
Abstract
Multiple factors influence end-of-life (EOL) care discussions that occur in health care systems, within organizations, among individuals working within these systems and in patients and family/friend support networks. This study examined barriers to EOL care discussions as experienced by health care providers working in a public safety-net health care system where the majority of their patients were low-income and immigrant Latinos seeking medical treatment. Qualitative data were collected in South Central Los Angeles through semistructured interviews with 46 health care providers from different disciplines in medicine, nursing, social work, and chaplaincy. The themes indicated communication barriers in the public sector health care setting and sociocultural patient- and family-level factors. All providers made valuable contributions to clarify the complexity of the problems. Universal strategies are needed to improve communication.
Keywords
Challenges in End-of-Life Care Communication
Gaps in end-of-life (EOL) care communication affect mismanagement of patients’ symptoms, influence over- or underuse of medical treatment, and increase psychological distress for patients. End-of-life communication involves providers, patients, and family members entering into meaningful discussions about poor prognosis, breaking bad news when recovery is not possible, exploring patients’ values and preferences for EOL medical care, and making advanced preparations for death and dying often documenting advance directives. Initiating EOL conversations early helps to lower distress and to improve quality of life; 1 it also helps to direct patients to EOL resources such as hospice and palliative care. 2 Barriers that limit the timing and quality of EOL discussions affect terminally ill individuals and their family members. This is especially important for low-income and underserved populations 3 –5 because potentially lacking health insurance, they may utilize urban safety-net medical settings for their care. 6 Health care providers often feel they lack the time to engage patients in EOL discussions, while patients avoid the topics of illness and death. 7 Other factors involve individuals who hold beliefs that patients will lose hope or become emotionally overwhelmed by talking about dying. 8,9
It is important to note that the “safety-net” is a term used to describe hospitals or health care systems that provide care to the poor and underserved. 6 In California, the health care safety-net serves many public health care systems that are members of the California Association of Public Hospitals and Health Systems consisting of county hospitals, academic medical centers, and their affiliated public clinics. These systems form the core of California’s public health care safety-net, providing cost-effective, high–quality, and culturally appropriate health care services for low-income and uninsured populations. 10
End-of-Life Communication With Vulnerable Populations
Clearly, some patients and providers have more difficulty talking about death and dying than others. 8,9 For example, immigrant and underserved populations experience low-health literacy and language barriers that complicate EOL discussions. Patients with limited resources often lack adequate preventive health care, health insurance, and financial resources to pay for medical treatment, and they are more likely to use the emergency department (ED) for their care. 11 This makes them especially vulnerable, increasing the probability of poor health outcomes. 12,13 In one study, with mostly Latino patients utilizing a public urban hospital, patients had prior difficulty accessing medical care, along with financial concerns, and presented to the ED because their symptoms were out of control. 14 They delayed seeking health care until they were in extreme pain. End-of-life care communication was particularly poor and complicated by communication and cultural differences between patients and providers. Such gaps in EOL care communication obstruct the connection of patients to EOL care resources such as hospice and palliative care. 8 However, very little research has focused on providers’ experiences with barriers to EOL communication that affect vulnerable populations, especially for those utilizing public safety-net health care systems at the end of life.
Providers working in public safety-net health care systems face special challenges when discussing EOL care with their patients. 15,16 Health care disparities and limited access to care create distrust and complicate discussion with providers about the possibility of dying. These challenges are made more complex for providers because their patients, coming from low socioeconomic backgrounds, are likely to have experienced difficulty seeking health care services prior to entering the medical system. 3 Disadvantaged and uninsured patients lacking preventive care tend to seek medical attention later in the course of the disease, making them more severely ill when entering the medial system. 17 –19 Patients who lack early intervention and detection of health problems risk receiving poor health care 17 and experience poor clinical outcomes and premature death. 20 Rather than seeking medical attention for curative treatment, socioeconomically disadvantaged patients may be closer to death when they enter the medical system. Under such circumstances, introducing the topic of EOL care, by engaging in advance care planning, discussing limiting medical treatment to focus on hospice and palliative care, and planning for place of death become extremely complex. 21
End-of-Life Care in Public Safety-Net Health Care Systems
Previous research explored the advocacy role of health care providers with low-income Latinos in a public sector health care system. 16 Providers described how advocacy was triggered when misunderstanding and lack of communication existed in managing EOL care for vulnerable Latinos. Competing agendas between patients’ needs, available resources within the system, and providers’ actions influenced EOL care outcomes. Multiple factors influence EOL care; these barriers occur in health care within organizational systems of care, among individuals working within these systems and among patients and their family/friend support networks. As these issues affect gaps in communication, it is important to understand providers’ experiences in managing EOL care communication with terminally ill patients utilizing a safety-net health care system as they are especially vulnerable without proper care.
