
Abstract
Objective:
To determine pediatric nurses’ perceptions of intensity, frequency occurrence, and magnitude score of selected barriers in providing pediatric end-of-life (EOL) care.
Method:
A translated modified version of National Survey of critical care Nurses’ s Regarding End-of-Life Care questionnaire was used to assess 151 nurses’ perceptions of intensity and frequency occurrence of barriers in caring for dying children.
Results:
The highest/lowest perceived barriers magnitude scores were “families not accepting poor child prognosis” (5.04) and “continuing to provide advanced treatment to dying child because of financial benefits to the hospital” (2.19).
Conclusion:
More high perceived barriers by nurses were family-related issues. One of the possible causes of such deficiencies was lack of palliative care (PC) education/PC units in Iran. Thus, developing EOL/PC education may enhance nurses’ knowledge/skill to face EOL care challenges.
Introduction
The idea that a child may die is simply unimaginable to most people, yet children die daily. 1 According to Morgan, 2 when a child dies, this cycle seems unnatural, causing loss of human potential, and dreams quickly shatter. 2 Children represent health and hope, and their death calls into question the understanding of life. 3 Unfortunately, annually about 50 000 children die in the United States. 4 Of these, over half die during the first year of life. 5 A child’s chronic illness may progress to the point of becoming a terminal illness that deemed to be incurable, ultimately leading to death. 1 Unlike adult populations, who more frequently die at home or in hospice-type settings, more than half of the children with acute and chronic illnesses die in inpatient hospital settings. 6 So providing comprehensive and compassionate end-of-life (EOL) care for these children within a family-centered and developmentally appropriate context is necessary. 7 End-of-life care is an important method of care for infants and children with terminal illness through the prevention or alleviation of physical, emotional, social, and spiritual suffering. 8 Unfortunately, the transition to EOL care is often late and abrupt in pediatrics 9 and seems inherently unnatural in the mind of many parents and doctors, who often struggle to accept that nothing more can be done for a child. 10 Pediatric palliative care (PPC) is a relatively new and developing specialty, 11 which begins when an illness is diagnosed and continues regardless of whether or not a child receives treatment directed at the disease. 12 Health care professionals face numerous obstacles and challenges while providing care to this unique population of clients and their families, 2 which differ from those cited for adults. 13 Although interdisciplinary care is essential for EOL care quality, nurses play the key role of child-family advocate. 1
Reviewing literature indicated a few studies 13 –15 that examined the views of pediatric nurses on providing pediatric EOL care. 14 In Western countries including United States, Beckstrand et al 14 using modified version of National Survey of critical Nurses’ Perceptions Regarding End-of-Life Care questionnaire asked 474 pediatric intensive care unit (PICU) nurses to rate size and frequency of listed obstacles and supportive behaviors in providing pediatric EOL care. They found that the item “language barriers” was the highest perceived obstacle with both the highest mean intensity and frequency scores. 14 In Spain, Iglesias et al 16 used the samequestionnaire to determine the relative importance of helpful behaviors and obstacles that affect EOL care for pediatric patients and their families in PICUs as perceived by nurses. Nurses viewed “evasive physicians” and “families are not accepting of a poor prognosis” as obstacles. 16 In California, Davies et al 13 also conducted a study using a self-report questionnaire to explore the barriers to palliative care (PC) experienced by pediatric health professionals (117 nurses and 81 doctors). Approximately one half of the respondents reported “uncertain prognosis,” “family not ready to acknowledge incurable condition,” and “language barriers” as frequently or almost always occurring barriers. 13 In Egypt, Moawad 15 using the NSCCNR-EOLC questionnaire assessed 94 PICU and NICU nurses’ perceptions of obstacles and supportive behaviors in providing EOL care. He revealed that the most perceived obstacle by nurses was “child having pain that is difficult to control or alleviate.” 15
To our knowledge, in the context of Iran, no study has been conducted to assess barriers in providing pediatric EOL care. This study, thus, conducted to assess nurses’ perceptions of intensity, frequency, and magnitude score of selected barriers in providing pediatric EOL care in pediatric units in Kerman hospitals.
