
Abstract
The hidden curriculum, or the socialization process of medical training, plays a crucial role in the development of physicians, as they navigate the clinical learning environment. The purpose of this qualitative study was to examine medical faculty and students’ perceptions of psychological, moral, and spiritual challenges during medical training in caring for critically ill patients. Focus groups were conducted with 25 Harvard Medical School (HMS) students, and interviews were conducted with 8 HMS faculty members. Five major themes emerged as important in shaping students’ medical training experiences. First, students and faculty discussed the overall significance of the hidden curriculum in terms of the hierarchy of medicine, behavioral modeling, and the value placed on research versus clinical work. Second, respondents articulated values modeled in medicine. Third, students and faculty reflected on changes in student development during their training, particularly in terms of changes in empathy and compassion. Fourth, respondents discussed challenges faced in medical school including professional clinical education and the psychosocial aspects of medical training. Finally, students and faculty articulated a number of coping mechanisms to mitigate these challenges including reflection, prayer, repression, support systems, creative outlets, exercise, and separation from one’s work. The results from this study suggest the significance of the hidden curriculum on medical students throughout their training, as they learn to navigate challenging and emotional experiences. Furthermore, these results emphasize an increased focus toward the effect of the hidden curriculum on students’ development in medical school, particularly noting the ways in which self-reflection may benefit students.
Introduction
The “hidden curriculum” in medical training is used to describe the behaviors, attitudes, assumptions, and beliefs of medicine that are instilled in medical students beginning in the first year of training and becoming more salient throughout residency. 1 –4 Hafferty 1 (p404) refers to the hidden curriculum as “the commonly held ‘understandings,’ customs, rituals, and taken-for-granted aspects of what goes on in the life-space we call medical education.” As opposed to the formal curriculum that occurs in the classroom through lectures, the hidden curriculum exemplifies the “cultural process” of medical training through the socialization of physicians, as they internalize the behaviors, attitudes, and values that are modeled to them in the “moral community” of medical school. 1 –5
As Ozolins et al 6 (p 610) note, the science of medicine is associated with the formal curriculum, while the art of medicine is related to the informal and hidden curriculum. 6 This notion of the hidden curriculum is often distinguished from the informal curriculum. While the informal curriculum refers to the specificities of the hidden curriculum that occur outside the hospital atmosphere, the hidden curriculum encompasses the broader culture of medical training. 7
The hidden curriculum is comprised of several important elements, including role model figures, rules and regulations, medical ethics, medical lingo and jargon, the development (or loss) of professionalism as well as the power hierarchy in medicine. 1,4,8 –11 Often, the content of the hidden curriculum in the clinical learning environment conflicts with what is taught in the formal curriculum in the classroom, and students must navigate these differentiations, especially if and when they may encounter gaps in professionalism and ethical issues. 1,2,11 –13 In addition, several studies have documented the changes, often negative, in students’ development due to the various attitudes and values that are modeled to them during their medical training. 7,14
The importance of the hidden curriculum is not to be overlooked. 4,6,15 While numerous studies have considered the hidden curriculum from the perspective of medical educators, few studies have evaluated the hidden curriculum from the perspective of students. 6 Our study builds on Ozolin et al’s study 6 of students’ views of the hidden curriculum in considering students’ experiences and perceptions of the hidden curriculum in addition to those of faculty members at the same institution. The purpose of this study was to qualitatively describe Harvard Medical School (HMS) students’ psychological, moral, and spiritual challenges and development during the training process of caring for critically ill patients. Our primary research question was how would you describe the changes that have taken place within you as a person in the course of learning how to care for seriously ill hospitalized patients? We also carefully examined the ways in which medical students responded to these changes during their training, in particular considering the challenges they encountered in the hidden curriculum.
