
Abstract
Background:
Palliative care services extend to meet the needs of patients with nonmalignant diseases.
Aim:
To explore the diagnoses, symptoms, and treatment of patients dying in hospice due to nonmalignant diseases, with special emphasis on amyotrophic lateral sclerosis (ALS).
Design:
A retrospective study based on a detailed analysis of patient records.
Setting/Participants:
All patients with nonmalignant diseases who died in Pirkanmaa Hospice during the period 2004 to 2013 were included.
Results:
Of the 67 patients studied, 48% had ALS, and the remaining had pulmonary (18%), cardiovascular (13%), neurologic (10%), and other (10%) diseases. Dyspnea, followed by pain and fatigue, was the most common symptom reported, increasing in frequency from admission to the last day of life (31% vs 48%; P < .05). Compared with ALS, patients with other diseases had more comorbidities (3.8% vs 1.4%, P < .001) and were more likely to have very short (≤3 days) final care periods (31% vs 9%; P < .05). During the last day of life, patients with ALS were more frequently unable to swallow (87% vs 31%, P < .001) and received significantly more antidepressants, antibiotics, and laxatives but less corticosteroids and oxygen compared to other patients. Noninvasive ventilation was used in 31% of all patients.
Conclusion:
Respiratory symptoms are important in the management of nonmalignant diseases in hospice. Especially, units taking care of ALS should be prepared to meet the special needs involved in ventilation support. In contrast to ALS, late referrals to hospice are common in patients with other nonmalignant diseases.
Keywords
Introduction
According to Finnish and international treatment guidelines, palliative care should be given to all dying patients regardless of diagnosis. 1 –3 In addition to cancer, many life-limiting diseases such as chronic obstructive pulmonary disease (COPD), heart failure, renal insufficiency, and progressive neuromuscular diseases cause symptoms that markedly decrease patient’s quality of life. 4 –7 During the past years and decades, there has been considerable improvement in the palliative care of patients with cancer, although many other patient groups still lack proper treatment guidelines. 8,9
Referring to a European Parliament report, one of the main development goals of Finland is to promote the availability of palliative care services for patients with nonmalignant diseases. 10 Compared to cancer, however, the end phases of other life-limiting diseases are particularly heterogeneous and more difficult to predict. 11 The symptoms and needs especially during the very last days of life in patients with nonmalignant diseases are largely unknown.
The main goals of this study comprised mapping out the spectrum of nonmalignant diseases cared for in hospice, the symptoms these patients have, and the care they receive during the last days of life. As a great majority of nonmalignant hospice patients in Finland have amyotrophic lateral sclerosis (ALS), the characteristics of this patient group were especially emphasized.
Methods
All consecutive patients admitted to Pirkanmaa Hospice from January 2004 to December 2013 were evaluated. Altogether, there were 2640 inpatient care periods and 2127 patients died during the years studied. After excluding patients with cancer, the care documents of those who died due to a nonmalignant disease were analyzed.
Data were collected on demographic characteristics, admissions, diagnoses, symptoms, medication, and other treatment, including nutritional routes, oxygen, and noninvasive ventilation (NIV). The presence of a chaplain, physiotherapist, and family members during the hospice stay were also recorded.
All symptoms reported by physicians or registered nurses experienced in hospice care were evaluated from the patient records. The symptoms were routinely evaluated in every patient on admission and thereafter on a daily basis. Standardized Edmonton Symptom Assessment Scale 12 (ESAS) tool was used to evaluate the presence of common symptoms when appropriate. However, as most patients in this cohort were not able to answer structured questionnaires, especially during the last 24 hours of life, single questions in the presence of symptoms and nonverbal assessment were also accepted for evaluation. The presence of a symptom was defined as being reported in the care documents.
The number of comorbidities was assessed by the number of diagnoses found in the patient’s medical records. The previous care units referring patients to the final hospice period were analyzed from the referral forms. These units were further categorized into 4 groups: homes, specialized health care units (tertiary and secondary health care hospitals), primary health care hospitals, and other health care units (nursing homes and rehabilitation centers). Very short (≤3 days) and very long (>90 days) care periods prior to death were recorded in order to assess the predictability of forthcoming death and factors possibly leading to suboptimal timing and duration of end-of-life care. The study was approved by the Regional Ethics Committee of Tampere University Hospital.
