
Abstract
Increasingly clinicians are using palliative care to address the symptomatic and psychosocial effects of disease often missed by routine clinical care, termed “early” palliative care. Within an inner-city medical center, we began a program to integrate early palliative care into HIV inpatient care. Patient symptom burden and desired services were assessed and compared to provider perceptions of patient’s needs. From 2010-2012, 10 patients, with a median CD4+ T-cell count of 32.5 cells/μL, and 34 providers completed the survey. Providers ranked their patients’ fatigue, sadness, anxiety, sexual dysfunction, and body image significantly higher than patients it for themselves. Patients ranked medical care, pharmacy, social work, physical therapy, and housing as significantly more important to them than providers estimated them to be. These differences may reflect the fact that physicians often overlook patients’ unmet basic needs. Early palliative care may narrow this gap between providers’ and patients’ perceptions of needs through good communication and targeting barriers, such as housing instability, which are vital to overcome for consistent long-term follow up.
Keywords
Introduction
The earlier integration of palliative care services (PCSs) into chronic disease management has become increasingly more common over the last several years. This movement began shortly after the World Health Organization first proposed this new model in 1990. 1 This same early PCS model was recommended specifically for diseases such as HIV/AIDS in their 2004 Bulletin on Palliative Care. 2 Joint United Nations Programme on HIV/AIDS (UNAIDS) also emphasized this approach while attempting to clarify the misconceptions that PCSs were limited to hospice care. The UNAIDS definition stated that palliative care (PC) “is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life.” 3 A seminal study by Temel et al in 2010 involving early PC in nonsmall cell lung cancer demonstrated enhanced quality of life, decreased hospitalizations, and prolonged survival. 4 While PC has been traditionally associated with cancer care, practitioners who provide care for patients with a variety of chronic diseases have begun to utilize PCS in conjunction with etiology-specific treatment. 5 –8
Undoubtedly combination antiretroviral therapy (cART) is the cornerstone of HIV care; however, the associated psychosocial challenges, spiritual concerns, and high symptom burden associated with HIV disease cannot be underestimated and must be addressed in order to optimize care. 9,10 If these issues are not adequately addressed during initial visits with a patient, the likelihood of establishing an effective relationship with the provider declines considerably. 11 Given that certain regions of the United States are failing to effectively contain the HIV epidemic, innovative strategies to improve linkage and retention in care are desperately needed. Integrating PCS to the initial care of patients with HIV offers a way to improve quality of life, strengthen adherence to treatment, promote trust within the patient–provider relationship, and increase life expectancy. 9
In 2010, we began a program to integrate early PCS into routine HIV inpatient care at an inner-city hospital with a substantial annual HIV admission rate. This study was conducted within Grady Memorial Hospital (GMH), which is the primary safety net hospital for the Atlanta metropolitan area. 12 Atlanta has one of the largest HIV populations in the United States. From 2001 to 2010, approximately 100 patients per year were newly diagnosed with HIV during an inpatient hospitalization at GMH with the median CD4+ T-lymphocyte count of 50 cells/µL at time of diagnosis (data not shown). Additionally, patients with HIV accounted for over 2000 admissions per year at GMH. About half of these patients receive care at the Infectious Disease Program (IDP) of the Grady Health System (GHS), which sees over 5500 patients for HIV primary care and advanced HIV disease. 12 In the inpatient wards of GMH, it is not uncommon to have patients with Pneumocystis, Cryptococcal meningitis, or many other opportunistic infections. A survey was administered to interested patients in order to assess the potential impact of this early PCS program through the assessment of patient symptom burden and desired services. These results were then compared to medical provider perceptions of patient symptom burden and desired services.
Methods
Enrollment and Data Collection
Eligible patients were referred by their primary hospital team, the Infectious Diseases consult service, or the HIV social work service. The inclusion criteria included a CD4 T-cell count less than 200 cells/μL and one of the following: known HIV diagnosis with fewer than 1 follow-up visit at IDP per year or no previous history of outpatient HIV care, or a new HIV diagnosis within the prior 6 months. All patients were older than 18 years of age and capable of giving informed consent. Pursuant to the definition of early PCS, those individuals eligible for hospice care were excluded from the survey (Table 1). These criteria were based on previously published hospice guidelines. 13 Providers of the patients who were eligible for hospice were encouraged to consult PC to explore hospice services. Other exclusion criteria included ineligibility for IDP enrollment, a migratory lifestyle, or an inability to provide consent.
Individuals With HIV Who Were Eligible for Hospice.