Research Objectives
The objective of this study was to evaluate barriers in EOL care discussions as experienced by health care providers working in a public safety-net health care sector where the majority of their patients were low-income and immigrant Latinos seeking medical treatment. This study builds upon prior research 16,22 and explores concepts pertaining to (1) critical components in beginning EOL discussions in a public safety-net health care sector, (2) barriers to EOL care transitions that impact Latinos with end-stage diseases, and (3) factors that make EOL discussions more difficult, considering communication involving patients, family members, other providers, and the medical system.
Methods
This study was part of a larger qualitative, mixed-methods study on improving EOL communication with low-income Latino patients with advanced cancer who used a public safety-net health care system in Los Angeles, California, for their care. The research was conducted in a South Central Los Angeles public medical setting with providers of inpatient and outpatient services. The location was important because California has one of the largest Latino/Hispanic populations in the United States, with many living below the federal poverty level and relying on a publicly funded safety-net system for their health care. 23 More than 4.5 million Latinos live in Los Angeles County alone, representing almost half (47.7%) of the County’s population. 24 Purposive sampling guided recruitment to enroll a diverse sample of providers; this was conducted in outpatient oncology clinics and open areas where providers gathered such as the cafeteria as well as through snowball sampling methods. 22 In this sample, the researcher collected qualitative data from 46 providers using in-depth, semistructured interviews that facilitated understanding of the explored barriers that influence EOL communication with terminally ill Latinos in the public health care system. Criterion sampling was used to recruit different types of providers across disciplines and experience levels, all of whom engaged in direct practice with patients. Eligibility criteria stratified participants by provider type across disciplines in medicine, nursing, social work, and chaplaincy as well as by provider roles in different departments and across responsibilities. All providers had some experience or expertise working with Latino patients with end-stage cancer in the hospital, primary care, emergency care, hematology, oncology, radiation oncology, pulmonology, endocrinology, and palliative care.
Data Collection and Analysis
Following internal review board approval from the University of Southern California, we collected audiorecorded in-depth interviews with providers (n = 46). Guiding questions were designed to elicit providers’ experiences of issues that raise concern or create problems engaging in conversations with their terminally ill patients (mostly low-income Latinos) from various viewpoints (patients, caregivers, other providers, and the medical system). Questions explored (1) barriers in the public-sector medical setting, (2) issues related to EOL care discussions with Latinos, (3) sociocultural factors and vulnerabilities, (4) provider roles, and (5) other factors. In-depth interviews were conducted by one author (FNH). Each provider received a US$20 gift card for his or her participation.
All audiorecorded interviews were conducted in English and transcribed verbatim into a Word document; the data were then entered into Atlas.ti, an analytical software package. 25 Transcripts of providers’ experiences were analyzed using a constant comparative method to explore providers’ perspectives on the barriers that exist in engaging patients in EOL care discussions. 26,27 Analysis involved an iterative process of repeated review of the data components during data collection, which also occurred over the course of the research project. Analysis was structured first through open coding using concepts that stemmed from providers’ words, statements, and phrases. Then an inductive approach to the data guided the analysis to create categories, subcategories, and themes from the codes. Analysis proceeded to redefine codes and concepts throughout the analytical process that included writing memos and developing outlines/diagrams to identify a typology of barriers. Providers’ interviews were then reexamined and coded for key words and phrases that reflected barriers to EOL discussions considering the context of providing care in a public health care setting. This helped to maintain a focus on providers’ experiences with the gaps in care. In order to ensure rigorous data analysis, two of the authors reviewed transcripts independently and then collaborated for additional review to ensure trustworthiness of the findings. 28 Additionally, coding consensus was reached through multiple discussions of coding discrepancies. 29 This coding strategy was also reviewed by two health care providers other than those interviewed for this study, which consisted of the final coding strategy and a summary of concepts, themes, and subthemes.