Statistical Analysis
Descriptive statistics were used to analyze the data on demographic characteristics, admission details, symptoms, medication, and treatment. Comparison of groups (ALS vs other diseases) was performed using Pearson χ2 or Fisher exact tests for differences in proportions of categorical variables and Mann-Whitney U test for differences in continuous variables. McNemar test was used for differences in proportions of categorical variables at different points in time. Statistical significance was defined as P < .05. All analyses were carried out using SPSS version 21.0 software.
Results
During the years studied, 67 patients died due to a nonmalignant disease (3.1% of all patients), with a total of 91 inpatient care periods before death. Characteristics of the patients are shown in Table 1. About half of the patients had ALS, the other most common diagnoses being COPD and lung fibrosis. At the time of death, the mean age of the patients with ALS did not significantly differ from that of patients with other diseases (69 vs 73 years, P = .1), but patients with ALS were more often women (75% vs 49%, P < .05). The mean number of comorbidities in patients with ALS and other nonmalignant disease was 1.4 (95% confidence interval [CI], 0.9-1.9) and 3.8 (95% CI, 3.0-4.6), respectively (P < .001).
Demographic Characteristics of Study Patients.
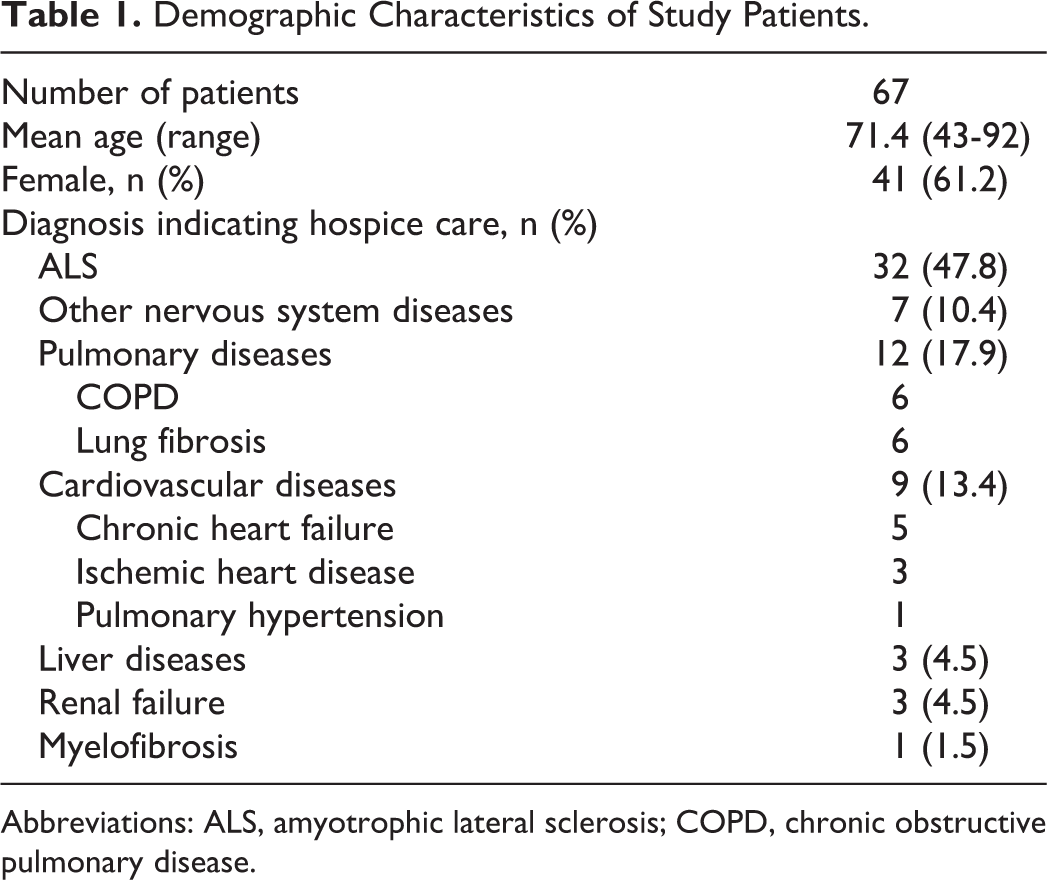
Abbreviations: ALS, amyotrophic lateral sclerosis; COPD, chronic obstructive pulmonary disease.
