
Abstract
Context:
Palliative sedation is a means of relieving intractable symptoms at the end of life, however, guidelines about its use lack consistency. In addition, ethical concerns persist around the practice. There are reports of palliative sedation in the pediatric literature, which highlight various institutional perspectives.
Objectives:
This survey of 4786 pediatric providers sought to describe their knowledge of and current practices around pediatric palliative sedation.
Methods:
Our survey was administered to pediatricians who care for children at the end of life. The survey assessed agreement with a definition of palliative sedation, as well as thoughts about its alignment with aggressive symptom management. Bivariate analyses using χ2 and analysis of variance were calculated to determine the relationship between responses to closed-ended questions. Open-ended responses were thematically coded by the investigators and reviewed for agreement.
Results:
Nearly half (48.6%) of the respondents indicated that the stated definition of palliative sedation “completely” reflected their own views. Respondents were split when asked if they viewed any difference between palliative sedation and aggressive symptom management: Yes (46%) versus No (54%). Open-ended responses revealed specifics about the nature of variation in interpretation.
Conclusions:
Responses point to ambiguity surrounding the concept of palliative sedation. Pediatricians were concerned with a decreased level of consciousness as the goal of palliative sedation. Respondents were split on whether they view palliative sedation as a distinct entity or as one broad continuum of care, equivalent to aggressive symptom management. Institutional-based policies are essential to clarify acceptable practice, enable open communication, and promote further research.
Introduction
Across the United States, hundreds of children having medical ailments die in hospitals each year. 1 Many of them die after the difficult decision to withdraw technological support that no longer meets the goals for care as outlined by the patient and family, 2 and others die without ever experiencing a pediatric intensive care unit environment. Regardless of circumstances, pediatricians at the bedside must treat symptoms as they manifest during the dying process.
Palliative sedation was first defined as “the use of sedative medications to relieve intractable and refractory distress by a reduction in patient consciousness.” 3 Numerous professional organizations have issued position statements and guidelines supporting the use of palliative sedation when all other alternatives to manage symptoms have been exhausted. 4 –10 Various reports in the literature have advocated the use of palliative sedation for patients experiencing intractable pain and suffering at the end of life. 9,11 –13
The use of palliative sedation in pediatrics comes with the added complexities of parental consent and understanding; however, palliative sedation has been endorsed as a valuable option for children. 14 Case reports of palliative sedation in pediatric oncology have been noted to improve comfort at the end of life without hastening death. 15 –18 However, ethical concerns persist. Agreement on when, and if, palliative sedation is warranted remains in question. 19
Sedating medications are almost always integrated into quality palliative care, thus, the distinction between aggressive titration of sedation in the management of difficult-to-treat symptoms and the provision of palliative sedation may be easily blurred. 20 –22 To explore and better describe the current understanding of palliative sedation within the pediatric workforce, we surveyed pediatric providers who commonly care for dying children about their viewpoints and practices. Revealing ambiguity in the concepts around palliative sedation could help clarify practice, ensure consistency, and serve as a framework for improving communication and research.
Methods
Institutional Review Board Oversight
This study was reviewed by the Cincinnati Children’s Institutional Review Board and was granted exempt status. Respondents provided consent to participate in this voluntary and anonymous survey by completing and submitting the instrument.
Study Design and Participants
This exploratory study utilized a custom-designed Web survey. The US pediatric physicians in critical care, oncology, neonatology, and palliative care were the targeted population because they are the providers most likely to manage complex pediatric end-of-life cases. The sampling frame was comprised a list of 4786 individuals belonging to one or more of these American Academy of Pediatrics membership subgroups in 2012. These subgroups are open to all practicing physicians, fellows, and residents and likely included members from each of these levels of training. E-mail addresses were available for all subgroup members. Duplicate entries within the list were removed. The survey was administered via e-mail as a census to all members on the list. The number of pediatric physicians who fell within the target population but not included in the sampling frame was indeterminable.
Survey Development, Design, and Implementation
Three investigators with expertise in pediatric palliative care and 1 with expertise in survey methodology designed the questionnaire using an iterative process that included reviews, input, and suggestions from several other physicians with experience in palliative sedation therapy. Two independent reviewers, both with expertise in palliative care, were asked to evaluate the survey and question/response options for clarity, ease of completion, and correspondence with the stated research objectives.