Context
Death in different cultures has become inextricably linked in the particular ceremonies and customs, which originated in inconsolable affections and feelings that has been painful experience. 17 Therefore, it seems necessary to mention the context in this study. Iran, officially the Islamic Republic of Iran, is a diverse country consisting of people with many ethnic backgrounds cemented by the Persian culture. The main language spoken is Farsi or Persian. 18 Persian literature, which is heavily informed and influenced by Islamic and mystical spiritual beliefs, is fraught with poems and stories that portray death as a glorious incident that takes people from one stage of their material/mortal existence through to the realm of divine immortality. 19,20 In the most celebrated and the great mystical Persian poems, Masnavi, Rumi narrates that death is the time of release from this cage of the body; the time when the bird of the soul flies free. The body, like a mother, is pregnant with the spirit-child: death is the labor of birth. All the spirits who have passed over are waiting to see how that proud spirit shall be born. 21 Health care in Iran is based on the following 3 pillars: the public-governmental system, the private sector, and non-governmental organizations 22 (NGOs). According to Mehrdad, 23 health care and public health services are provided through a nation-wide network consisting of a referral system, starting at primary care centers in the periphery going through secondary-level hospitals in the provincial capital and tertiary hospitals in major cities, which is managed by Ministry of Health and Medical Education (Figure 1). He goes on that there are many NGOs active in health issues in Iran. Non-governmental organizations are mainly active in special fields like breast cancer, diabetes, thalassemia, and children with cancer (MAHAK), which are run by charitable foundations. This organization was founded in 1991. It is funded entirely by donations and has supported 11 505 children over the past 17 years. 23 Iranian children are cared for within the primary health care (PHC) system up to the age of 6 years. 24
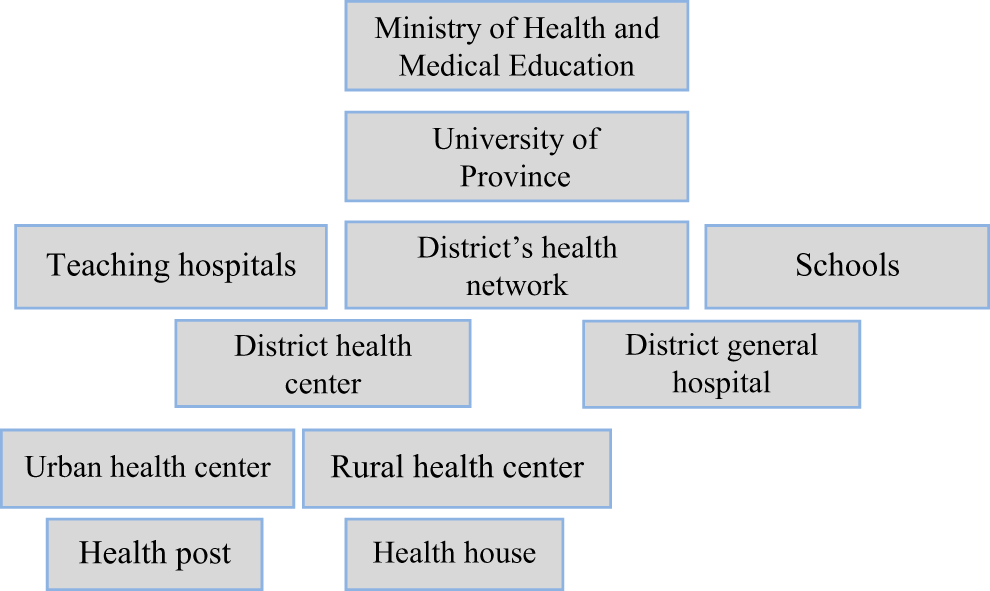
Health system network in Iran. 23
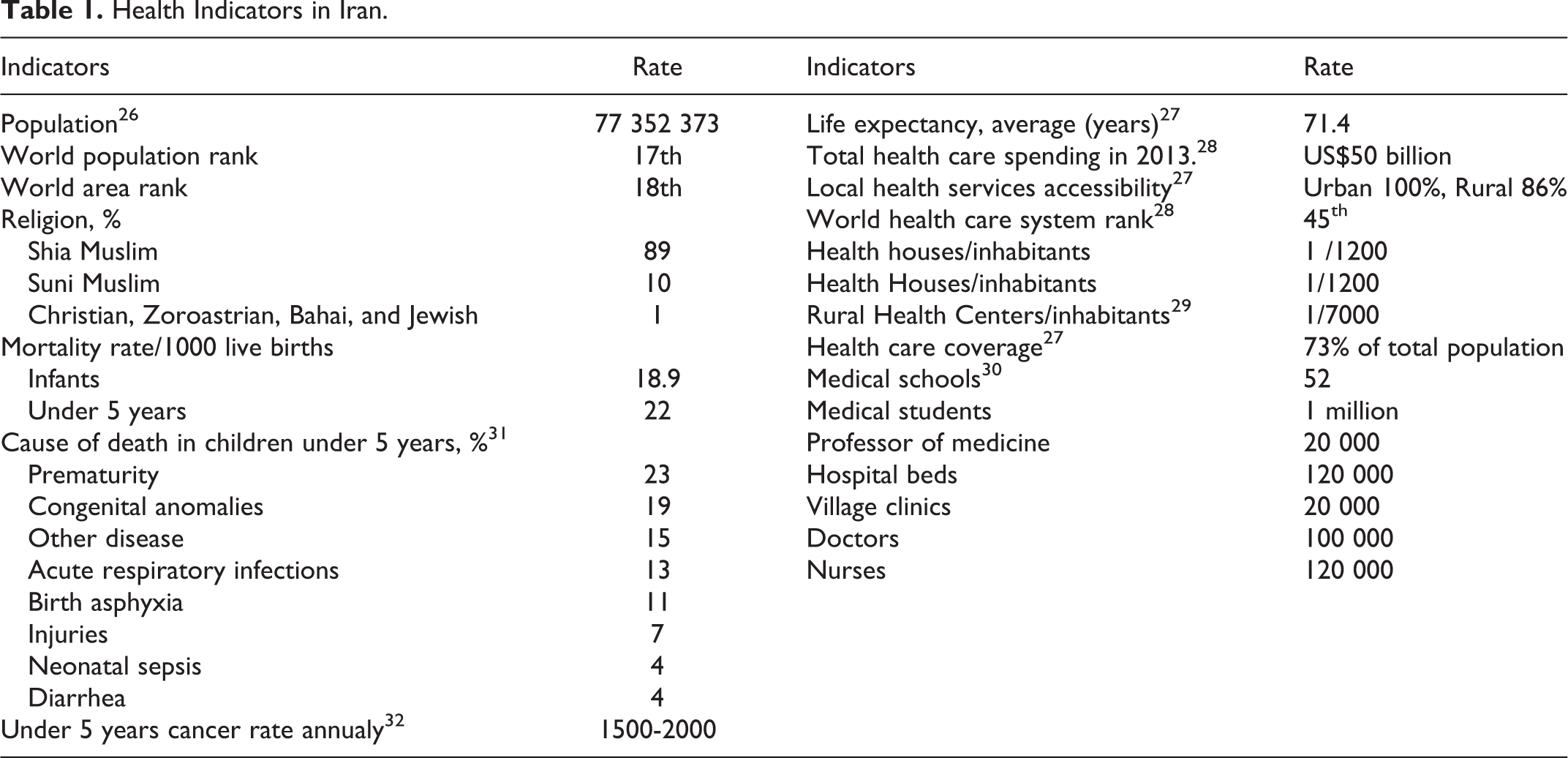
According to Lankarani, 25 the expansion of medical education despite suffering from an 8-year imposed war, as well as facing a 29-year lasting sanction has fulfilled all the health and medical sciences needs in higher education (as it is indicated in Table 1). In line with many developing countries, 33 PHC services in Iran do not offer any kind of palliative and EOL care to patients and their families. Although providing specific care services is highly recommended within the second and third levels