
Abstract
Background:
Palliative care service (PCS) has been shown to be utilized less in patients with leukemia and malignant lymphoma than in those with solid tumors. Previous studies have suggested hematologists’ limited awareness of PCS as one of the reason for low PCS referral in hematology. However, little is known about such an awareness and potential barriers to collaboration between hematologists and PCS.
Aim:
The present study aimed to assess ematologists and palliative care specialists’ perception about the roles of the hospital-based palliative care team (HPCT) and the barriers to collaboration between hematologists and palliative care teams on relapse or refractory leukemia and malignant lymphoma patients’ care
Materials and Methods:
A qualitative study was conducted using semistructured interviews with hematologists and palliative care specialists recruited from a hospital that provides hematology and palliative care by the HPCT. Data were evaluated via content analysis.
Results:
The study included 11 hematologists and 10 palliative care specialists. Our results revealed that they shared many common perceptions about the roles and expectations of the HPCT. Additionally, 7 categories of barriers to collaboration were identified, including not feeling the need to refer, the difficulty in referral timing, the lack of aggressive approach, the negative image of the HPCT, the need for hematologic malignancy-oriented management, the lack of communication, and others.
Conclusion:
We have identified hematologists’ and palliative care specialists’ perceptions of the HPCT’s roles and the barriers to their collaboration. A better understanding of such barriers may lead to effective collaboration between hematologists and the HPCT.
Keywords
Introduction
The development of molecular target drugs and improved chemotherapy regimens have increased both remission and survival rates of patients with leukemia and malignant lymphoma in the recent years. However, many patients continue to endure relapsed disease, be in the refractory phase, or become progressively ill and eventually die from their diseases. 1 -4 They often need additional chemotherapy, frequent blood transfusion, antimicrobials requirement, and G-CFS supports resulting in extended hospitalization. 5 -7 Consequently, patients with relapse or refractory leukemia and malignant lymphoma usually experience physical, emotional, social, and spiritual distress associated with disease progression and therapy-related complications. 6,8,9 With this in mind, the handbook entitled National Institute for Clinical Excellence: Guidance in Cancer Services Improving Outcomes in Haematological Cancers The Manual recommends that there should be effective integration between palliative care and hemato-oncology services throughout a patient’s illness, not just when he or she reaches the terminal phase, and that adequate palliative care is important to maximize quality of life (QOL). 10 Nevertheless, many studies have shown that palliative care service (PCS) is utilized less in patients with leukemia and malignant lymphoma than in those with solid tumors. 11 -14 Additionally, access to PCS is often provided to patients with leukemia and malignant lymphoma later than to those with solid tumors. 15
McGrath and Holewa also suggested a lack of hematologists’ understanding about palliative care via research interviews with nurses. 16 Moreover, Auret et al reported that hematologists were concerned about the lack of flexibility in continuing treatments that were considered “active” by palliative care but “symptom control” by hematologists. 17 Although hematologists’ awareness of PCS is thought to be one of the reasons for low referral to PCS in hematology, no studies are available on hematologists’ perception of PCS’s roles and the barriers to collaboration between hematologists and PCS from their own perception. A better understanding of such barriers may aid in improving collaboration. Thus, we hypothesized that hematologists and palliative care specialists have different perceptions on PCS, creating an obstacle to patient referral to PCS. Since the majority of patients with relapse or refractory leukemia and malignant lymphoma are hospitalized, the present study targeted the hospital-based palliative care team (HPCT).
We examined the perception of hematologists and palliative care specialists about the roles of the HPCT and the barriers to collaboration between hematologists and palliative care teams on relapse or refractory leukemia and malignant lymphoma patients’ care.
Method
Participants and Recruitment
Hematologists and palliative care specialists who are board certified in their specialty and work for a hospital providing hematology medicine services or a HPCT were recruited. All participants had been working in the areas of expertise for a minimum of 5 years and were identified by the snowball sampling technique.
