown. Approximately 100 Muslim physicians practicing in other countries were also approached on the basis of personal acquaintance by the authors. These various sources of Muslim physicians were targeted in order to obtain survey responses from a demographically diverse sample of Muslim physicians.
The e-mail also contained a Uniform Resource Locator that directed the physicians to an anonymous online survey. The initial e-mail was sent in November 2010 and a second request was sent 3 weeks after the initial e-mail to enhance the response rate. No incentives were offered for the study. If the physician proceeded to the survey questionnaire, consent for participation was assumed. Institutional review board approval was obtained from the University of Illinois, Urbana-Champaign, Illinois, and Carle Foundation Hospital, Urbana, Illinois.
Demographics are expressed as percentages. Relationships between the primary outcome variable (response to the question “Do you think that making a patient DO NOT RESUSCITATE (DNR) is allowed in Islam?) and each primary exposure variable were examined by presenting the percentages and frequency of responses of each type for each value of primary exposure variable in 2-way tables. Chi-square tests and Fisher exact tests were used to test the association between 2 variables. The primary exposure variables included country of graduation, country of origin, country of practice, level of training, and practice specialty. Multiple logistic regression analysis was used to identify variables most impacting the primary outcome. Results are reported as odds ratios that were calculated by keeping only the significant variables in the model. Descriptive analysis is reported for questions regarding withdrawal of care. A P value <.05 was considered statistically significant for all tests. The statistical analysis was conducted using the FREQ procedure and LOGISTIC procedure from SAS version 9.2 (SAS Institute Inc, Cary, North Carolina).
Results
A total of 461 physicians completed the online survey. In all, 374 physicians responded to the first e-mail and an additional 87 Muslim physicians responded to the reminder e-mail. Table 1 presents the baseline characteristics of the respondents. Respondents with missing information are categorized as others. Table 2 presents the knowledge and practices about EOLC issues. Not mentioned in this table, 37.4% physicians wrote a DNR order within the last week, 24.69% in the last month, and 23.05% within the last year; 14.8% wrote such an order more than a year ago. In all, 218 respondents did not answer this question. The reason so many respondents did not answer this question is unclear and not discernible from the study. However, it may be plausible that these physicians had not written DNR order in their lifetime; additional study is required to clarify this issue. Table 3 depicts the responses to the questions about knowledge and practices related to EOLC issues. Table 4 shows the distribution of the responses to the survey question “Do you think that making a patient DNR (DO NOT RESISCITATE) is allowed in Islam?” for each value of the primary exposure variables. Higher percentage of physicians graduating from the United States, United Kingdom, and other countries responded “yes” to the question than those graduating from Muslim countries (93.18%, 83.33%, and 82.5% respectively). This difference was statistically significant (P ≤ .0001). None of those graduating from the United States responded “no” (0%) to the question. Those graduating from Muslim Countries had the highest percentage to have never thought about the question (27.57%). These differences in percentages are statistically significant (P < .0001).
Demographics and Characteristics of the Survey Respondents.
