
Abstract
Background:
Withdrawing artificial nutrition in palliative care is an issue that often leads to ethical dilemmas among health care providers, despite clinical guidelines.
Objectives:
To describe the experience of health care providers confronted with the withdrawing of artificial nutrition at the end of life and identifying the factors related to the level of ethical dilemmas.
Methods:
Cross-sectional survey questionnaire of all the nurses and nurses’ aides working in medicine, surgery, and palliative care departments of a regional hospital and who have already been confronted with the withdrawal of artificial nutrition.
Results:
Of 818 questionnaires sent, 274 were returned (response rate 33.5%); 60% (163) of the care providers who responded were involved in withdrawing artificial nutrition at the end of life. Among these, 42 (25.8%) had always or often been affected with ethical dilemmas, and 97 (60%) responded that withdrawing artificial nutrition had always or often been preceded by a multidisciplinary discussion. Items significantly associated with a high level of ethical dilemmas were (1) existence of differences in opinion within the health care team, (2) lack of information regarding the indication of the withdrawal of artificial nutrition, (3) feeling uncomfortable with the patient and his or her relatives, (4) guilt, (5) feeling of abandonment of care, and (6) uneasiness.
Conclusion:
Health care providers seem to have a lack of information and consensus regarding the withdrawal of artificial nutrition at the end of life. The ethical dimension of withdrawing artificial nutrition in palliative care has a strong impact on care providers, regardless of the circumstances of the withdrawal.
Introduction
The benefit of artificial nutrition in terminally ill patients has been a highly debated issue for the past 30 years, and abundant data are available regarding its effects on patients.
Several clinical guidelines have specified the criteria to be considered before initiating artificial nutrition or hydration. 1,2 If these guidelines appear consensual in theory, the situation is much less straightforward in practice. The attitude of physicians appeared very variable when it came to prescribing or withholding artificial nutrition or hydration, 3 –5 and the lack of training, among other parameters, seemingly encouraged health care professionals to prescribe artificial nutrition or hydration. 6
Furthermore, the decision of the care provider is unconsciously complicated due to figurative representations associated with food regarding, among other aspects, the mother–child relationship, social cohesion, or religious beliefs. 7 –14
These differences are more important since the opinion of physicians and nurses is the one that carries the most influence on the patients’ decision when deciding to initiate artificial nutrition 15 and because artificial nutrition and hydration are a common source of ethical dilemmas in health care teams. 16,17 Furthermore, stopping artificial nutrition or hydration could be misconstrued as euthanasia. 18
We deemed it of interest to evaluate the experiences of health care providers confronted with the withdrawal of artificial nutrition, given that since that the French legal framework was modified by the law of April 22, 2005, artificial nutrition and artificial hydration are explicitly considered as treatments and can therefore legally be stopped under specific conditions and depending on whether the patient is able to give consent or not.
The aim of this study was to better understand the experiences of nurses and nurses’ aides confronted with the withdrawing of artificial nutrition through 2 objectives: (1) to describe the perception of care providers with regard to the withdrawal of artificial nutrition, and (2) to identify the factors associated with the occurrence of ethical dilemmas.
Methods
Study Design
The data presented herein are from a larger study regarding the experiences and feelings while withdrawing artificial nutrition in terminally ill patients. This study was conducted by sending a questionnaire to health care providers working at the regional hospital of Metz-Thionville, located in Lorraine (France), comprised of nearly 2000 beds. The questionnaire was personally sent to every care provider, in order to maximize the response rate, along with a cover letter explaining the goals of the study and guaranteeing the anonymity of the responses. The questionnaire, approved by hospital management, was sent by internal mail with a return envelope. The sending of questionnaires ranged from May 17 to May 25, 2010, and answers were taken into account until the deadline of August 2, 2010.
Population
The target population included all senior nurses, nurses, and nurses’ aides working in medicine, surgery, and palliative care departments of the regional hospital of Metz-Thionville, France.
Care providers working in pediatrics, gynecology and obstetrics, psychiatry, and emergency departments were deliberately excluded, given that they are seldom concerned with withholding artificial nutrition in patients at end of life.
The questionnaire was sent to 818 care providers working in 51 different departments (24 senior nurses, 444 nurses, and 350 nurses’ aides).