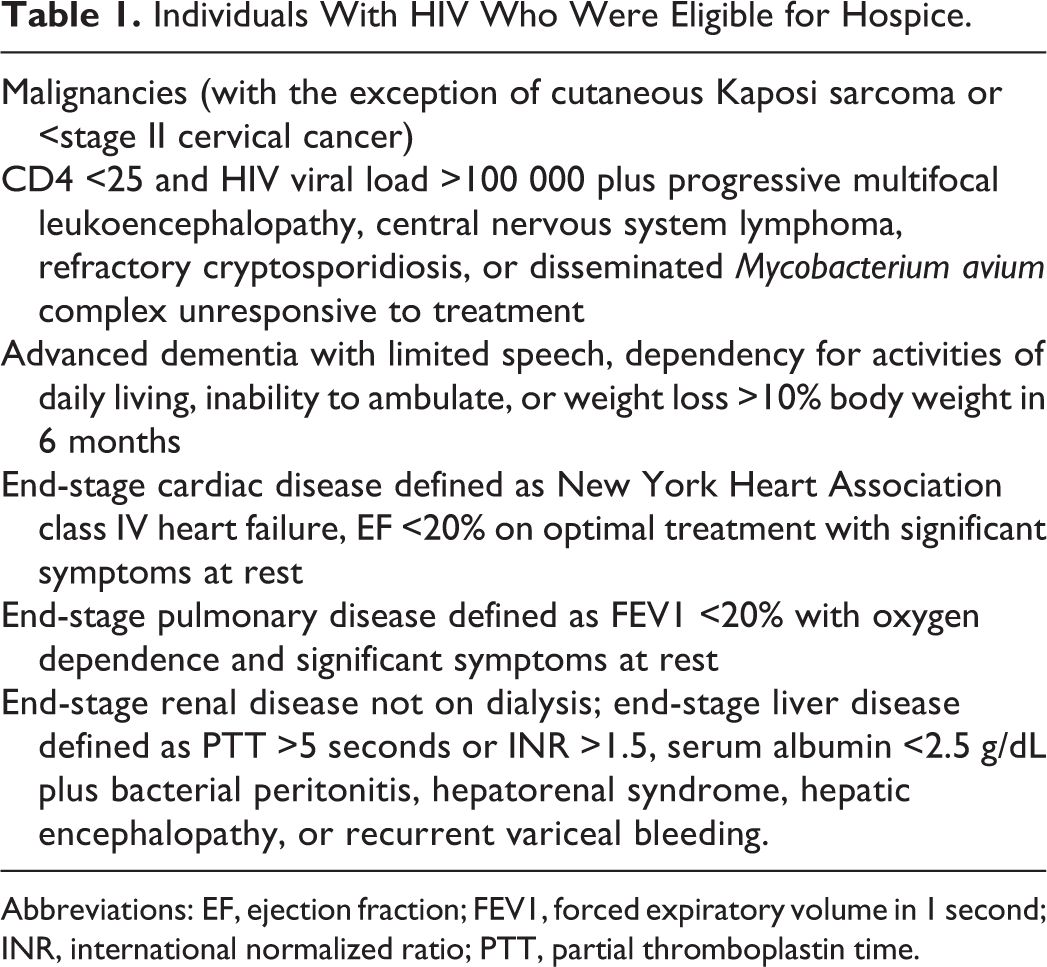
Abbreviations: EF, ejection fraction; FEV1, forced expiratory volume in 1 second; INR, international normalized ratio; PTT, partial thromboplastin time.