Data Collection
In-depth interviews were conducted to identify attributes of the barriers to collaboration between hematologists and palliative care teams. Face-to-face semistructured interviews were scheduled in private rooms from August to December 2011. All interviews were conducted by one researcher (MM), recorded, fully transcribed, and supported by detailed field notes.
We asked all participants about the roles and expectations of the HPCT, and the barriers to collaboration between hematologists and palliative care teams in relapse or refractory leukemia and malignant lymphoma patients’ care. Demographic details of all participants including their age, the type of facility they worked in, and their years of clinical experience in their specialty were recorded. In addition, we asked palliative care specialists about the annual number of HPCT referrals from the whole hospital and the hematology unit alone.
Analysis
Interview data were transcribed verbatim from audiotapes. Content analysis was performed on the transcribed date. First, a research nurse (MM) extracted all statements related to the study topics from each transcript, such as the role and expectation for the HPCT, and the barriers to collaboration between hematologists and the HPCT. Then, under the supervision of an experienced hematology nurse (YS) and a researcher specialized in qualitative study (RO), we carefully conceptualized and categorized the text into content areas using the Content Analysis by Klaus Krippendorff. 18 The text was divided into meaning units that were then condensed, abstracted, and labeled with a code. Palliative care specialists’ and hematologists’ codes were then sorted into categories and subcategories on the basis of similarities and differences in the abstracted and coded data. Next, another qualitative researcher with experience caring for patients with hematologic malignancies (the coder) was asked to review the categorization. The rate of agreement between the researchers and the coder was 74.8%. Finally, cases with discrepancy were reviewed in consultation with the coder.
Ethical Considerations
Verbal and written explanations of the research objectives and procedures were provided to all participants, and written consent was obtained. This study was approved by the Institutional Review Board of the Graduate School of Medicine of the University of Tokyo.
Result
Characteristics of Respondent Participants
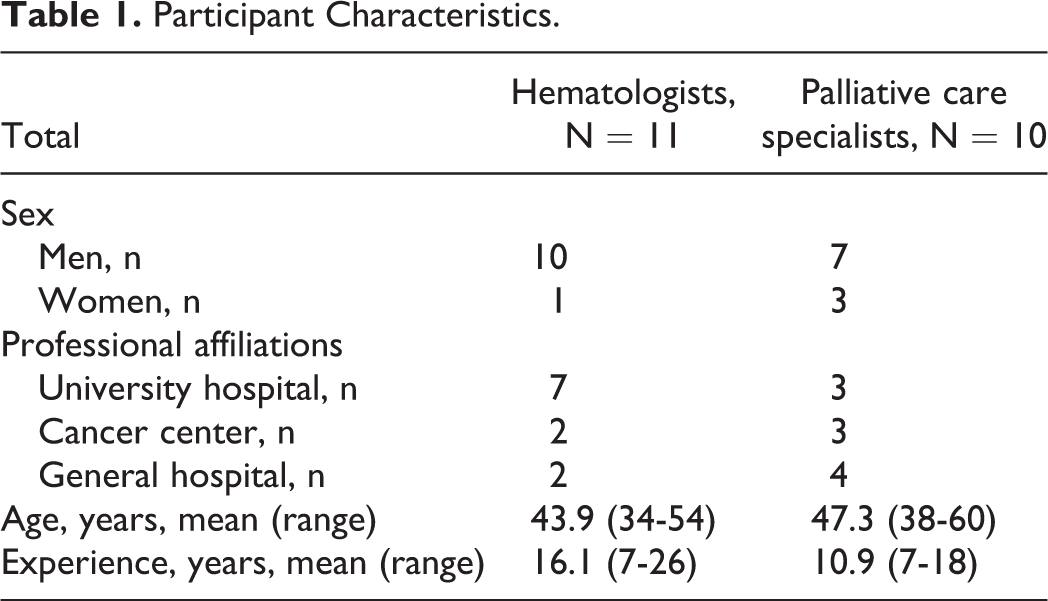
Semistructured in-depth interviews were conducted with 21 physicians, including 11 hematologists and 10 palliative care specialists. Table 1 shows the participant characteristics. The interview duration was 28 to 60 minutes. The hematologists’ age ranged from 34 to 54 years whereas that of the palliative care specialists ranged from 38 to 60 years. All participants were working in a university hospital, a cancer hospital, or a general hospital. The annual number of HPCT referrals from all departments at each hospital was 176 to 915 cases, whereas that from the department of hematology alone was 1 to 65 cases.
