
Abstract
There are several kinesthetic parameters that can be used to measure fatigue including strength, endurance, sense of effort, perception of force exerted, and tapping speed. We developed a protocol and tested the feasibility of correlating subjective fatigue with kinesthetic parameters in a small group of patients with cancer having fatigue and in controls. Accrual was limiting. We discuss the limitations and potential modifications in the procedure, which may allow improved accrual and the rationale behind performing such a study.
Introduction
Cancer-related fatigue (CRF) is a common symptom experienced by patients and survivors and has a profound impact on quality of life. 1 –3 Cancer-related fatigue results in impaired physical, psychosocial, and economic status for both patients with cancer and caregivers. 2 Cancer-related fatigue differs from normal fatigue in that it occurs without exertion. Although fatigue is a symptom that is commonly experienced in the noncancer population, CRF is more severe, chronic, pervasive, unrelieved by rest, unrelated to activity, and impinges on activities of daily living. 2 –5 The exact mechanisms of CRF are not well understood and may be multifactorial. 6 It is not known whether CRF is central or peripheral. Pharmacological interventions may improve CRF severity. 7 Chemotherapy, opioids, and narcotics used to treat neoplasms promote cachexic and worsen fatigue. Cachexia is associated with decrease in muscle mass (sarcopenia) and may result in functional impairment of somatic muscles. 8
The prevalence of CRF varies depending on the criteria used as case definition. 1 The International Classification of Diseases, Tenth Revision (ICD-10) criterion requires “significant fatigue, diminished energy, increase need to rest, disproportionate to any activity level” 1(p3386) present every day or nearly every day for 2 weeks in the past month. 8 Cancer fatigue excludes comorbid psychiatric depression.
Fatigue may arise from peripheral (originates from muscle) or central (from central nervous system) mechanisms. 9 Associated symptoms with fatigue involve peripheral (weakness) and central (reduced concentration) descriptors within the ICD-10 criterion. Physiologic fatigue can be loss of force (strength), activation failure of muscle or capacity to exercise (endurance), increased sense of effort, altered perception of force, or loss of power (velocity plus strength). 9 We have recently demonstrated impaired activation of muscle as measured by increased twitch force by motor nerve stimulation at the time of task failure in individuals having cancer fatigue. 10 We have also reported differences in electroencephalography frequency power dynamics during a sustained elbow flexion, which are distinct from normal nonfatigued individuals. 11,12 Both findings suggest to us that a significant component of CRF is central in origin.
Most studies of CRF are prevalence or prospective observational studies involving cohorts of individuals with various stages of cancer. It has been assumed in these studies that associated factors are causally responsible for CRF. Many associative factors involve individual demographics, psychological symptoms, physical symptoms, and laboratory studies. 5 No single factor correlates well with fatigue severity, however, empiric treatment based on associative factors has had very little impact on fatigue. 6,7
Fatigue in the Control Population.
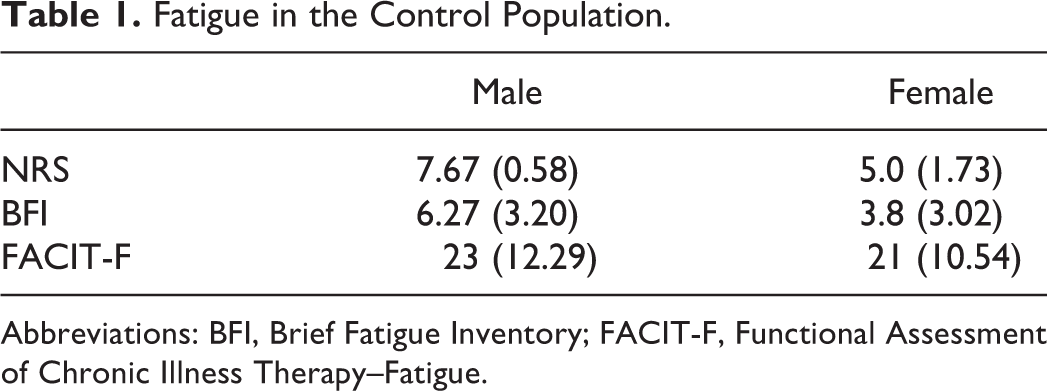
Abbreviations: BFI, Brief Fatigue Inventory; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue.
Fatigue in the Sample With Cancer.