Method
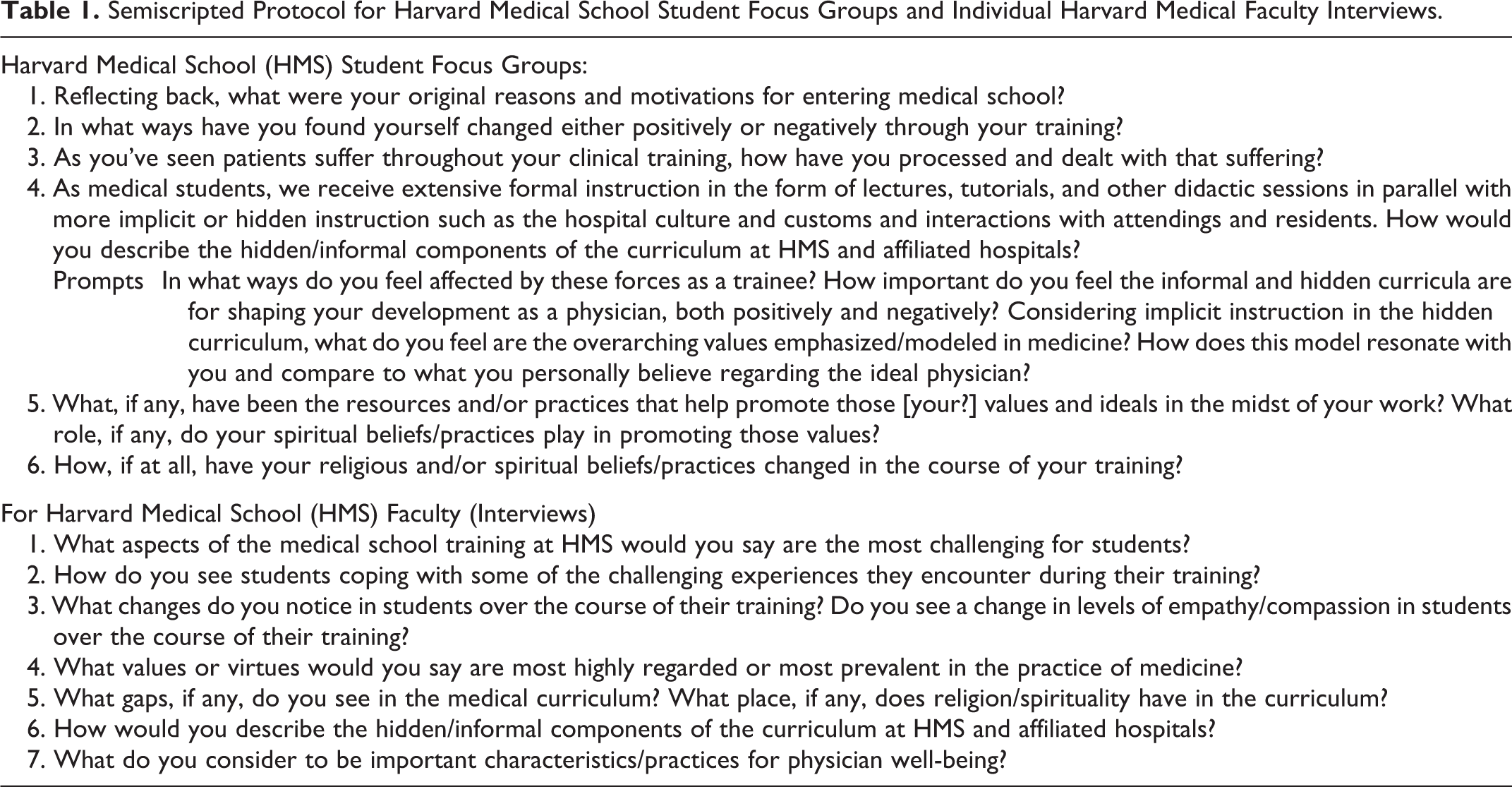
The data for this study come from focus groups conducted with 33 students from HMS and Harvard Divinity School and semistructured interviews conducted with 11 faculty members from both institutions. The data for this article are drawn specifically from students and faculty from HMS for a total of 25 students and 8 faculty members (total sample = 33). The protocol was approved by the Harvard University Faculty of Medicine Institutional Review Board (IRB), and documentation of consent was waived by the IRB. Five focus groups were conducted with students from HMS and included 3 to 5 students per focus group (N = 25), and interviews were conducted with faculty from HMS (N = 8) during 2013 (see Table 1 for interview protocol). Due to the logistical challenges of scheduling a single meeting with multiple senior faculty, we decided to conduct one-on-one interviews with faculty members. We chose to conduct focus groups with students in order to increase the number of students and the range of perspectives and experiences among senior medical students. The interviews and focus groups ranged from 30 to 120 minutes in duration, and the respondents also filled out an anonymous online survey to obtain demographic information. Respondents received a US$25 gift card for participation in the study.
