
Abstract
Improving symptom management for palliative care patients has obvious benefits for patients and advantages for the clinicians, as workload demands and work-related stress can be reduced when the emergent symptoms of patients are managed in a timely manner. The use of emergency medication kits (EMKs) can provide such timely symptom relief. The purpose of this study was to conduct a survey of a local service to examine views on medication management before and after the implementation of an EMK and to conduct a nationwide prevalence survey examining the use of EMKs in Australia. Most respondents from community palliative care services indicated that EMKs were not being supplied to palliative care patients but believed such an intervention could improve patient care.
Introduction
Poor symptom management for palliative care patients is an issue that arises for both patients and caregivers and consequently can have a significant impact on workload and demands on clinical staff to manage unexpected symptoms, as they emerge if preemptive treatment planning is not implemented. Obtaining and providing symptom relief to patients when parenteral medications are unavailable in the home can be time consuming and distressing 1 and decrease the likelihood that patients will remain at home if this is their preferred place of death. 2,3 In contrast, the provision of an emergency medication kit (EMK) provides a minimal supply of medications to address exacerbations of pain, nausea, agitation, and respiratory distress in a timely manner. 1,4,5
Emergency medication kits contain parenteral subcutaneous medications that address symptoms, which frequently arise in palliative care patients. Previous international studies have found that the provision of EMKs is an effective way of reducing emergency hospital admissions due to poorly controlled symptoms. 4,6 Wowchuk and colleagues4 demonstrated that the placement of an EMK in homes of palliative care patients increases the likelihood of a death at home. The provision of EMKs to patients with cardiac disease has also been found to significantly decrease the likelihood of an emergency hospital admission. 6 However, these studies are not without limitations and should be interpreted with caution.
Currently, the research published to date about EMKs and their use has been limited with no literature regarding implementation published in the Australian context. Therefore, in order to better understand the difficulties of medication management and the diversity of processes in community palliative care services in Australia, palliative care services were surveyed about their use of EMKs to further the research of Bishop and colleagues in an Australian context.
The purpose of this study was to conduct a local and a nationwide survey of community palliative care services to develop an understanding of symptom management across services and whether there was perceived value in the concept of an EMK as an intervention that could improve patient outcomes.
Objectives
To explore views of staff at the local community palliative care service on management of medication before and after the implementation of an EMK. To conduct an online survey of clinicians working in community palliative care services to determine prevalence of use of EMKs and existing procedures of supplying medication.
Method
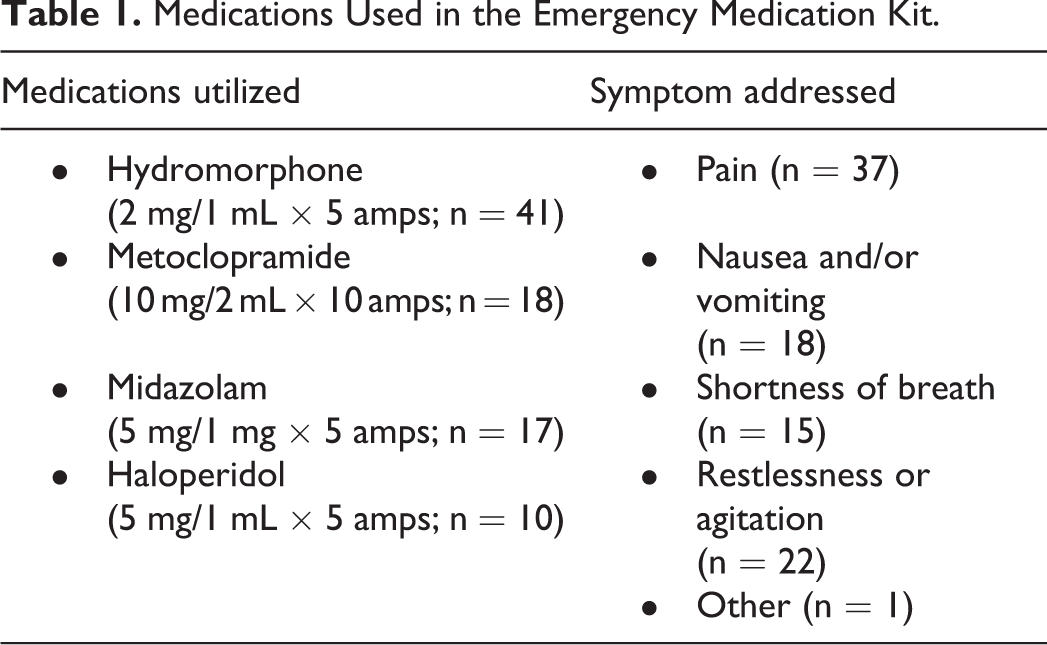
This study was an uncontrolled prospective pilot intervention performed within a single community specialist palliative care service. Patients who were referred to the community specialist palliative care service were identified along with their caregiver and screened for eligibility. Consenting patient caregiver dyads were provided with an EMK and a medication diary. The EMK consisted of minimal dosage ampoules of hydromorphone, metoclopramide, midazolam, and haloperidol as recommended by the Therapeutic Guidelines: Palliative Care 7 for subcutaneous injections (see Table 1). The medication diary was adapted from a current validated resource package 8 as an educational resource for patients and caregivers and to record when medications were accessed.