The first set of survey items included 2 closed-ended questions, each with an open-ended follow-up question to assess pediatricians’ views regarding the appropriate framing of the definition and concept of palliative sedation therapy. The survey’s definition was selected from a commonly available Pediatric Palliative Care Medicine textbook,
23
with “intent” added by the survey authors to reflect the current discussions in the literature. The definition read as follows: Palliative sedation therapy is the use of sedative medications to relieve intolerable suffering from refractory symptoms by a reduction in patient consciousness.
A final set of survey items requested information related to demographic variables as well as each respondent’s experience with palliative sedation cases and institutional practices pertaining to palliative sedation. Respondents were not required to answer any given question before moving to the next item.
Additional questions, based on 3 clinical vignettes, were also included in the survey to assess the kinds of decisions that physicians might make in terms of treatments and drug administration as well as the individuals and factors that might influence those decisions when caring for pediatric patients at the end of life. Data from these questions will be analyzed and shared in a follow-up report (see Appendix A for a print version of the full survey).
The survey was designed and administered using Qualtrics (Provo, Utah), a Web-based survey application that allows for complete respondent anonymity. Additional advanced functions such as question routing and display logic were incorporated to make the survey flow as smoothly as possible, thereby minimizing respondent fatigue and associated nonresponse error. Respondents received an invitation and survey link via e-mail that included a brief, clear description of the purpose of the project, along with assurance of anonymity. The survey remained open for 3½ weeks, with a reminder sent at the end of each week.
Analysis
Descriptive statistics were calculated for each of the closed-ended questions. Three coauthors independently coded the responses to the open-ended questions by themes. The investigators then met to review and resolve any disagreements on the appropriate theme for a given response.