Questionnaire
Because of a lack of validated tools, the questionnaire was developed through literature review. 10,16,17,19 –24 The literature review first showed that withdrawing artificial nutrition is one of the most important ethical dilemmas in palliative care. 17,24 The literature also highlighted several concepts that may contribute to care provider stress, such as the existence of work stressors (team communication problems, communication problems with patients and family or role ambiguity, among others) or lack of information on the management of patient care. The expert panel proposed a series of items corresponding to each of the concepts highlighted by the above-mentioned review. Items were then selected by consensus between the experts and the questionnaire was tested on a sample of 5 nurses to whom it was asked to identify the difficulties in understanding the items or in answering the proposed questions.
The questionnaire consisted of 11 questions divided into 3 distinct parts regarding (1) care provider characteristics, (2) the experiences of care providers when confronted with withdrawing artificial nutrition in terminally ill patients, and (3) the feelings and general knowledge of care providers with regard to the withdrawal of artificial nutrition, whether they had encountered such situations in their daily practice or not.
The response modalities were either yes/no or always/often/rarely/never. Only the questions of the first 2 parts of the questionnaire were analyzed in the present study and are detailed in Table 2 (for example: “have you always, often, rarely or never been informed of the reason for withdrawing artificial nutrition?” or “when artificial nutrition was withdrawn, did you feel or not a sense of abandonment of care?”). Data from the third part are the subject of a parallel study, the aim of which is to compare the perception of withdrawing artificial nutrition among care providers having faced this situation with those who have never faced this situation. 25 The questionnaire is available from the authors (in French).
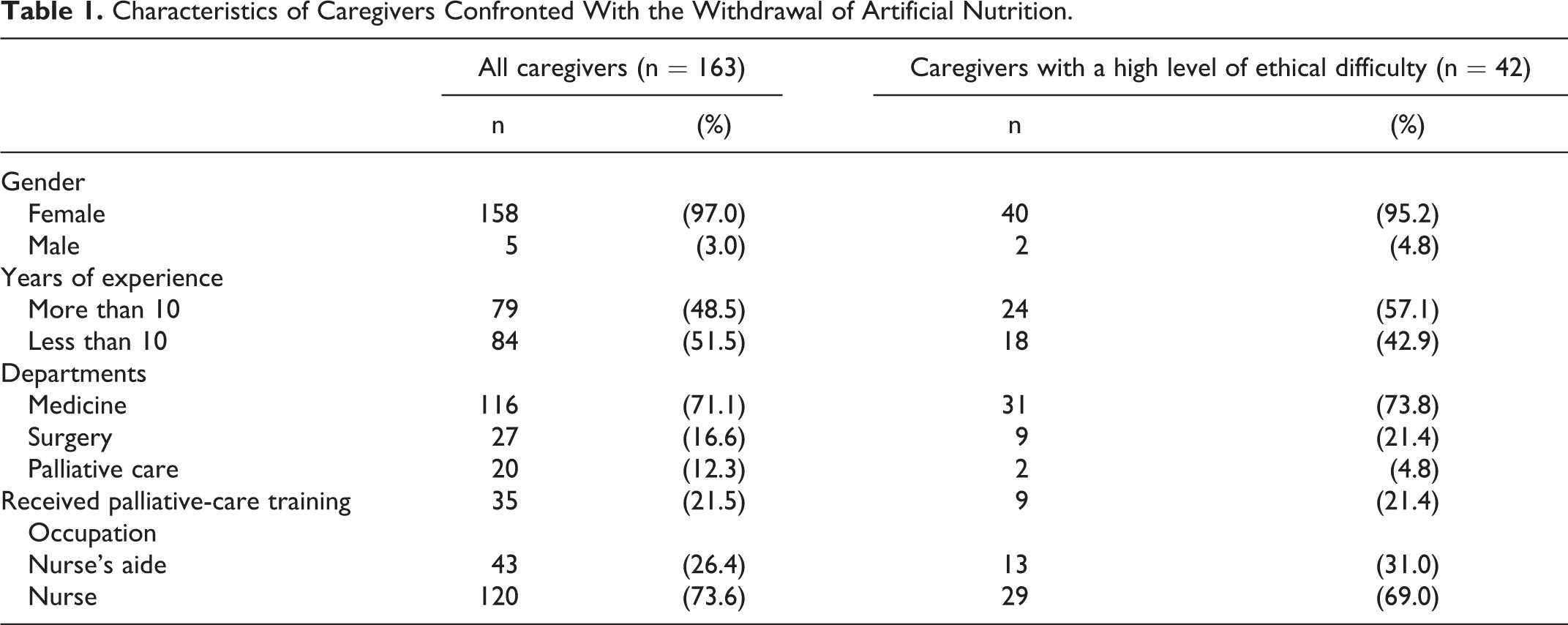
Characteristics of Caregivers Confronted With the Withdrawal of Artificial Nutrition.
