
Abstract
Little is known about the quality of life (QoL) for informal caregivers of disabled older adults aged 65+ with diverse backgrounds. Forty-two caregivers were interviewed in English and Cantonese about their caregiving experiences, their recollections of QoL over time, and the factors influencing their appraisals. Overall, 52% of caregivers experienced a decline in QoL. Factors associated with decreased QoL were less time for self, competing financial demands, and the physical and emotional impact of the patient’s illness. Factors associated with no change in QoL were minimal caregiving responsibilities, a sense of filial duty, and QoL being consistently poor over time. Factors associated with improved QoL were perceived rewards in caregiving, receiving institutional help, and increased experience. Chinese caregivers were more likely to cite filial duty as their motivator for continued caregiving than were Caucasian caregivers. In conclusion, informal caregivers take on a huge burden in enabling older adults to age in the community. These caregivers need more support in maintaining their QoL.
Introduction
Older adults with late-life disability makeup a large and growing segment of the American population and will need increasing assistance with activities of daily living (ADLs) to remain independent. 1 Our present health care system is not equipped to support the needs of these older adults, resulting in a large dependence on informal caregivers, most of whom are untrained and unpaid family members. 2,3 In 2009, about 42 million people served as unpaid family caregivers at any given point in time, providing an average of 18 hours of care per week, or an estimated economic value of approximately US$450 billion, up from an estimated US$375 billion in 2007. 4,5
The social circumstances of patients affect their health outcomes, including morbidity, mortality, and quality of life (QoL). 6 –8 Informal caregivers are an integral component of these social circumstances, particularly as patients approach the end of their lives and require increased levels of caregiving. Since the palliative model of care is designed to support both the patient and their informal caregivers, evidence about the factors affecting informal caregivers’ QoL has direct implications for palliative care practice, research, and policy. The current literature on informal caregivers is dominated by studies of individuals who care specifically for persons with cancer and dementia, yet caregivers provide care such as direct care or social support, especially in late life, for care recipients of all types. 9,10 However, surprisingly little is known about the informal caregivers who provide unpaid care to older adults experiencing disability in late life due to a multitude of causes, particularly as it pertains to caregiver QoL. 11 Moreover, little is known about the caregiving experience of culturally diverse elders living with late-life disability. This qualitative study was done as a first step to generate hypotheses about the QoL for caregivers of diverse older adults with late-life disability.
Methods
Study Design and Sample
For this qualitative interview study, semi-structured interviews were conducted with informal caregivers caring for disabled older adult relatives aged 65+. A broad cross section of caregivers were recruited from multiple sites, including a Program of All-inclusive Care for the Elderly (PACE), caregiver support groups, multipurpose senior facilities, geriatrics clinics—all in Northern California—and an advertisement through a national caregiver advocacy group Web site (Family Caregiver Alliance; https://www.caregiver.org/).
Calls and e-mails from interested caregivers were screened over the phone by our research team to determine eligibility. Caregivers who spoke English or Cantonese and who provided assistance to a disabled older adult relative aged 65+ were eligible for participation in the study. Late-life disability was defined as needing assistance with at least 1 ADL—bathing, toileting, transferring, eating, and dressing. Caregivers could be bereaved (within the last 5 years) or currently providing care and could be coresiding, proximal, meaning living within 1 hour travel time, long distance (>1 hour travel time), or mixed, meaning sometimes coresiding with the patient, sometimes apart. We included informal caregivers of older adults residing at home as well as in nursing homes, as the literature suggests that informal caregivers of nursing home residents experience substantial caregiver stress. 12
Data Collection
After obtaining informed consent, willing and eligible caregivers were interviewed by telephone (∼45 minutes) using a common interview guide. Interviews were conducted in English and Cantonese. After translation from English into Cantonese, the interview guide was reverse translated to ensure accuracy. Where words or concepts did not translate well from English to Cantonese, we located a word or concept that worked well in Cantonese and translated back to English. Participants were asked open-ended questions that explored their caregiving experience, including how they rated their QoL over time. Participants were also asked to complete a short demographic survey after the interview.
To assess QoL changes over time, caregivers were asked to respond to the question, “How would you rate your overall quality of life?” with 1 of the following 5 answers: excellent, very good, good, fair, or poor. Caregivers were asked to reflect back on their time at 2 different time points: (1) when they first started caregiving and (2) for caregivers of living patients, QoL during the past month before enrollment in the study or, for caregivers of patients who died, QoL during the last month of the care recipient’s life. Participants were also probed to appraise their caregiving experience by explaining why they assigned their QoL a certain rating. Probes included inquiries about the types of care provided, expectations about patient’s disease progression, coping strategies/personal resources, and QoL for the patient.