Medications Used in the Emergency Medication Kit.
Phase 1
The first phase of the study was a pre–post comparison design to assess the views of medication management of the nursing staff working within a specialist community palliative care service prior to participant recruitment and at the conclusion of a trial implementing an EMK to determine whether the implementation of the EMK had improved clinical practice. The clinical staff also completed a survey evaluating their experiences of participating in the trial.
Members of the clinical team were directly approached by the members of the investigating team to participate in the study, as the researchers were colocated within the service. The surveys and consent forms were distributed to the community specialist palliative care staff as they were responsible for recruitment and administration of emergency medications to patients and were impacted directly by problems with symptom crises.
All members of the community specialist palliative care team attended regular education sessions about the trial that addressed issues regarding the nature of the kit, obtaining consent, questionnaire measures, and recruitment. All 10 members of the community team were level 2 registered nurses and completed the pretrial questionnaire prior to the research study training session in order to minimize bias in the responses.
Phase 2
The second phase of the study was a cross-sectional quantitative design. One hundred and eighty nine community palliative care services were identified across Australia, which had publicly available e-mail addresses. Contact information was obtained from the Palliative Care Australia service directory. The survey details were e-mailed to the palliative care services by the research investigator, and the survey was completed online between November 2012 and February 2013 with the aim of obtaining a single response from each service approached to obtain a brief understanding of current medication management practices in community palliative care services. The survey was designed to replicate 2 international studies 1,5 in order to compare the findings with the Australian context. The data collected using the survey tool included whether the service used EMKs and whether current practice met patient needs. The survey also assessed the impact of use of the kits, EMK usage, and cost. Respondents answered different questions dependent upon whether the service used EMKs or not. Most participants were clinical nurse consultants or hospice managers. Ethics approval was obtained from the relevant industry and university Human Research and Ethics Committees.
The research team purpose designed the phase 1 questionnaire for staff who were participating in the trial as recruiters to identify current unmet needs in practice and to see whether the presence of the kit had addressed these needs. A copy of the items exploring medication and symptom management issues is provided in the appendices. The phase 2 questionnaire combined survey items from 2 international studies examining the use of EMKs in the palliative setting to obtain a complete picture of hospice management of symptom crises in the Australian context (see Appendix B). 1,5 Items included in the phase 1 survey were also included in the prevalence survey for comparison purposes. Information was collected to obtain profiles on both services that currently used or did not use EMKs.