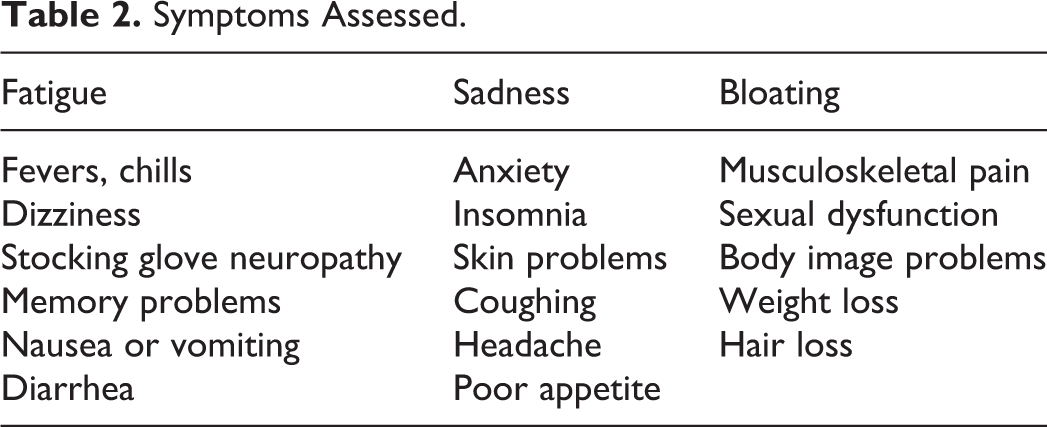
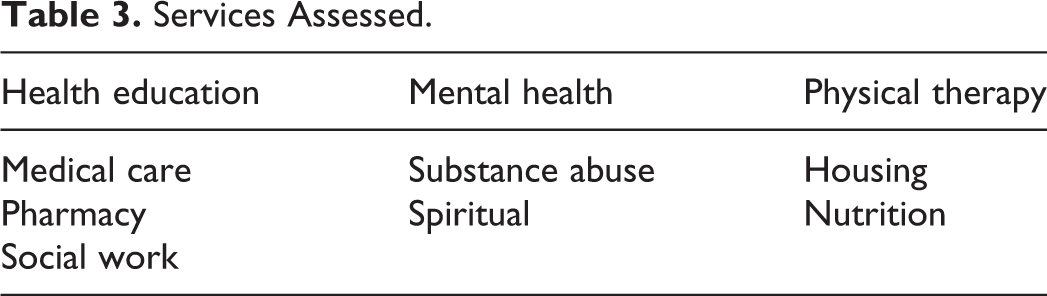
After obtaining informed consent, patients were enrolled and the survey was conducted by one of the study physicians. All participants also underwent an inpatient PC consultation. The study questionnaire included perceived symptom burden and needed services as detailed in Tables 2 and 3 (instruments in supplemental material). Additionally, outpatient and inpatient providers within the GHS were given written, self-administered questionnaires assessing their perceptions of the average symptom burden and need for services of a patient with HIV. Certain aspects of the provider questionnaire were designed to mirror the patient questionnaire. The symptoms were ranked using a Likert-type scale (0-4). A rank of zero indicated that the patient had not had the symptom in the past 4 weeks. A rank of 1 to 4 indicated that the patient had the specified symptom in the past 4 weeks but it (1) did not bother the patient, (2) bothered patient a little, (3) bothered the patient a lot, or (4) bothered the patient terribly. The patients answered for themselves and the providers were asked to imagine a typical nonterminal patient with HIV having a CD4 count less than 200 cells/mm3.
Symptoms Assessed.
Services Assessed.
Statistical Analysis
Descriptive statistics required Student t tests for continuous variable comparisons and P values of .05 or greater were considered significant. The data were analyzed using Microsoft Excel (2010 Microsoft Corporation, Redmond, WA, USA).
Ethics
The study was approved by the Emory University institutional review board and the Grady Research Oversight Committee. All study participants provided written informed consent.
Results
Between 2010 and 2012, 15 patients were enrolled in the study. Of those, 10 participants completed the survey giving a 67% completion rate from those enrolled (the others chose not to participate or were unable to fully complete the survey due to a deteriorating clinical condition). The median age of those who completed the survey was 37 years, 92% were male, and the median CD4 count (interquartile range) was 32.5 (5-52) cells/µL. Four were recently diagnosed with HIV (diagnosis within the last 6 months).
There were 34 providers who participated in the survey. Of these, 5 were faculty physicians in the Department of Medicine, 12 in the Division of Infectious Disease and working regularly in a HIV clinic (6 fellows in Infectious Diseases and 6 physician assistants or advance practice nurse practitioners), and 17 were internal medicine residents.
Symptom Assessment
Figure 1 shows the percentage of participants and providers reporting any symptoms (ie, 100% indicates all patients reported the symptom and 0% indicates no patient reported the symptom). We found providers reported symptoms more frequently than patients in all categories. For example, 97% of providers thought sexual problems would be present though only 30% of patients reported them. Other symptoms, such as pain, were more equally identified by providers and patients (91% and 90%, respectively).