Data Analysis
Interviews were audio-recorded, transcribed, and then analyzed using NVivo 8. 13 Data were analyzed using a constant comparative analysis and reiteratively reviewed to identify new themes. 14 –16 A random subset of transcripts (N = 10) were jointly coded by the authors (J.N.T., J.G.C., and A.K.S.), and an initial common codebook was developed. Quality of life was assessed in two different ways: using the QoL ratings to determine the trajectory of QoL over time and using descriptions of how caregiver QoL changed to look for common themes. Codes were added as new themes emerged throughout the coding process. When no new themes emerged, saturation was reached and no further interviews were conducted. Themes were examined for potential differences by cultural group. The Committee on Human Research of the University of California at San Francisco and the San Francisco Veterans Affairs Research and Development Committee reviewed the informed consent forms and approved this study.
Results
Characteristics of Caregivers and Care Recipients
The mean caregiver age was 54 years, ranging from 28 to 85 years, 76% (n = 32) of the caregivers were female. Caregivers represented all 4 US Census regions, with predominance from the West (see Table 1). Fifty-two percent of the caregivers specifically mentioned providing help with at least 1 ADL, 69% with at least 1 instrumental ADL (IADL), and 40% with both ADLs and IADLs (note 26% of care recipients were nursing home residents and received full ADL support from nursing home staff). The majority (79%) of care recipients were 75+ years, 60% were female, and 74% were community dwelling. The top 3 diagnoses reported for the care recipients were dementia (38%), frailty/nonspecified decline in function (17%), and heart disease/stroke (17%).
Sample Characteristics of Caregiver Respondents (N = 42) and Patients.
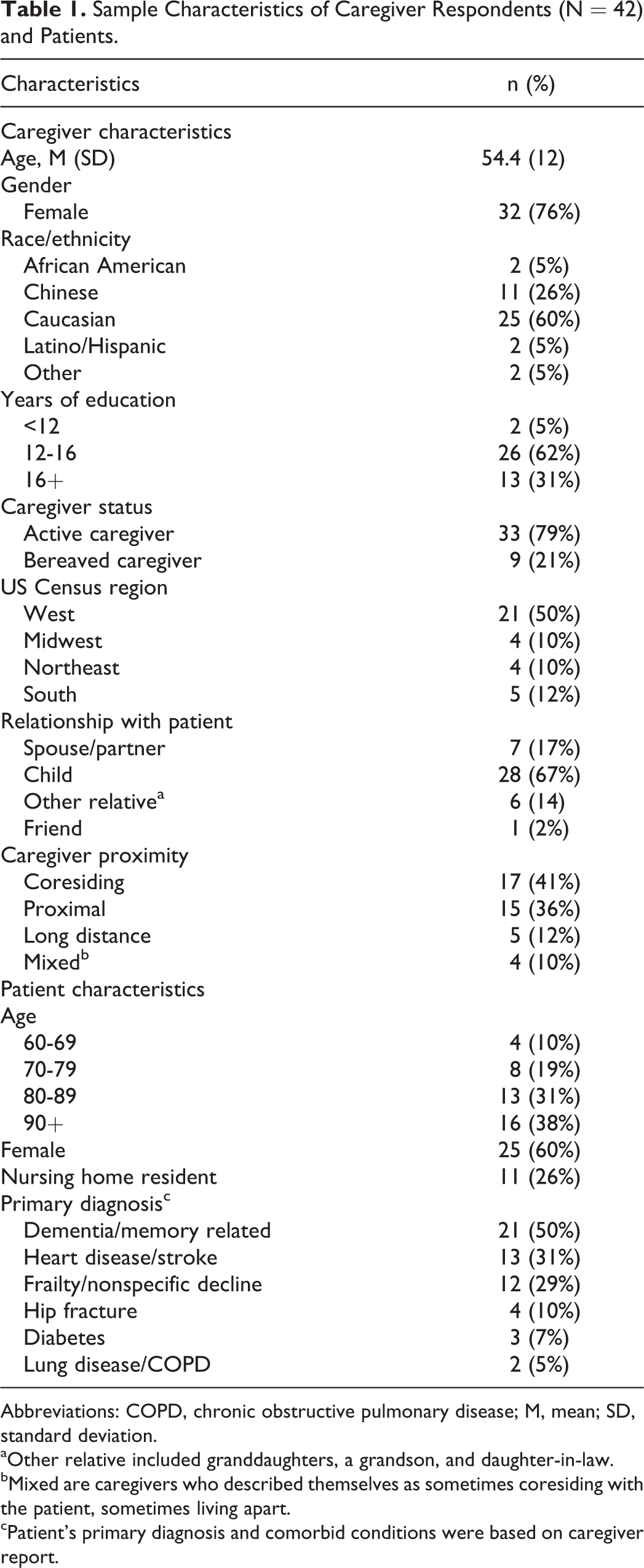
Abbreviations: COPD, chronic obstructive pulmonary disease; M, mean; SD, standard deviation.