Semiscripted Protocol for Harvard Medical School Student Focus Groups and Individual Harvard Medical Faculty Interviews.
The interviews and focus groups were transcribed and were then imported into the qualitative software program, NVivo (10, QSR International), for data analysis. The data were examined by 5 independent reviewers from 5 different disciplines including psychiatry, chaplaincy, public health, medicine, and theology in order to create a single coding scheme. Three individuals from 3 different disciplines (medicine, chaplaincy, and sociology) then independently coded the data according to the principles of grounded theory. 16 A κ score 17 was calculated (.75), and the coding was compared across the 3 coders to develop 1 master coding list.
Results
The total sample included 33 respondents (51.5% male) of 25 HMS students and 8 HMS faculty. The HMS students were primarily in their fourth year, and eligible Harvard faculty and administration were faculty members identified as being interested in this topic (see Table 2 for demographic information on participants).
Demographic Information of Harvard Medical School Students and Faculty Interview Participants.
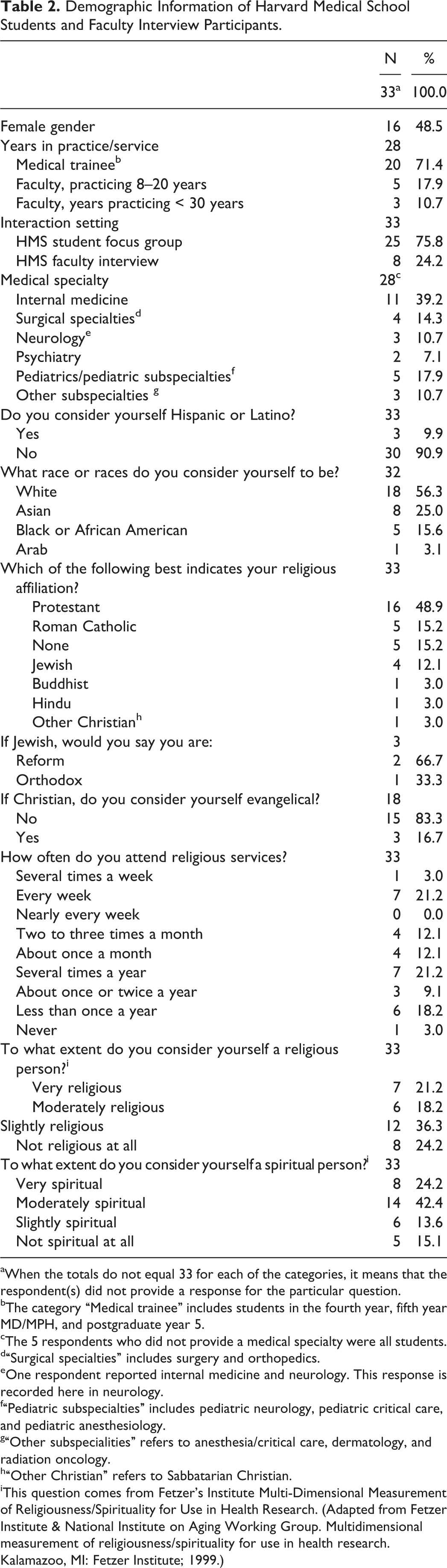
aWhen the totals do not equal 33 for each of the categories, it means that the respondent(s) did not provide a response for the particular question.
