
Abstract
Context:
Approximately 1 in 10 infants require neonatal intensive care unit (NICU) hospitalization, which causes parental stress. Palliative care (PC) provides an opportunity to alleviate suffering and stress.
Objectives:
This study examines the effects of PC on NICU parent stress and satisfaction.
Methods:
A prospective cohort design compares stress and satisfaction among families receiving or not receiving PC.
Results:
No significant differences in stress scores were found (P = .27-1.00). Palliative care parents (100%) were more likely to report being “extremely satisfied” with care than usual-care parents (50%).
Conclusion:
This study supports the feasibility of evaluating NICU PC services. Infants referred for PC typically have higher morbidity/mortality; therefore, higher parental stress scores may be expected. Stress levels were similar in both cohorts, thus PC did not increase stress and may decrease PC parent stress.
Introduction
Approximately 1 in 10 infants in the United States require admission to a neonatal intensive care unit (NICU) due to illness or prematurity. 1,2 Hospitalization of one’s infant results in substantial physical, emotional, and mental stress and can lead to decreased bonding and poor future outcomes including developmental delays, behavior problems, and an increased risk of child abuse. 3 –13 New approaches to reduce NICU parent stress are needed to improve life-long outcomes for individuals, families, and society at large.
Palliative care (PC) is patient/family-centered care that focuses on relieving symptoms, suffering, and stress that accompany serious illness. This approach addresses physical well-being but also aims to improve social, spiritual, and psychological well-being for the patient and family. Research outside the NICU suggests PC decreases costs and improves quality of life for patients/families. 14 –20 There is increasing interest in integrating PC into the NICU, yet little empiric PC outcomes research in this setting has been reported. This study aims to examine the effects of PC on NICU parent stress and satisfaction.
Methods
Study Design and Population
This prospective, convenience sampling, cohort design compares stress and satisfaction scores of NICU parents who received PC services with those who did not. Physician orders for PC services were based on hospital policy (birth gestational age 28 weeks or less, known/suspected congenital/chromosomal anomalies, and coordination of multidisciplinary support). Parents of infants with an anticipated NICU stay greater than 2 weeks were eligible to participate. The NICU PC service at this institution included 1 advanced practice nurse and 1 bachelors prepared RN with extensive NICU experience both thoroughly trained and educated in PC; additional medical support was available to the nurses as needed. The PC nurses provided important continuity of care for NICU infants/families; all other NICU health care providers (except social workers) change/rotate during the course of the infant’s hospitalization. In addition to continuity of care, PC services included assessments (of both infants and parents), interdisciplinary collaboration and care coordination, and at least weekly verbal support of parents. The PC service also coordinated family conferences, provided or requested orders to improve infant symptom management and comfort, and addressed parental coping and self-care.
Medical center and university institutional review boards approved the study. Eligible parents were informed of the study; interested parents were consented. Study enrollment took place over 4 months (August-November 2012) in a large level III NICU with an established pediatric PC program in California.
Survey Content and Administration
Infant clinical information was collected via chart review. A questionnaire collected parental demographics and recent stressor exposure (death of family/friend, divorce/marriage, and job loss/change). The Parental Stress or Scale: NICU (PSS:NICU) and Stanford Acute Stress Reaction Questionnaire (SASRQ) measured stress scores at study enrollment, 2 weeks later, and at discharge. The PSS:NICU, a validated 26-item Likert-type scale, measures stress via 3 subscales (NICU environment, infant behaviors/appearance, and alterations in parental role experiences). 21 Total scores and individual subscale scores are reported. The SASRQ, a validated 30-item Likert-type scale, measures dissociation, peritraumatic anxiety, and presence of diagnostic symptoms of acute stress disorder (ASD) including avoidance, dissociation, anxiety/hyperarousal, functional impairment, and re-experiencing of trauma in regard to a specific event 22 operationalized in this study as the infant’s NICU hospitalization. Parental satisfaction with care was measured once at discharge (or study closure for infants who remained hospitalized) via a researcher-created tool based on extensive current literature review. 23 –26 This single-item, 4-point (extremely dissatisfied to extremely satisfied) Likert-type scale allowed parents to provide feedback regarding overall satisfaction with care received. An opportunity to provide free-text description of specific experiences impacting satisfaction with care was available but not required. Face and content validity was established by methods articulated by Polit and Beck 27 and through rigorous review by multiple NICU and PC experts (neonatologist, social worker, clinical nurse specialist, and PC nurse practitioner) and previous NICU parents.