aOther relative included granddaughters, a grandson, and daughter-in-law.
bMixed are caregivers who described themselves as sometimes coresiding with the patient, sometimes living apart.
cPatient’s primary diagnosis and comorbid conditions were based on caregiver report.
Overall QoL
Overall, 52% of caregivers reported a decline in their QoL over time, 26% recalled no change, and 21% recalled an improvement. The reasons behind their QoL trajectories were due to modifying factors that we grouped into 4 domains: social, physical, emotional, and financial.
Quality of Life Declined
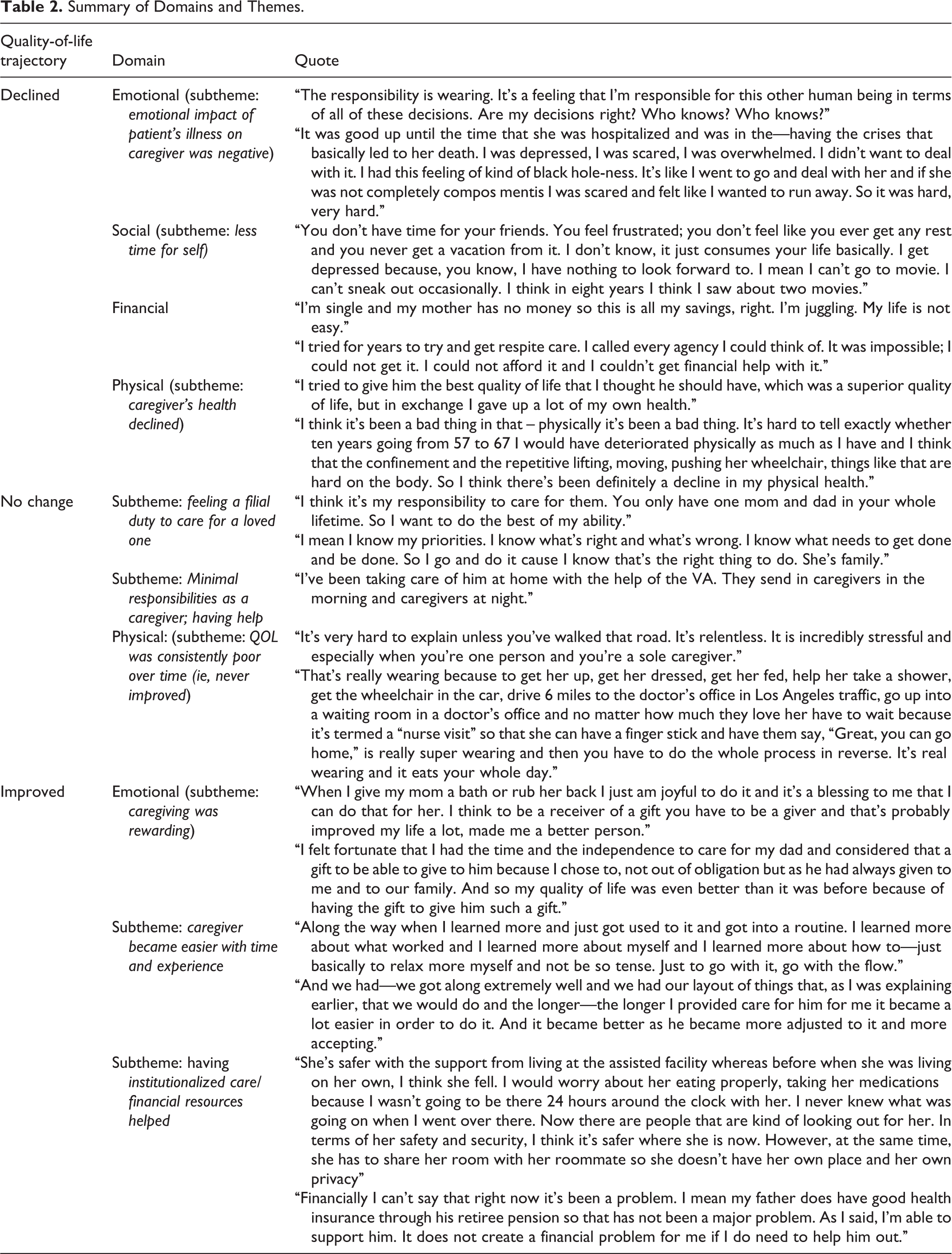
The caregivers who experienced a decline in their QoL identified the following reasons: they had less time for self (social and financial domains), their health declined (physical domain), and the emotional impact of the patient’s illness took a toll on them (emotional domain; see Table 2).