Description of the Circumstances of the Withdrawal of Artificial Nutrition and Experiences of Caregivers.a
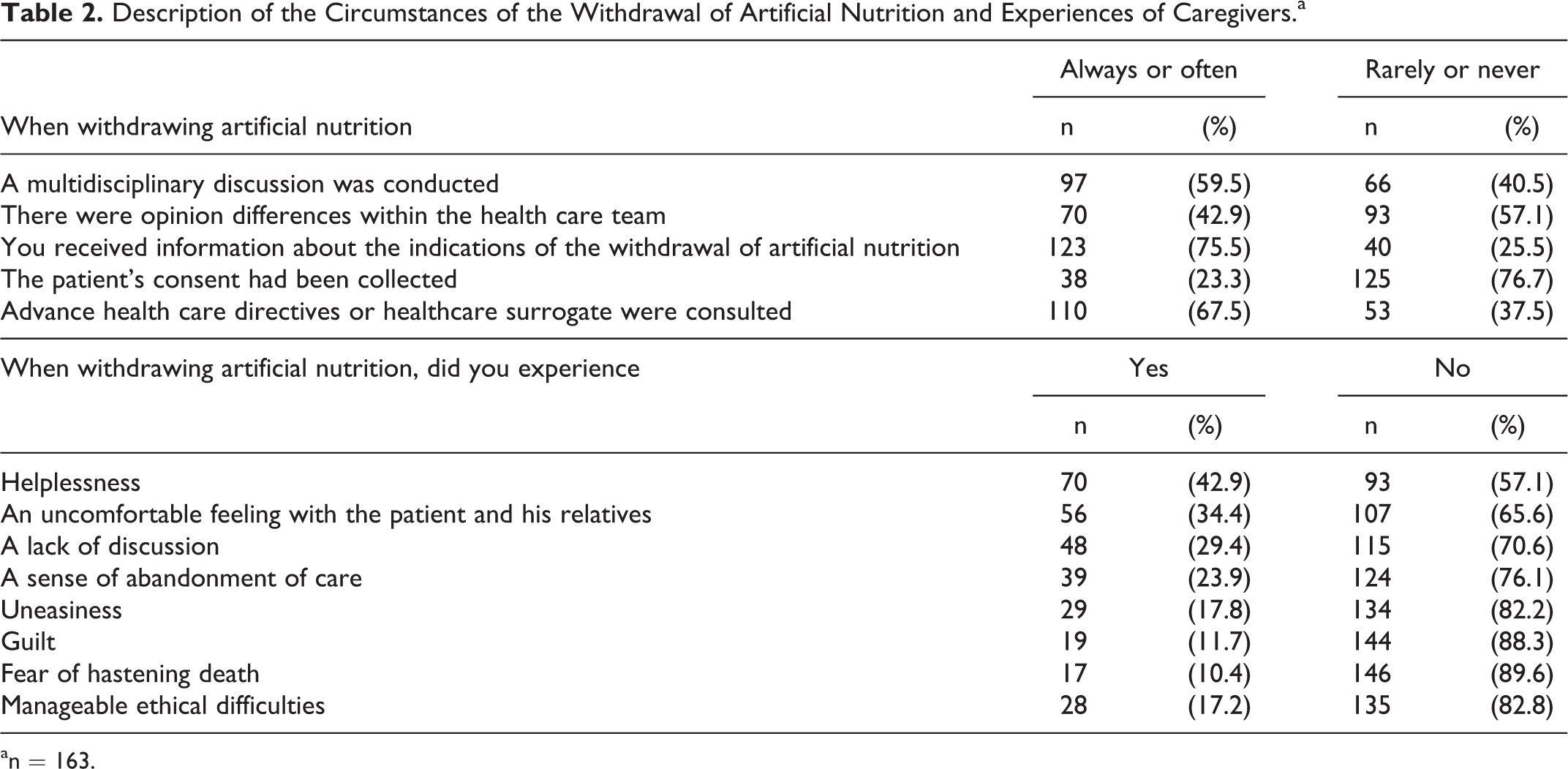
a n = 163.