Data Analysis
Measures of central tendency (frequencies, means, and standard deviations [SDs]) described parental demographics and infant clinical attributes. Because data were not normally distributed, nonparametric methods compared stress and satisfaction scores between cohorts. Analysis was completed in SPSS Version 19.
Results
In all, 66 parents were eligible to participate, 33 (23 usual care [UC] and 10 PC) consented (50% response rate). However, only 22 (16 UC and 6 PC) parents had complete baseline data for analysis. Sample numbers decline at subsequent intervals due to attrition, death, and unanticipated infant discharge (Figure 1). Parent’s mean age was 30 years (range 19-47, SD 7.9). Baseline parental demographics and stressors did not statistically differ between cohorts (Table 1). Mean infant birth weight was 1745 g (3 lb 13 oz); birth weight ranged from 572 to 3560 g (1 lb 4 oz-7 lb 13 oz). Mean birth gestational age was 31 weeks (range 25-40, SD 4). Length of NICU stay ranged from 13 to 85 days (mean 44.6, SD 22.7); at study completion, 5 infants remained hospitalized. Two infants died during the study, both from the PC cohort (Table 2).
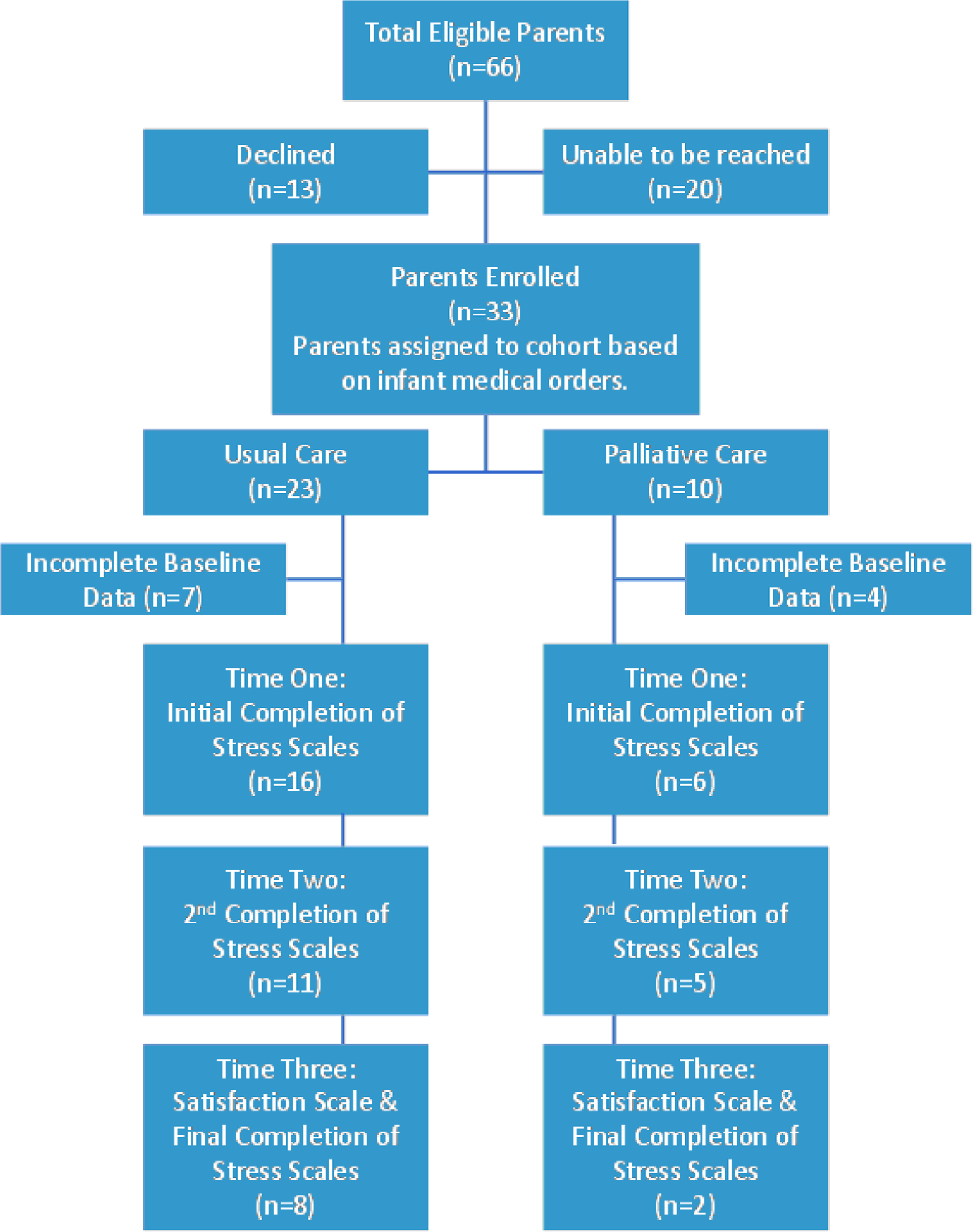
Flow chart of parent eligibility and participation.