of the PHC system in the country, 34 PC has not been accepted by the Ministry of Health and Medical Education, as well as by the administrative and political health authorities. However, outpatient palliative department (OPD) has been newly established (since 3 years) in 2 large cities (Tehran and Isfahan), and one of the cities (Isfahan) also has a PC unit. 35 Palliative care and PPC education is neither included as specific clinical education nor as a specific academic course in the Iranian nursing educational curriculum. The BSc nurses’ curriculum contains only 2 to 4 hours of theoretical education about death and caring for a dead body. Recently, just 1 credit unit about PC was added to MSc of critical care nursing curriculum.
Health Indicators in Iran.
Method
Design
This is a cross-sectional, descriptive study that examined pediatric nurses’ perceptions of intensity and frequency occurrence of selected barriers in caring for dying children. Approval of the study was received by Kerman Medical University (KMU). There was also an approval from the heads of 2 hospitals supervised by KMU, prior to the collection of data.
Sample
The sample consists of staff nurses working in pediatric units including pediatric general units, pediatric oncology units, PICU, and pediatric emergency units in 2 hospitals (Shahidbahonar and Afzalipour) supervised by KMU. Afzalipour is a general hospital with 462 active beds and Shahidbahonar is a trauma hospital with 367 active beds. These hospitals located in an area called Kerman in the center of Kerman Province in Southeast Iran, which provides medical services for the whole province. All nurses working in the aforementioned units were surveyed. Staff nurses who were considered eligible for the study had at least six-months working experience in these units and provided care to dying children.
Background Information
First, a demographic questionnaire consisting of 17 questions that was assumed to influence pediatric nurses’ perceptions of barriers in providing pediatric EOL care was designed. The questions developed were based on previous literature review and authors’ experiences. The items included the following 4 categories: (1) personal characteristics like gender, age, marriage status, and level of education; (2) professional characteristics like ward, work hours per week, number, and age range of dying children who were cared for; (3) previous personal experiences related to death and dying, such as family and closed friends’ death experience, dying family member care experience, duration of caring for a dying family member, and personal EOL care education; and (4) religiosity index consisting of intrinsic (belief in God) and extrinsic (attendance at religious services and activities) religiosity.