Summary of Domains and Themes.
One caregiver, a 58-year-old wife of an older man with Huntington disease, likened her caregiving to incarceration. She said: It drains everything and ruins your social life. There’s a prison in our community and when I would drive by, I would be so jealous because the prisoners were given an hour outside to play basketball and have fun and I was working every single minute 7 days a week. I also have my own health issues that have arisen in the last few years where I deal with a lot of pain. As things get worse for him I know my stress level goes up and therefore I have a lot more pain. My quality of life is a lot worse than it was a few years ago. My quality of life declined substantially because I loved—still do—my father so much and seeing him decline and the thought of losing him was extremely upsetting. Dealing with mortality is a very depressing thing.
Quality of Life Stayed the Same
The reasons for caregivers’ QoL remaining the same depended on caregivers’ individual circumstances and included feeling a filial duty to care for loved ones (emotional), viewing their caregiving duties as unobtrusive or minimal (social/financial), and perceiving their QoL as being consistently poor over time (physical). For example, a 28-year-old man caring for his grandmother discussed having to fulfill a filial duty: I know my priorities. I know what’s right and what’s wrong. I know what needs to get done and be done. So I do it because I know that’s the right thing to do. She’s family. Everything was relatively easy. All I had to do was drive my father around—it was just like visiting my father pretty much … and I’d be able to do whatever I needed to do. It was very difficult to process. I wondered how I going to continue on with life. It’s just as hard as before. How can it be better? It is just as difficult.
Quality of Life Improved
The caregivers who gave a positive assessment of their experiences described their experiences as “rewarding” (emotional), or had their QoL improved due to the help of professional care providers (financial and social), or increased experience (physical and emotional). As one 31-year-old caregiver said: After I dealt with the initial questions, I came to find it a very rewarding experience to take care of my grandma—she raised me. In the beginning, it was more difficult. Ever since she went to institutionalized care it has been easier. It’s been better with institutionalized care’s help. It’s not as problematic.
Gaining experience and mastery over care-related tasks was also reported to contribute to improvements in QoL over time. In one case, after caring for his 83-year-old grandfather, one caregiver became so inspired that he sought training as a nurse’s aide. He shared: I learned to help people and I began to like helping people.
Findings by Cultural Group
Compared to the non-Chinese group, Chinese caregivers more frequently cited filial piety as a primary motivator for providing care. One Chinese woman caring for her mother-in-law with Alzheimer’s disease said: I should care for her. I’m her daughter-in-law. I’m a pretty traditional person. What I see is that Asian families stick together. They care for their own. Just like my grandma, she lives with us. She doesn’t live in a caregiver’s home or retirement home or whatever you want to call it. She lives with us. Some people friends seem to push putting her in a facility and to me it’s not an option because you’re talking about substantial money. When the time comes, our goal is to keep him at home for as long as financially possible.
Discussion
Our study found that the majority of caregivers for diverse older adults with late-life disability perceived their overall QoL to have declined, though a substantial minority felt that their QoL had either improved or remained the same. Although these findings are not surprising, what is most interesting about the results are the reasons caregivers gave for their respective QoL appraisals. Specifically, the factors that caregivers described as influencing their QoLs fell within a range of 4 domains: social, physical, emotional, and financial. Caregivers whose QoL declined described lack of personal time, dwindling financial resources, severely constricted social lives, and the toll of caregiving on their physical and emotional health. In the cases in which QoL stayed the same or improved, caregiving was perceived to have either little or a positive effect on the 4 domains. Caregivers whose QoL remained the same over time generally felt that it was their filial obligation to provide care. Moreover, the caregivers whose QoL showed improvement felt emotionally rewarded in serving as their loved ones’ primary caregiver.