Demographic Characteristics of Parent Participants.a
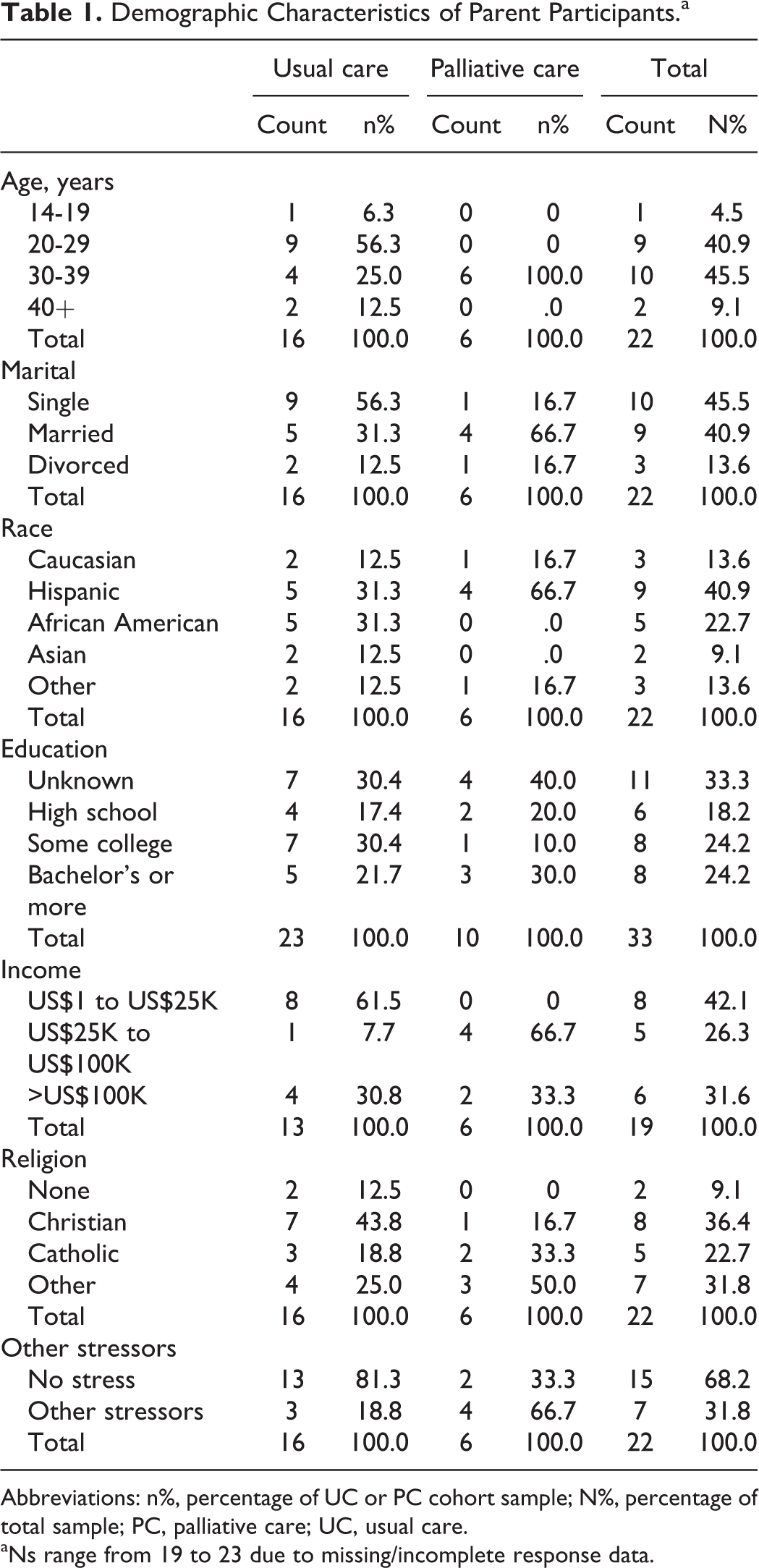
Abbreviations: n%, percentage of UC or PC cohort sample; N%, percentage of total sample; PC, palliative care; UC, usual care.