Bivariate analyses using Chi-square and analysis of variance (ANOVA) were used to analyze the relationships between closed-ended questions and comparison variables that included demographic variables and questions pertaining to their experience. In addition, descriptive frequency cross-tabulations were calculated to explore differences in responses to the open-ended questions across the comparison variables. All analyses were performed using IBM SPSS Statistics for Window, version 19 (IBM Corp, Armonk, New York).
Results
Respondent Characteristics
Eight hundred thirty-one people submitted responses, for a response rate of 17.8%. The item response rate varied among the questions because responses were not required for any individual item. Submitted surveys had a median completion time of 12 minutes 25 seconds. The frequency breakdowns of respondents by gender, age, primary clinical role, location, and various indicators of experience with palliative sedation are shown in Table 1 and include the number of respondents who skipped a particular item. The targeted subgroups contained many generalists or hospitalists who completed the survey. Their responses were considered equally and are indicated by the group name generalist/hospitalist/primary care.
Comparison Variables.a
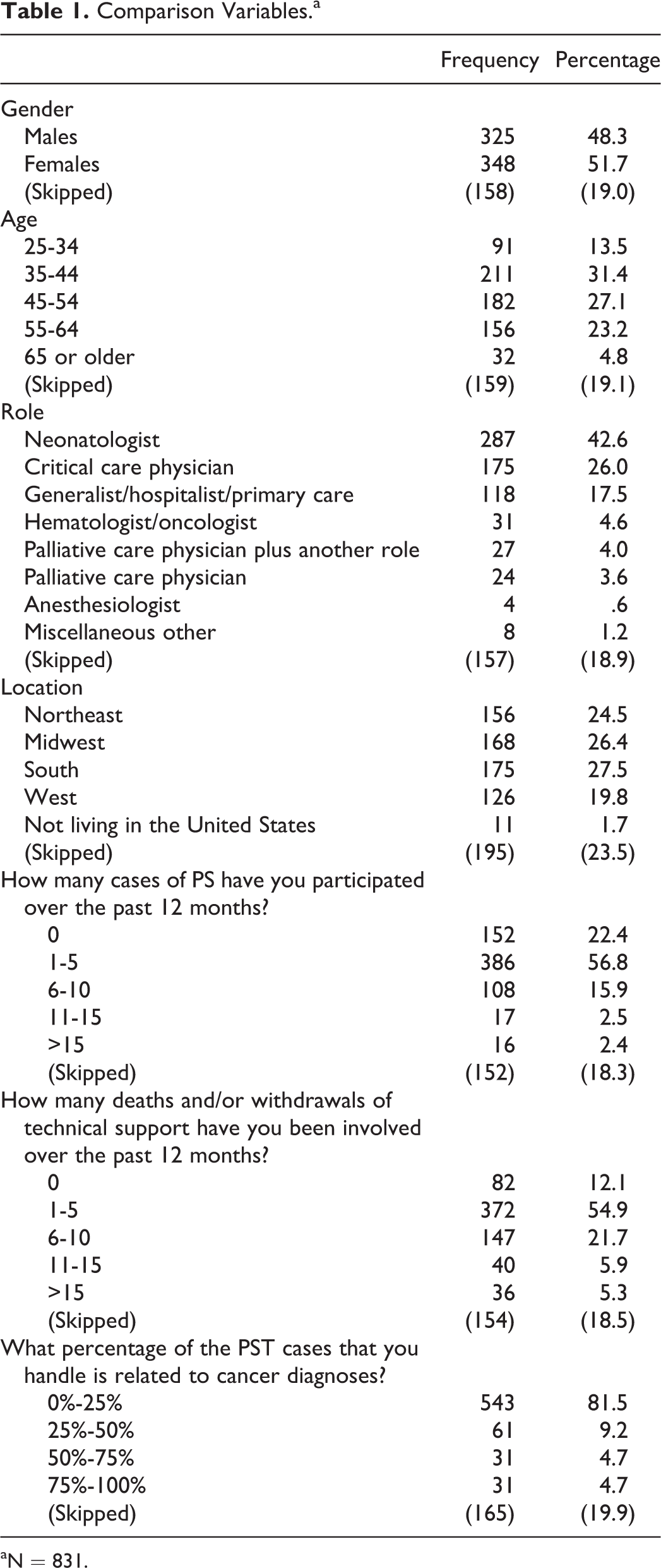
aN = 831.
Definition and Concept of Palliative Sedation Therapy
Nearly half (48.6%) of the respondents indicated that the stated definition of palliative sedation “completely” reflected their own views. Response frequencies for each of the response options are shown in Table 2. The ANOVA revealed no significant mean differences based on any of the comparison variables. Also shown in Table 2 are the most common themes along with illustrative quotes regarding the changes respondents would make to the definition provided to better reflect their own views. The themes included objection to decreased consciousness as a goal, adding anxiolysis, implying timing to be near impending death, and removing the term “intolerable.” The