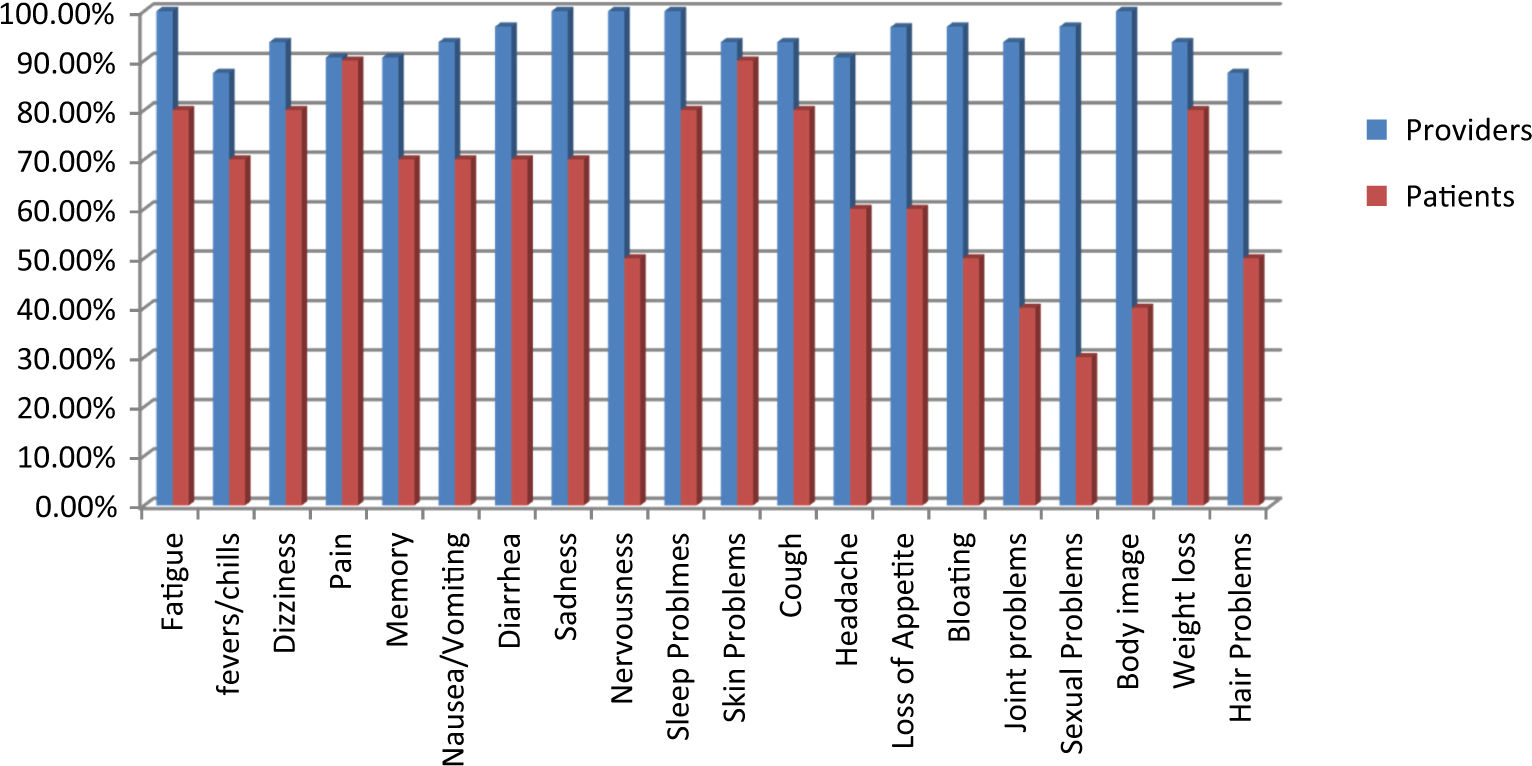
Frequency distribution of patients and providers reporting symptoms.
Figure 2 shows a comparison of the rankings of different symptoms as reported by patients and providers. Overall, providers generally perceived that patients had higher symptom burdens than patients reported. The only symptoms that were ranked higher by patients than providers were dizziness, neuropathy, skin problems, and cough.