Statistical Analysis
Responses to each item of the questionnaire were analyzed in terms of numbers and percentages. In order to identify the factors associated with the perception of ethical dilemmas by care providers, the respondents were divided into 2 groups according to the level of perceived ethical dilemma, estimated from the answers to the question “have you always, often, rarely, or never experienced ethical dilemmas when confronted with the withdrawal of artificial nutrition”: (1) care providers with a high level of ethical dilemmas (combining those who claimed that they always or often perceived ethical dilemmas when confronted with withdrawing artificial nutrition) and (2) care providers with a low level of ethical dilemmas (combining those who claimed they rarely or never perceived ethical dilemmas when confronted with withdrawing artificial nutrition). The other items whose answer modalities were always/often/rarely/never were analyzed by combining already/often and rarely/never responses. The variables were first compared between groups with high and low levels of ethical dilemmas using Fisher exact test (bivariate analysis), after which a multivariate analysis was performed using logistic regression with the level of perceived ethical dilemmas as dependent variable and all suspected factors as explanatory variables. The significance level was set at 5%. Analyses were performed using SAS 8.01 software (SAS Inst, Cary, North Carolina).
Results
Of the 818 care providers surveyed, 289 returned the questionnaire. Of these, 15 questionnaires were excluded because of incomplete responses, hence a total of 274 questionnaires were finally analyzed (effective response rate: 33.5%). A total of 163 of the 274 care providers who answered the study claimed that they were involved in withdrawing artificial nutrition.
The characteristics of the care providers who had already been confronted with withdrawing artificial nutrition are detailed in Table 1. No significant differences were observed with regard to characteristics between care providers with a high level of ethical dilemmas and those with a low level of ethical dilemmas.
Of the 163 care providers who were faced with the withdrawing of artificial nutrition, 42 (25.8%) reported they had always or often encountered ethical dilemmas (high level of ethical dilemmas). More than half of the care providers said that withdrawing artificial nutrition had always or often been preceded by a multidisciplinary discussion and that there had rarely or never been differences in opinions within the health care team (Table 2). Three-quarters of the care providers said that they had always or often been informed about the indication of the withdrawal of artificial nutrition while the patient’s consent had rarely or never been collected. Two-thirds of the care providers said that the advance health directives or health care surrogate had always or often been consulted.
The 3 most common feelings experienced by care providers when withdrawing artificial nutrition were helplessness, an uncomfortable feeling with the patient and his or her relatives, and the lack of dialogue (Table 2). Guilt and the fear of hastening death were mentioned by only 1 care provider of 10.