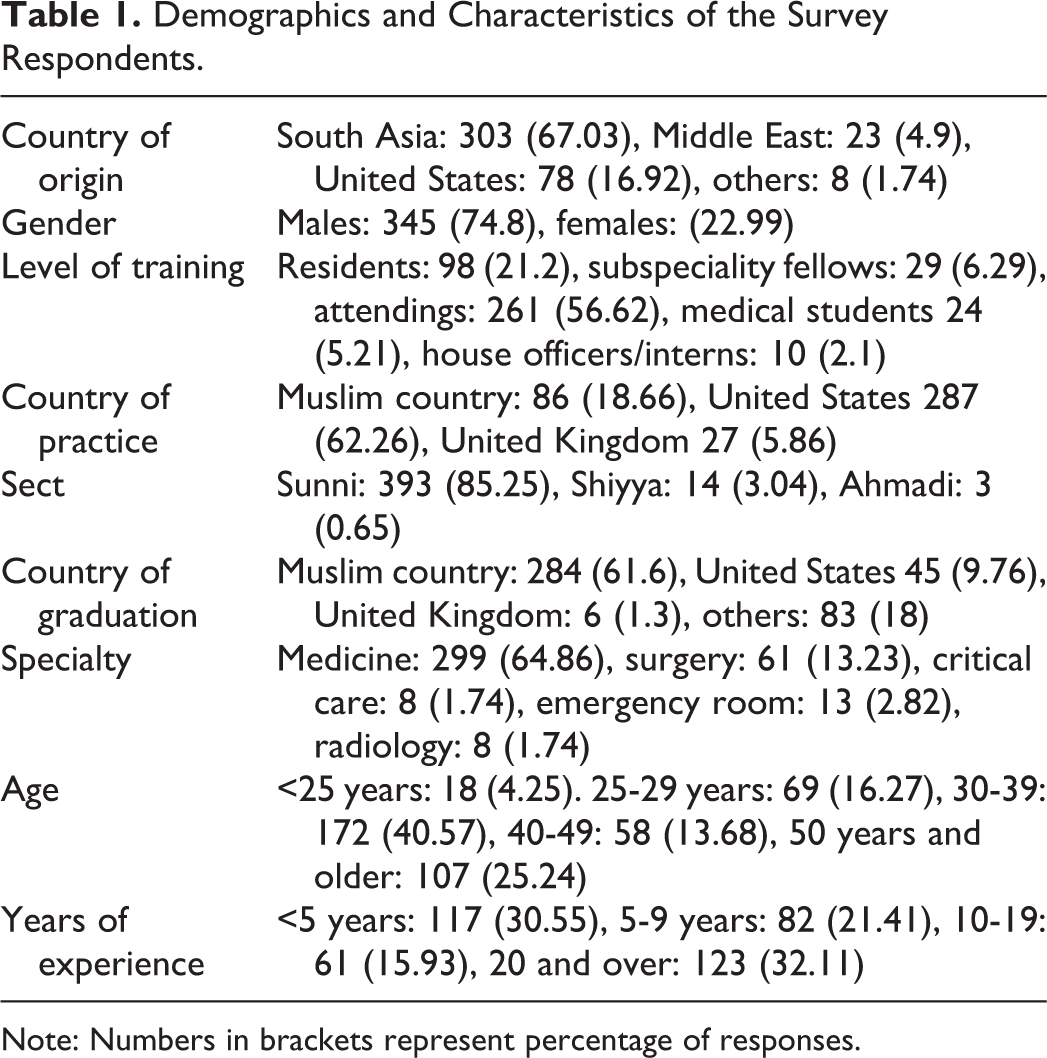
Note: Numbers in brackets represent percentage of responses.
Physicians’ Knowledge and Practices Related to End-of-Life Care Issues.
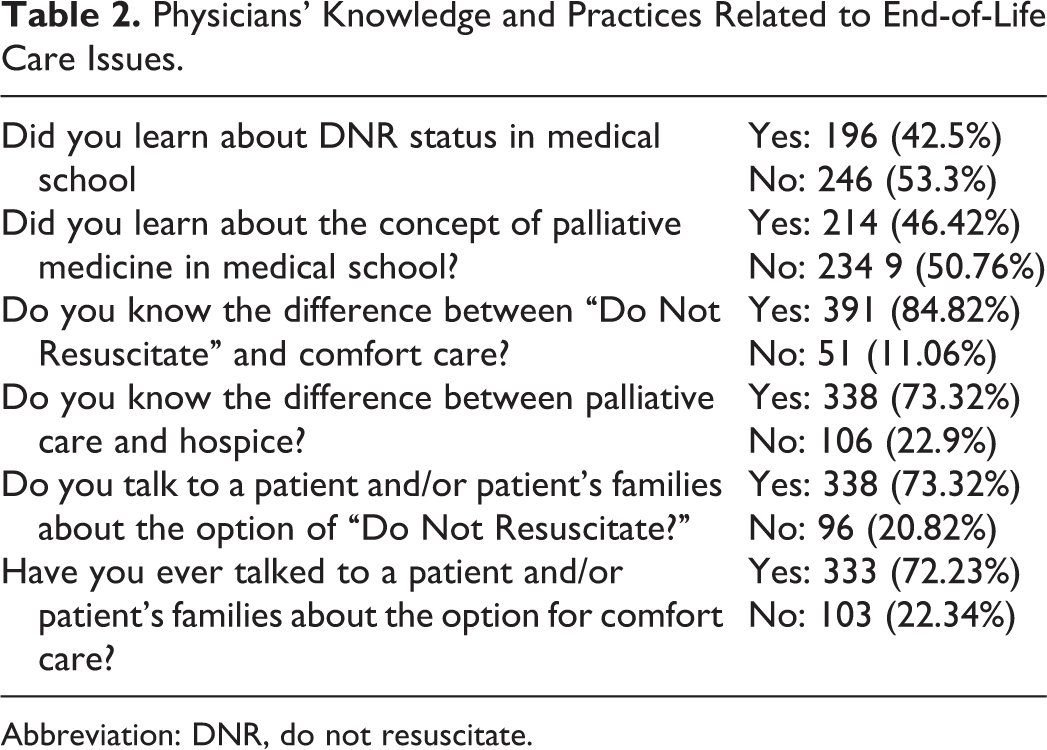
Abbreviation: DNR, do not resuscitate.
Beliefs on End-of-Life Issues.a
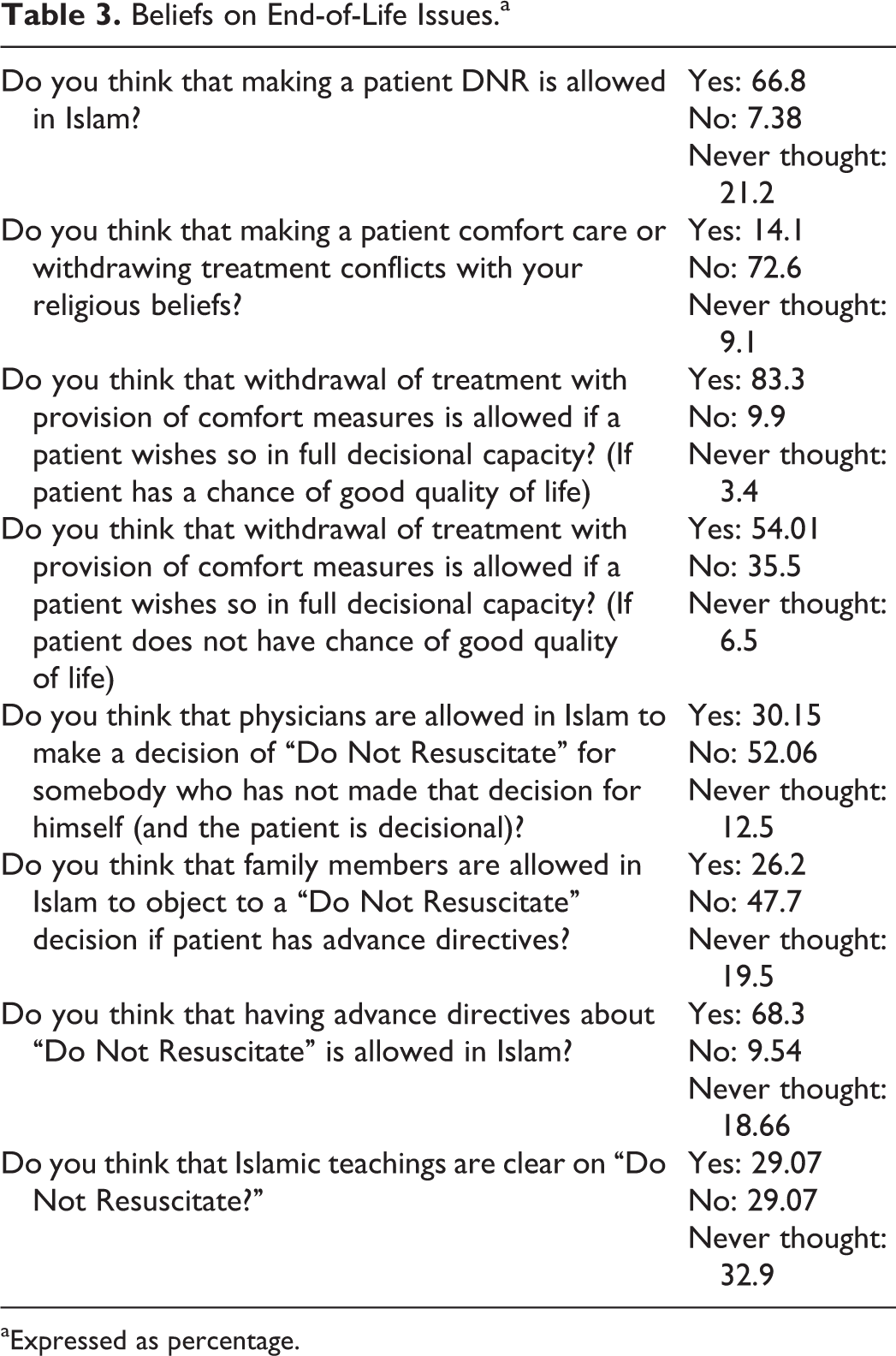
aExpressed as percentage.
Results According to Various Exposure Variables.