Instrument
To determine pediatric nurses’ perceptions of intensity, frequency occurrence, and magnitude score of selected barriers in providing pediatric EOL care, a translated modified version of the NSCCNR-EOLC questionnaire was used. This questionnaire was developed, pretested, and administered in 1998 and revised in 2005. 36 The final version of questionnaire consists of 56 items including 29 obstacle items, 24 supportive behaviors, and 3 open-ended questions. 37 Separate responses are required for intensity and frequency. Barriers intensity and frequency were rated on a 6-point Likert-type scale. For this study, the 6 intensity and frequency alternatives in the original article were grouped together in a single category, and 6 levels were reduced to 4 levels including 0 = not a barrier, 1 = little barrier, 2 = moderate barrier, and 3 = large barrier and 0 = never happens, 1 = rarely happens, 2 = sometimes happens, and 3 = always happens. The items are ranked from highest to lowest based on their mean scores to determine which items are perceived to be the most intense obstacles or supportive behaviors and which items are perceived to occur most frequent. To determine which barrier items were perceived as the most intense and the most frequently occurring, the mean intensity score (MIS) of each item was multiplied by the item’s mean frequency score (MFS) to achieve an overall perceived barriers magnitude (PBM) score. The possible perceived magnitude score for each item ranged from 0 to 25 and for the following study 0 to 9. For the current study, facilitator items and 3 open-ended questions were omitted and just barriers subscale was used. For translation of the questionnaire from English into Farsi, the standard forward-backward procedure was applied. Translation of the items was performed by 2 professional translators (SI and MAF) who are nurse educators. Their native language is Farsi, and their second language is English. Both of them have had experience of living abroad, and SI was educated about PC in a Western country for 5 years. Therefore, she has knowledge about EOL and PC in both Eastern and Western cultures. A helpful reference at this stage was the Haiiem English-Farsi dictionary. Based on their religious beliefs, they suggested that it is better to divide the item “Family not having a support person, for example, social worker or religious leader” to 2 items including family not having a support person, for example, social worker and family not having a support person, for example, religious leader. They believed that each item should not be devoted to more than one concept. Therefore, the total barriers were 30 items. Afterward they were back-translated into English, and after a careful cultural adaptation, the final versions were provided. The translated questionnaire went through pilot testing. Suggestions by nurses (n = 20) were combined into the final questionnaire versions.
Reliability and Validity
Reliability and content validity for NSCCNR-EOLC has been checked in previous research. 27 The authors found an acceptable validity and reliability for the instrument. In Iran, no study was found that assessed the reliability and validity of this scale; therefore, the validity and reliability of the scale was rechecked. The validity of scale was assessed through a content validity. Ten faculty members at the Nursing and Midwifery School reviewed the contents of the scales from cultural and religious perspectives. They left the same suggestions as the translators. They agreed that the translated scale has an acceptable validity. These experts were also asked to independently rate each item in terms of its relevance, clarity, and simplicity on a 4-point scale. According to their comments, to reassess the reliability of translated scale, an α coefficient of internal consistency (n = 20) was computed. The α coefficient for the scale was 0.91. Therefore, the translated scale presented acceptable reliability. The questionnaire obtained an acceptable validity (content validity index [CVI] = 0.92) for barriers section and for facilitators section (CVI = 0.89).
Data Collection and Analysis
Accompanied by a letter, including some information about the aim of the study, the questionnaires were handed out by the second author to all the convenient staff nurses (registered nurses and auxiliary nurses) working in the mentioned pediatric units during the 2 months (November/December 2013). Some oral information about the study was also given by the second author to all participants in a seminar. Informed consent form was obtained from all the participants. Participation in the study was voluntary and anonymous. In total, 173 sets of questionnaires were distributed with a dropout of 22. Finally, 151 nurses (response rate, 87.2%) were included in the study. Data from the questionnaires were analyzed using Statistical Package for Social Scientists (SPSS version 21). A Kolmogorov-Smirnov test indicated that the data were extracted from a population with a normal distribution descriptive statistics was computed for the study variables. Mean scores were individually computed for the intensity and frequency for each item. Items were ranked according to their mean scores to determine which ones were perceived as the most intense barriers, as well as the most frequent barriers. In addition, the PBM scores were ranked from highest to lowest. Based on the purposes of this study, emphasis was placed on the overall magnitude scores to answer the research questions (Table 2).
Barriers to Providing EOL Care in Pediatric Units: Intensity, Frequency, and PBM, Ranked by PBM Score.