Symptoms and Medication
The prevalence of the most common symptoms during the first and the last 24 hours of the final care period is presented in Figure 1. In addition, depression, dry mouth, or loss of appetite were occasionally reported (<3% of the patients). The occurrence of dyspnea, fatigue, and pain all increased toward death, although the increase was statistically significant only for fatigue and dyspnea. More than 1 symptom was reported in 69% and 84% of the cases during the first and the last day, respectively (P < .05). We found no statistically significant differences in the prevalence of symptoms between patients with ALS and others. During the last 24 hours, dyspnea occurred in 46.9% of patients with ALS and 48.6% of the others, while the same percentages for pain were 46.9% and 37.1%, respectively.
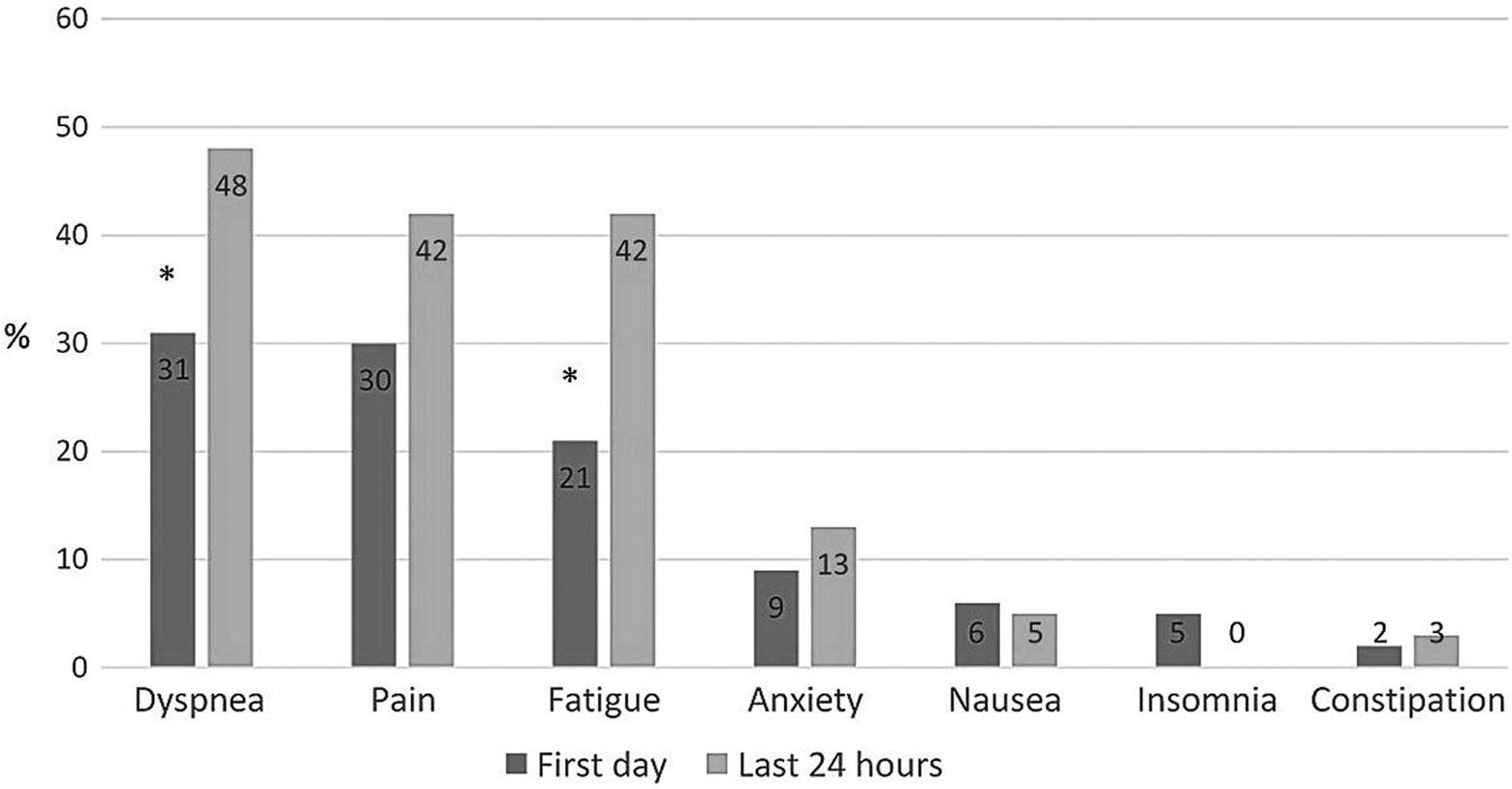
Proportion of patients with different symptoms reported during the first and last 24 hours of their final care period. *P < .05.