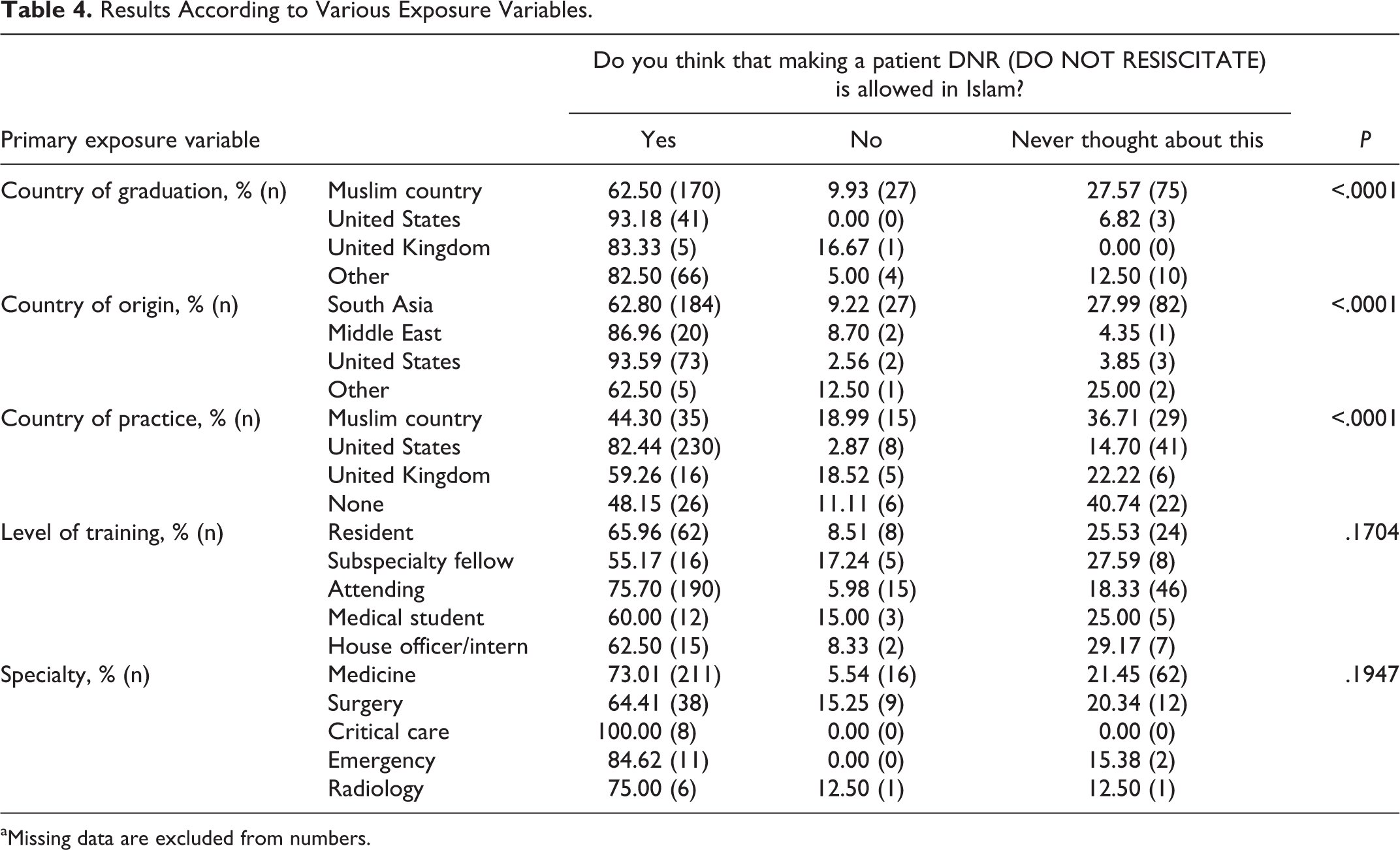
aMissing data are excluded from numbers.
Physicians born in the United States and Middle East were more likely to respond “yes” (93.59% and 86.96%) and less likely to report never having thought about the question (3.85% and 4.35%), compared to those born in South Asia and other countries. US-born Muslim physicians were least likely to respond “no” (2.56%). These