bThe category “Medical trainee” includes students in the fourth year, fifth year MD/MPH, and postgraduate year 5.
cThe 5 respondents who did not provide a medical specialty were all students.
d“Surgical specialties” includes surgery and orthopedics.
eOne respondent reported internal medicine and neurology. This response is recorded here in neurology.
f“Pediatric subspecialties” includes pediatric neurology, pediatric critical care, and pediatric anesthesiology.
g“Other subspecialities” refers to anesthesia/critical care, dermatology, and radiation oncology.
h“Other Christian” refers to Sabbatarian Christian.
iThis question comes from Fetzer’s Institute Multi-Dimensional Measurement of Religiousness/Spirituality for Use in Health Research. (Adapted from Fetzer Institute & National Institute on Aging Working Group. Multidimensional measurement of religiousness/spirituality for use in health research. Kalamazoo, MI: Fetzer Institute; 1999.)
Five major themes emerged from the student and faculty responses in the interviews and focus groups (see Table 3). First, respondents commented on the hidden curriculum broadly in medical school. Second, the theme of values modeled in medicine was also important. Third, students and faculty described the changes and development during medical training. Fourth, respondents noted the challenges of medical training, and finally, students and faculty articulated coping strategies for dealing with the difficulties in medical school.
Salient Quotations From the 5 Main Themes From Focus Groups and Interviews With Harvard Medical School Students and Faculty.a
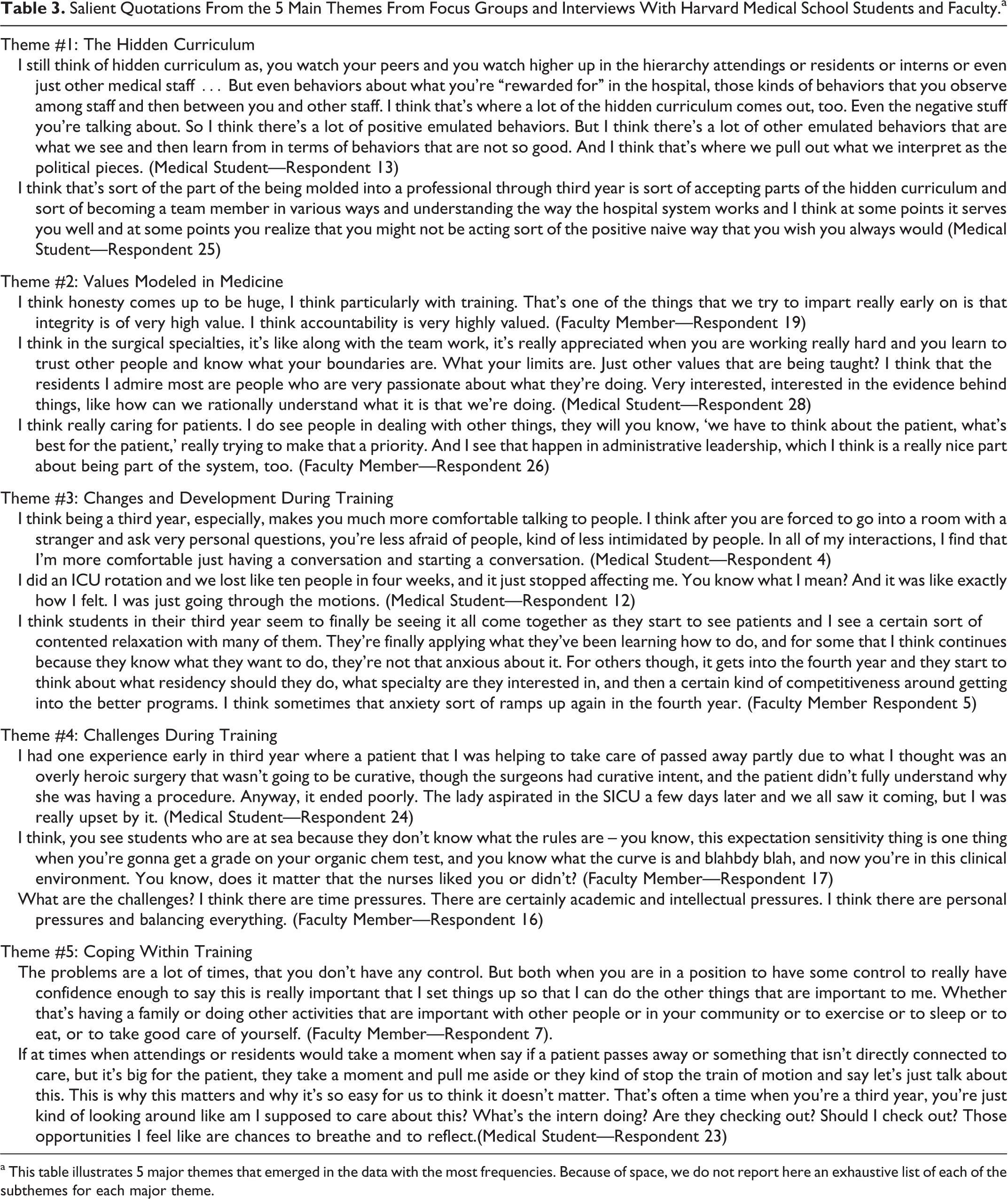
a This table illustrates 5 major themes that emerged in the data with the most frequencies. Because of space, we do not report here an exhaustive list of each of the subthemes for each major theme.
Hidden Curriculum
Students and faculty spoke of the hidden curriculum broadly and of its impact on their training. Four major themes emerged within the theme of the hidden curriculum: the hierarchy of medicine, behavioral modeling, research versus clinical work, and the importance of the hidden curriculum. First, the hierarchy theme was defined as the hospital culture that creates and reinforces power differentials in clinical team environments. As 1 female medical student stated, “You have to learn when it’s