Participant Characteristics.
Perception of the Roles and Expectations for the HPCT
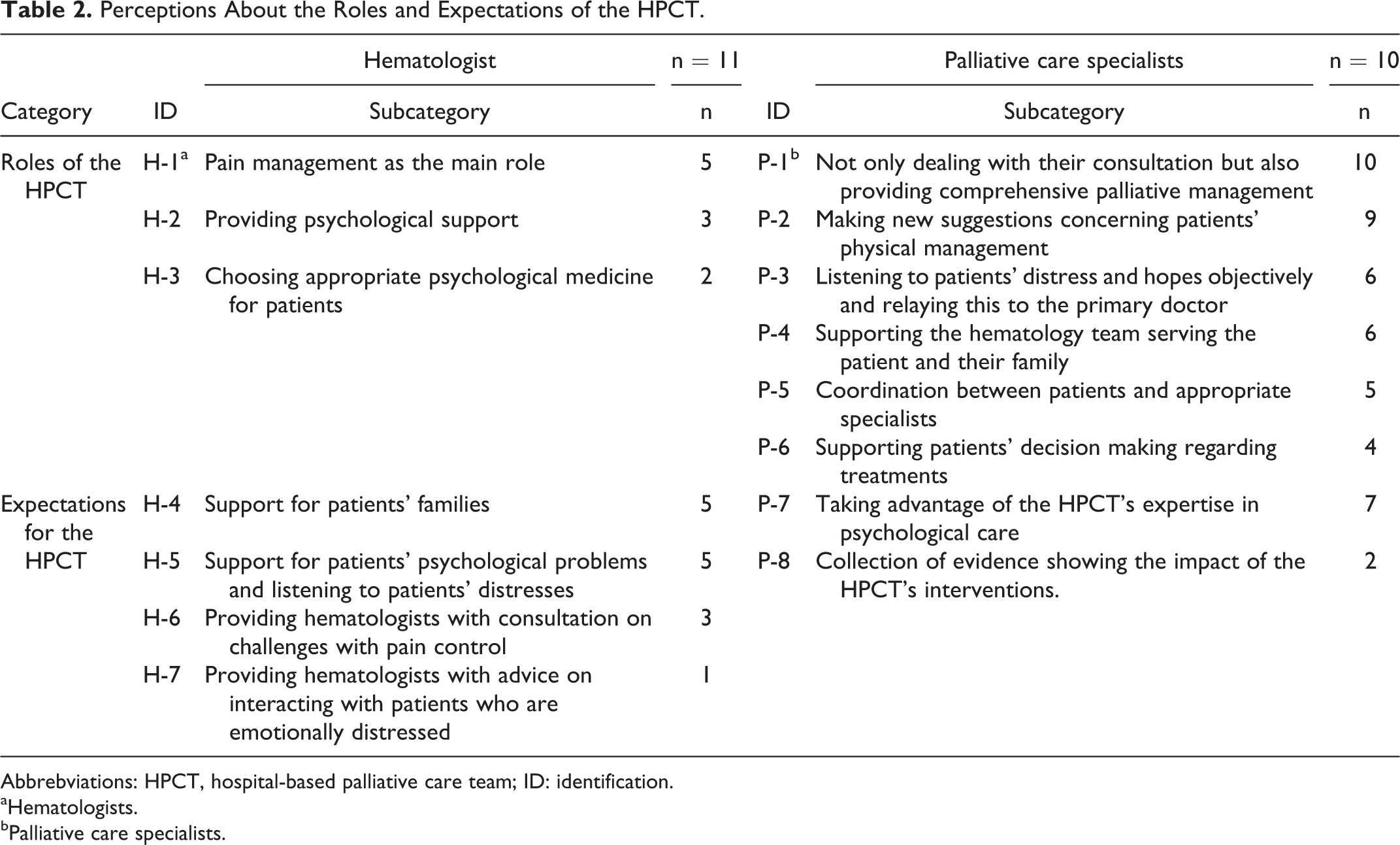
Hematologists’ and palliative care specialists’ perceptions about the roles of the HPCT are shown in Table 2. We have indicated a subcategory of hematologists as “H-number” and a subcategory of palliative care specialists as “P-number.”