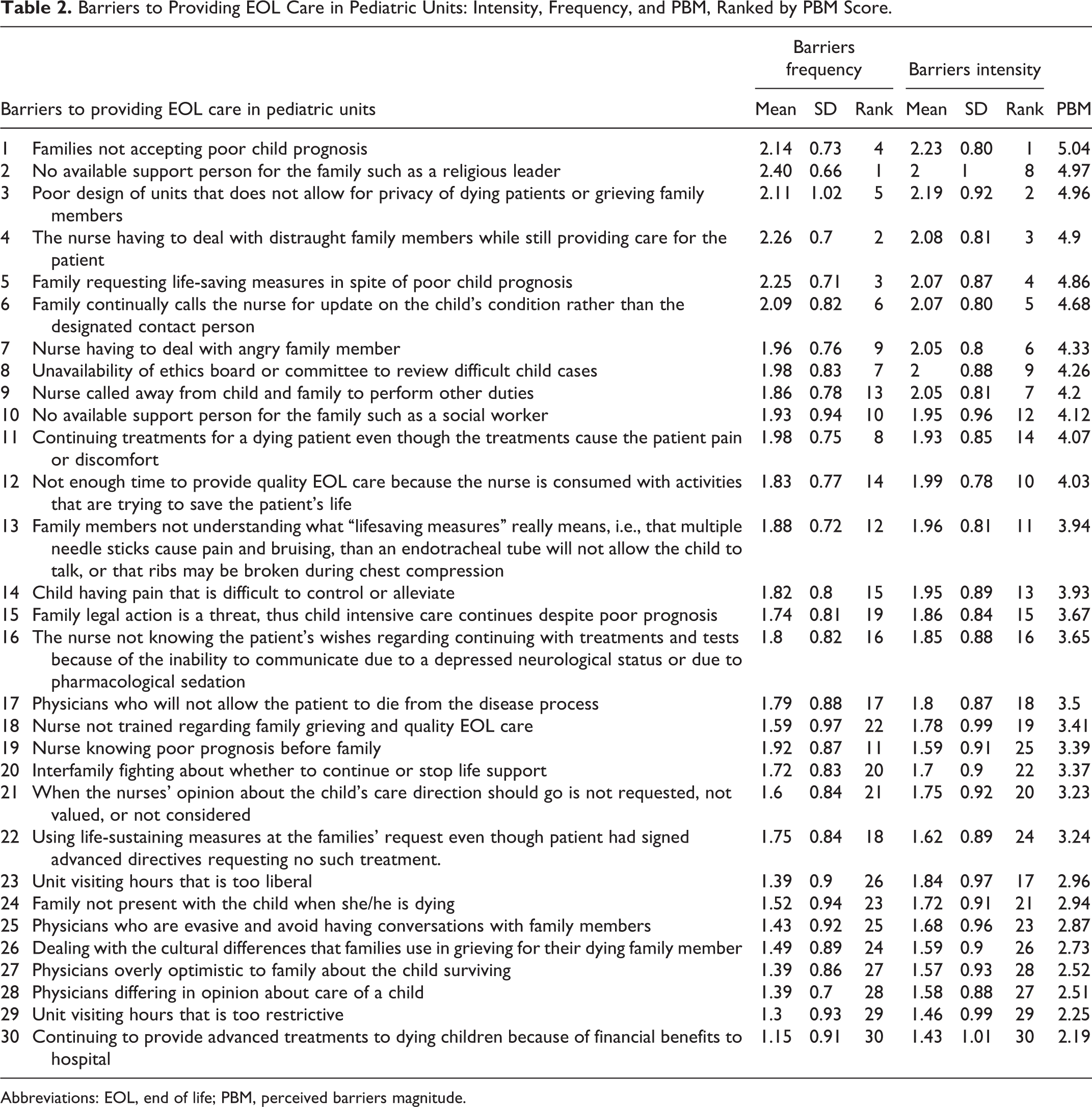
Abbreviations: EOL, end of life; PBM, perceived barriers magnitude.
Results
Participants
The sample consisted of 151 participants. A descriptive analysis of background information (Table 3) revealed that the participants’ age ranged from 20 to 65 years with a mean age of 32.7 years (standard deviation [SD] = 6.12). They were mainly female (98.7%) and married (80.1). Most of them had a B Sc in nursing (82.1) and stated that they receive no education about EOL care (77.5%). Approximately half (54.3) of participants were working in non-ICUs including pediatric general units, pediatric oncology units, and pediatric emergency unit. Rest (45.7) of them was working in PICUs. The participants reported that they had experience of 0.5 to 31 years in nursing, with a mean of 8.7 years (SD = 6.63). All the participants experienced caring for dying children. More than half (62.9) of them cared for less than 10 dying children during their professional career. The age of less than half of the dying pediatric patients (42.4) ranged between 2 and 5 years. Reported weekly employment hours ranged from less than 30 hours to more than 40 hours; 46% of the participants worked more than 40 hours weekly; 25.8% of the participants experienced caring for a dying family member. The mean years of participants’ experiences of caring for a dying member of family were 0.9 years. All respondents were Muslim and Shia. The majority (97.4%) of participants stated that they always experienced the existence of God in their daily living. Most (72.2%) of them claimed that they performed religious activities daily.