Results
Interviews were conducted with 11 physicians, 13 nurses, 11 social workers, and 11 chaplains (n = 46). Of the 46 providers interviewed, most were female (63.1%), caucasian/white (36.9%) or Latino (32.6%), and born in the United States (74%). Most providers spoke Spanish as second language (41.2%), were of the Catholic religion (41.4%), and attended religious services several times a week (30.4%). In terms of work experience in health care settings, the majority had 5 to 10 years of experience (33%), with many having more than 20 years of experience (30%). In terms of experience working with terminally ill patients with cancer, 28% of the providers specialized in oncology, 22% had some experience, and 50% had occasional interactions with patients having cancer.
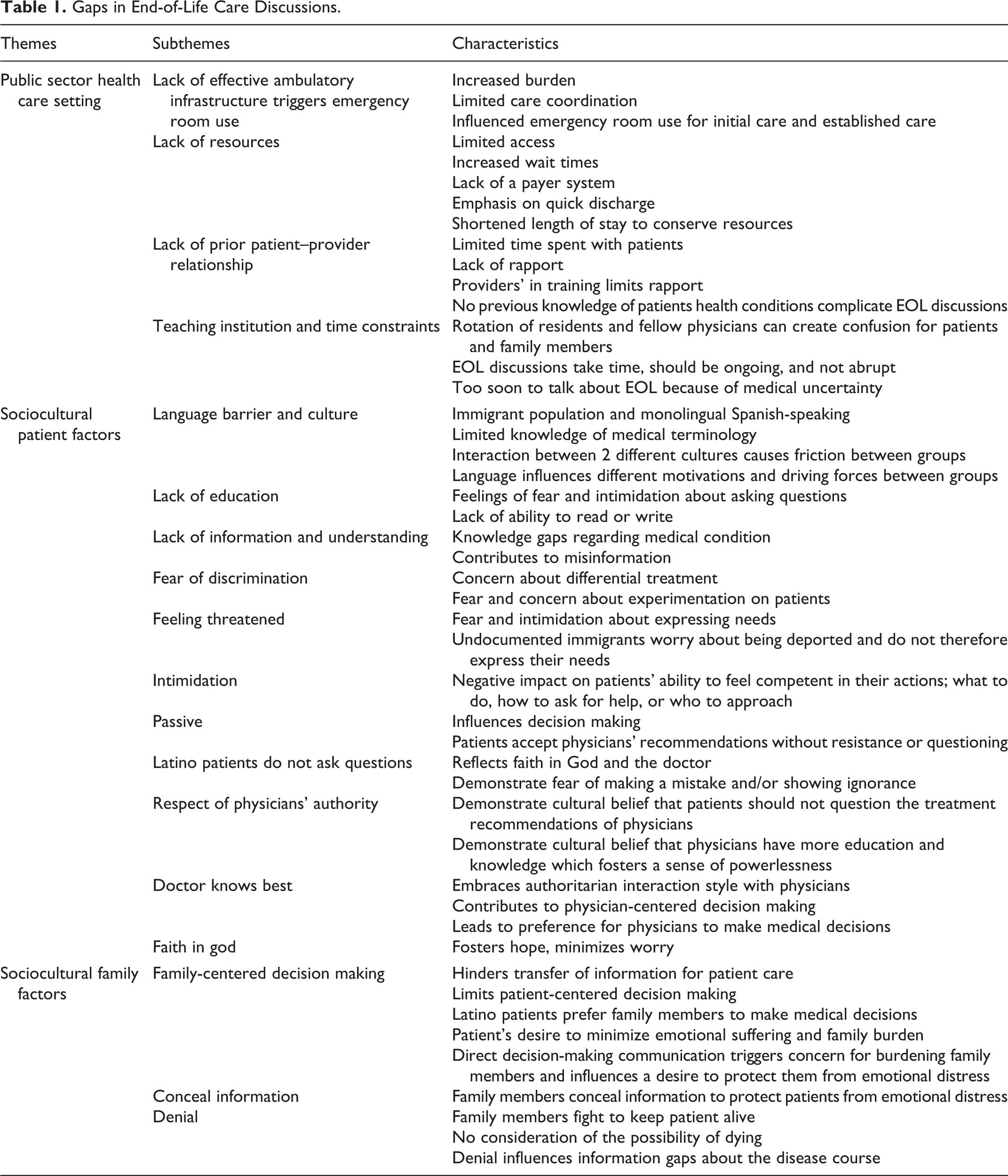
Three overarching themes elucidate the barriers to EOL care discussions, representing gaps in (1) public sector health care settings, (2) sociocultural patient factors, and (3) sociocultural family member factors (see Table 1).