okay to talk, when it’s okay to ask questions, and when you need to just kind of be a fly on the wall. I think that’s something that no one can teach you and you just have to pick it up” (Respondent 29). Students also spoke of the importance of team dynamics in the hierarchical system, especially in terms of learning how to interact with others. Second, a majority of students and faculty spoke of behavioral modeling that was defined as student observations and perceived expectations derived from resident and attending behavior as well as attitudes within the hospital culture. Students and faculty spoke of “good” behaviors specifically in terms of positive role models and mentors. On the other hand, faculty and students described having observed “bad” behaviors including “making fun” of patients and objectifying patients. While students did often note these poor behaviors, some of their reflections and the faculty comments reveal that students were able to critically consider these observations: “In fact, we, a number of my students the other day, commented that a number of the doctors they saw were not as patient as they had hoped. In other words, they maybe cut patients short or didn’t spend as much time” (Respondent 18, Faculty Member).
The third theme within the hidden curriculum was the importance of research in addition to clinical work. As one student notes, “That’s the ethos. It’s not good enough to just be an excellent clinician” (Respondent 24), and another student responds to this comment in the focus group: “I think that’s reinforced by students too, not just faculty. I’ve heard students express that view” (Respondent 20). Finally, students and faculty spoke of the importance of the hidden curriculum as a reflection on the impact of the hidden curriculum on student professional development. Students consistently spoke of the hidden curriculum as highly influential, especially in terms of their decision making in medical school: “I think they’re [hidden curriculum] extremely powerful, and it definitely has influenced decisions I’ve made. I kind of feel bad reflecting on it now, but I’m absolutely sure they’ve made a huge impact on decisions, behaviors” (Respondent 22, Student). These cultural norms modeled by others higher up in the hierarchy greatly influenced students’ engagement and early practice of medicine.