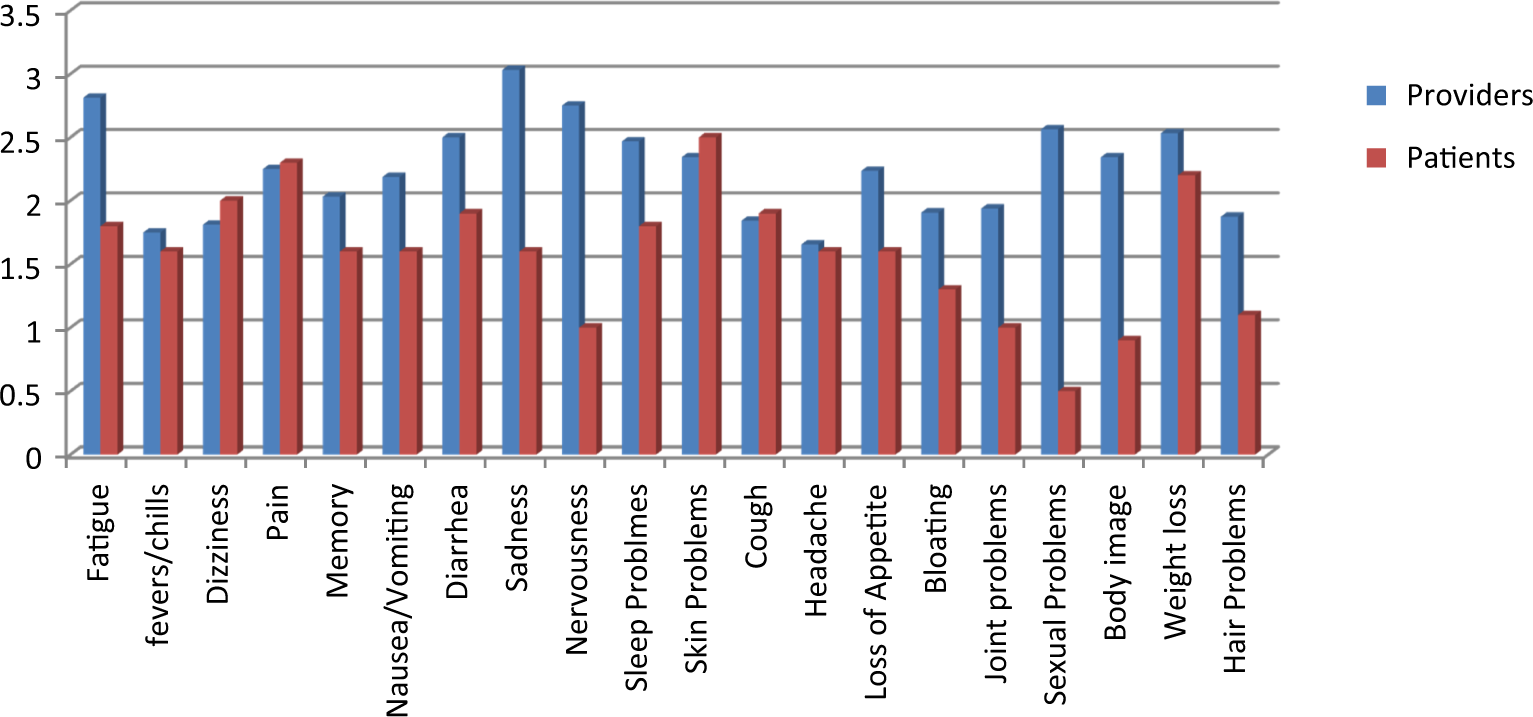
Comparison of patient and provider perceptions of symptoms ranking.
The symptoms ranked significantly differently between patients and providers were fatigue, sadness, anxiety, sexual dysfunction, and problems with body image (Table 4). For each of these symptoms, the providers had higher scores than the patients.
Symptom Rankings Showing Statistical Significance Between Providers and Participants.
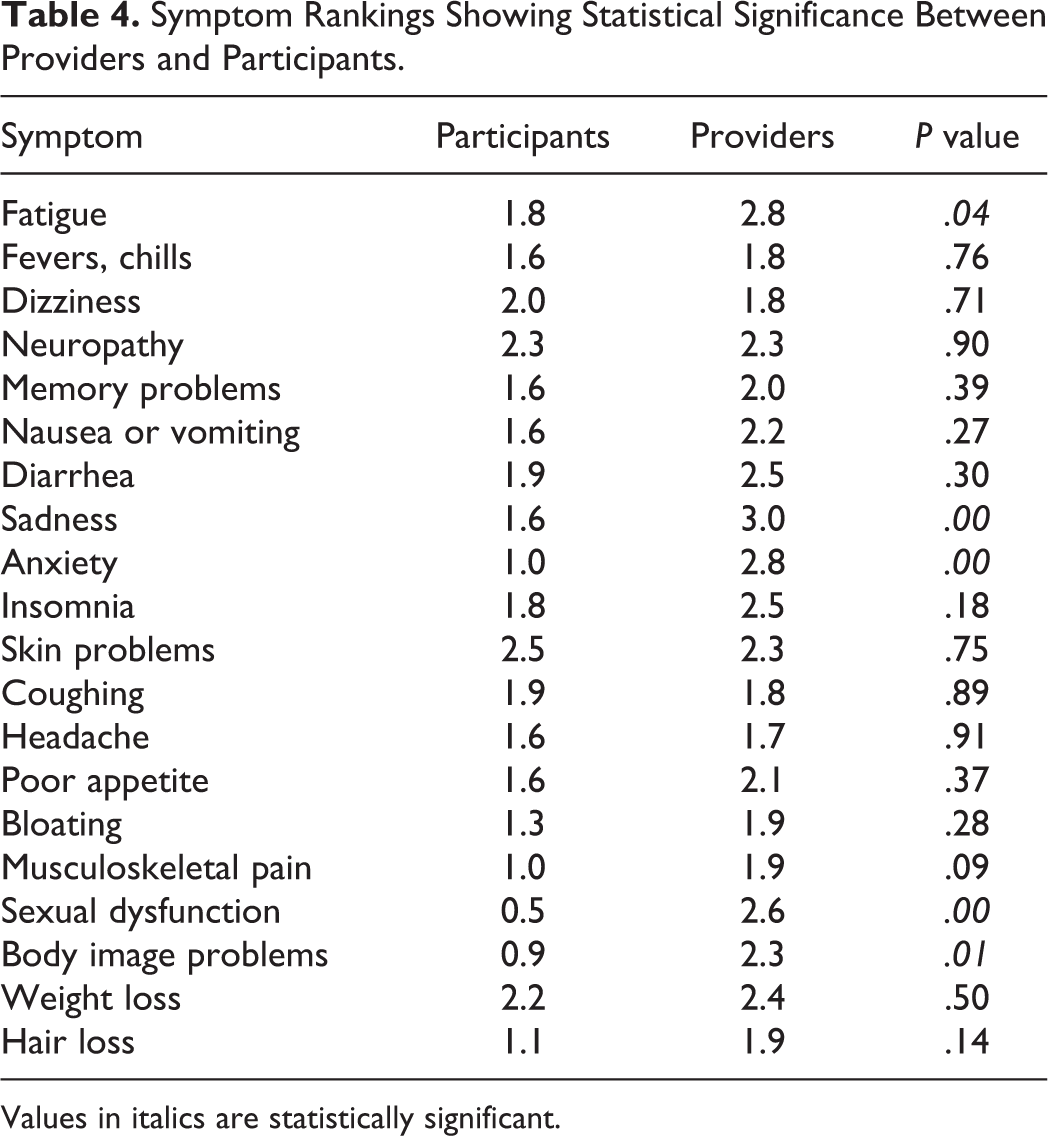