Gaps in End-of-Life Care Discussions.
Theme 1: Gaps Within a Public Safety-Net Health Care System
Providers described significant issues in the public health care setting that negatively influenced patients and their families who faced a terminal illness and used the public safety-net system for their care. The lack of an ambulatory infrastructure was difficult for providers working with vulnerable patients because they often used the ED to access health care. The biggest problem as I see it is we don’t have an effective ambulatory infrastructure, and as a consequence, patients end up coming to the hospital using the Emergency Room as their access site for care; and they’re newly diagnosed with end-stage cancer [or some other life-limiting disease] (Administrative Physician 2).
As such patients wait a long time to be seen in a crowded ED. Lack of resources was a substantial burden for everyone caring for such patients. Accessibility is a problem [patients] can’t get an appointment. [They] sit in the waiting room too long…The issue is kind of like once you’re in, you’re gonna get really good care. Getting in is not going to be easy. We just don’t have enough resources… You can go in our ER today and you’ll find anywhere from 30 to 60 patients that have probably been waiting more than 12 or 15 hours to be seen. That’s horrific! (Social Work Administrator 2).
The lack of an effective ambulatory infrastructure made it emotionally challenging for providers to assess patients’ needs and develop interventions, especially when patients lacked insurance or were not a US citizen, because many were not eligible for Medicaid/MediCal benefits. Providers had difficultly arranging continuity of care for follow-up. Frequently, these issues influenced providers’ ability to provide basic care for patients, much less to have an EOL care discussion A good number of our patients end up getting their initial care, and sometimes their established care, by coming into the ER…It’s so crowded, they’re so many people that they don’t get appropriate follow-up appointments (Administrative Physician 2).
Although providers might want to schedule a follow-up appointment, they could not get their patients in for several months. Consequently, before they could be seen:
Patient ends up getting more ill or there’s complications. And then they come back…in the ER…But, they come in because there’s all of the other barriers, whether there wasn’t an appointment scheduled or there was a miscommunication, something didn’t happen, the patient is lost through the cracks. So, they come in through the ER and maybe by then they’ve developed pneumonia or something else (Social Worker 1). The resources, it’s really sad. The people are desperate here. The need is great. And it’s limited. Everybody’s limited in what they can do because of resources. And there’s only so much help you can give them. So, people really get frustrated, really frustrated, really, really frustrated, angry (Chaplain 4).
Providers said that they had difficulty engaging in EOL discussions with patients because they were often acutely ill when they finally entered the medical system. Providers explained that this was due to limited access to preventive medical care, primarily because these patients lacked health insurance or the finances to pay for care. Part of the problem was the nature of holding a serious EOL conversation with a socioeconomically poor population in an ED or hospital environment, especially among those without prior access to medical care. The setting and timing of EOL discussions were a part of this problem because underserved patients were more likely to have been denied access to care in the past due to their limited resources. When such patients were finally diagnosed with a life-threatening condition, they gained access to the medical system, but because of the advanced stage of their illness, medical treatment was unlikely to benefit them. Although treatment was likely to be ineffective, one provider said that he was most concerned about introducing the concept of withholding or withdrawing life-sustaining treatments under such circumstances: [Engaging in EOL] discussion upon admission to a hospital is the last place to do that for an impoverished population because that’s their access to care. They’ve been knocking on the door trying to get into healthcare systems, they haven’t been able to…Finally, they get into the hospital and the first thing you ask them is “How much care do you NOT want?” So it’s not the ideal place (Administrative Physician 2).
Providers said that building rapport under such circumstances was extremely difficult, making advanced care planning and discussions about EOL care wishes almost impossible.