Data Analysis
Analyses were conducted with SPSS version 21.0. Descriptive statistics were used to report the staff data. Frequencies and percentages of the survey variables were computed. For the prevalence survey study, the frequencies and percentages for each survey item using the total number of valid responses (n) were reported. As the survey items varied depending on whether the respondent’s service utilized EMKs or not, these frequency data are reported separately.
Results
Survey of Clinical Staff
All members of the community nursing team completed a pretrial survey about medication management (n = 10). The majority of the community nursing team reported a number of areas of medication management that were inadequate or needed to be improved (see Table 2).
Pretrial and Posttrial Assessment of Community Palliative Care Medication Management.
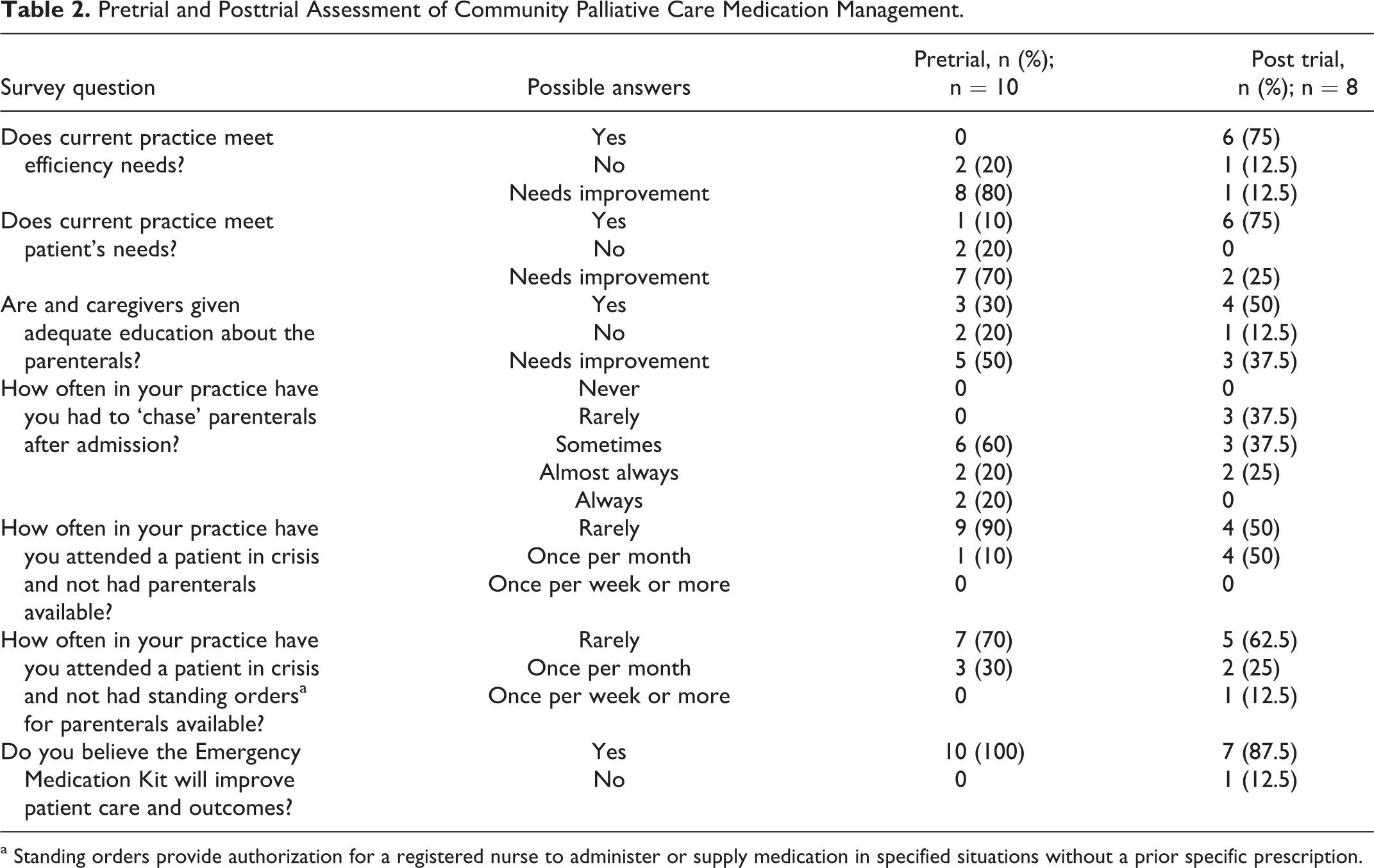
a Standing orders provide authorization for a registered nurse to administer or supply medication in specified situations without a prior specific prescription.