Values Modeled in Medicine
When asked about the values of medicine, students and faculty elaborated on a variety of ideals including efficiency and integrity. Excellent patient care was also highly valued, specifically in terms of being a compassionate and thoughtful/respectful clinician, providing patient-centered care and listening to patients. As one HMS faculty member responds to the question of the values of medicine: “In general, integrity, compassion, love, respect, and being a good listener” (Respondent 6). Students also noted evidence-based medicine as an important value in medicine: “I think evidence-based medicine in terms of referencing literature is really highly valued, and I like that. There’s actually less rote memorization and just spitting out information than I expected and people challenge you to back up your findings and if you can cite where the study came from, I think that’s really adding value and I think that’s a really great thing that I’ve learned from HMS” (Respondent 20, Student). Students and faculty also mentioned the importance of teamwork and communication.
Changes and Development During Training
Students and faculty spoke of development through medical school and in particular during the third year. They articulated these changes in terms of empathy and compassion, describing the development of as well as the loss of empathy and compassion. One student stated, “I feel you become very desensitized during your third and fourth-year training, and I think someone said ‘People who are the most sympathetic and empathic tend to be the ones that tend to get jaded more quickly and burnt out towards the end of the third year.’ And I think that’s true in a lot of ways” (Respondent 33). Respondents reported seeing students or themselves becoming cynical or embittered by medical school experiences, while others described no change at all in empathy and compassion. A majority of students and faculty described development during medical training in terms of a growth in confidence, comfort, and maturity, and as one student stated, “you really do become a professional in the true sense of the word” (Respondent 25). Some respondents described changes in behaviors based on efficiency and time management, but these changes were not always positive as some students noted their increasing impatience both in their professional and personal lives. Finally, students also mentioned changes in religion and spirituality during their medical school training, which has been reported in a previous study. 18
Challenges During Training
Students reported facing a number of challenges during their medical training. Both students and faculty articulated these challenges in their professional training in terms of acquiring and assimilating a large knowledge base and facing emotional experiences in the clinical environment. One student described preparing oneself for the challenges of working with critically ill patients: “I think one thing that was harder for me with adults was this loss of dignity, this loss of self, and I hated seeing. for instance, people say, ‘How could you deal with sick kids?’ But, for me, there’s nothing sadder than seeing an adult who is now in diapers or has neurological problems and has lost control of their limbs when they used to be a strong, healthy, athlete or something” (Respondent 10). Both students and faculty also described challenges in confidence and identity, as students faced challenges navigating their career goals and paths. As one faculty member notes: “A lot of them have self-assuredness issues. Am I good enough? Will I be able to make it here, seeing all of their classmates” (Respondent 6). Students and faculty also described challenges with maintaining a positive work–life balance. Finally, students and faculty noted the difficulties in navigating interpersonal relationships in terms of dealing with competition among students, navigating dynamics among team members, finding and building role models, dealing with the lack of communication among medical team members, and facing tension with loved ones.
Coping
While students experienced a variety of challenges throughout their medical training, they did rely on a number of coping strategies. Many students and faculty noted the importance of having a support system whether it be family, friends, or role models within the medical system. As one female medical student notes, “for me, it’s been a lot of mentors, people that you find who have the same values as you and who really prioritize their life to be what you would like yours to be, that have really been the biggest resources for me, and just really models of kind of medical life in spite of being at HMS sometimes” (Respondent 29). Faculty also described emotional maturity as a coping strategy of using innate, developed resiliency mechanisms. Students and faculty also spoke of a variety of coping practices including reflection, prayer, repression, creative outlets, exercise, and separation from one’s work. Students spoke of reflection as an important coping strategy that took many forms: Some described reflection in terms of talking and “venting” with others or journaling, while others spoke of Patient-Doctor 3 (PD3), a case-based course for third-year HMS students to prepare them for patient care, as an opportunity for reflection. Some students spoke of reflecting too often while others not reflecting enough and putting it off. Faith and prayer also played an integral role in coping with the challenges of medical training, particularly with watching patients suffer: “the only way I could deal with it [emotional experience in clinical training] was praying, and yeah, you kind of just find comfort in believing, in really believing, that this is not the all there is to it, that it’s not the end” (Respondent 1).