Providers described feeling pressured to conserve resources. For example, they felt the need to see as many patients as possible and to move quickly to discharge their patients from the hospital. These issues hindered EOL care discussions. Part of the pressure involved the complexity of discharge planning and follow-up care for acutely ill patients who lacked health insurance. Although acutely ill patients finally gained access to medical care, they were difficult to discharge from the hospital. The pressure seemed to come from competing agendas in the medical system, indicating the need to conserve resources that minimized their focus on providing patient-centered EOL care discussions.
When somebody doesn’t have any money or resources, one of the biggest issues is…the hospital wants them quickly discharged [to] a lower level of care. But, you don’t have a lower level of care to send them to because they don’t qualify for an inpatient nursing home or any kind of an inpatient hospice. So, you are left with home and then you’re left now with somebody who is seriously ill requiring everything and they have no family members to take care of it. So, agendas, I think that to me is one of the most frustrating things (Physician 8). There’s a lot of pressure to get patients out, like, “Why is this patient still here?”…You know, the patients in the ER are backing up!.Oh yeah, we [social workers] argue with the doctors all the time, “This patient is not ready for discharge.” And we won’t send them out…if we don’t think that patient [is ready to discharge], we won’t participate ! (Social Work Administrator 2).
Finally, this public health care setting was a teaching institution where providers experienced the rotation of residents and fellow physicians as a serious problem for managing the continuity of EOL communication. When physicians rotated to different units each month, the transition and handoff of patient information were complex, especially with regard to EOL cases. Confusion arose because a new team would come in and had to quickly understand the focus of treatment, which could shift drastically day to day in EOL care. For example, information already discussed by one physician could be lost during transition to a new physician creating confusion. One provider mentioned, “Here at the County, we’re a teaching facility, medical teams rotate every four weeks We have a new team. There’s all these different doctors…And that can be very confusing (Nurse 8)” for patients and family members. Another provider stated that: The residents can have the [EOL] discussion, but would prefer to not do it because they rotate for a month’s period, when the time comes…they’ll have it [the EOL discussion]. [But] There’s got to be continuity of that when the next team comes. It’s more difficult because it’s not the same face…[Try to tell the patient], “My partner will be here next month” (Physician 24).
Again, this was confusing for patients because, “I think the new faces, it’s kind of like, What happened to the other doctor (Physician 27)?”
Another factor was the time it took to hold effective EOL discussions. Although the timing of a discussion was critical to EOL decision making or planning for place of death, many providers felt it was not the right time to begin a discussion. Consequently, they did not have the necessary discussions early enough, which led patients and providers to discuss these issues later, often under crisis circumstances. One provider reflected on the pressure within the system of not having enough time during the day to begin discussions during medical rounds saying: There’s pressure to get them out…[But] There is a problem that they [physicians] tend to do it on their schedule as opposed to the patient and family’s schedule. You just gotta stop and be ready to spend an hour with them on rounds…[Yet, physicians] just have their set schedule, time limits, time constraints. That’s the excuse. I don’t know what the real reason is, but that’s the excuse. And, I suppose to some degree there’s validity there, with time constraints (Physician 24).
Because they were busy during medical rounds, physicians “may tend to rush in the explanation of things. And everything may not always be clear (Nurse 9)” And, “if you’re rushing, you’re bound to make a mistake because if you miss a step or something in taking, like a shortcut, then you’re bound to make a mistake (Administrative Nurse 15).”
Theme 2: Sociocultural Patient Factors
Providers working in the public health care system reported seeing mostly underserved Latino patients, “… about 80% of our population over at the County is Latino in origin (Physician 35),” and “50% or more are on MediCal/Medicaid (Social Work Administrator 2).” Providers working with this population reported several sociocultural issues that negatively influenced EOL discussions with their patients and family members. This was especially important because patients entered the public medical setting when they were acutely ill.
First, and especially among immigrants, language barriers, compounded by knowledge deficits, and cultural beliefs influenced care because patients could not speak English or understand medical terminology and they had difficulty in relating to medical information even when it was provided in Spanish. Such issues increased the complexity of EOL discussions and medical decision making. Since patients were mostly impoverished and/or immigrants with limited English-speaking abilities, one provider said, “there’s sort of a knowledge deficit…as well as the language barrier. It requires getting a translator…[and] sometimes communication is touch and go (Physician 4).” Another provider said, A lot of them lack education. And patients feel like they shouldn’t question. How can they question? They don’t have an education. Some of them, they don’t read, they don’t write (Social worker 5).