Participants’ Demographic Characteristics.a,b,c
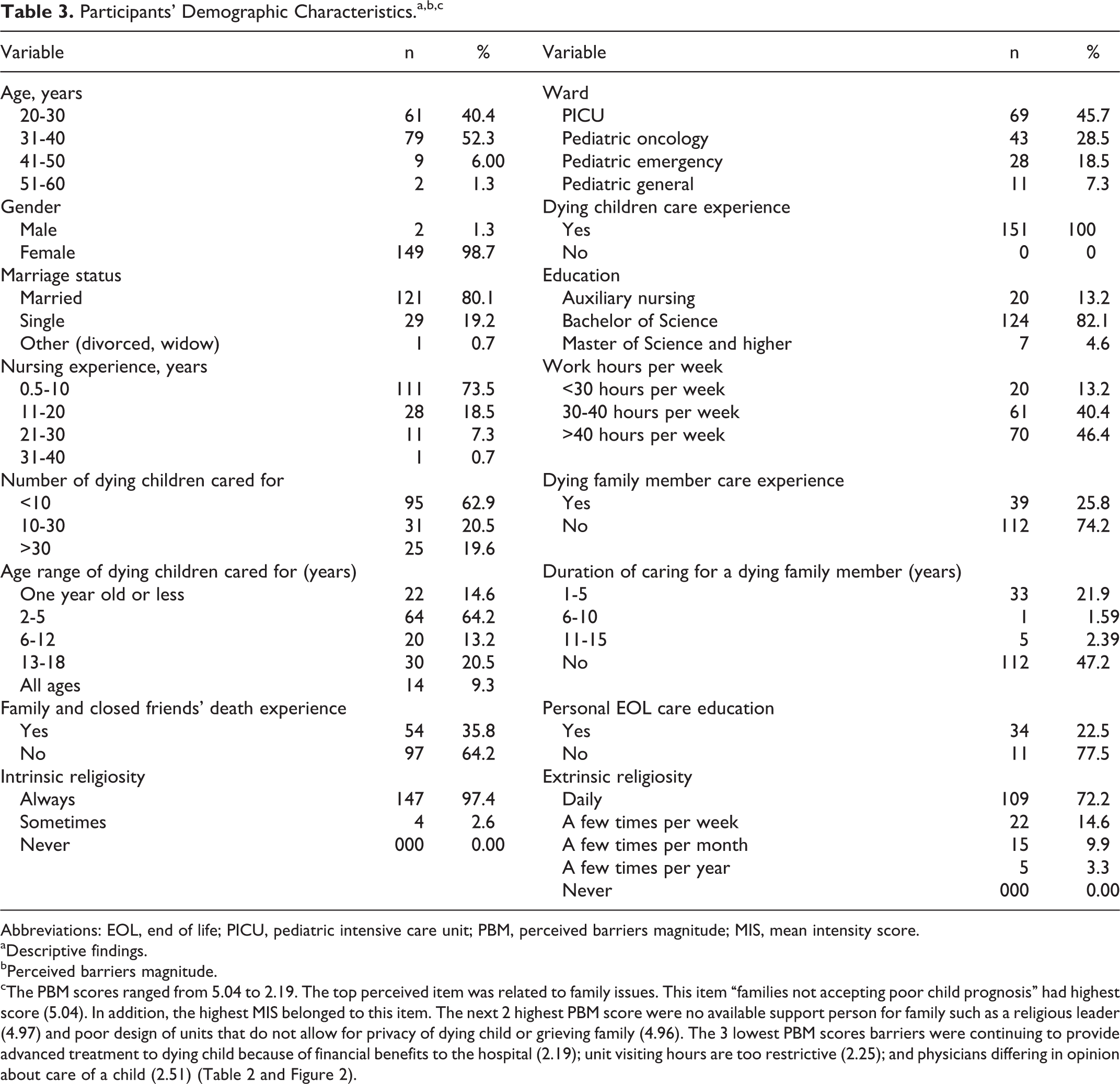
Abbreviations: EOL, end of life; PICU, pediatric intensive care unit; PBM, perceived barriers magnitude; MIS, mean intensity score.
aDescriptive findings.
bPerceived barriers magnitude.
cThe PBM scores ranged from 5.04 to 2.19. The top perceived item was related to family issues. This item “families not accepting poor child prognosis” had highest score (5.04). In addition, the highest MIS belonged to this item. The next 2 highest PBM score were no available support person for family such as a religious leader (4.97) and poor design of units that do not allow for privacy of dying child or grieving family (4.96). The 3 lowest PBM scores barriers were continuing to provide advanced treatment to dying child because of financial benefits to the hospital (2.19); unit visiting hours are too restrictive (2.25); and physicians differing in opinion about care of a child (2.51) (Table 2 and Figure 2).