Discussion
In addition to examining faculty perceptions of the hidden curriculum, this study critically considers the ways in which medical trainees understand and internalize various aspects of the hidden curriculum in their professionalization as physicians. Students and faculty noted the significance of the hidden curriculum in recognizing the importance of research versus clinical work, and they also acknowledged other such values modeled in medicine such as efficiency, integrity, excellent patient care, and teamwork. Many of these values modeled to students through the hidden curriculum influenced their development in their medical training in terms of their orientation toward empathy and compassion for patients, their confidence and maturity, and efficiency, as students learned to adopt many of these values and adapt to the pressures of the medical environment that they came to understand through the hidden curriculum. Medical trainees and faculty members also articulated a number of challenges students faced during their training and the coping mechanisms they employed as a result. As the data from this study demonstrate, the students’ development and changes throughout their training are directly influenced by the hidden curriculum and the values and behaviors that are modeled to them.
These 5 themes are consistent with other studies on the hidden curriculum in medical school. Lempp and Seale’s qualitative study 8 of the hidden curriculum in medical education revealed that personal encouragement from positive role models was an important factor in students’ training, which is similar to our finding of positive behavioral modeling in the hidden curriculum. Other studies have also noted the importance of the hierarchy in medicine in terms of learning through the hidden curriculum. 4,8,19,20 Similar to our finding of the importance of teamwork in medicine, studies have addressed the effect of collegiality in the medical environment as the relationship between group membership and individual performance as well as the importance of communicating and working within teams. 4,20
Related studies have also found that students believe that excellent and patient-centered care and compassion are crucial to the practice of medicine and that the hidden curriculum is highly valued among students as they are transition into becoming physicians. 14,15,21 Previous work has considered the importance of the hidden curriculum, as it contributes to the development of professionalism for physicians-in-training, and our study confirms these findings. 10,21 In addition, the data from this study confirm previous findings that students are not only passive recipients of the hidden curriculum but also internalize what they learn as it contributes to their identity as soon-to-be physicians. 11,19
There is little opportunity within the formal medical curriculum to discuss the various emotional experiences of students, but self-reflection through small group discussions and mentorship is especially important in order to maximize the positive effects of the hidden curriculum and to think critically about the mixed messages medical students may receive between the classroom and the clinical learning environment. 12 In addition, several other studies have noted that medical educators need to recognize the role of internal and external factors in medical training that students receive. 7,22,23 The data from this and previous studies inform the future development of physician well-being curricula and wellness initiatives, as the data clearly articulate the content of the hidden curriculum and its effects in an important way. Curricula are needed to help students understand ways to reduce physician burnout and compassion fatigue by engaging their own spirituality into their medical practice as physicians.
This study is limited by the fact that it draws on qualitative interview and focus group data from 1 medical school and cannot be generalizable to all medical training programs in the country. Despite the limitations of this study, the data provide insight into the ways in which medical students respond to the hidden curriculum and adds to the existing literature on the importance of the hidden curriculum to students’ socialization in medicine. Future research that provides a comprehensive understanding of medical students’ psychosocial experiences and emotional challenges during their training will be helpful in designing opportunities for students to reflect on their experiences so that they can focus on providing the best care possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a Templeton Foundation Award and a University of Chicago Program in Religion and Medicine Faculty Scholars Award.