Such factors contributed to misunderstanding and problematic EOL discussions because patients “don’t know what’s going on” with their medical condition (Chaplain 2); and “They’re not well informed of their plan of care (Social Worker 9).”
Second, providers said that patients who lacked health insurance often had limited knowledge about the health care system and accessed it only during a crisis. Patients had difficulty navigating the system in a timely manner and then experienced complex EOL situations because they generally lacked understanding and had limited resources. They may need to go to the county clinic, they need to find [it], but they don’t know where it is and then they go to the Emergency Room, they get an appointment to clinic, and then find out about the costs and restrictions to doing this. These are the problems. Well, they cannot get in quickly if they are totally unaware of the system, then this gets delayed (Physician 1).
Other sociocultural factors, such as fear of discrimination, influenced EOL discussions. Providers said that Latino patients often felt too threatened and intimidated to speak with their providers, especially in a public health care setting where the majority were immigrants and some without documentation. In the providers’ experience, Latinos generally followed their physician’s suggestions passively. Providers experienced Latinos as passive because they did not ask questions and generally followed their physician’s suggestions without questioning. Providers commonly reported that Latinos believed in God and in the doctor knowing what was best for their condition; therefore, they simply accepted their medical treatment. Although such strong religious beliefs fostered a sense of powerlessness, they also helped patients cope with a terminal condition. However, the same beliefs hindered EOL discussions. Many Latino patients are timid, quiet, and not asking a lot of questions, or maybe it may be that they’re putting their faith in the doctor. It may also be that they are here on tenuous grounds and they don’t want to make trouble in clinic. (Physician 1)
Latino patients using the public medical system were “afraid to make mistakes…they’re afraid to speak and afraid to ask questions of the doctors…, not knowing the [medical] terms and then also not wanting to show ignorance (Chaplain 8).”
Theme 3: Sociocultural Family Level Factors
End-of-life discussions were complicated when family members lived elsewhere and were unaware of their loved one’s illness or the serious nature of their terminal condition. Family members engaged in EOL discussions too late, which sometimes caused conflict between patients and providers, especially when information was provided to the patient without their family members present and when they had made decisions about the course of treatment. They have family members from out of state or the country. So, we want to keep this person alive until their family member can come in from Mexico; and we have to do the immigration letter. And there are other factors involved too; maybe they want to keep them alive NOT necessarily for the benefit of the patient, but because of the finances. So, a lot of these other ancillary issues are involved which maybe on the surface they don’t express to us. But, ultimately it comes into play in decision-making. So it’s complicated (Physician 27).
Family members had emotional reactions to being uninformed about their loved one and then were promptly engaged in decision making which was difficult to comprehend. Now suddenly we have more conflict “Why did you do this? Why did you do that? Why didn’t you discuss it with me?” And it’s like well, I [pause] “the patient and I had an agreement. We were doing it this way.” It’s tough sometimes, the whole thing is [pause], whenever someone has end-of-life issues its tough (Physician 31).
Sociocultural family-level factors also contributed to the complexity of EOL discussions because family members sometimes made decisions for the patient without clearly knowing the patient’s wishes. “A lot of times they don’t speak to each other about what they want (Nurse 13).” One provider explained that Latino patients might prefer to let their family members make decisions without their input: Many times the patient doesn’t want to hurt her family or his family. So they accept whatever the family decides. [Latino patients], we allow our families to make the decisions for us because we trust in them. And even though at times it’s not what I really want, I trust that they will make that best decision for me (Chaplain 3).
Conversely, in circumstances where patients were unable to participate in decision making, some Latino families preferred to disengage and refused to designate someone to assist with EOL decision making. The problem with this was that no one person in the Latino family wanted to be singled out to talk with providers because if this person were to make any medical decisions, other family members might hold him or her accountable for anything that happened to their loved one.
Another issue involved family members wishing to hide medical information from the patients; they sometimes asked the physician not to disclose bad news. With very sick patients, their families: … tend to want to make decisions and tend to want to kinda [pauses, chooses words slowly] hide certain things from the patient. They don’t want them to know everything. And so sometimes…there may be some type of miscommunication in understanding…And, sometimes family members have a difficulty in that too. But, the biggest thing is hiding information from the patients themselves (Nurse 9).