The drugs most commonly given to the patients are shown in Figure 2. Among these, the use of opioids (regularly or as needed) and anticholinergic drugs significantly increased toward death. During the last 24 hours, opioids to be given in need had been prescribed to nearly all patients (98%), while 75% of them actually received the drug.
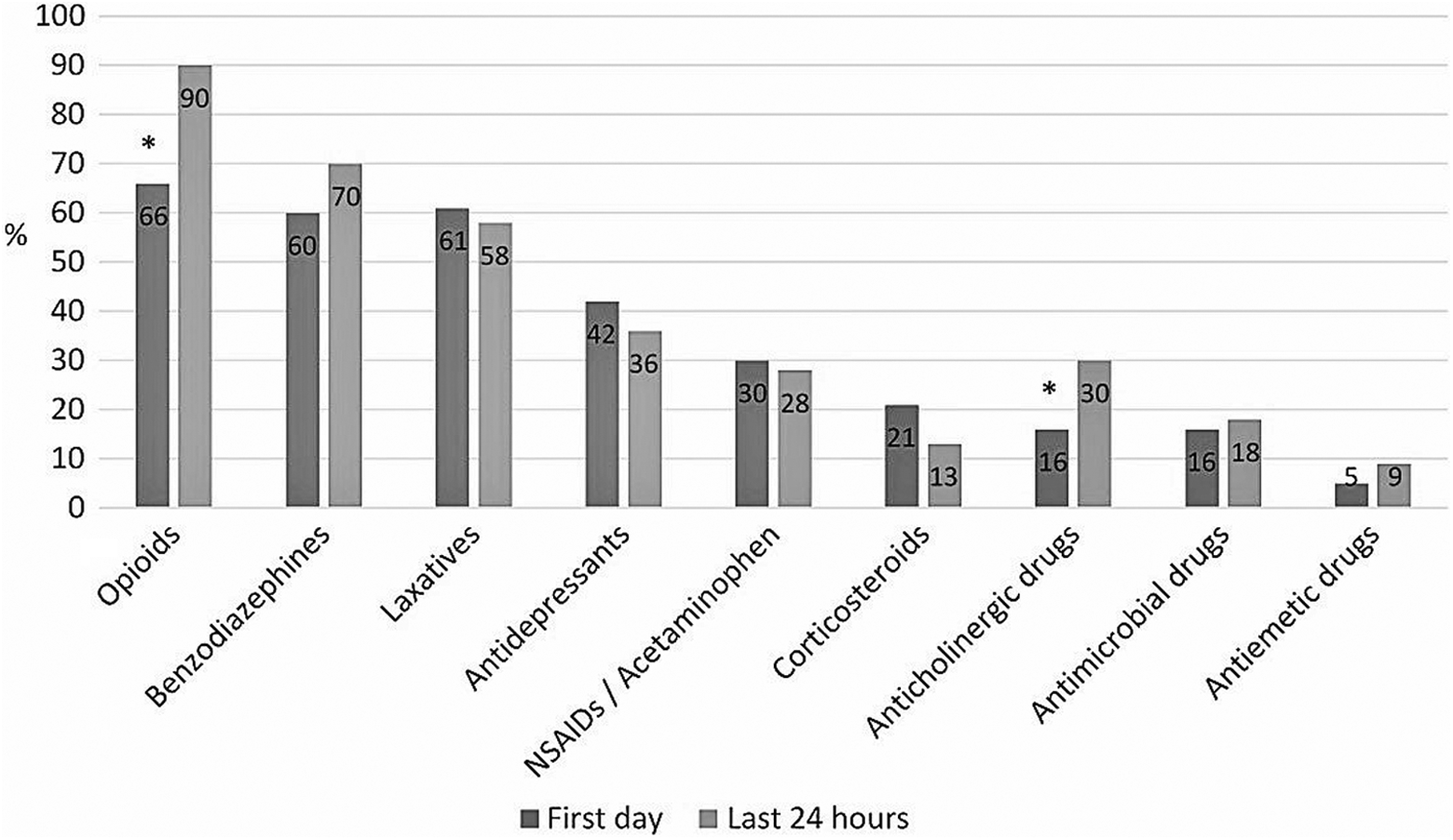
Proportion of patients who received different drugs during the first and last 24 hours of their final care period. *P < .05.