proportionality of these responses was similar across demographic variables, but there was a notable difference based on respondents’ primary roles. A smaller percentage of generalist/hospitalist/primary care respondents (19% or 8 of the 42) and hematology/oncology respondents (15% or 2 of the 15) cited an “objection to decreased consciousness as the goal” when compared to all other roles, which ranged from 32% (41 of the 129) of neonatology respondents to 42% (31 of the 74) of critical care respondents. It should be noted that proportional differences are only descriptive and cannot be compared statistically since they were based on voluntary responses to the open-ended questions.
Views Regarding the Appropriate Definition of Palliative Sedation.
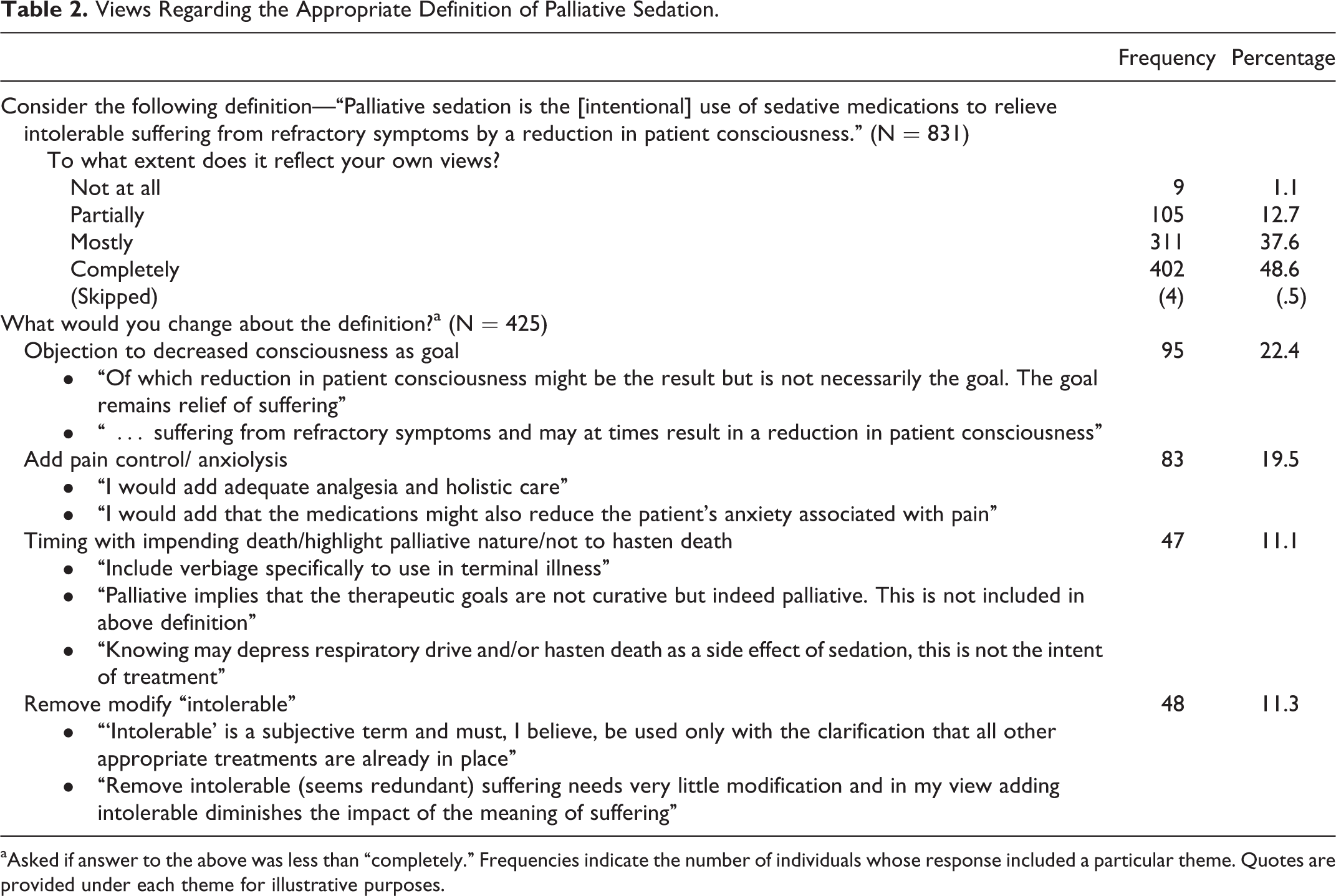
aAsked if answer to the above was less than “completely.” Frequencies indicate the number of individuals whose response included a particular theme. Quotes are provided under each theme for illustrative purposes.
A One-sample binomial test indicated that there was a statistically significant difference in the proportion of those who said Yes (46%) versus No (54%) in response to the question asking whether they viewed any key differences between palliative sedation and aggressive symptom management (exact binomial P = .028). The χ2 analyses also indicated a significant relationship between a respondent’s primary clinical role and responses to this question (χ2 [4, N = 667] = 14.269, P =.006). More specifically, those who identified critical care (66% or 116 of 175) and oncology (66% or 19 of 29) as their primary role were more likely than others to have the view that there is not a difference between palliative sedation and aggressive symptom management. There were no significant relationships between responses to this question and other comparison variables. Themes and example responses to the follow-up question asking those who viewed a difference between palliative sedation and aggressive symptom management to describe those key differences are included in Table 3.
Views Regarding the Difference Between Palliative Sedation and Aggressive Symptom Management.