Eight team members completed the survey at follow-up. The reason for the attrition was that 2 members of the team had left the service. When the posttrial evaluation survey was administered, 88% of respondents (n = 7) reported the implementation of the EMK had improved patient outcomes. The post-EMK trial survey also assessed the clinicians’ experiences of implementing the EMK and found all respondents had administered medications from an EMK for a patient during the trial, and in the majority of instances, the medications in the kit had met patients’ needs. In addition, most staff reported a reduction in work stress following the implementation of the EMK (see Table 3).
Survey Results Post-EMK Implementation.
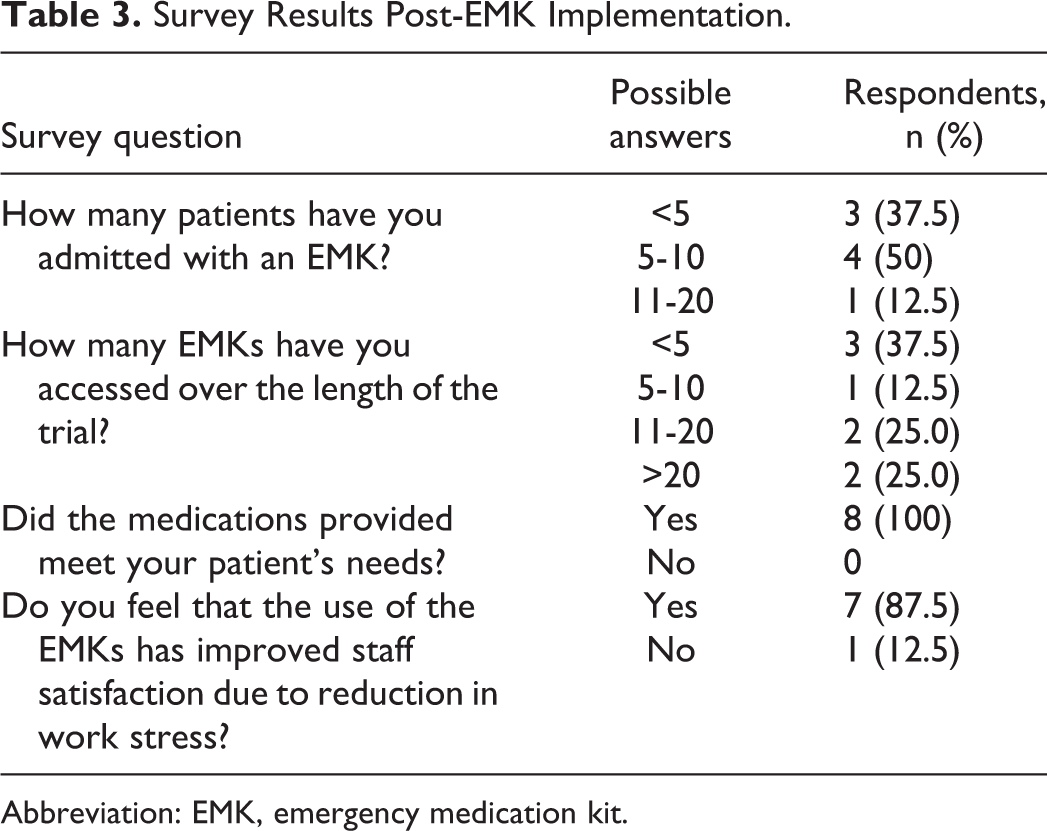
Abbreviation: EMK, emergency medication kit.