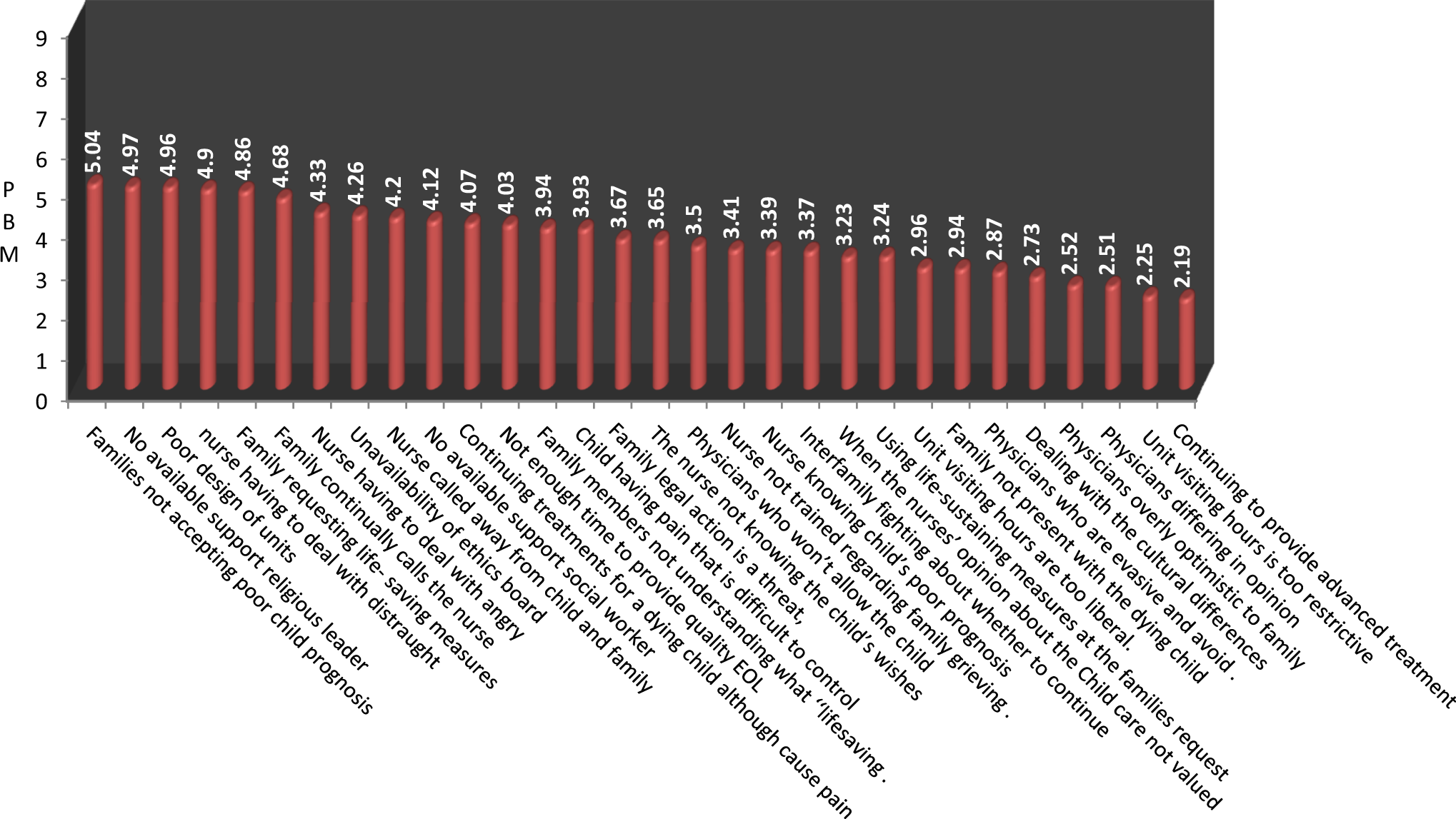
Barriers of providing end-of-life care to terminally ill children ranked by PBM.