Perceptions About the Roles and Expectations of the HPCT.
Abbrebviations: HPCT, hospital-based palliative care team; ID: identification.
aHematologists.
bPalliative care specialists.
Five hematologists indicated H-1 (the main role of the HPCT is pain management), and 9 palliative care specialists indicated P-2 (making new suggestions concerning physical management of patients). On the other hand, all palliative care specialists indicated P-1 (not only dealing with their consultation but also taking on comprehensive palliative management).
Regarding the expectations for the HPCT, 5 hematologists indicated H-4 (support for patients’ families) and H-5 (support for patients’ psychological problems and listening to patients’ distress), whereas 7 palliative care specialists indicated P-7 (take advantage of PCT expertise in psychological care).
Barriers to Collaboration Between Hematologists and the HPCT
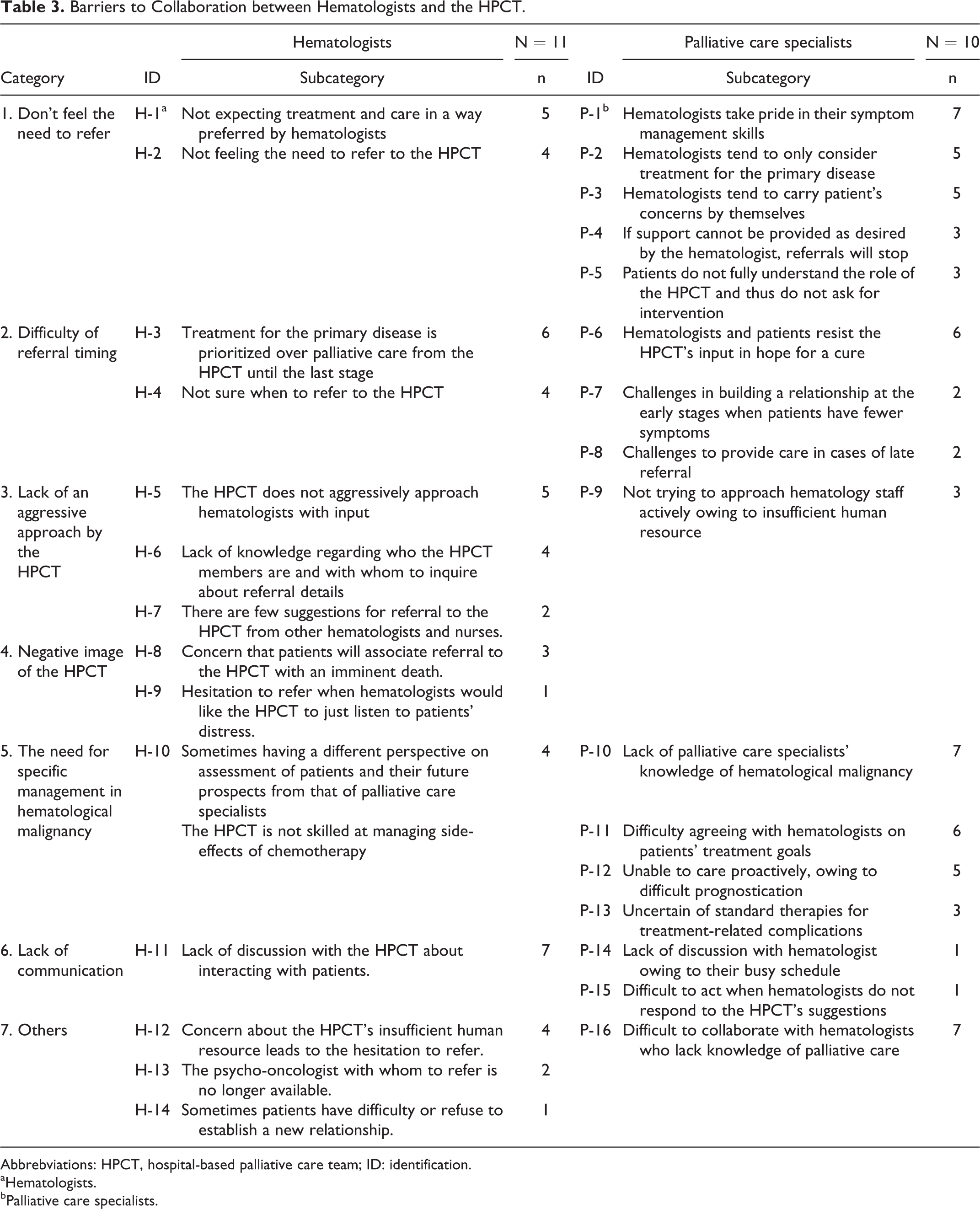
Our content analysis revealed 14 barriers listed by hematologists and 16 by palliative care specialists (Table 3). We divided these barriers into the following 7 categories:
Barriers to Collaboration between Hematologists and the HPCT.
Abbrebviations: HPCT, hospital-based palliative care team; ID: identification.
aHematologists.
bPalliative care specialists.
Don’t feel the need to refer: Both hematologists and palliative care specialists mentioned that hematologists often do not require much intervention by the HPCT. Five hematologists indicated H-1 (not expecting treatment and care in a way preferred by hematologists) and 7 palliative care specialists indicated P-1 (hematologists take pride in their symptom management skills) or P-2 (hematologists tend to only consider treatment of the primary disease).
Difficulty of the timing of referral: Both hematologists and palliative care specialists identified the timing of referral as a barrier to collaboration between hematologists and the HPCT. More than half of the hematologists interviewed indicated H-3 (the treatment of primary disease is given priority over palliative care from the HPCT until the last stage). Similarly, more than half of the palliative care specialists indicated P-6 (hematologists and patients resist HPCT input when they hope to be cured).
Lack of an aggressive approach by the HPCT: Five hematologists indicated H-5 (the HPCT does not aggressively approach hematologists with input). They listed not only the timing but also the proposal of referral as barriers to collaboration between hematologists and the HPCT.