differences in percentages are statistically significant (P < .0001).
Discussion
Our findings show that country of origin, country of practice, and whether the physician had talked about comfort care with families in the past were significant determinants of belief in the validity and acceptability of DNR order (see Table 5). Other variables such as specialty, years since graduation, and sect had no effect. To the best of our knowledge, this is the first study assessing the beliefs of Muslim physicians in DNR orders and the association between various exposure variables on DNR order acceptability.
Significant Associations With Belief in Validity of DNR Order in Islam.
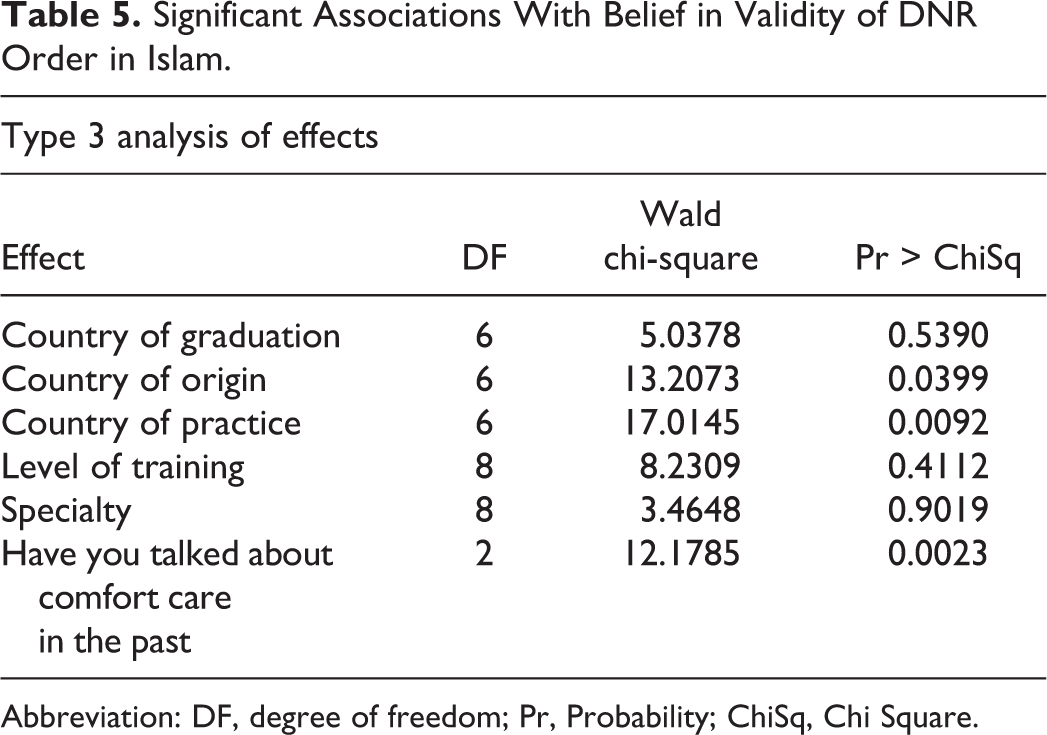
Abbreviation: DF, degree of freedom; Pr, Probability; ChiSq, Chi Square.