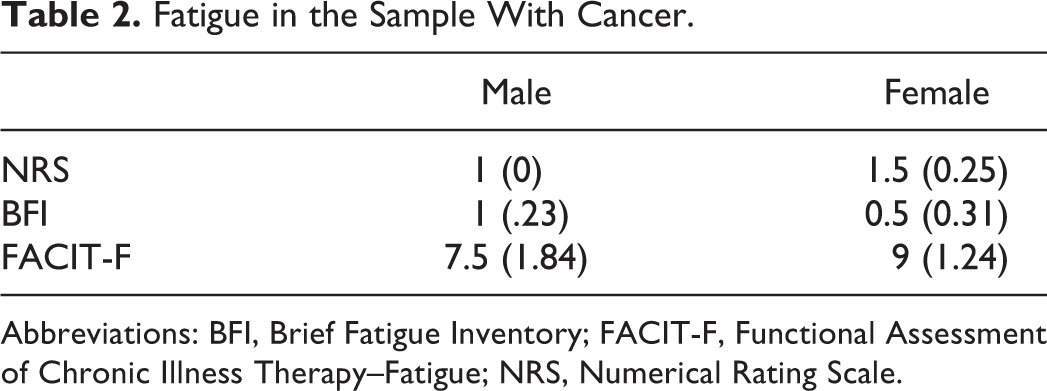
Abbreviations: BFI, Brief Fatigue Inventory; FACIT-F, Functional Assessment of Chronic Illness Therapy–Fatigue; NRS, Numerical Rating Scale.
Two kinesthetic parameters that can easily be measured in the clinic and hospital are perception of force and perception of effort. Perception of force arises from corollary feedback to sensory and motor cortex from motor commands required to maintain the force of a sustained contraction, hence largely central in origin. 13 –15 The objective measurement of force perception involves matching force exerted by one muscle group (reference) with contraction of the corresponding (mirror image) muscle group on the contralateral side of the body (matching) for the purpose of matching the reference arm force. 16 Fatigue may lead to an overperception of force exerted resulting in an overmatching of force by the matching (mirror image) limb. 14,17 Manual muscle testing (MMT) and finger tapping testing (FTT) provide kinesthetic variables of physical exertion. Fatigue in multiple sclerosis is associated with slow tapping finger speed and power. 18 Motor speed is indicative of physical function. The FTT is not an overly burdensome test and is able to be performed within the cancer population. Force exerted by the hand can be measured by using a manual muscle dynamometer. Muscle dynamometers have been proven valid through test–retest and reflect the force of all gripping muscles within the hand. 2 Obtaining force output using manual muscle dynamometry in patients with cancer is advantageous due to the accurate kilogram recording and adjustable gripping positions. Interventions designed to target fatigue as a specific symptom of cancer and cancer treatment/recovery would be of significant value to patients and caregivers. 4 Objectively measuring CRF through performance measures may help in interventional trial outcomes.
Both FTT and MMT provide potential objective measures of fatigue. Subjective fatigue encompasses the emotional, psychological, and overall sense of well-being. Sensory bias influences force output during isometric muscle contractions and perception. 15 Previous studies indicate that with prolonged muscle activation and usage, the perception of effort is increased and misperception of force is greater at exhaustion or task failure. 16
Within the cancer and palliative care populations, the Brief Fatigue Inventory (BFI) and the Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) are valid questionnaires that assess subjective fatigue. 19,20 For investigation, we piloted a study using MMT, FTT, and the BFI in patients with cancer experiencing fatigue. We compared this population to normal controls in this pilot study as a step toward feasibly measuring the correlation between fatigue and the sense of effort, force output, perception of force, strength, and finger tapping speed.
Objectives
The objectives of this study are to develop clinically based objective outcome measures for subjective CRF.
Primary Objective
The primary objective of the study was to compare the perception of force during 30% of the maximum sustained handgrip between individuals with CRF (BFI ≥ 4) and normal controls (BFI < 4) and also to compare results between these 2 study populations to determine the ratio of change in perceived force to endurance time.
Secondary Objective
The secondary objective was to compare strength, endurance time (duration of sustained handgrip contraction until failure to maintain a 30% maximum handgrip), finger clicking speed, perception of force during sustained handgrip task, and effort between individuals with CRF and normal individuals.
Tertiary Objective
The tertiary objective included comparing the results obtained from the BFI and the FACIT-F as a means of determining proper questionnaire designation for future studies.
Methods
The BFI and FACIT-F questionnaires were verbally administered in person by research staff to inpatient, palliative medicine patients who were physically able to hold the clickers and manual muscle dynamometers, did not have an active infection, were not delirious, 18 years of age or older, were able to sit upright, and provided written consent. Upon completion of the BFI and FACIT-F, participants were asked to sit in an upright position with both arms flexed at approximately 90 degrees relative to seated midline. Once participants were properly positioned, fatigue tests were administered. Clicking speed was obtained by using grocery counting clickers and a stop watch. Total clicks achieved per 30-second time interval were collected on both the dominant and nondominant hand. Upon completion of the clicking, patients were asked to use the Borg scale (0-10) to rate their perception of difficulty for this task. Muscle dynamometers were then used to obtain the maximum exertion on the dominant hand by averaging a total of 3 grip trials. Once the average maximum volumetric contraction (MVC) was obtained, 30% of the MVC was calculated and used as the matching value for the sustained contraction in order to accurately determine endurance. Once the endurance time was recorded, participants were then asked to use 1 muscle dynamometer in each hand to bilaterally match forces. The dominant hand sustained contraction with the dynamometer facing the participant. The nondominant hand was to match the sustained contraction in time increments of 15 seconds up to 75 seconds (or until failure). At the end of each task, patients rated their perception of difficulty/exertion using the Borg scale. Once MMT was completed, participants repeated the clicking test and rated it in accordance with the Borg scale.