Negative image of the HPCT: A few hematologists identified the image of the HPCT as a barrier to HPCT referral by indicating H-8 (concern that patients will associate referral to the HPCT with imminent death).
The need for specific management in hematologic malignancy: Four hematologists were concerned about proper support for patients with hematologic malignancy by indicating H-10 (sometimes having a different perspective on assessment of patients and their future prospects from palliative care specialists). Alternatively, 7 palliative care specialists indicated P-10 (lack of palliative care specialists’ knowledge of hematological malignancies). Moreover, more than half of the palliative care specialists indicated P-11 (difficulty agreeing with hematologists on patient’s treatment goals) and P-12 (unable to care proactively, due to difficult prognostication).
Lack of communication: A lack of communication was mentioned more often by hematologists than by palliative care specialists. Seven hematologists indicated H-11 (lack of discussion with the HPCT about ways of interacting with patients).
Others: Furthermore, 4 hematologists indicated H-12 (concern about the lack of HPCT manpower, so hesitation to refer) and 7 palliative care specialists indicated P-16 (difficult to collaborate with hematologists who have a lack of knowledge of palliative care).
Discussion
The present study is, to our knowledge, the first to clarify the barriers to collaboration between referring hematologists and the HPCT simultaneously in this area. We confirmed that the perception of hematologists and palliative care specialists about the roles of the HPCT had common points and different points. Additionally, we identified 7 categories of barriers to collaboration.
First, we hypothesized that hematologists and palliative care specialists have different perceptions about the HPCT, creating an obstacle to patient referral to the HPCT. Nearly half of the participating hematologists mentioned pain management, support for patient’s family, and patients’ psychological problems as a role of palliative care team. These roles are equivalent comprehensive palliative management which all palliative care specialists mentioned as their roles. The result of this study suggests that as common points, both hematologists and palliative care specialists recognize the roles of the HPCT.