Discussion
The aim of this study was to determine pediatric nurses’ perceptions of intensity, frequency of occurrence, and magnitude score of selected barriers in providing pediatric EOL care in Southeast Iran. The first highest perceived barrier magnitude score among all items was “families not accepting poor child prognosis.” Lack of family readiness to acknowledge an incurable condition is congruent with the results of earlier studies where they found this item as one of the most frequent barriers to providing optimal EOL care. 13,37,38 Understanding that a child will die from an underlying illness is most likely multifactorial. Rowse 39 stated that in a death-denying society, children are viewed as being at the beginning of life and are expected to live long and healthy lives. 39 This is highlighted more in the Iranian context, while there is an intense family solidity and bond, as well as strong emotional family relationship. Discussions of death and dying and even the mention of cancer are still taboo in many countries in the Middle East due to lack of education and understanding. 40 Iran represents most religions with a majority of Islam. In Islam, a child is considered to be a gift from Allah, 41 and parents are required to seek treatment for their sick child and to follow the medical and nursing suggestions relevant to the child’s care. 42 Families want to have everything possible done for their dying family member even when those treatments are unnecessary. 43 Families not accepting poor child prognosis could also be related to the uncertain prognosis and unrealistic expectation of technology developments that makes parents to be overly optimistic about the possibility of cure. 13 According to Graham and Robinson, 44 parents’ hopes for recovery, boosted by miraculous recoveries recounted in the media, entice them into believing that the seemingly “endless possibilities of medicine’s technologic prowess” will save their child. 44 Moreover, denying this fact is a coping strategy for family to tolerate this great grief. As Davies et al 13 stated that denial can be a powerful coping mechanism, allowing parents the emotional energy to support their child. The result “families not accepting poor child prognosis” could also be related to the insufficient participants’ knowledge in the field of PC. Based on the results, only 22.5% of the participants were educated about EOL care. As mentioned before, participants had no PC education, which may cause lack of appropriate communication skills to create effective relationship with family.
The second reported high PBM score among all items was no “available support person for family such as a religious leader.” Compared with earlier studies, 13 –16,37,45 this item gained a significant higher PBM score in the following study (with a high MFS, 2.40). The aforementioned studies showed that interdisciplinary teams for EOL care are available. An interdisciplinary team, which consists of at least a nurse, physician, social worker, and a chaplain, is a cornerstone to enhance the quality of EOL care. 46 In the Iranian context, as a religious country with majority of Muslims, there is no chaplain as a member of an interdisciplinary PC team at any age (from children to adult patients) to spiritually support patients and their families. In Iran, chaplains just are accessible after a person dies for consoling the family and holding funeral and mourning ceremony. According to Abedi, 47 a cultural view of death as preventable only by a divine entity highlights the significance of spirituality and hope associated with it as effective notions central to a support system for Iranian patients. 47
The results revealed that “continuing to provide advanced treatment to dying child because of financial benefits to hospital” has the first lowest PBM score among all items, which is in agreement with previous studies. 15,37,45 Culture and religion are 2 important factors that may contribute to the perception of society about EOL issues. 48 According to Shiite experts in Islamic Sciences, life-prolonging treatments should not aim at keeping the patients alive only to save their lives. They go on that in situations that has no cure, people can refuse death-prolonging procedures including cardiopulmonary resuscitation. 49 However, in Iran, a do not resuscitate (DNR) order is not legally accepted. Iranian physicians are reluctant to write such orders because there have been no published guidelines, position papers, legislation, or official statements concerning EOL care, making them fearful of legal problems and criminal prosecution. 50 Mogadasian et al 51 reported that Iranian nurses have negative attitudes toward DNR in many key items of attitudes of DNR questionnaire. This study highlighted that DNR laws and religious aspects of DNR in Islam may change the attitudes of health care providers toward DNR orders. 51 Children are valued and respected in Islam as individuals with inherent rights, and they have the right to be treated with respect and without violence. 52 When the child is not ventilated, but a decision of DNR or limiting vital support measures is made, none has objections to limit therapy. 53 Therefore, based on the principle religious rules in the context hastening or postponing death is forbidden, terminally ill patients cause a large financial burden for health care services.
The findings indicated that the item “Unit visiting hours is too restrictive” has the second lowest PBM score among all items. This is consistent with the finding of earlier research. 54,55 The restrictive visiting hours result in several disadvantages for EOL care. Restricting visiting hours isolate families from a dying child at a time when families need to be close to their loved ones. 37 The cultural background of most Islamic countries stresses about the family ties. Therefore, it is more the responsibility of the family and close relatives and friends to provide the care in a dedicated way. 56 In the Iranian culture, patient may never be left alone by family or friends. This facilitates family to be with the dying child to provide happiness and a peaceful mind. Nonrestrictive visiting hours allow family members to be included in daily interdisciplinary rounds. Consequently, nurses or other health care professionals have time to share critical information with family members. 57
Conclusion
Nurses in this study perceived that the most important barriers in pediatric EOL care are family issues. One of the possible causes of this result mentioned in the discussion was lack of PC education and unit. Therefore, developing EOL and PC education based on Islamic beliefs and Iranian culture may enhance nurses’ knowledge and skill, which enable them to face the challenges of EOL care. Providing some educational programs for the families about death and dying, especially about copying strategies, could be helpful. Establishing OPD and PC units in the community, as well as developing palliative home care programs that focus on family members who play an important role in children’s care, may have a positive effect on children’s EOL care. Active involvement of chaplain and a psychologist to the treatment team in order to provide spiritual and psychological support for the family may strengthen EOL care. This also reduces the unnecessary cost of hospitalization and extra medical examination costs for incurable patients. Finally, expanding NGOs and charities such as “MAHAK” would be very helpful to diminish family economical and psychological burden.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.