Values in italics are statistically significant.
Services
Figure 3 shows the comparison of perceived services needs between patients and providers. From these data, it appears that patient needs were generally greater than those perceived by providers. Substance abuse services were the only services providers ranked higher than patients in their perception of need.
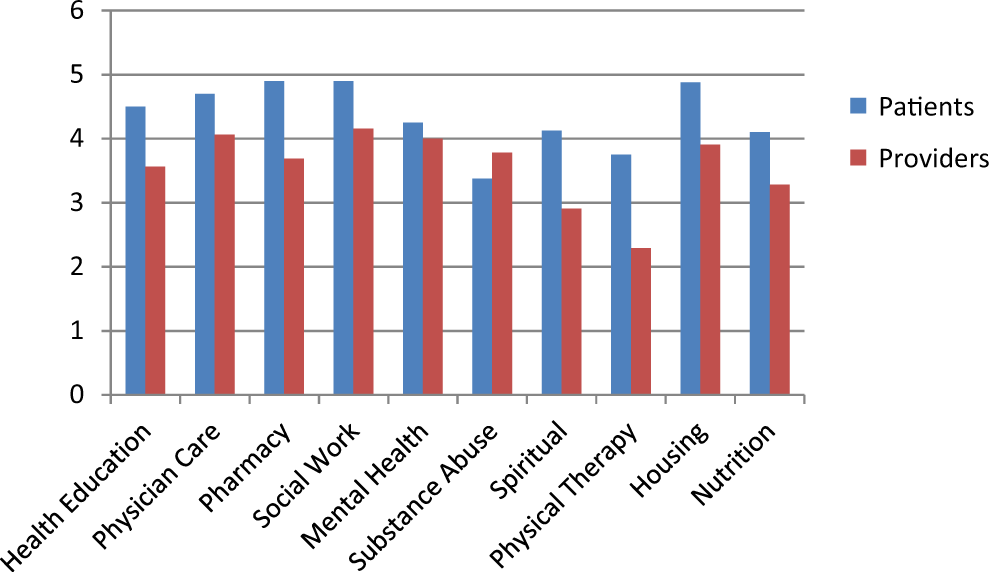
Comparison of patient and provider perceptions of needed services.