Survey of Community Palliative Care Services
A total of 54 respondents from 43 community palliative care services completed the online survey. Within this group of respondents, 32% were from Victoria, (n = 17), 28% were from New South Wales (n = 15), 22% were from Queensland (n = 12), 15% were from South Australia (n = 8), and 4% from the Northern Territory (n = 2). Participants were employed in a variety of positions (see Table 4). Of the services surveyed, 23 respondents reported using an EMK (see Table 5). These services had a variety of names for these medications including emergency medications, support medications, or crisis kits. When emergency medications were ordered by “other” professionals, it varied between the palliative care specialist and the patient’s general practitioner. Contents of the kits addressed pain, nausea, agitation/distress, and dyspnea. Other symptoms addressed included respiratory secretions, delirium, or seizures. Cost of the kit varied between US$1 and more than US$50 with the majority of kits costing between US$31 and US$50, and cost of the EMKs was not provided by 6 respondents. One service indicated that EMKs were provided upon admission. Most respondents reported that the administration of emergency medications was highly variable and usually occurred when the patient entered a deteriorating or terminal phase of care.
Participant Designation.
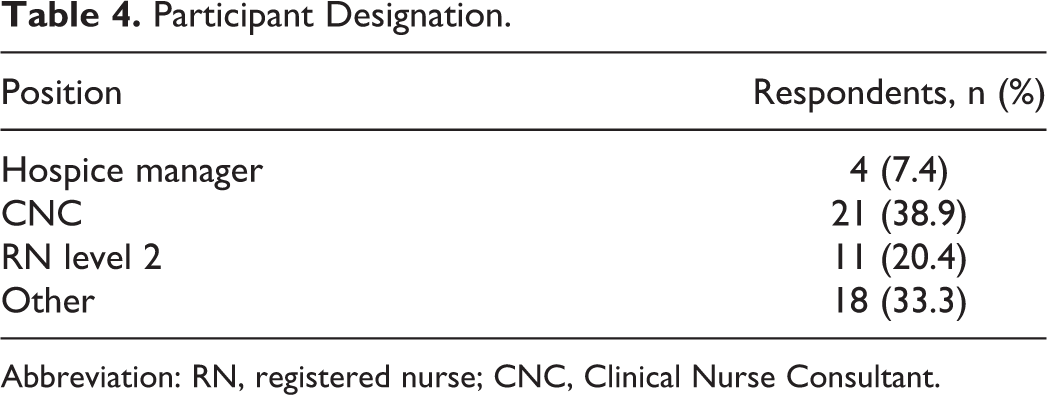
Abbreviation: RN, registered nurse; CNC, Clinical Nurse Consultant.
Survey Results of Services That Use Emergency Medication Kits.