Other studies of QoL for informal caregivers of older adults with other specific conditions suggest similar findings. Glozman and Duggleby et al found that most caregivers had experienced some degree of decline in QoL due to competing employment or familial responsibilities, loss of social life, and lack of personal time. 17,18 As in our study, Duggleby observed that receiving help with caregiving improved caregiver QoL. Our study builds on these findings by demonstrating that these domains of caregiver QoL also apply broadly in late-life disability. Our study is also unique in that it examined how caregivers perceive their QoL changing over time, which adds another layer of perspective to factors affecting caregiver QoL. Additionally, in our diverse cohort, we found that a sense of obligation or filial duty was particularly important for Chinese caregivers, suggesting that factors related to caregiver QoL are highly contextualized within the cultural backgrounds of caregivers. Moreover, our study found that cultural differences had a significant influence on the motivation for providing care. Specifically, Chinese caregivers were more likely to state tradition as the reason for not placing an elderly relative in a nursing home, whereas their non-Chinese counterparts were more likely to cite financial reasons for avoiding institutionalized care.
We recognize that as a primarily qualitative study, these findings cannot be used to make generalizations about the informal caregiving experience and that due to the small sample size, correlations between caregiving circumstances and how they affect QoL cannot be made. However, the perspectives of our caregiver participants and the identified themes can be used to inform descriptive models of the caregiver experience or guide the development of supportive interventions for caregivers. Furthermore, this was not a longitudinal study and cannot serve to delineate changes in QoL for caregivers over an extended period of time. This study was also retrospective and therefore subject to recall bias. For example, the recalled perceptions of the start of the caregiving process may differ from reports of caregivers assessed prospectively. It is unclear, however, whether this bias would favor a more negative or positive direction with regard to QoL. Perspectives of bereaved caregivers may have been influenced by recollections of the death experience in ways that current caregiver experiences were not. Nevertheless, this study serves to inform larger studies whose data would allow for developing associations to better understand the effects of various aspects of caregiving on QoL in late-life disability.
Findings from our semistructured interviews reveal that QoL for informal caregivers is affected by physical health, social circumstances, financial status, and emotional well-being. Because caregivers largely shape their care recipients’ social circumstances, which affect patient health outcomes, more attention should be paid to the QoL of family caregivers. 19 Unfortunately, the present system often does not do enough to support caregivers who provide care in the home. The National Family Caregiver Support Program, though specifically created in 2000 to provide support for family caregivers, varies widely from state to state in its effectiveness and often leaves service gaps in important areas such as transportation, financial assistance, and respite services, all areas that would affect a caregiver’s physical health, social circumstances, financial status, and emotional well-being and therefore their QoL. 20,21
Another problem is access. Even when sufficient support services are available, many caregivers either do not know the services are available or do not know where to get the services. 22 Since caregivers consider healthcare providers one of their primary sources of support, increasing access could begin with the patients’ care team, which can act as a point of reference, informing caregivers of the resources available to them. 22 Although the care team may feel that caregivers are outside their scope of responsibility, given the burden that family caregivers often assume, physicians and nurses should see them as both part of the care team and potential patients who may need attention of their own.
To alleviate the burden caregivers assume, we should push for health policies that support improved caregiver QoL. Specifically, more funding should go toward implementing formal education programs that would train caregivers to more effectively care for their loved ones or toward expanding palliative care teams, which often provide much needed emotional and educational counseling to informal caregivers. Furthermore, we should push for the nationwide expansion of programs such as the Family Caregiver Alliance (FCA), which supports caregivers through education, services, research, and advocacy. By working to improve caregiver QoL, we will enable informal caregivers to more easily allow disabled older patients to age in place, which has large implications for both improved patient health outcomes and health care savings. 5 –8
Footnotes
Authors’ Note
The 4 listed authors were the sole contributors to this manuscript. All authors who meet the criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals have been listed. AKS designed and supervised the study. JNT recruited study participants, carried out data collection and analysis, and led the drafting of the manuscript. CEB helped with the drafting and revision of the manuscript. JGC assisted with data analysis. All authors contributed to critical revisions of the manuscript. As corresponding author, AKS had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The funding sources had no involvement in this study and had no influence in the collection, analysis, and interpretation of data, nor in the writing of this report or the decision to submit the paper for publication. An abstract of this paper was awarded the American Geriatrics (AGS) Clinical Student Research Award at the 2014 Annual Meeting in Orlando, Florida.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Julie Thai’s effort on this project was supported by the “Medical Student Training in Aging Research (MSTAR)” Program funded by the National Institute on Aging (T35AG026736), the John A. Hartford Foundation, the MetLife Foundation, and the Lillian R. Gleitsman Foundation. Dr Cagle’s efforts were supported by a training grant from the National Institute on Aging (NIA), 5T32AG000212. Dr Smith’s effort on this project was supported by the Beeson Career Development Award from the National Institute on Aging and the American Federation of Aging Research (K23AG040772) and by the ASP-T. Franklin Williams Society of General Internal Medicine Scholars Award in Geriatrics.