Among the circumstances in which the decision to withdraw artificial nutrition was made, no significant correlation was observed between the existence of a multidisciplinary discussion, the collection of the patient’s informed consent, and the consultation of advance health directives or of the health care surrogate’s opinion on one hand and the level of ethical dilemmas on the other. The existence of differences in opinion within the health care team and the lack of information regarding the indication of the withdrawal of artificial nutrition were significantly associated with a higher level of ethical dilemmas in bivariate analysis but not in multivariate analysis (Table 3).
Factors Associated With Level of Ethical Difficulty When Withdrawing Artificial Nutrition.a
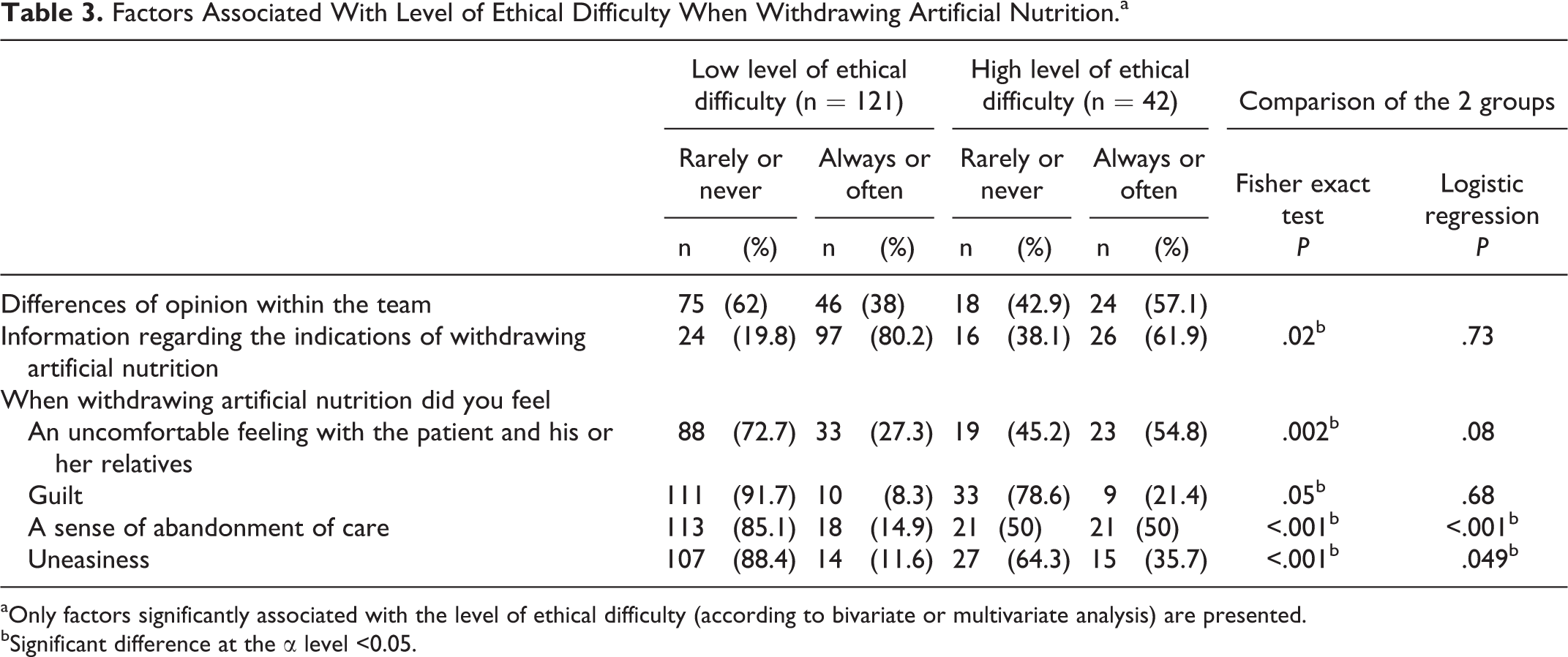
aOnly factors significantly associated with the level of ethical difficulty (according to bivariate or multivariate analysis) are presented.
bSignificant difference at the α level <0.05.
Among the feelings experienced by care providers when withdrawing artificial nutrition, the uncomfortable feeling with the patient and his or her relatives, guilt, the sense of abandonment of care, and uneasiness were significantly associated with a high level of ethical dilemmas in bivariate analysis, whereas only the sense of abandonment of care and uneasiness were significantly different in multivariate analysis.
Discussion
Among the health care providers confronted with withdrawing artificial nutrition, more than a quarter reported a high level of ethical dilemmas. The circumstances in which artificial nutrition was withdrawn did not appear to influence the level of ethical dilemmas, while, among the feelings experienced by the care providers, the sense of uneasiness and abandonment of care were most often reported in the group with a high level of ethical dilemmas.
This result is in keeping with the literature data in which withdrawing artificial nutrition is one of the most important ethical dilemmas in palliative care and is likely to affect the daily management of the patient. 17,24 A study 16 published in 2000 reported that withdrawing artificial nutrition was discussed for a quarter of the 246 patients followed.
Although the result was not significant, care providers with more than 10 years experience tended to have a higher level of ethical dilemma. This may be explained by their lack of training, given that specific palliative care training was only implemented in France in the past decade.
We observed less ethical dilemmas for care providers working in palliative care departments, although the difference was not significant and the small number of care providers in palliative care reduced the power of the analysis. This can be explained by a more regular practice of team discussion, multidisciplinarity being at the core of palliative care.
Although a multidisciplinary approach is not systematic, it is required by the French law of April 22, 2005, with regard to the withholding or withdrawing of treatments, and differences in opinion are common. Our study also highlights the lack of information for health care providers with regard to the indications of the withdrawal of artificial nutrition in palliative care. Care providers expressed a clear need for training and awareness of care providers regarding clinical guidelines on artificial nutrition at the end of life and on advantages and disadvantages of providing artificial nutrition in palliative care 26 appeared essential.