aNs range from 19 to 23 due to missing/incomplete response data.
Clinical Characteristics of Infants.
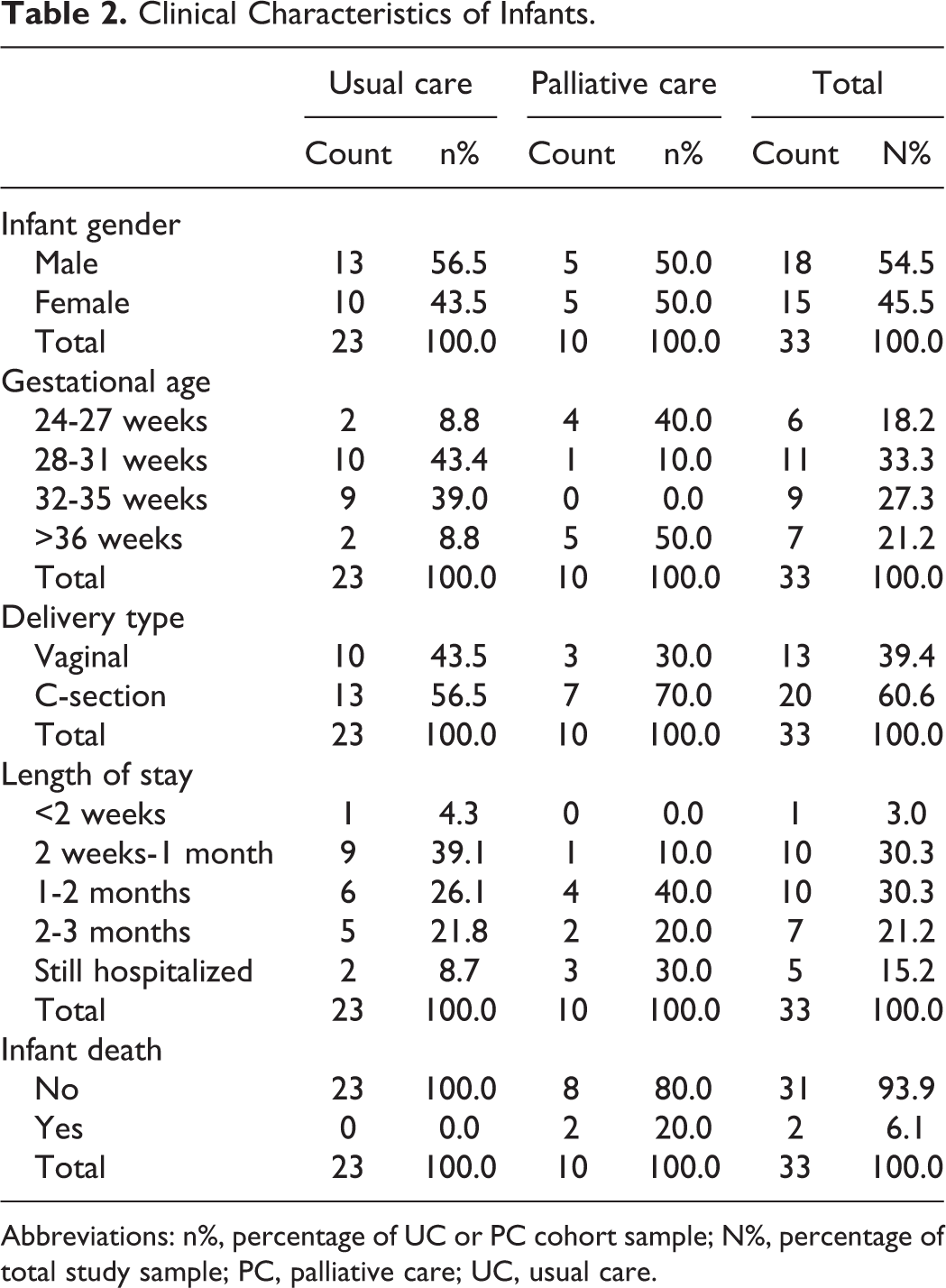
Abbreviations: n%, percentage of UC or PC cohort sample; N%, percentage of total study sample; PC, palliative care; UC, usual care.