The service needs that differ significantly (<0.05) are medical care, pharmacy, social work, physical therapy, and housing. Patient scores were higher than the provider scores for each of these (Table 5).
Need for Service Rankings Showing Statistical Significance Between Providers and Patients.
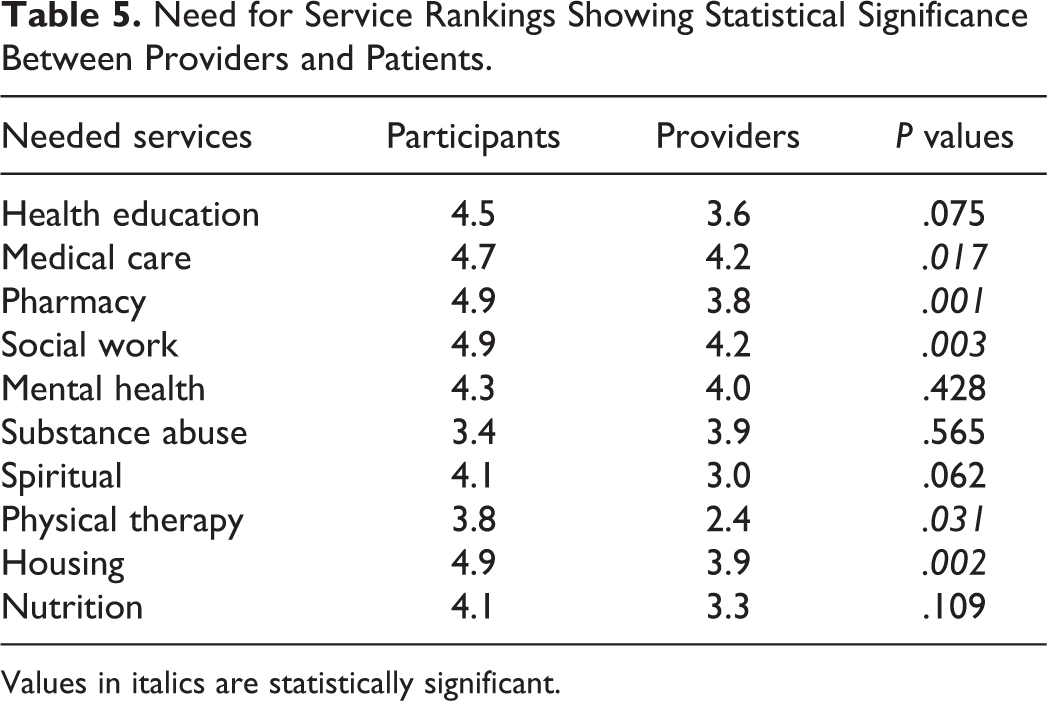
Values in italics are statistically significant.
Discussion
We report results from a survey that examined the perception of symptom burden and needed services for patients with HIV from both the patient and provider perspectives. The statistically significant differences in reported symptoms include fatigue, sadness, anxiety, sexual dysfunction, and problems with body image, all of which providers estimated to be higher. Fontaine et al also examined symptom burden of patients with HIV. 14 The percentages of inpatients reporting symptoms were similar to our percentages for fatigue (77% vs 80%), anxiety (64% vs 50%), depression (63% vs 70%), and lack of appetite (55% vs 60%) for patients in the Fontaine study compared to the present study, respectively. More participants in our study had skin problems (37% vs 90%), sleep problems (62% vs 80%), cough (57% vs 80%), diarrhea (45% vs 70%), and nausea (48% vs 70%) again for patients in the Fontaine study compared to the present study, respectively. However, Fontaine et al found that patients reported a higher symptom burden than providers. It is unclear why we found the opposite effect. In the Fontaine study, the providers interviewed directly cared for the patients, which was not the case for our study. Providers may be more likely to report symptoms in general than for a specific patient. Only 81% of their patients had a CD4 count less than 200 cells/μL, compared to 100% of our patients, which could explain why our patients reported a higher symptom burden. An exception to this trend was psychological symptoms, which might be more evident when fewer medical symptoms are present.