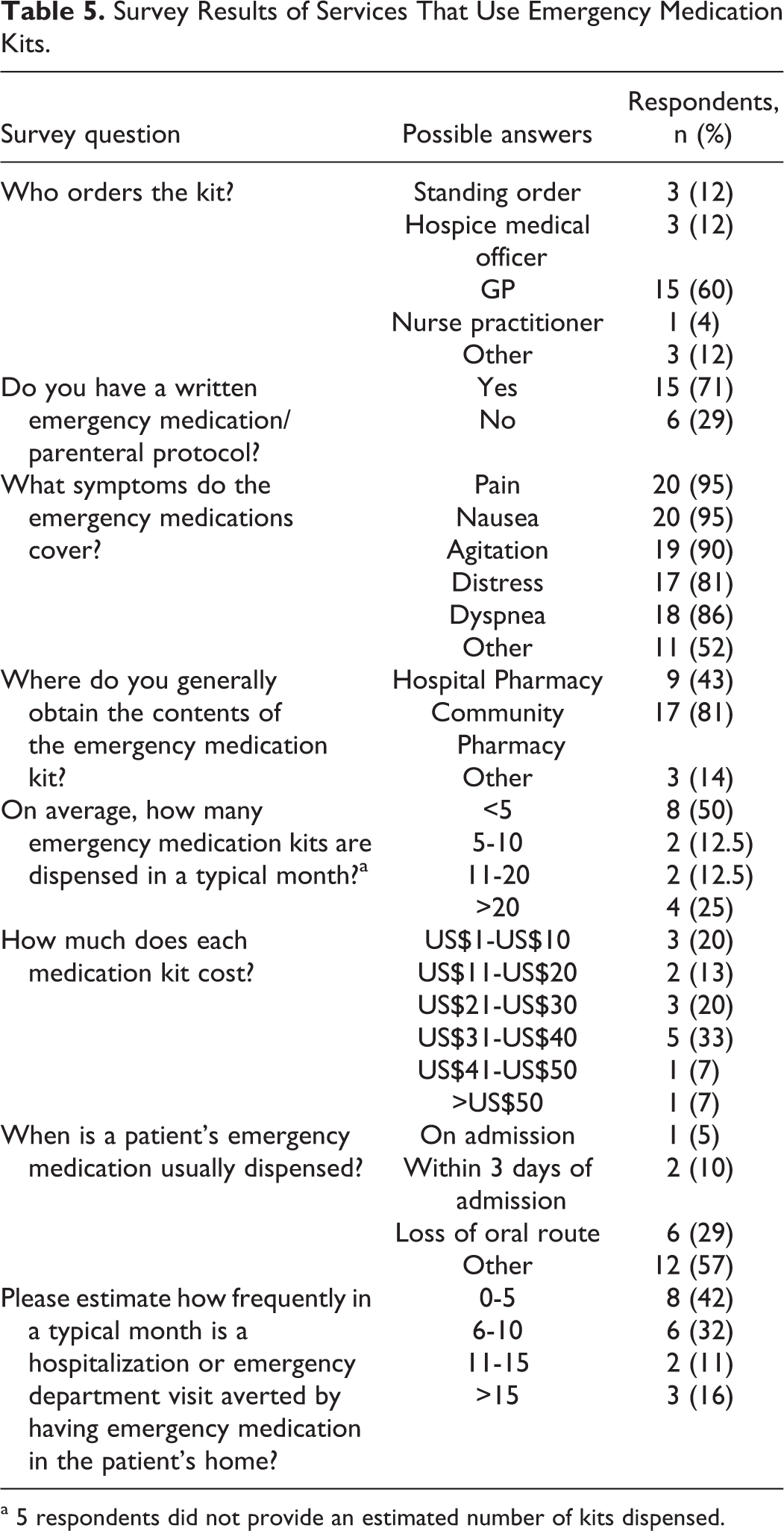
a 5 respondents did not provide an estimated number of kits dispensed.