No statistically significant differences (P = .267-1.000) were found in stress scores between cohorts (Tables 3 and 4). Total PSS:NICU scores suggest parents find NICU hospitalization at least moderately stressful (mean PSS:NICU score approaching or above 3). 21 Examination of PSS:NICU subscales shows the majority of stress for both cohorts results from alterations in parental role experiences. Of the total number of parents who completed SASRQ documents (n = 22), 14% (3 parents) met diagnostic criteria for ASD (2 UC and 1 PC). Additionally 4 parents, all from the UC cohort, were 1 criterion below ASD diagnosis (subclinical ASD); no PC parents exhibited subclinical ASD, which may indicate that PC helped to alleviate acute stress. Thus, 32% (n = 7) of participating parents (n = 22) approached or met diagnostic criteria for ASD at some time during the study, suggesting that stress is significant for NICU parents (Figure 2).
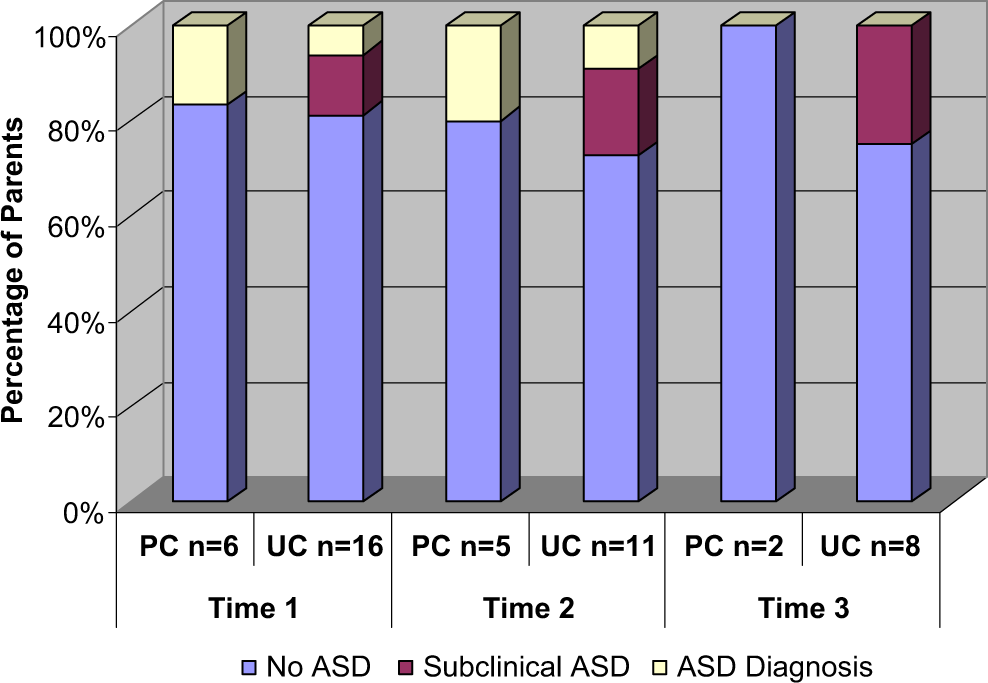
Incidence of acute stress disorder (ASD) diagnosis, subclinical ASD, and no ASD at each time interval for palliative care (PC) and usual care (UC) cohorts.