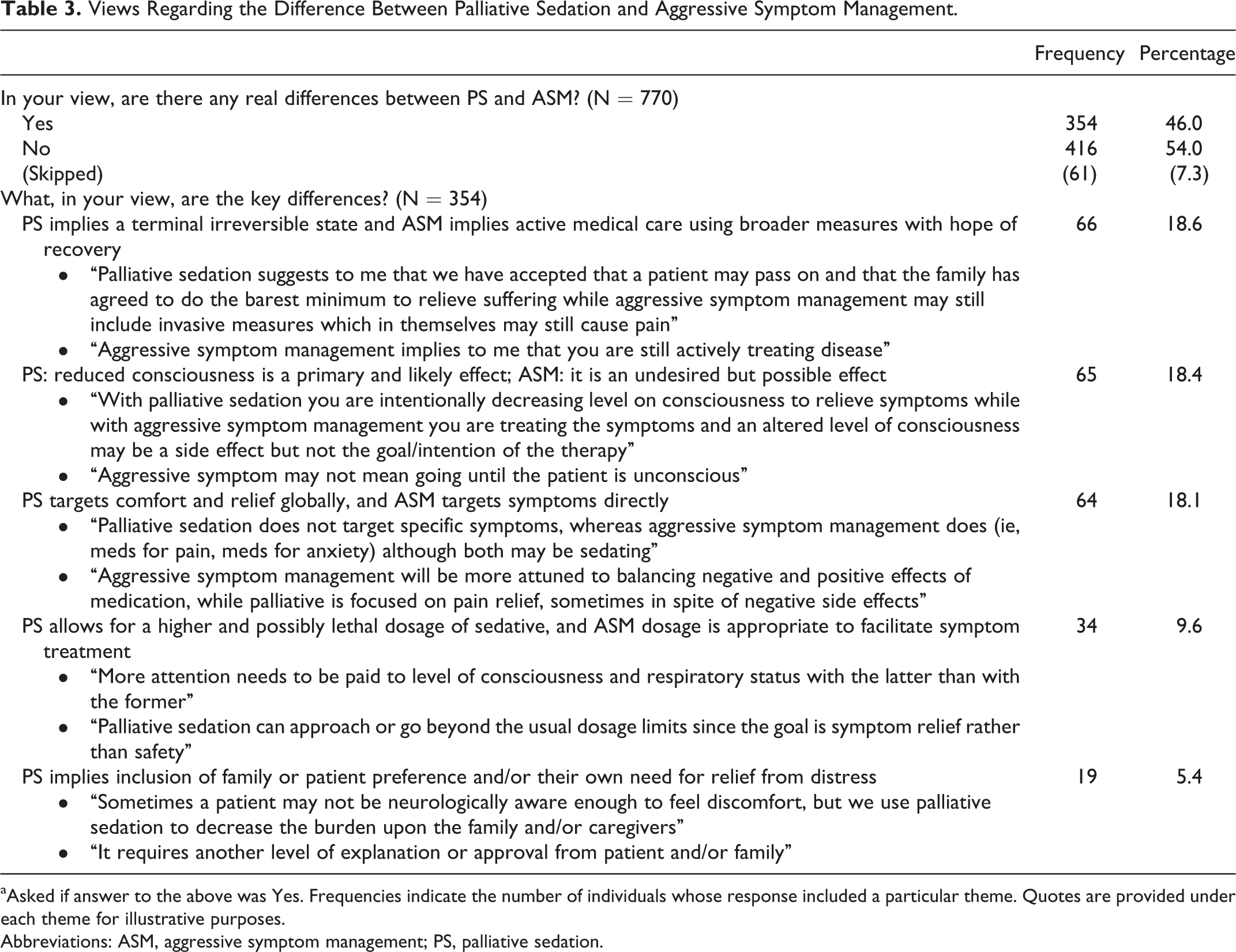
aAsked if answer to the above was Yes. Frequencies indicate the number of individuals whose response included a particular theme. Quotes are provided under each theme for illustrative purposes.
Abbreviations: ASM, aggressive symptom management; PS, palliative sedation.