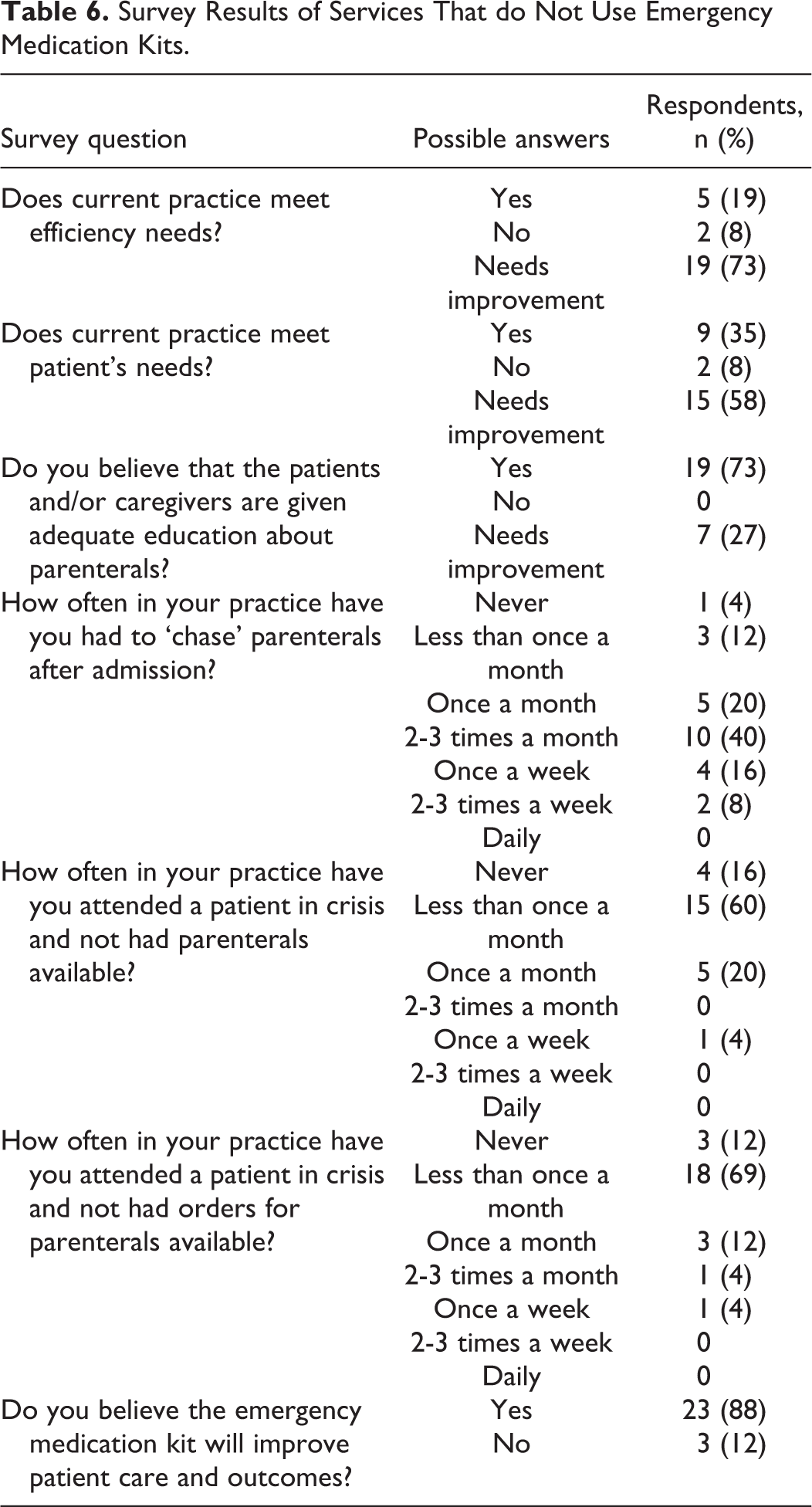
The majority of services surveyed reported they did not use an EMK (n = 31, see Table 6). These respondents reported that the current practice of obtaining parenteral medications needed improvement in meeting efficiency and patient needs. For majority of the services, emergency medications were unavailable less than once per month when needed for patients. Most participants from services who did not utilize EMKs believed that EMKs could improve patient care.
Survey Results of Services That do Not Use Emergency Medication Kits.
Discussion
Based on our findings, the implementation of the EMK in the local community service had improved current practice. The practice change had lead to an improvement in meeting patient needs, as the frequency of needing to obtain parenteral medications unexpectedly following admission had reduced. The majority of staff also reported the use of the EMK had improved patient outcomes and reduced work stress. Interestingly, a search of the literature failed to identify any previous studies that explored the impact of EMK use upon staff. However, improving symptom management of patients in the community can enhance the capacity of palliative care nurses to care for more patients. 8
For context, the prevalence survey data will be discussed in relation to the results of previous international studies. 1,5 Similar to the results of Walker and McPherson, there was variability across services as to whether an EMK had been implemented. This is unsurprising, as there are differing legislative requirements across jurisdictions in Australia relating to the transport of restricted medications. Such variability in the transportation of scheduled medications has the potential to impact upon quality of care across services at a time when national standards and benchmarks for palliative care are being implemented.