Care providers perceived more difficulties in obtaining the patient’s consent than in studying advance health directives or questioning the health care surrogate. The law of April 22, 2005 on the patients’ rights and end of life in France allows a patient informed of the consequences of his or her decision to ask for the cessation of any treatment including artificial nutrition and hydration. The law requires the physician to agree to the patient’s request if it is repeated and informed. If the patient is unable to give his opinion and if the withdrawal of artificial nutrition or hydration is considered, the law requires the physician to acquaint himself or herself with the advance health directives if they were prepared by the patient or to consult with the patient’s health care surrogate or relatives. These different points of view should help the medical decision, the aim being to know what the patient would have wished. In our study, only a quarter of the care providers mentioned collecting the directives of the patient, while two-thirds reported the collection of advance health directives or a discussion with the health care surrogate. Although these data could be explained by an alteration in the patient’s consciousness causing communication disorders, it is also possible that the opinion of the patient’s relatives prevails over the patient’s own opinion, which seems detrimental to the quality of care.
A study 23 published in 2008 focused on 2 aspects of artificial hydration in patients with cancer in palliative care: first, the perception of nurses with regard to the decision-making process and, second, his or her distress. More than half of the nurses stated that preliminary discussions surrounding the withdrawal of hydration were insufficient. These data are in keeping with the present findings insofar as to the lack of multidisciplinary discussion or the collection of the patient’s opinion when withdrawing artificial nutrition is concerned.
The uncomfortable feeling with the patient and his or her relatives and the lack of dialogue and consultation were frequently experienced by the care providers interviewed. These data are similar to those of a literature review on the stress of palliative care teams 22 which highlighted among the sources of stress at work (1) the difficulties in team communication and (2) communication difficulties with the patient and his or her relatives. The experience of health care providers could be improved in a first instance by appropriate organizational measures and in a second instance with external intervention such as supervision. The above-mentioned review also mentioned young age as a predisposing factor to stress and burnout in palliative care. In the present study, we were unable to demonstrate a link between seniority and the level of ethical dilemmas, although the comparison of data is difficult, especially since having low seniority is not necessarily synonymous with young age, as some care providers begin their career at a later age.
The feeling of abandonment of care, although experienced by only a quarter of the surveyed care providers, was 1 of the only 2 variables associated with the high level of ethical dilemmas. Among the 6 categories of motivations described in a study of teams treating dying patients, 27 intellectual appeal and the desire for control and mastery over illness, pain, and death were the most prominent. This may explain why the feeling of abandonment of care was associated with a high level of ethical dilemmas, in the present study. Indeed, the care providers who feel they abandon care when they withdraw artificial nutrition may feel to be out of touch of their professional mission and feel fundamentally affected in their motivation to work.
Among the potential sources of ethical conflicts at the end of life is sedation for intractable distress in terminally ill patients. One study reported that the family’s stress level was associated, among other factors, with the lack of compassion of physicians and nurses. 28 Herein, we observed that the stress level of care providers confronted with the withdrawal of artificial nutrition was associated with the feeling of abandonment of care and the sense of uneasiness. Although the situations considered in these 2 studies (sedation and artificial nutrition) and the studied populations (care providers and families) differ, it does appear that their respective results overlap in that when they feel that the patient is not properly surrounded, and care providers and relatives are in greater difficulty.
Our study has several limitations. The response rate was limited (33.5%) although still satisfactory for this type of study. A response bias may be suspected: the health care providers who are most concerned with the withdrawal of artificial nutrition in palliative care, and therefore mostly inclined to answer the questionnaire, are the most likely to have concerns with this issue. As a result, the rate of care providers describing ethical dilemmas could be overestimated. Nonetheless, the use of a self-administered questionnaire with anonymous responses enables to reduce the social desirability bias whose effect would have raised the issue of underreporting of perceived concerns.
The number of respondents stemming from the numerous departments and the various sites of the regional hospital is a strongpoint of this study. The results are thereby representative of the health care providers of the region. However, the perception of the withdrawal of artificial nutrition is influenced by cultural context, and our results cannot easily be extrapolated to other regions or countries.
Conclusion
More than a quarter of the care providers confronted with withdrawing artificial nutrition reported a high level of ethical dilemmas (42 of 163). Care providers seemed to have a lack of information and consensus regarding the withdrawal of artificial nutrition at the end of life. Although the circumstances of the withdrawal did not appear to influence the level of ethical dilemmas, care providers with a high level of ethical dilemmas often experienced a sense of uneasiness and abandonment of care. One means to improve the ethical perception of the withdrawal of artificial nutrition may be to work on our limitations as care providers and on the acceptance of a certain degree of helplessness (in the context of end of life, when faced with patients at end of life).
Footnotes
Acknowledgment
We thanks Mr Pierre Pothier for English review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.