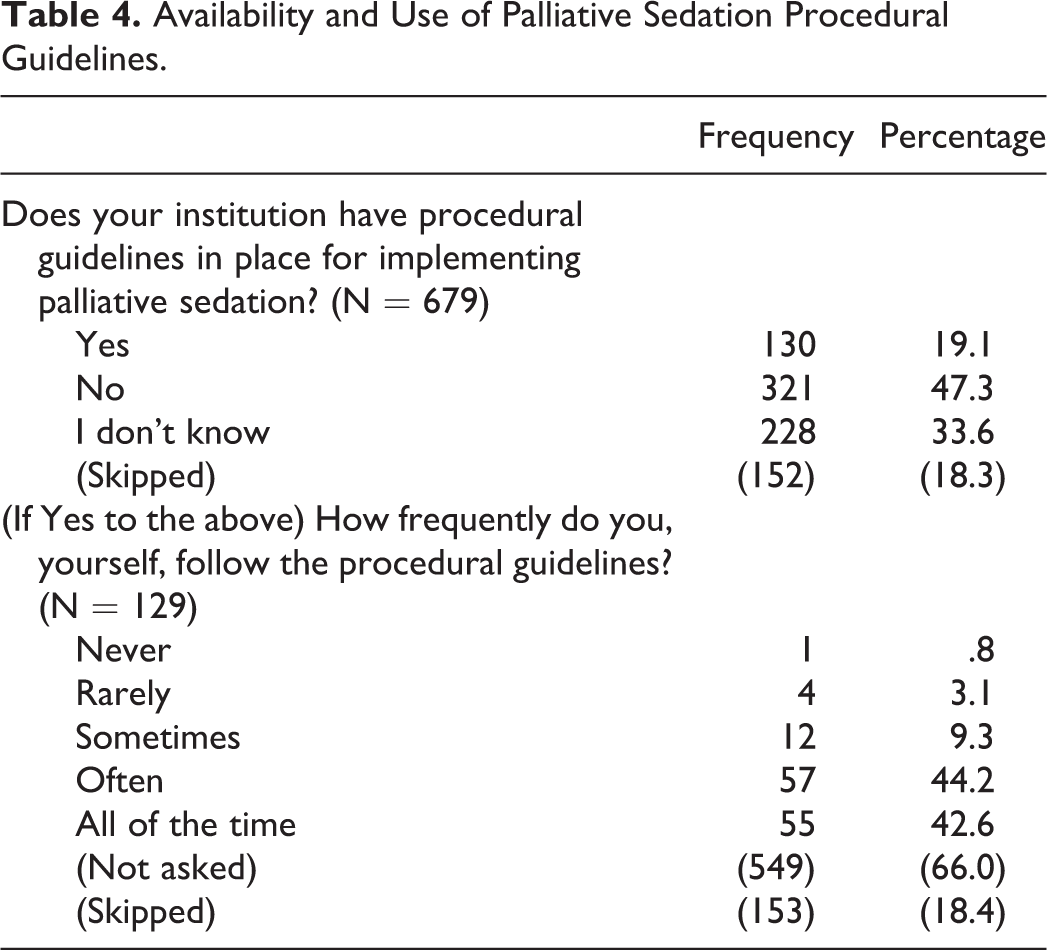
Table 4 provides the descriptive frequencies for responses to questions related to institutional and individual use of palliative sedation guidelines. It should be noted that some individuals in this group might be reporting for the same institutions.
Availability and Use of Palliative Sedation Procedural Guidelines.
Discussion
Although palliative sedation can be considered a specific and distinct intervention along the continuum of care at the end of life, our study points to various ambiguities surrounding this practice. A recent report scrutinizing the available guidelines for palliative sedation asserted that “The lack of quantitative and qualitative research on the provision of palliative sedation in the United States is not an indicator of rarity in its use but rather a sign it is not being defined as such.” 19(p9)
In our survey, palliative sedation was defined as “the use of sedative medication to relieve intolerable suffering from refractory symptoms by a reduction in patient consciousness,” 23 presuming a clear shift on the care continuum from the targeting of symptom management to the relief of suffering and comfort. Although many of the surveyed pediatric providers either mostly or completely agreed with the definition (48%), a bare majority, including 38% who partially agreed, endorsed changes. The most frequently cited concern involved the identification of a decreased level of consciousness as the goal of palliative sedation, despite the fact that the proposed definition describes this as a means to relieve intolerable suffering rather than a goal. This concern shared by some of the respondents is reflected in a recent survey by Putman et al that explored the nuances of the definition of palliative sedation with internal medicine providers and noted intentional sedation to unconsciousness is neither the norm nor broadly supported. 24
When considering the ethical concerns that surround sedation at the end of life, notably the principles of proportionality, preservation of patient autonomy, and the prevention of harm, 11 the potential to violate these ethical imperatives during the deliberate decrease in patient consciousness treads too closely to euthanasia for some practitioners. 14,25 –28 Although a great number of respondents agreed with the definition put forth, our findings indicate that some pediatric providers are more comfortable with symptom management that produces sedation proportional to the symptom distress, accepting unconsciousness as a foreseen but unintended side effect of symptom management.
Our survey also explored differences in how respondents view palliative sedation within a spectrum of care. Although aggressive symptom management was not defined, respondents were asked if they viewed palliative sedation differently from it. Half of the providers surveyed view end-of-life sedation as one broad continuum of care, perceiving no difference between aggressive symptom management and palliative sedation, whereas the other half see delineation. Distinctions proposed between them in response to the open-ended question varied considerably, further suggesting lack of consensus and the need for greater clarity.