Parental Stress Scale:NICU Subscale and Total Score Means and P Values.a
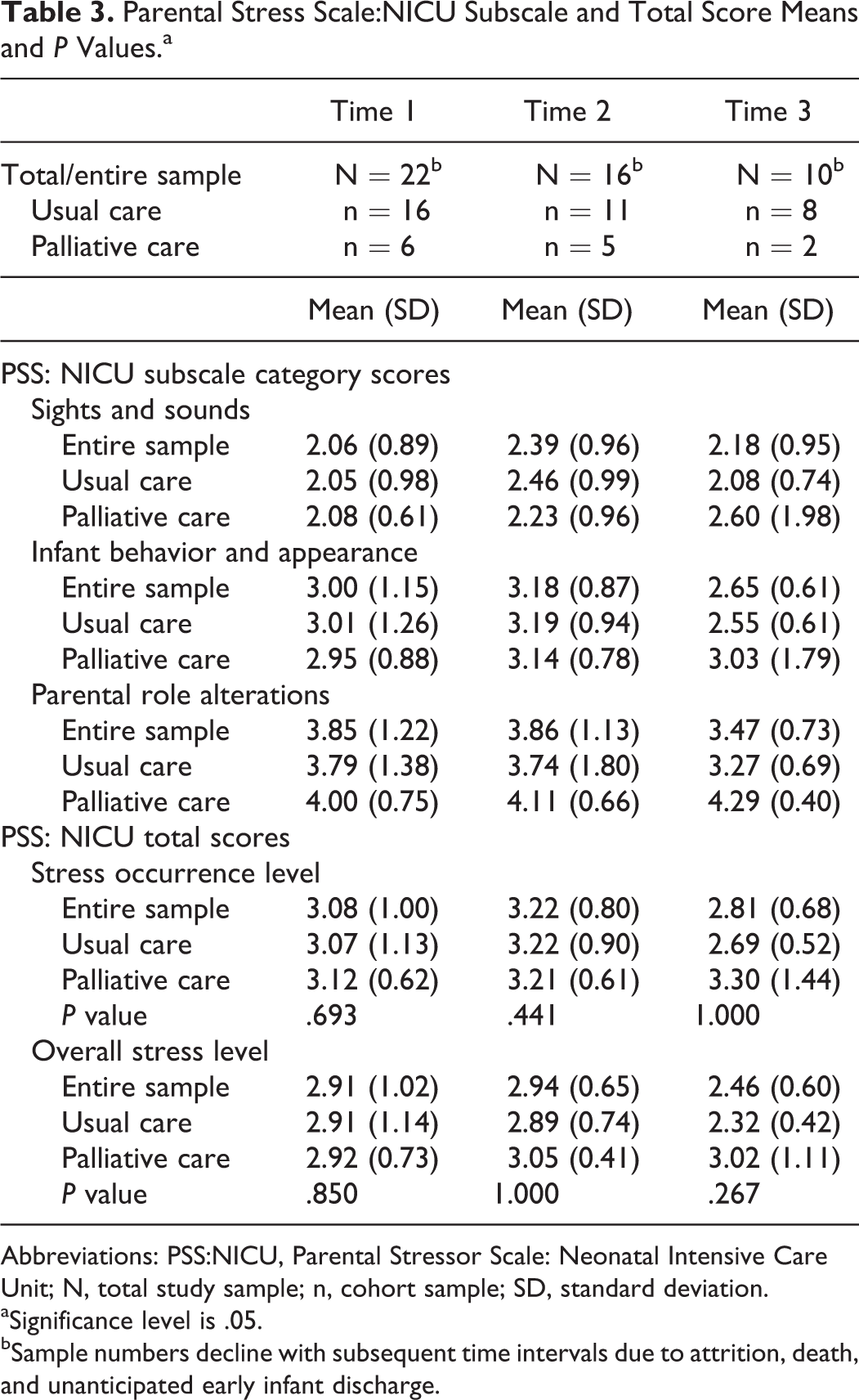
Abbreviations: PSS:NICU, Parental Stressor Scale: Neonatal Intensive Care Unit; N, total study sample; n, cohort sample; SD, standard deviation.
aSignificance level is .05.
bSample numbers decline with subsequent time intervals due to attrition, death, and unanticipated early infant discharge.