End-of-Life Care in ALS Compared With Other Diseases
Differences regarding end-of-life care among patients with ALS and other nonmalignant diseases are presented in Table 2. Patients with nonmalignant diseases other than ALS were more likely admitted from specialized health care units (74% vs 41%, P < .05) and more often had a very short (<3 days) final care period, although there was no significant difference in the proportions of patients having 2 or more hospice care periods (17% vs 25%, P = .4).
End-of-Life Care of Patients With ALS and Other Nonmalignant Diseases.
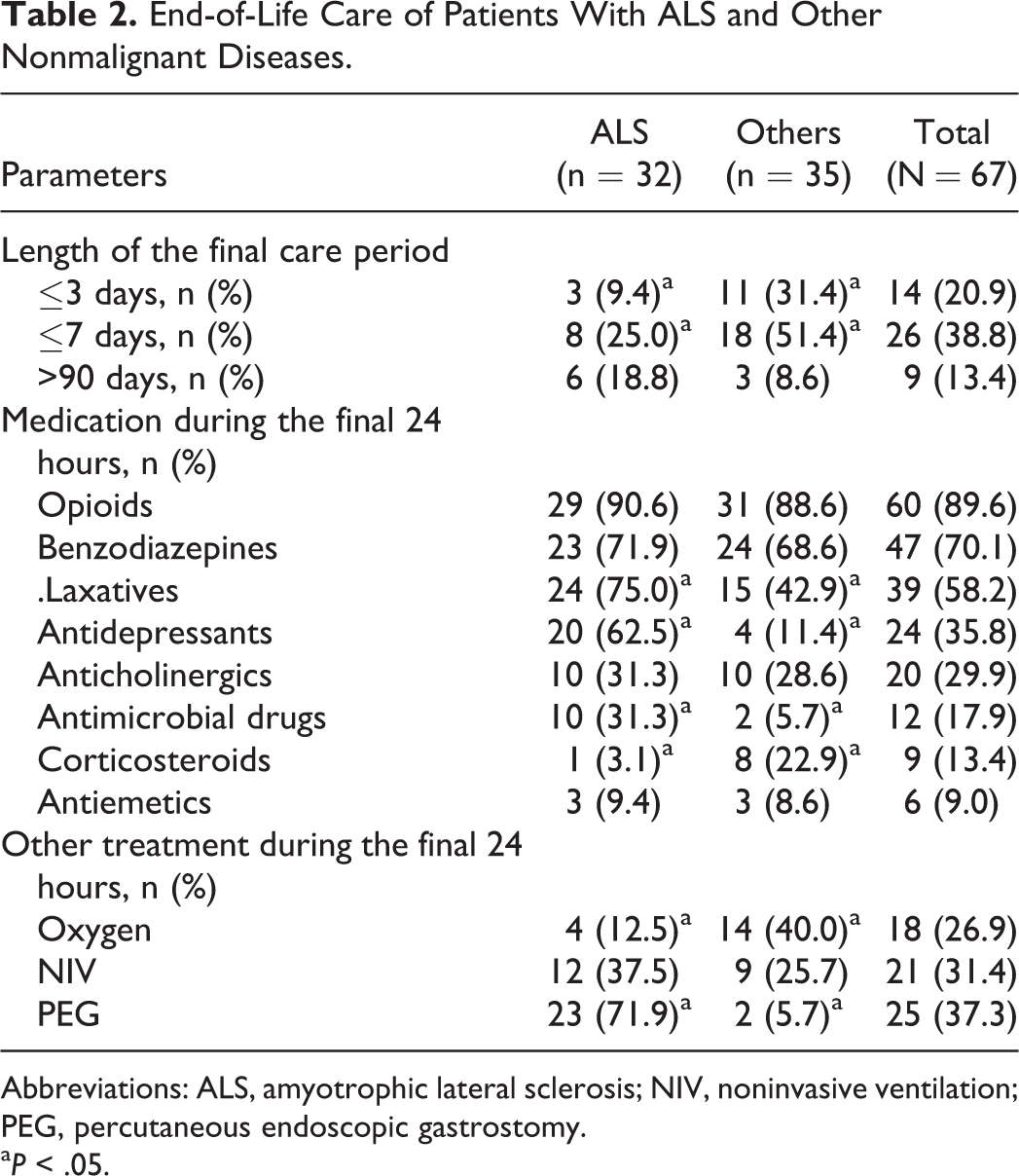
Abbreviations: ALS, amyotrophic lateral sclerosis; NIV, noninvasive ventilation; PEG, percutaneous endoscopic gastrostomy.