Interestingly, providers perceived a higher symptom burden but a lower need for services, which was statistically significant for several factors. Significant differences in services were found in medical care, pharmacy services, social work, physical therapy, and housing. The differences in these symptoms and services may reflect the fact that providers often do not recognize the depth of poverty experienced by their patients. 15 When patients struggle with basic needs such as housing, these ultimately take precedence over psychological concerns which providers more often perceive their patients would have. An outpatient study done in 1995 before cART was widely available and surveyed patients, providers, friends, or family members of individuals living with HIV, as well as members of the general public in order to determine what services were needed most. 16 This study found that medical care was the most important service to all surveyed. Our patients also reported medical care, as among the most important service. It is possible that patients living in poverty lack basic resources and naturally prioritize more immediate needs such as housing. Although cART and other medical therapies are available to our patients free of cost, patients still perceived a significantly higher need for medical care than did the providers. This could reflect poverty and inadequate transportation limiting access to medical treatment, despite verbalizing a desire for it.
Pellowski et al describe how poverty complicates treatment for those who have HIV. 17 Those in poverty often have lower health literacy, poor access to medical care, and higher relationship instability. Although socioeconomic disparities are most chronic diseases, HIV almost exclusively affects those with the lowest socioeconomic status. Some of the practical manifestations of poverty worsen the outcomes for patients living with HIV. For example, food insecurity when combined with a low BMI can predict mortality over and above medication adherence. Additionally, sexual trauma, which can predate HIV infection, may precipitate mental health and substance use disorders subsequently reducing adherence to HIV treatment.
Despite continual advances in cART, there remains a vulnerable subset of people living with HIV who have multiple medical and psychosocial comorbidities that detract from their ability to effectively engage in and remain in care. Our patient population reflects such a vulnerable population. A retrospective chart review of a similar HIV population in Toronto, Canada, 18 found that patients experienced a mean of 5.9 medical and 1.9 psychiatric comorbidities. More strikingly, 8.4% of those patients had unstable housing in addition to 3 or more medical comorbidities and 2 or more psychiatric comorbidities (including substance abuse). These issues need to be addressed comprehensively in vulnerable HIV populations. Early integration of PCS may offer a way to do so effectively, using good communication and identification of goals of care. The use of an integrated approach might connect patients with resources that are available to them as an outpatient, yet keep them from connecting with the outpatient center that houses these resources such as transportation, child care, and housing. Palliative care could also assess psychological concerns such as depression or schizophrenia, which may interfere with patient motivation and organization needed to remain in outpatient care.
Ideally patients selected for our study would be identified “earlier” in their HIV disease course (closer to when they are infected and diagnosed with HIV) for early PCS to be initiated. The patients in our study had very low CD4 T-cell counts (ranging 5-52 cells/µL) and were already at significant risk of morbidity and mortality due to opportunistic infections and medical complications that would only be compounded by psychosocial factors. If possible we would have selected these patients earlier when they had CD4 counts in the 300 to 400 cells/μL range in order to avoid AIDS-related complications. The advanced stage of HIV found in our referred patients suggested that referring providers consider PC to be more effective in an end-of-life context than for chronic disease management. This implies that more education about the benefits of early PCS may be needed within our own institution. Recognizing these deficiencies and developing subsequent interventions were the goals of this work.
There are a few limitations of our study design. The first is a relatively small sample size. We were also surveying hospitalized patients with AIDS, very low CD4 counts, and high rates of poverty, which can affect generalizability. We surveyed providers (not necessarily those who referred patients) in the same health system as the patients but their average patient may have less advanced HIV than these patients. The symptoms experienced by patients may be different depending on the degree of HIV disease progression (ie, a patient with a CD4 count of 30 might report less sexual symptoms than a patient with a higher CD4).
Conclusion
Individuals living with HIV reported a high symptom burden and a multitude of services needed. This study looked at the differences in perceptions of symptoms and services between patients and providers. Both patients and providers perceived many symptoms and many services needed but differed on specific symptoms and services. These differences appear to reflect the fact that patients focused on needs for basic necessities such as housing while providers focused more on treatment-focused needs. Ultimately, these findings demonstrate a divide between patient needs and the services provided by the health care system. Early PCS offers a way to meet these unmet needs using effective communication and goals of care, and these data provide targets for care and services.
Footnotes
Acknowledgments
First, we thank all our patients at Grady for their support and participation in this study. We also thank the providers who completed our surveys and serve the patients of Grady every day. Next, we thank everyone who helped with the study design and implementation of it. We also thank everyone who helped with the interpretation of data, writing, and editing of this work.
Authors’ Note
This work has not been presented orally.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Emory University Center for AIDS Research (CFAR; P30AI050409) and the Emory University School of Medicine Division of Infectious Diseases.