SASRQ Results: Number of Participants With Presence of ASD Diagnosis, Subclinical ASD, or No ASD; and P Values.a
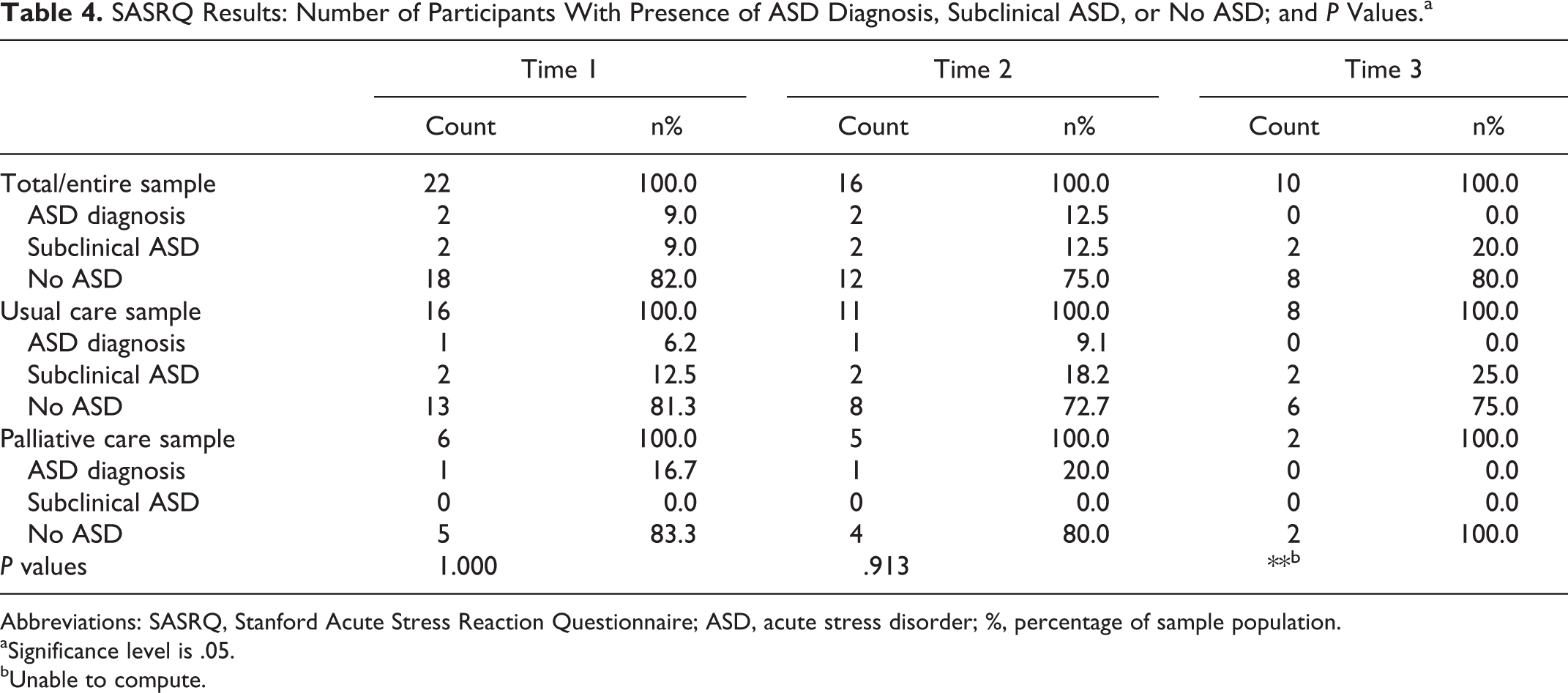
Abbreviations: SASRQ, Stanford Acute Stress Reaction Questionnaire; ASD, acute stress disorder; %, percentage of sample population.
aSignificance level is .05.
bUnable to compute.
Parent satisfaction response numbers were small (n = 10), thus statistical comparison of parental satisfaction between cohorts was not possible. However, 100% of responding PC parents (n = 2) reported being “extremely satisfied” with care, whereas only 50% of responding UC parents (n = 4) reported extreme satisfaction (Figure 3).