Although providers agreed that family members were trying to protect their loved one from bad news by doing this, they restricted the ease of patient–provider EOL communication.
Discussion
An array of factors burden the system, making EOL care communication more problematic. Working in a public safety-net health care system presented unique challenges for providers who intended to dialogue with their terminally ill patients about EOL care. Similar to other research with vulnerable patients, providers indicated that their patients, mostly Latino, delayed seeking medical treatment until acutely ill, which prompted them to utilize the ED and hospital for their care. 30 Under such conditions, patients were very sick when they entered the medical system, making it more difficult to discuss the possibility of dying and plan for death. Although public safety-net health care systems provide free or low-cost medical care to many individuals, they have limited resources so uninsured patients, with multiple socioeconomic barriers, may be more likely to receive substandard care. 31 Providers limited information about EOL care resources because they felt rushed or pushed to move patients quickly through the system. This affects the timing of discussions.
Providers experienced time constraints stemming from multiple agendas within the public safety-net system. They often lacked resources and, as a teaching institution, afforded patients and providers limited time together. Consistent with prior qualitative studies with similar sample size, providers experienced time barriers where a provider might wait to initiate EOL discussions until patients or family members appear ready to talk or wait until the patient initiates a discussion. 32 Findings from Clayton et al 32 suggest that providers need to carefully clarify important information in detail while gathering information about what patients already know regarding their illness and determining how much information they wish to know before giving too much. 32 In this study, EOL care communication was especially complicated because individuals entered the medical setting when they were already seriously ill and in late stages of their disease. Patients may have never seen a physician for their medical problems. Conflict can arise when they meet their physician and learn about their terminal, life-threatening condition for the first time. Under such conditions, there might never be a “right time” to begin an EOL care discussion; this created further communication gaps between patients and providers.
Sociocultural patient and family-level factors also influenced EOL discussions which made beginning an early EOL discussion extremely complex for providers, patients, and families utilizing the public safety-net medical system for EOL care. Consistent with other qualitative research in which semistructured interviews were used, providers experienced barriers that limited the timing of discussions and hindered referrals to hospice and palliative care, especially among Latinos. 8,33 Carrion 8 found that providers lacked knowledge about cultural beliefs and had limited skills to engage Latino patients in EOL care communication. 8 In this study, although providers promptly needed to engage patients in patient-centered discussions, cultural factors, like strong religious beliefs, fostered a sense of powerlessness while limiting EOL discussions. This is especially important for vulnerable Latinos because they can feel intimidated to express their needs when they are undocumented and/or uninsured and because their family members may have limited prior involvement in their care.
Implications
The challenges in EOL communication were clearly more complex for providers working in safety-net health care systems. Improving EOL care for vulnerable populations at the end of life will require collaboration across all disciplines including physicians, nurses, social workers, and chaplains. Although some providers might consider nonmedical staff, like social workers and chaplains, as ancillary staff who are not involved in the provision of medical care, such providers clearly recognize the barriers to EOL communication. Although the diverse, small sample of providers represented in this study limits generalizability of these findings, the rich data demonstrated that all providers made valuable contributions to clarify the complexity of the problems that impact EOL care discussions in this context. As suggested by Smith et al 34 , all providers could use universal strategies to improve communication by asking patients and family members what they already know about the likelihood of dying, using simple language, encouraging questions, respecting patients’ wishes for engaging in EOL conversations, and using teach-back methods to confirm patients’ understanding. 34
Additionally, we suggest that all providers involved in patient care must work together to improve EOL communication through strategies that foster cross-disciplinary and inter-disciplinary teamwork throughout medical systems. Clear documentation of EOL discussions could indicate patients’ preferences for conversations and identify limitations that providers are obligated to understand when engaging patients in difficult conversations. Together, providers must embrace new strategies to develop and foster trustworthiness of all health care professionals for the most vulnerable populations.
Footnotes
Author’s Note
A version of this manuscript was presented as a poster at the Society for Social Work and Research (SSWR) 16th Annual Conference in Washington, DC, on January 14, 2012.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the American Cancer Society Doctoral Training Grants in Oncology Social Work DSW-06-220-01-SW (F. R. Nedjat-Haiem, PI), and US Department of Veterans Affairs, Hartford/VA Social Work Scholars Program.