a P < .05.
During their last 24 hours, patients with ALS received more antidepressants, laxatives, and antimicrobial drugs but less corticosteroids compared to other groups. Amitriptyline was given to 50% of patients with ALS and to 2.9% of the remainder. Furthermore, other antidepressants were likewise given more frequently to patients with ALS (31% vs 5.7%, respectively, P < .05).
More than one-third of patients with ALS used NIV during the last 24 hours of their life, whereas oxygen was more often given to patients with other diseases. Patients with ALS were more often incapable of swallowing (87% vs 31%, P < .001), and most had a percutaneous endoscopic gastrostomy tube as the main nutritional and medical route.
Patients with ALS met a physiotherapist more often during their hospice stay (84% vs 60%, P < .05), while there was no such difference regarding psychological or existential support given by chaplains (59% vs 46%, P = .3). Most patients met their family members during the final 24 hours, with no difference between patients with ALS and those with other diseases (91% vs 74%, P = .08).
Discussion
We here evaluated the end-of-life care of nonmalignant diseases in a hospice. Our special interest was in ALS, as little is known as to the management of patients with ALS during the final day of life. Dyspnea, followed by pain and fatigue, was the most frequently reported symptom both among patients with ALS and others, although these groups differed significantly in terms of treatment. Furthermore, patients with other diseases had shorter hospice stays and were more likely to have multiple comorbidities.
Only 3.1% of the patients who died in the hospice during the 10-year study period had nonmalignant diseases. The proportion is lower than those reported from other palliative care units in general, although the numbers vary greatly from 3.5% to 63.5%. 13,14 During the years studied, Pirkanmaa Hospice (the only hospice in the area) took care of about 5% of all the decedents in the county of Pirkanmaa. 15 Thus, it is likely that only the most severe cases of nonmalignant diseases were referred to hospice.
A relatively high proportion (48%) of patients in our study had ALS, despite its low prevalence in the general population. 16 Similar findings have been reported in earlier studies. 13,17,18 This might be due to the physically, psychosocially, and emotionally challenging care of ALS with its inevitably progressive nature. 19,20 Special management of ALS in a hospice is reasonable, since palliative care interventions are shown to improve the quality of life both in patients with ALS and their caregivers. 21
Many patients with diseases other than ALS were actually patients having multiple diseases with many comorbidities. We would suggest that this involved challenges to the prognostication of the final stages of life, which in turn may have led to late referrals and very short hospice stays among these patients. We selected 3 days as the limit of unreasonably short hospice stay, since this definition has also been used in the context of underutilization of hospice care by the National Quality Forum and as a sign of overaggressive treatment prior to death in a study by Temel and associates. 22,23 Changes in the place of care during the very last days of life are usually futile, and it is unlikely that a patient benefits markedly from hospice care in such a short time. More studies and education on prognostication, including recognition of the dying phase, should be considered when planning palliative care for patients with nonmalignant diseases.
Dyspnea proved to be the most frequent symptom, being reported in almost half of the patients with ALS as well as other diseases. This is in line with earlier findings singling out dyspnea as the most common symptom in the ALS and the COPD patient group. 5,24 Respiratory symptoms in general have been shown to be the most common reason for end-of-life hospitalization in patients with nonmalignant diseases and a more notable problem compared to patients with cancer. 13,25 Hospices taking care of patients with nonmalignant diseases should thus be prepared for the advanced management of respiratory symptoms.