Among services that used EMKs, there were similarities to services that utilized them in the United States. Among those providing kits, visits to the emergency department or unexpected hospitalizations were estimated to have been averted on up to 5 occasions in a typical month in the majority of cases for both Australian services using EMKs and in Maryland. The numbers of kits dispensed in a typical month (less than 10) and the cost of each medication kit (less than US$50) were also comparable, suggesting that this intervention is a relatively low cost approach to potentially improving patient care given it appears to assist in averting emergency visits to hospital when symptom crises occur. Similar to findings of Walker and McPherson, there was variation as to when medication kits were ordered, whether there were protocols in place for the kits’ use, and contents of the kits. However, the presence of analgesic and antiemetic medications seemed reasonably consistent both in Australia and internationally. The current study found that emergency medications tended to be implemented later during an admission such as when patients were noticeably deteriorating or there was a change in their condition, suggesting that if emergency medications were supplied it was on an individualized basis. In contrast, Bishop and colleagues found these medications were generally dispensed at admission or within 72 hours of admission to the service. Greater consistency when parenteral medications are provided to community palliative care patients has the potential to improve the efficiency of a service and address patient needs more quickly and averting more emergency visits to hospital. 4
Among the respondents from participating services who did not use an EMK, a sizable percentage reported that an EMK would improve patient outcomes if implemented in their service which was supported by the findings that current practice needed improvement as trying to obtain parenteral medication following admission was a frequent occurrence. Such a strong response regarding the implementation of an EMK indicates a definite need for an alteration in the current practice. Study of Walker and McPherson further supports this view, given that for services where EMKs were not in use despite having access to a 24-hour pharmacy delivery times could vary between 1 and 3 hours which would be inadequate for a patient experiencing an exacerbation of symptoms such as pain or distress. Delays such as this can decrease the likelihood of patients remaining at home if this is their wish.
Limitations
There are important limitations to this study. Although attempts were made to contact a large number of community palliative care services seeking participation, the number of respondents were low resulting in a small sample size, thus the results may not generalize to services elsewhere. However, participants came from a number of states providing a snapshot of current practice across the country. The divergence in practice, that is, the differences in frequency of providing EMKs, suggests this is one area of palliative care where consistency in service provision to meet national standards can be improved. Second, the brief survey assessed perceptions of health care professionals, and the findings were not verified by service statistics to determine accurate usage levels of emergency medications. This study does, however, provide some insight into the similarities and differences in dispensing practices both in Australia and in the United States and strengthen the hypotheses that adverse outcomes such as unplanned admissions to hospital can be averted with the preemptive planning for symptom crises. Further research comparing community palliative care services with contrasting approaches to emergency medication provision should be developed.
Conclusions
The use of the EMK intervention is not consistent across Australia; however, the survey results of the nursing staff of the local service did indicate an improvement in meeting workload efficiency and patient needs following the implementation of the EMK as well as a perceived improvement in work stress which is not only a benefit for acutely unwell patients but also for those providing crucial care. This study contributes to the knowledge base of medication provision for further research and practice change. There appears to be perceived advantages to providing EMK to eligible palliative care patients due to the contribution of EMKs to improve the management of patient needs and reduce work stress which in turn has the potential to improve the management of symptom exacerbations in a timely manner. The interest in facilitating the use of EMKs where they are currently not being implemented also suggests that the way symptom crises are being managed needs to be improved for patients and caregivers and also for clinicians. Future research exploring the economics and feasibility of this intervention is warranted.
Footnotes
Appendix A
Appendix B
Acknowledgement
The authors wish to acknowledge the contribution of the community specialist palliative care services who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The trial was funded by a Practice Development Grant awarded by the Australian National University Research Centre for Nursing and Midwifery Practice, Canberra, Australia.