The results from the sample population were compared to the results of a controlled population, which consisted of 2 male and 2 female, noncancer, age-matched, participants.
Results
Of the 23 screened patients, 17 were eligible, 11 provided written consent, 7 completed the study, and 1 patient had incomplete records. Of the 6 completed patients, 3 were females and 3 males. Because of the small sample size, mean values were obtained rather than using descriptive analysis to provide a more generalized finding. The mean MVC in the study population was 43.0 kg, with a standard deviation (SD) of 22.8. The FACT-F questionnaire mean score was 22 (SD 10.3). The mean BFI score was 5.1 (SD 3.2). The mean endurance time using the manual muscle dynamometers in determining grip strength over time was 23.9 seconds (SD 14.1). The study is closed to accrual due to difficulty of performing tasks by patients with advanced cancer in a palliative care setting. The control group comprised 2 males and 2 females who were within or less than 4 years of age difference compared to the patients with cancer. Due to the small size of the control group, male and female averages were combined. The mean age of the control group was 62. The mean NRS score was 1.25 (SD 0.25). The mean BFI score was .75 (SD 0.5). The mean FACIT F is 16.5 (SD 2.5). The mean endurance time before muscle failure within the normal control group was 25.5 seconds. The time interval of 30 to 45 seconds is the most reflective of true force perception in both populations. A noticeable trend in Borg scales was that effort plateaued rather than increased with task. Women tended to have greater misperception than men had. On average, women also rated their fatigue worse than men did.
Discussion
Although inconclusive results were obtained, this pilot study generated information that will inform future studies in which we hope to have patients enroll in earlier stages of cancer. We believe that the low enrollment was multifactorial. First and foremost, the inclusion and exclusion criteria for participation are fairly rigorous for the inpatient palliative medicine population. A considerable number of inpatient palliative medicine patients have active infections and are on opioids or other sedative pharmacological interventions. We had to modify the study to remove the prohibition to opioid use. Opioids have been associated with underperception of exertion. 21 The vast majority of patients were too ill to effectively participate, had brain and/or bone metastases, or delirium. Another common issue our research team experienced was that once the patients showed improvement, they were discharged before completing the study. Many patients expressed that the manual muscle tests and clicking tests were simply too burdensome and that they were too fatigued to participate.
Although we experienced difficulty in accrual, the patients who did successfully complete testing provided valuable data that can be used in future studies. As hypothesized, the population with cancer did experience slower clicking speeds, lower force output, and more perception of fatigue and overperception of force exerted, though numbers are too small to consider statistically valid. Females had higher rates of overperception of force and rated their fatigue severity as being worse than males had. There was a significant correlation between the misperception of force, fatigue severity, and Borg ratings of effort. The population with cancer perceived a higher force output than that of noncancer population.
The etiology of fatigue is not known. Cancer-related fatigue may vary depending on primary cancer site, metastatic sites, and cancer treatment. Supplemental studies focused on cancer type versus fatigue may be useful to gaining a further understanding of the CRF population. It is important to separate gender when testing muscle function and fatigue in order to compare profiles. A more in-depth comparison could be performed by cancer types during treatment, prior to illness and/or hospitalization.
Further studies using this method in cancer could be successful if outpatients and healthier individuals were included. It is unlikely that completion rates would significantly improve if inclusion was limited to inpatient palliative medicine patients. Palliative medicine patients are generally very ill, fatigued, and many may be too frail to effectively participate. For matching force using dynamometry, we would recommend decreasing time intervals from 15 to 10 seconds, which would allow matching hand muscles to relax yet decrease the amount of time patient sustains a 30% MVC on opposing hand. The procedures of this study should be further modified in order to determine clinical correlations and to explore kinesthetic mechanisms involved in CRF. By gaining an understanding of the relationship between fatigue and force perception, further studies to identify central mechanisms of fatigue could be conducted. This also would provide objective correlates to subjective fatigue.
Repeat measures of force perception during interventions could potentially provide objective measures of fatigue that would complement subjective fatigue measurements. The muscle dynamometer is portable and feasible on an inpatient palliative medicine unit.
Conclusion
Force perception and tapping speed may complement handgrip strength and sustained contraction as a measure of CRF. Further investigation is required to confirm our findings in order to gain a deeper understanding of force perception in patients with CRF. Modification of the procedure will be necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.