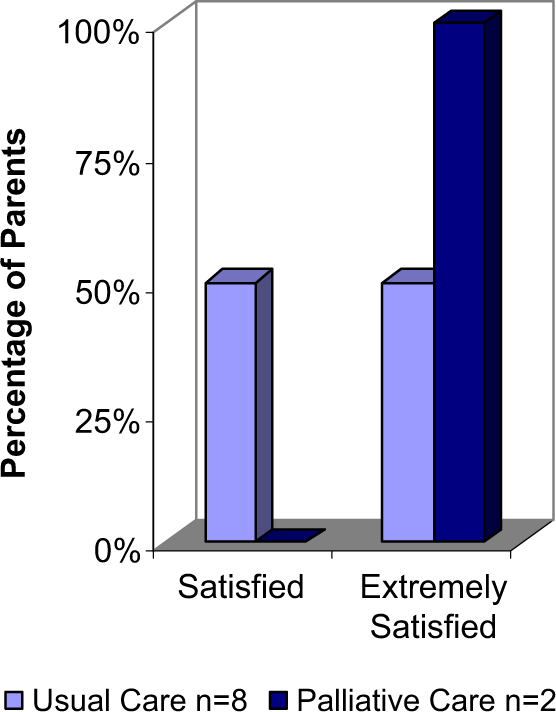
Satisfaction with care.
Discussion
This pilot study was undertaken to consider the feasibility of evaluating NICU PC services by comparing the influence of PC on NICU parent stress and satisfaction scores. When appraising our findings, it is important to consider that infants referred for PC tend to be more critically ill and have higher morbidity/mortality than other NICU infants; thus parents of PC infants may be more likely to have higher stress scores. However, stress levels in PC and UC cohorts were not significantly different at any time point. Although the small sample size precludes this analysis, the PC services provided may have lowered PC parent stress to a level similar to that of UC parents. Our findings show that PC services did not increase parent stress levels and may decrease stress in parents of the frailest, sickest infants.
Study results suggest that infant hospitalization is stressful for families, confirming previous research regarding NICU parent stress. 6,9 –11,28,29 One-third of the total participating sample met or nearly met ASD diagnosis, indicating that 1 in 3 NICU parents may have ASD/subclinical ASD. As this study employed convenience sampling, it must be noted that elevated stress may have contributed to parental decisions to decline study participation and to attrition. Thus, actual numbers of parents having ASD or subclinical ASD may be greater than 1 in 3. Similar to previous research, 21 results show the highest incidence of stress from alterations in parental role experiences. Results indicate that future interventions addressing parental role alterations may decrease stress significantly.
Parents whose infants received PC services were more likely to be “extremely satisfied” with care than parents whose infants did not receive PC, which is consistent with research in non-NICU populations that shows improved patient/family stress and satisfaction in response to PC. 14,17,18,30 In the era of health care reimbursement based on client satisfaction, this finding may have economic significance. Further research exploring the influence of PC on NICU parent satisfaction is warranted.
This research fills a void as minimal NICU outcomes-based PC research has been reported. We recognize a larger sample and randomized design would have significantly strengthened findings; however, this study was undertaken as part of a master’s thesis, thus there was limited time for enrollment and analysis. Nevertheless, this study breaks new ground by demonstrating the feasibility of completing an outcomes-based investigation of PC in an NICU. This study reflects the incredible challenges of recruitment and retention in NICU settings but also points to the potential of integrating PC for families facing infant morbidity and death. The short time frame available for data collection and single study location also limit study findings. Yet this site experiences over 1200 NICU admissions per year and has an average daily census of more than 60 infants. Additionally, this NICU utilizes a seasoned PC team that provides experience and credibility to the study. This study offers guidance in planning future NICU PC research.
Conclusion
The birth of a critically ill infant places an enormous burden on families. Palliative care approaches to family-centered care provide opportunities to address the suffering of infants and families facing these difficult circumstances. Future interventions to mitigate parent stress should incorporate methods to support NICU parenting experiences, foster parent–infant bonding, and improve parental self-confidence to positively impact individuals, families, and society as a whole. Additional quantitative and qualitative research is vital to understanding the effects of PC on stress, satisfaction, and other NICU outcomes.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank the NICU and PC staff for the excellent care they provide. We remember the infants who died and the families who experienced the loss of a loved one during the course of this study, and extend a special thanks to all families who participated. We hope that this study will encourage further NICU PC research and contribute to improving care and outcomes for future NICU infants and families.
Authors’ Note
For permission and further instruction on the use of the stress evaluation tools utilized in this research study, please contact the following persons: for the PSS:NICU, contact Margaret S. Miles, RN, PhD FAAN at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.