Therefore, it is suggested that a difference in perception between hematologists and palliative care specialists about the HPCT is likely not to be obstacles to referral. Besides, our study also indicates the need for more support for patients’ psychological problems. Hosaka et al reported that because patients with hematologic malignancy tended to restrain their anxiousness and strain, it was challenging to identify their psychiatric symptoms. 19 Additionally, Zimmermann et al reported that 41% of patients with acute leukemia rated their pain as moderate to severe, despite the frequent use of opioid analgesics and that no patients with moderate-to-severe pain were referred for PCS, while only 13% of those with serious worry/sadness were referred to psychiatry/psychology within 1 month of such an assessment. 20 Intense pain was associated with other symptoms such as the lack of appetite, fatigue, nausea, and psychological distress as in patients with solid tumors. 21 -23 In patients with a hematologic malignancy, pain is thought to cause the potential symptom similar to those with solid tumors. It is therefore important that the HPCT addresses comprehensive palliative care in patients with hematologic malignancies.
Barriers to Collaboration Between Hematologists and the HPCT
Nearly half of the hematologists interviewed indicated that they did not expect treatment and care in a way preferred by hematologists. Hematologists often conduct treatment for leukemia or lymphoma malignancy concurrently with the management of side effects and symptoms. 17,24 Similarly, a previous study reported that hematologists felt such comanagement cannot be expected from palliative care specialists. 17 Contrary to this notion, palliative care specialists recognized that hematologists required fewer referrals to the HPCT because they took pride in symptom management skills and were more likely to attempt resolving the patient’s concerns by themselves.
Hematologists remarked that they expected limited care in a way preferred by them from the HPCT, whereas they expected the HPCT to support patients’ family, patients’ psychological problems, and patients with intractable pain. Palliative care specialists indicated that they could provide comprehensive palliative management and propose new suggestions for the physical management of patients, whereas it was a future issue if they could exert expertise in psychological care. A retrospective case comparison study involving 320 inpatients with cancer demonstrated that there was a significant improvement in physical symptoms, such as pain and fatigue, and psychological symptoms, such as insomnia and depression, as a result of the care by the HPCT. 25 In addition, other study targeting elderly patients with Acute Myeloid Leukemia (AML) had again pointed out the psychological burden of patients with leukemia and psychological support care importance of palliative care collaboration. 7 , 26 Therefore, symptom management is where patients can benefit from the intervention of the HPCT. These results suggest that collaboration between hematologists and HPCT could lead to early referral to HPCT for effective psychological care when the HPCT can demonstrate their expertise in comprehensive and physical management of patients with intractable pain, while hematologists better appreciate the roles of HPCT.
In this study, hematologists and palliative care specialists felt it was difficult to refer patients to the HPCT during intent-to-cure treatment. Our findings resonate with previous research. 11,16,27 Previous studies in patients with solid malignancies showed that early referral to the HPCT improves patients’ QOL. 28 -30 In patients with hematologic malignancies, there is a possibility that early intervention by the HPCT is effective. As there is hope for a response in advanced hematologic malignancies with intensive salvage therapies and allogeneic or autologous stem cell transplants, many patients remain in a curative system until their death. Alternatively, curative treatment transitions to QOL improvement in other cases. It is often difficult to identify the timing of transition between the curative, life-prolonging, and palliative phases of disease in many patients. 7,31,32 Hematologists in this study recognized the difficulty in such timing and the need for a liaison between hematologists and the HPCT.