Suicide and euthanasia are forbidden in Islam. In Islam, the primary source of guidance is Quran (the holy book). If guidance is not available from Quran, Hadith is the next source of information. Hadith is what Prophet Muhammad (peace be upon him) had said or did in his life and is preserved in religious scriptures. If enough evidence is not available from Quran or Hadith, Islamic scholars get together and come up with a commandment in the light of clues from Quran and Hadith.
The Islamic perspective regarding DNR decisions is a moving target. In Hadith, Prophet Muhammad (peace be upon him) said that “None of you should wish for death because of a calamity befalling him but if he has to wish for death, he should say “O Allah! Keep me alive as long as life is better for me, and let me die if death is better for me (Sahih Al-Bukhari.Hadith no 575).” Dr Saiyad interpreted this as the duty of Muslim to seek medical treatment to the extent that knowledgeable experts expect therapy to be successful, regard harm from that mode of therapy as unlikely, and the mode of therapy is permissible.
7
In one of the published reviews in this issue, decision of medical futility and decision of DNR were left up to the treating physicians rather than the patient and famlies
5
This issue was also addressed by Presidency of the Administration of Islamic Research and Ifta, Riyadh, Kingdom of Saudi Arabia, in their Fatwa No. 12086 issued on 30.6.1409(Hijra), 1988 (
Because the issue of DNR is embedded within the scope of palliative medicine education, we also asked about exposure to palliative medicine teaching in the survey. Nearly half of our respondents did not learn about palliative medicine in medical school. Almost 83% of the respondents overall did not feel comfortable withdrawing care if the patient had a chance of a good quality of life. The perception of good quality of life was left up to the respondent. This issue may need to be considered when Muslim physicians are dealing with terminally ill patients as the ethics of withdrawal differ among this group of physicians. According to the aforementioned Fatwa, a DNR order or withdrawal of care is a physician-based decision that does not need involvement of families. However, more than half of the respondents did not agree with this and nearly one-third felt that families could over rule the patient’s decisions despite his wishes. About 29% of the surveyed physicians felt that the religious teachings are not clear. The concept of advance directives needs further elaboration in Islamic literature as there is no formal Fatwa on this to our knowledge.
Our study has several limitations. Our survey study did not undergo reliability or validity testing. Accurate response rate cannot be determined in our study due to unknown number of physicians in 2 medical school blogs. In addition, bias may have affected the responses as survey completion was voluntary. The strength of the study is that it addresses the current gap in knowledge regarding Muslim physicians’ attitudes and beliefs toward DNR orders and illuminates the importance of country of training and practice on beliefs.
In summary, religious beliefs can play an important role in making judgments. However, our study results are in concordance with some of the previously published data that the area of practice influences EOLC decision making more than the religious beliefs. 10 Further study is needed to explore how religious beliefs underscore and impact EOLC delivery.
Footnotes
Authors’ Note
Both Drs Nadia Kousar and Sohaib Aleem are second authors.
Acknowledgments
The authors also thank Islamic Medical Association of North America (IMANA) for their support with the survey distribution to their members. The authors thank Carle Foundation hospital for providing statistical support for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The authors received funding from Carle Foundation Hospital for statistical analysis.