The great number of patients receiving opioids and benzodiazepines in our study is in line with a previous report by Oliver and associates. 26 This is probably due to the high and temporally increasing prevalence of dyspnea and pain among these patients. Similarly, the growing use of anticholinergics toward death was probably due to increased respiratory secretions and death rattle associated with forthcoming death. 27 Patients with ALS rarely used medical oxygen, since, due to the nature of the disease, they basically had hypoventilation rather than hypoxemia. However, 38% of patients with ALS were using NIV during their last day, which is more than that reported in the study by Oliver and group. 26 A relatively high proportion of the patients with other nonmalignant diseases were using NIV as well. In general, NIV improves survival and enhances quality of life in ALS, whereas its use in the dying phase and in the palliative care of other diseases is more controversial. 28,29 Nevertheless, withdrawing NIV or using it as a comfort-only measurement until death requires special skills, resources, and expertise. 30,31
Despite the disputed role of antibiotics in end-of-life care, relatively many patients with ALS received antibiotics during their last 24 hours. This might indicate that even in the hospice environment, it may be difficult to differentiate infections from the death process, although antibiotics were presumably prescribed to alleviate symptoms such as excessive mucous amounts rather than to prolong the patient’s life expectancy.
The use of antidepressants among the ALS group was surprisingly high. However, this included amitriptyline, which was probably prescribed mainly for indications other than depression, for example, sialorrhea, insomnia, and pseudobulbar emotional lability. 32 Nevertheless, even excluding tricyclic drugs, patients with ALS were treated with antidepressants more frequently than the others. This is probably explained by 2 facts. First, depressive symptoms are frequent in patients with ALS due to the devastating nature of the disease. 33 Second, the easier medical route with a gastrostomy tube might have prevented the appropriate discontinuation of these orally administrated drugs even in the dying phase.
Almost all patients with ALS met a physiotherapist compared with 60% of other patients. This might be not only due to longer hospice stays but also due to the respiratory problems and muscular weakness with restricted mobility that appears before failure of other organs in patients with ALS. The physiotherapist has long been a part of the multidisciplinary team in the Pirkanmaa Hospice, which may also increase the use of physiotherapy as an important component in treatment.
In addition to the probable difficulties in prognostication among other nonmalignant diseases, there would seem to be challenges in the recognition of the dying phase and withdrawal of inappropriate therapies (antibiotics, antidepressants, and NIV) also in patients with ALS. Further studies are thus needed not only to find the best treatment modalities for end-of-life care but also to identify the main factors involved in prognostication during the final days of life in patients with nonmalignant diseases.
We acknowledge some limitations to the present study. First, we evaluated symptoms as they were reported in the care documents, which might differ from patient’s subjective experience, and this definition for the presence of a symptom may have low sensitivity or specificity. However, as symptoms were routinely assessed by the registered nurses and palliative care physicians specially educated in symptom evaluation, we would suggest that the most important symptoms were brought out and reported in the documents. Furthermore, many patients were in a very weak clinical condition, necessitating the use of single questions in the presence of various symptoms or nonverbal assessment as the only possible means of symptom evaluation, especially during the final hours of life and with patients having advanced ALS.
Second, the total number of patients in this study was rather small, although the number of patients with ALS was comparable to those in earlier studies. Third, we arbitrarily chose to compare ALS with other nonmalignant diseases, the clinical relevance of which might be debated. Nevertheless, our original aim was to describe the hospice care of different groups of nonmalignant diseases. When ALS showed up to be the largest patient group, we found it important to further highlight the unique nature of ALS and to compare it with other diseases to enable planning of hospice care for patients with different nonmalignant diseases.
Conclusion
Respiratory symptoms are common during the dying phase in patients with nonmalignant diseases. Especially, units taking care of patients with ALS should be prepared to meet the special needs involved in ventilation support. In contrast to ALS, patients with other nonmalignant diseases have many comorbidities and late referrals to hospice. This may call for better recognition of the dying phase.
Footnotes
Acknowledgments
The authors sincerely thank the staff of the Pirkanmaa Hospice for data entry and help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.