Hematologists indicated that it was difficult to identify the timing of referral and that no one within the care team proposed a HPCT referral. This finding suggests that a health professional who acts as a liaison between hematologists and the HPCT is needed. A previous study noted palliative care teams provide an additional layer of support to patients, family caregivers, and the primary medical team through close attention to symptoms and emotional, practical, and spiritual needs. Barriers to routine palliative care comanagement in hematologic malignancies include persistent health professional confusion about the role of palliative care and its distinction from hospice; inadequate availability of palliative care provider capacity; and widespread lack of physician training in communicating about achievable goals of care with patients, family caregivers, and colleagues. 33 Furthermore, a qualitative study involving 19 nurses working in hematology acute care revealed that, in most cases, they noted clear clinical indications of terminal stage. 34 The finding of this study suggests that a nurse can take a leading role in identifying when comprehensive palliative management should be prioritized for a patient. Besides, a previous study showed that maintaining good communications within an interdisciplinary team is effective for the assessment of patients’ QOL in a palliative setting. 35 -37 From these findings, it is suggested that good communications and a more significant role of the care nurse could lead to better collaboration between hematologists and the HPCT.
A questionnaire study showed that the negative image of palliative care by patients and their families was one of the barriers to receiving care. 38 In this study, a few hematologists were concerned about patients associating referral to the HPCT with imminent death. A previous survey revealed that oncologists and mid-level providers preferred the term supportive care and indicated that they were more likely to refer patients on active primary and advanced cancer treatments to a service named supportive care. 39 Therefore, it may be necessary to paraphrase and provide an impression to patients that “palliative care” aims to improve the QOL, such as pain relief and quality of sleep.
More than half of the participating palliative care specialists and a few hematologists reported that it was difficult to reach an agreement on patients’ treatment goals owing to the distinct medical culture between each department. This could be the reason for the ambiguous point of transition between the curable to palliative phases of disease because the treatment of hematologic malignancy involves concurrent symptom relief and side effect management. Furthermore, palliative care specialists mentioned the lack of knowledge on hematological malignancy. As hematologic malignancy only represents 5% to 8% of cancers, 40 they only see a few patients with these conditions per year. Since they could be less familiar with hematologic malignancies, they may hesitate to suggest active intervention. Therefore, it is necessary for hematologists and palliative care specialists to discuss a patient’s condition from their specialized viewpoints and the goal of medical care.
Furthermore, although more than half of the participating hematologists also mentioned the lack of communication with the HPCT about ways to interact with patients, only one palliative care specialist did otherwise, suggesting that palliative care specialists consciously communicated with hematologists. On the other hand, hematologists recognized the need to discuss with the HPCT about patients’ condition but felt there was not enough communication. These results suggest that it is necessary for a good collaboration that hematologists improve future discussion with the HPCT on patients’ condition and that the hematology team staffs communicate with the HPCT to compensate for the lack of information.
Moreover, palliative care specialists indicated the lack of hematologists’ knowledge of palliative care, which further suggests the importance of communication to overcome the differences from each other.
There are several limitations for this study. First, the study was conducted using a snowball sampling and a small number of participants who were from single country. Therefore, its findings cannot be generalized across the groups. Second, although we tried to recruit both hematologists and palliative care specialists from the same hospital, the number of participants from the same hospital is not uniform. However, this study was conducted among standardized facilities providing treatments and palliative care system, and participants were recruited from multiple hospitals with equivalent numbers of the HPCT referral to the national average. 41 Therefore, we consider that there is no significant bias in the results.
Conclusion
The roles of the HPCT were perceived similarly by hematologists and palliative care specialists as pain and psychological management. However hematologists have inadequate knowledge about comprehensive palliative care as the roles of the HPCT. Therefore, the difference in perception of the HPCT’s roles is one of barriers to collaboration. Furthermore, based on hematologists’ and palliative care specialists’ viewpoints, significant barriers to collaboration exist, including not feeling the need to refer, the difficulty in referral timing, the lack of aggressive approach, the negative image of the HPCT, the need for hematologic malignancy-oriented management, and the lack of communication. In this study, we identified the barriers that should be addressed by both the hematology team and the HPCT for a better collaboration. Further work is needed to develop streamlined practices that are sensitive to specialty needs and patients.
Footnotes
Acknowledgments
We would like to thank the participants of this study for their cooperation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI for Grant-in-Aid for Young Scientists Number 23792581 (a representative of the research YUKI SHIRAI).