The literature is replete with research in palliative sedation, which has a lack of consistent definition. 19,29 Our respondents frequently perceived the goal of palliative sedation to be that of deliberate sedation to unconsciousness rather than understanding that an alteration in the level of consciousness was simply a means to accomplish the goal of relief of suffering. It is not clear if their disagreement was with the practice or if they found the concept as stated in our survey insufficiently clear. Nonetheless, among pediatricians, this notion appears to be neither uniformly understood nor endorsed.
The concerns and disagreements noted by pediatricians in this survey will hopefully inform leaders in pediatric palliative care who are working toward developing more specific pediatric guidelines for palliative sedation. Yet, much can be done at an institution level to aid practicing physicians. Quill et al 11 and Gurschick et al 19 have advocated that explicit institutional-based policies are necessary to clarify what is considered acceptable practice in each institution. Utilizing established guidelines, such as those from the National Hospice and Palliative Care Organization (NHPCO), 4 institutions could develop explicit palliative sedation protocols that include important considerations such as patient selection, documentation requirements, medication choice, and duration of therapy. Over 80% of our respondents stated that their institution had no formal policy or procedural guideline for palliative sedation or that they were unaware of any such policy.
Adopting rigorous protocols could also foster open communication about end-of-life care between patients and providers, providing a mechanism to intentionally explore options with families considering palliative sedation or other end-of-life considerations. In pediatrics, children are rarely able to offer their consent or assent, leaving parents to make decisions in their best interest. Considerations around informed consent for pediatric palliative sedation warrant further exploration.
Finally, the importance of clear definition and practice of palliative sedation cannot be underestimated with regard to further research. Consistency both within and across institutions, as well as between providers, will enable thorough evaluation of the process in the literature and work toward assessing the true need for palliative sedation as a therapy at the end of life for pediatric patients. Further work is needed to better appraise palliative sedation in pediatrics, identifying its usefulness and indications outside oncology.
Study Limitations
The generalizability of our results to the larger population of US pediatric physicians in critical care, oncology, neonatology, and palliative care is threatened by the questionable accuracy of the list we used for our population. Some physicians in the population were likely not included in the list—or had incorrect e-mails—and a number of the names on the list are probably no longer part of the population. Consequently, there is a possibility of both undercoverage and overcoverage error. In addition, the low response rate achieved after sending the invitation to all members of the population list does raise concerns that our respondents differ in some systematic way from the broader population (ie, nonresponse bias). It should be noted, however, that low response rates do not necessarily equate to higher response bias, and emerging evidence is indicating that there is poor correlation between the two. 30,31 In addition, nonresponse bias may be of even less concern in physician surveys than in surveys of the general public. 32 Given these points and the fact that our respondents are represented by various ages, geographic regions, and levels of experience with palliative sedation, we believe that these results are a good initial indicator of the range of opinions and concerns regarding this important issue among our population and should be shared.
Our conclusions regarding responses to the question asking physicians to describe their views regarding the differences between palliative sedation and aggressive system management might have been biased by the fact that we provided a definition for palliative sedation but not for aggressive symptom management. A more pure assessment of respondents’ views might have been obtained by presenting the question without a definition of either.
Finally, there is a possibility that some respondents provided responses that did not, in fact, represent their true views and practices. This may have been due to uncertainty regarding the subject matter or due to a desire to remain neutral when answering questions around an ethical topic.
Conclusion
Pediatricians are increasingly likely during their career to encounter patients for whom palliative sedation constitutes an end-of-life alternative. Although varying levels of sedation are often incorporated in the management of challenging symptoms, the term palliative sedation has become a universal term incorporating all manners of sedation at the end of life. 19 Our findings indicated that the practicing pediatricians we surveyed had variable interpretations of the meaning of palliative sedation and its ethical acceptability. The development of institutional-based explicit palliative sedation protocols could lend toward clarifying acceptable practice, ensuring consistency between providers and institutions, and serve as a basis for meaningful communication and research.
Footnotes
Appendix A
Acknowledgments
The authors express our gratitude to Sarah Friebert, MD, and David E. Weissman, MD, for editorial assistance in conceptualization and design of the survey. The authors would also like to thank Jo Anne Fordham for her critical appraisal and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.